
Multimodal Management of Fecal Incontinence Focused on Sphincteroplasty: Long-Term Outcomes from a Single Center Case Series

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Surgical Technique
2.2. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Parks, A.G.; McPartlin, J.F. Late repair of injuries of the anal sphincter. Proc. R. Soc. Med. 1971, 64, 1187–1189. [Google Scholar] [CrossRef] [Green Version]
- Tjandra, J.J.; Han, W.R.; Goh, J.; Carey, M.; Dwyer, P. Direct repair vs. overlapping sphincter repair: A randomized, controlled trial. Dis. Colon Rectum 2003, 46, 937–942. [Google Scholar] [CrossRef] [PubMed]
- Malouf, A.J.; Norton, C.S.; Engel, A.F.; Nicholls, R.J.; Kamm, M.A. Long-term results of overlapping anterior anal-sphincter repair for obstetric trauma. Lancet 2000, 355, 260–265. [Google Scholar] [CrossRef]
- Halverson, A.L.; Hull, T.L. Long-term outcome of overlapping anal sphincter repair. Dis. Colon Rectum 2002, 45, 345–348. [Google Scholar] [CrossRef] [PubMed]
- Glasgow, S.C.; Lowry, A.C. Long-term outcomes of anal sphincter repair for fecal incontinence: A systematic review. Dis. Colon Rectum 2012, 55, 482–490. [Google Scholar] [CrossRef] [PubMed]
- Nicholls, J. Sphincter repair for incontinence. Colorectal Dis. 2009, 11, 545–546. [Google Scholar] [CrossRef]
- McNicol, F.J.; Bruce, C.A.; Chaudhri, S.; Francombe, J.; Kozman, E.; Taylor, B.A.; Tighe, M.J. Management of obstetric anal sphincter injuries—A role for the colorectal surgeon. Colorectal Dis. 2010, 12, 927–930. [Google Scholar] [CrossRef]
- Roos, A.M.; Thakar, R.; Sultan, A.H. Outcome of primary repair of obstetric anal sphincter injuries (OASIS): Does the grade of tear matter? Ultrasound Obstet. Gynecol. 2010, 36, 368–374. [Google Scholar] [CrossRef]
- Jarrett, M.E.; Mowatt, G.; Glazener, C.M.; Fraser, C.; Nicholls, R.J.; Grant, A.M.; Kamm, M.A. Systematic review of sacral nerve stimulation for faecal incontinence and constipation. Br. J. Surg. 2004, 91, 1559–1569. [Google Scholar] [CrossRef]
- Chan, M.K.; Tjandra, J.J. Sacral nerve stimulation for fecal incontinence: External anal sphincter defect vs. intact anal sphincter. Dis. Colon Rectum 2008, 51, 1015–1024. [Google Scholar] [CrossRef]
- Melenhorst, J.; Koch, S.M.; Uludag, O.; van Gemert, W.G.; Baeten, C.G. Is a morphologically intact anal sphincter necessary for success with sacral nerve modulation in patients with faecal incontinence? Colorectal Dis. 2008, 10, 257–262. [Google Scholar] [CrossRef]
- Ratto, C.; Litta, F.; Parello, A.; Donisi, L.; De Simone, V.; Zaccone, G. Sacral nerve stimulation in faecal incontinence associated with an anal sphincter lesion: A systematic review. Colorectal Dis. 2012, 14, e297–e304. [Google Scholar] [CrossRef] [PubMed]
- Lehur, P.A.; Christoforidis, D. Is anal sphincteroplasty out-dated in the era of sacral neuro modulation? J. Visc. Surg. 2020, 157, 1–2. [Google Scholar] [CrossRef] [PubMed]
- Berg, M.R.; Gregussen, H.; Sahlin, Y. Long-term outcome of sphincteroplasty with separate suturing of the internal and the external anal sphincter. Tech. Coloproctol. 2019, 23, 1163–1172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gotzsche, P.C.; Vandenbroucke, J.P.; Initiative, S. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. Lancet 2007, 370, 1453–1457. [Google Scholar] [CrossRef]
- Jorge, J.M.; Wexner, S.D. Etiology and management of fecal incontinence. Dis. Colon Rectum 1993, 36, 77–97. [Google Scholar] [CrossRef]
- Rothbarth, J.; Bemelman, W.A.; Meijerink, W.J.; Stiggelbout, A.M.; Zwinderman, A.H.; Buyze-Westerweel, M.E.; Delemarre, J.B. What is the impact of fecal incontinence on quality of life? Dis. Colon Rectum 2001, 44, 67–71. [Google Scholar] [CrossRef]
- Corman, M.L. Anal incontinence following obstetrical injury. Dis. Colon Rectum 1985, 28, 86–89. [Google Scholar] [CrossRef]
- Mazur-Bialy, A.I.; Kolomanska-Bogucka, D.; Oplawski, M.; Tim, S. Physiotherapy for Prevention and Treatment of Fecal Incontinence in Women-Systematic Review of Methods. J. Clin. Med. 2020, 9, 3255. [Google Scholar] [CrossRef]
- Grey, B.R.; Sheldon, R.R.; Telford, K.J.; Kiff, E.S. Anterior anal sphincter repair can be of long term benefit: A 12-year case cohort from a single surgeon. BMC Surg. 2007, 7, 1. [Google Scholar] [CrossRef] [Green Version]
- Zorcolo, L.; Covotta, L.; Bartolo, D.C. Outcome of anterior sphincter repair for obstetric injury: Comparison of early and late results. Dis. Colon Rectum 2005, 48, 524–531. [Google Scholar] [CrossRef]
- Oom, D.M.; Gosselink, M.P.; Schouten, W.R. Anterior sphincteroplasty for fecal incontinence: A single center experience in the era of sacral neuromodulation. Dis. Colon Rectum 2009, 52, 1681–1687. [Google Scholar] [CrossRef] [PubMed]
- Maslekar, S.; Gardiner, A.B.; Duthie, G.S. Anterior anal sphincter repair for fecal incontinence: Good longterm results are possible. J. Am. Coll. Surg. 2007, 204, 40–46. [Google Scholar] [CrossRef] [PubMed]
- Londono-Schimmer, E.E.; Garcia-Duperly, R.; Nicholls, R.J.; Ritchie, J.K.; Hawley, P.R.; Thomson, J.P. Overlapping anal sphincter repair for faecal incontinence due to sphincter trauma: Five year follow-up functional results. Int. J. Colorectal Dis. 1994, 9, 110–113. [Google Scholar] [CrossRef] [PubMed]
- Barisic, G.I.; Krivokapic, Z.V.; Markovic, V.A.; Popovic, M.A. Outcome of overlapping anal sphincter repair after 3 months and after a mean of 80 months. Int. J. Colorectal Dis. 2006, 21, 52–56. [Google Scholar] [CrossRef]
- Lehto, K.; Hyoty, M.; Collin, P.; Huhtala, H.; Aitola, P. Seven-year follow-up after anterior sphincter reconstruction for faecal incontinence. Int. J. Colorectal Dis. 2013, 28, 653–658. [Google Scholar] [CrossRef]
- Osterberg, A.; Graf, W.; Holmberg, A.; Pahlman, L.; Ljung, A.; Hakelius, L. Long-term results of anterior levatorplasty for fecal incontinence. A retrospective study. Dis. Colon Rectum 1996, 39, 671–674. [Google Scholar] [CrossRef]
- Lamblin, G.; Bouvier, P.; Damon, H.; Chabert, P.; Moret, S.; Chene, G.; Mellier, G. Long-term outcome after overlapping anterior anal sphincter repair for fecal incontinence. Int. J. Colorectal Dis. 2014, 29, 1377–1383. [Google Scholar] [CrossRef]
- Evans, C.; Davis, K.; Kumar, D. Overlapping anal sphincter repair and anterior levatorplasty: Effect of patient’s age and duration of follow-up. Int. J. Colorectal Dis. 2006, 21, 795–801. [Google Scholar] [CrossRef]
- Miller, R.; Orrom, W.J.; Cornes, H.; Duthie, G.; Bartolo, D.C. Anterior sphincter plication and levatorplasty in the treatment of faecal incontinence. Br. J. Surg. 1989, 76, 1058–1060. [Google Scholar] [CrossRef]
- Bravo Gutierrez, A.; Madoff, R.D.; Lowry, A.C.; Parker, S.C.; Buie, W.D.; Baxter, N.N. Long-term results of anterior sphincteroplasty. Dis. Colon Rectum 2004, 47, 727–731. [Google Scholar] [CrossRef] [PubMed]
- Zutshi, M.; Tracey, T.H.; Bast, J.; Halverson, A.; Na, J. Ten-year outcome after anal sphincter repair for fecal incontinence. Dis. Colon Rectum 2009, 52, 1089–1094. [Google Scholar] [CrossRef] [PubMed]
- Warner, M.W.; Jones, O.M.; Lindsey, I.; Cunningham, C.; Mortensen, N.J. Long-term follow-up after anterior sphincter repair: Influence of age on functional outcome. Colorectal Dis. 2012, 14, 1380–1388. [Google Scholar] [CrossRef] [PubMed]
- Karoui, S.; Leroi, A.M.; Koning, E.; Menard, J.F.; Michot, F.; Denis, P. Results of sphincteroplasty in 86 patients with anal incontinence. Dis. Colon Rectum 2000, 43, 813–820. [Google Scholar] [CrossRef] [PubMed]
- Mevik, K.; Norderval, S.; Kileng, H.; Johansen, M.; Vonen, B. Long-term results after anterior sphincteroplasty for anal incontinence. Scand. J. Surg. 2009, 98, 234–238. [Google Scholar] [CrossRef] [Green Version]
- Ong, K.; Bordeianou, L.; Brunner, M.; Buntzen, S.; Collie, M.H.S.; Hanly, A.; Hunt, C.W.; Matzel, K.E.; O’Connell, P.R.; Rydningen, M.; et al. Changing paradigm of sacral neuromodulation and external anal sphincter repair for faecal incontinence in specialist centres. Colorectal Dis. 2021, 23, 710–715. [Google Scholar] [CrossRef]
- Maeda, Y.; Lundby, L.; Buntzen, S.; Laurberg, S. Suboptimal outcome following sacral nerve stimulation for faecal incontinence. Br. J. Surg. 2011, 98, 140–147. [Google Scholar] [CrossRef]
- Oliveira, L.; Pfeifer, J.; Wexner, S.D. Physiological and clinical outcome of anterior sphincteroplasty. Br. J. Surg. 1996, 83, 502–505. [Google Scholar] [CrossRef]
- Barbosa, M.; Glavind-Kristensen, M.; Moller Soerensen, M.; Christensen, P. Secondary sphincter repair for anal incontinence following obstetric sphincter injury: Functional outcome and quality of life at 18 years of follow-up. Colorectal Dis. 2020, 22, 71–79. [Google Scholar] [CrossRef]
- Oom, D.M.; Steensma, A.B.; Zimmerman, D.D.; Schouten, W.R. Anterior sphincteroplasty for fecal incontinence: Is the outcome compromised in patients with associated pelvic floor injury? Dis. Colon Rectum 2010, 53, 150–155. [Google Scholar] [CrossRef]
- Johnson, E.; Carlsen, E.; Steen, T.B.; Backer Hjorthaug, J.O.; Eriksen, M.T.; Johannessen, H.O. Short- and long-term results of secondary anterior sphincteroplasty in 33 patients with obstetric injury. Acta Obstet. Gynecol. Scand. 2010, 89, 1466–1472. [Google Scholar] [CrossRef] [PubMed]
- Bordeianou, L.G.; Anger, J.T.; Boutros, M.; Birnbaum, E.; Carmichael, J.C.; Connell, K.A.; De, E.J.B.; Mellgren, A.; Staller, K.; Vogler, S.A.; et al. Measuring Pelvic Floor Disorder Symptoms Using Patient-Reported Instruments: Proceedings of the Consensus Meeting of the Pelvic Floor Consortium of the American Society of Colon and Rectal Surgeons, the International Continence Society, the American Urogynecologic Society, and the Society of Urodynamics, Female Pelvic Medicine and Urogenital Reconstruction. Dis. Colon Rectum 2020, 63, 6–23. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| n = 120 | |||
|---|---|---|---|
| Age (Years) * | 59 (16–84) | ||
| Gender | Male | 7 (6) | |
| Female | 113 (94) | ||
| Duration of symptoms before surgery (Months) * | 120 (10–480) | ||
| Baseline CCIS | Total * | 18 (9–20) | |
| 0–8 | 0 (0) | ||
| 9–15 | 11 (9.2) | ||
| >15 | 109 (90.8) | ||
| Preoperatory Manometric Variables | RP (LNR: 65 mmHg) ‡ | 27 (20–35) | |
| MSP (LNR: 140 mmHg) ‡ | 50 (38–64) | ||
| SL (cm) ‡ | 2.6 (2–3) | ||
| Endoanal Ultrasound (81) | EAS defect | 81 (100) | |
| IAS defect | 41 (50.6) | ||
| Previous Obstetric History ¥ | Vaginal Deliveries | 98 (86.7) | |
| Episiotomy (Range 1–5) | 78 (69) | ||
| Third-Fourth degree tear | 41 (36.3) | ||
| Concomitant Pelvic Floor Disorders ¥ | Rectocele | 15 (13) | |
| Recto-Vaginal Fistula | 10 (9) | ||
| Pelvic floor descent | 9 (8) | ||
| Rectal Prolapse | 4 (3.5) | ||
| Enterocele | 3 (2.6) | ||
| Anal Incontinence Surgical Techniques | Apposition Sphincteroplasty | 1 (0.83) | |
| Overlapping Sphincteroplasty (119 cases/99.1%) | OSph Alone | 12 (10) | |
| OSph + ALev | 14 (11.6) | ||
| OSph + IAS repair | 16 (13.3) | ||
| OSph + ALev + IAS repair | 68 (56.6) | ||
| OSph + TPFR | 8 (6,6) | ||
| OSph + Postanal Repair | 1 (0.83) | ||
| Associated Pathologies Surgical Treatment | Rectocele | 13 (10.8) | |
| Corman’s graft | 8 (6.6) | ||
| Recto-Vaginal Fistula | 6 (5) | ||
| Enterocele | 2 (1.66) | ||
| Hemorrhoidectomy | 2 (1.66) | ||
| Rectal Prolapse (Delorme) | 1 (0.83) | ||
| Rectal Villous Adenoma Removal | 1 (0.83) | ||
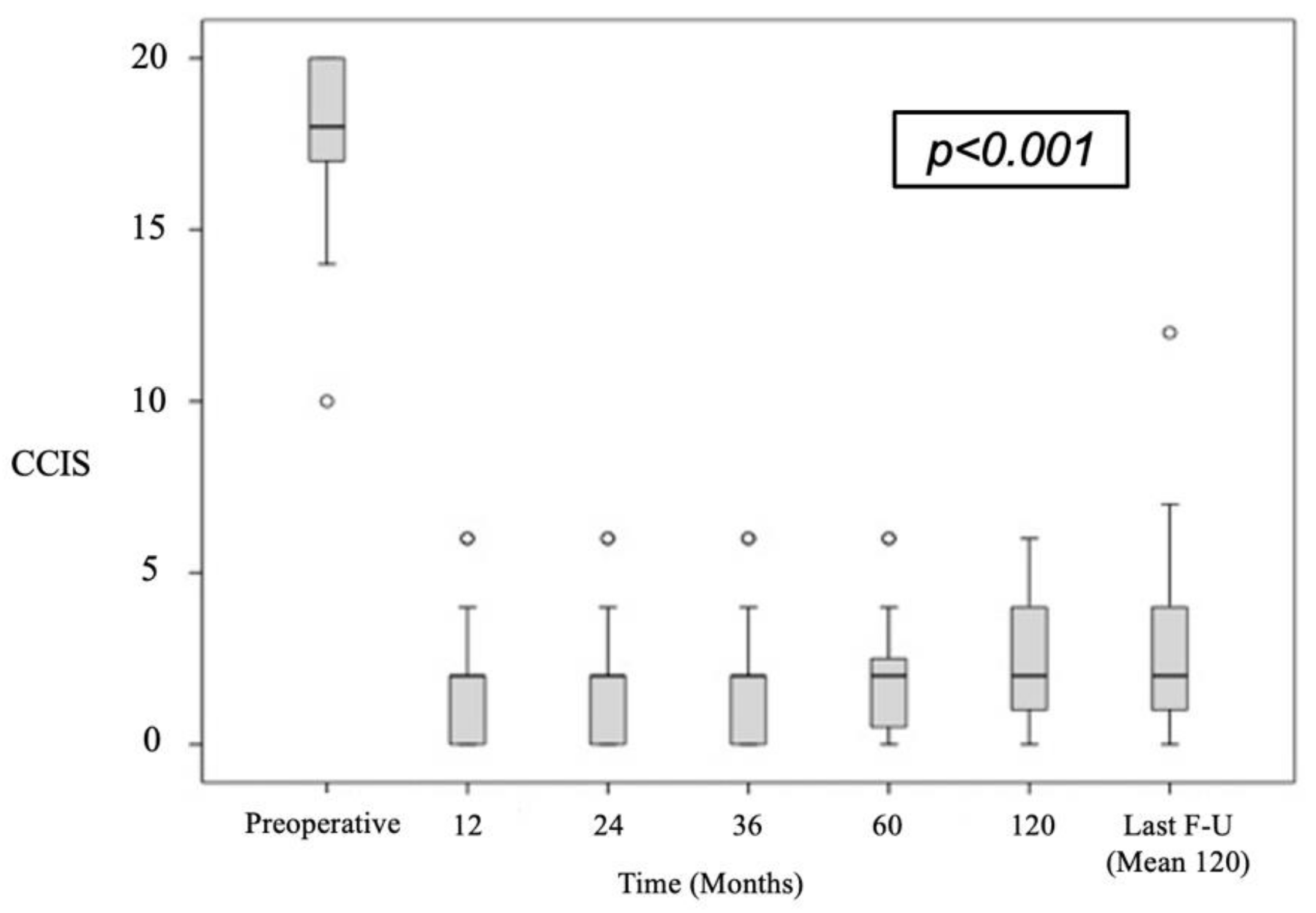
| CCIS | 95%-CI | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Time | n | Preop. | SD | Postop. | SD | Mean Dif. | Inferior | Superior | p |
| 12 m | 117 | 17.9 | 2.3 | 2.8 | 3.3 | 15.1 | 14.4 | 15.9 | <0.001 |
| 24 m | 116 | 17.9 | 2.3 | 3 | 3.4 | 15 | 14.2 | 15.8 | <0.001 |
| 36 m | 107 | 18 | 2.1 | 2.6 | 3 | 15.4 | 14.6 | 16.2 | <0.001 |
| 60 m | 95 | 18 | 2.1 | 2.8 | 3 | 15.2 | 14.4 | 16 | <0.001 |
| 120 m | 60 | 18.1 | 2.1 | 2.4 | 1.9 | 15.8 | 15.1 | 16.5 | <0.001 |
| Last F-U | 105 | 18 | 2.3 | 3.7 | 3.9 | 14.3 | 13.5 | 15.1 | <0.001 |
| Need of Additional Treatments | Satisfactory Results (>50% Reduction in CCIS) | ||||||
|---|---|---|---|---|---|---|---|
| No n (%) | Yes n (%) | p | No n (%) | Yes n (%) | p | ||
| Age (years) * | 53.9 (17) | 56.4 (13) | 0.4 | 56 (14) | 53.8 (15) | 0.67 | |
| Sex | Female (113) | 73 (64.6) | 40 (35.4) | 0.71 | 8 (7.6) | 97 (92.4) | 0.45 |
| Male (7) | 5 (71.4) | 2 (28.6) | 0 (0) | 7 (100) | |||
| Duration of FI (months) * | 55.4 | 39.6 | 0.29 | 51.1 | 49.2 | 0.95 | |
| Location of Sphincter Tear | Anterior (104) | 67 (64.4) | 37 (35.6) | 0.49 | 7 (7.2) | 90 (92.8) | 0.71 |
| Posterior or Lateral (16) | 11 (68.8) | 5 (31.3) | 1 (6.7) | 14 (93.3) | |||
| Tear Grades * | 126 (27) | 126 (30) | 0.93 | 115 (30) | 128 (27) | 0.27 | |
| IAS Repair | Yes (84) | 54 (64.3) | 30 (35.7) | 0.8 | 4 (5.1) | 74 (94.9) | 0.21 |
| No (36) | 24 (66.7) | 12 (33.3) | 4 (11.8) | 30 (88.2) | |||
| Levatorplasty | Yes (82) | 55 (67.1) | 27 (32.9) | 0.48 | 6 (7.8) | 71 (92.2) | 0.69 |
| No (38) | 23 (60.5) | 15 (39.5) | 2 (5.7) | 33 (94.3) | |||
| Associated Surgical Techniques | Yes (33) | 25 (75.8) | 8 (24,2) | 0.13 | 2 (6.7) | 28 (93.3) | 0.9 |
| No (87) | 53 (60.9) | 34 (39.1) | 6 (7.3) | 76 (92.7) | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cerdán Santacruz, C.; Cerdán Santacruz, D.M.; Milla Collado, L.; Ruiz de León, A.; Cerdán Miguel, J. Multimodal Management of Fecal Incontinence Focused on Sphincteroplasty: Long-Term Outcomes from a Single Center Case Series. J. Clin. Med. 2022, 11, 3755. https://doi.org/10.3390/jcm11133755
Cerdán Santacruz C, Cerdán Santacruz DM, Milla Collado L, Ruiz de León A, Cerdán Miguel J. Multimodal Management of Fecal Incontinence Focused on Sphincteroplasty: Long-Term Outcomes from a Single Center Case Series. Journal of Clinical Medicine. 2022; 11(13):3755. https://doi.org/10.3390/jcm11133755
Chicago/Turabian StyleCerdán Santacruz, Carlos, Débora M. Cerdán Santacruz, Lucía Milla Collado, Antonio Ruiz de León, and Javier Cerdán Miguel. 2022. "Multimodal Management of Fecal Incontinence Focused on Sphincteroplasty: Long-Term Outcomes from a Single Center Case Series" Journal of Clinical Medicine 11, no. 13: 3755. https://doi.org/10.3390/jcm11133755