
The Risk of Developing Alzheimer’s Disease and Parkinson’s Disease in Patients with Inflammatory Bowel Disease: A Meta-Analysis


Abstract
:1. Introduction
2. Methods
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Quality Assessment
2.4. Data Extraction
2.5. Statistical Analysis
3. Results
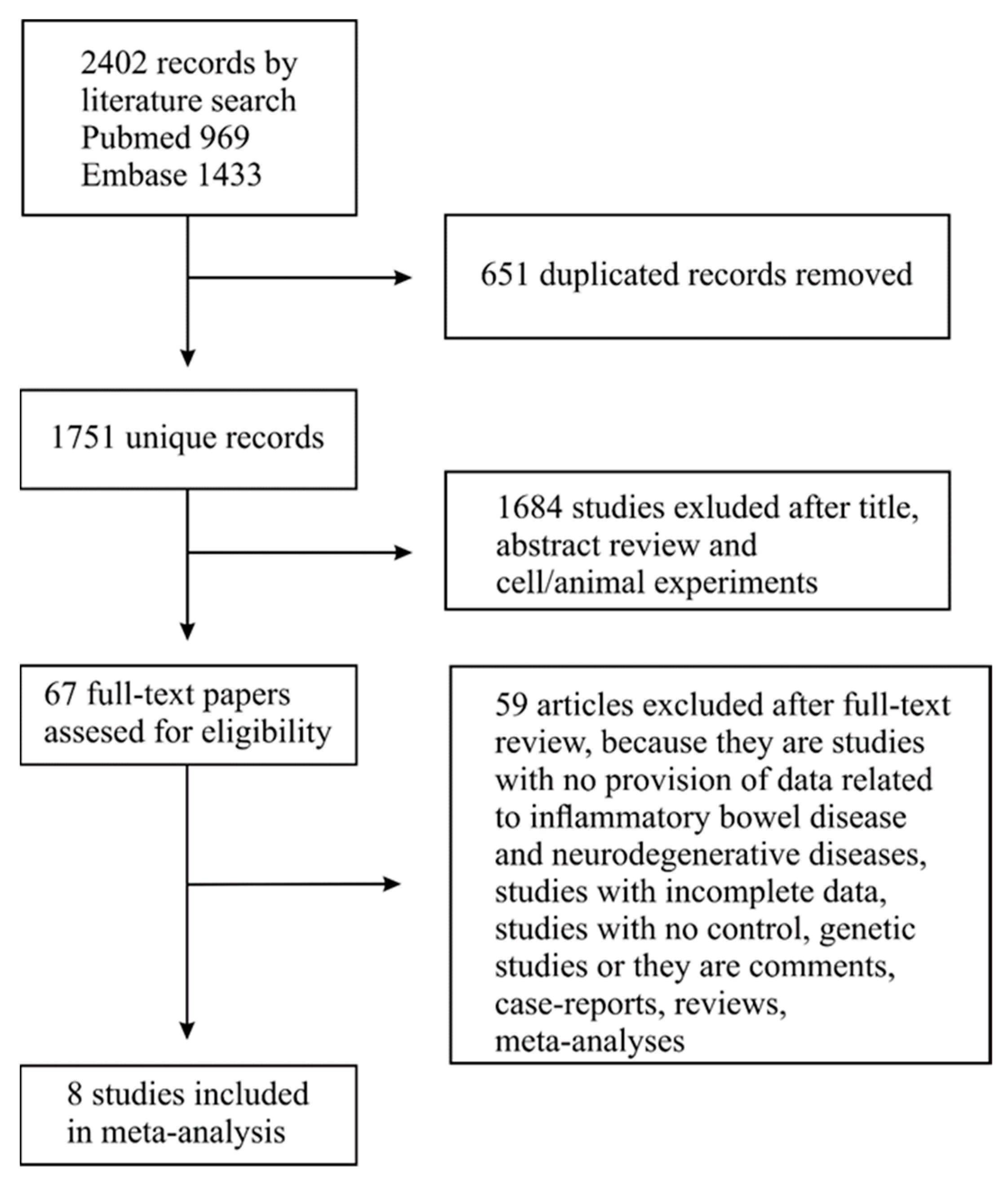
3.1. Search Results
3.2. Characteristics of the Included Studies
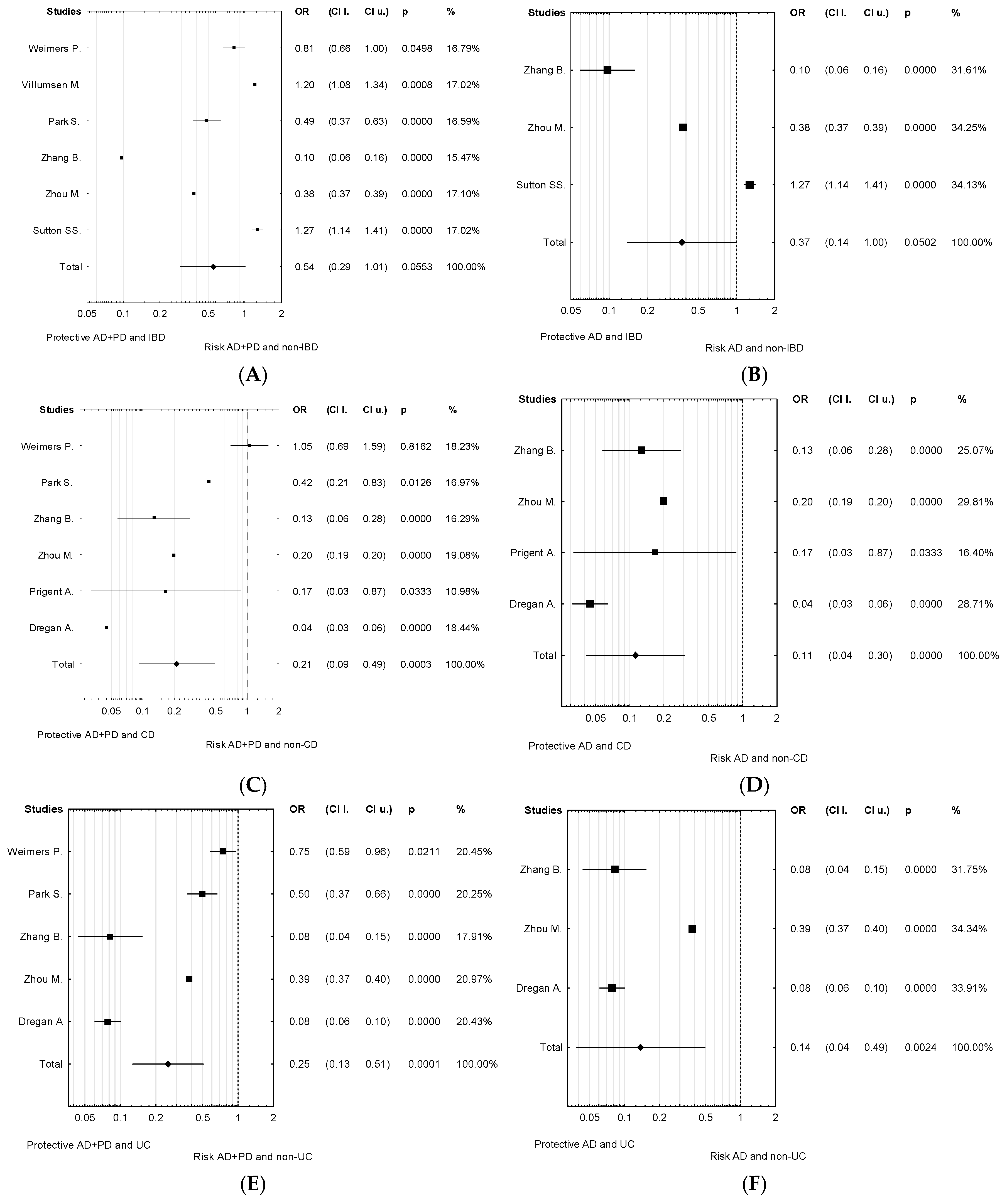
3.3. Association between IBD and Neurodegenerative Diseases
3.4. Evaluation of Publication Bias
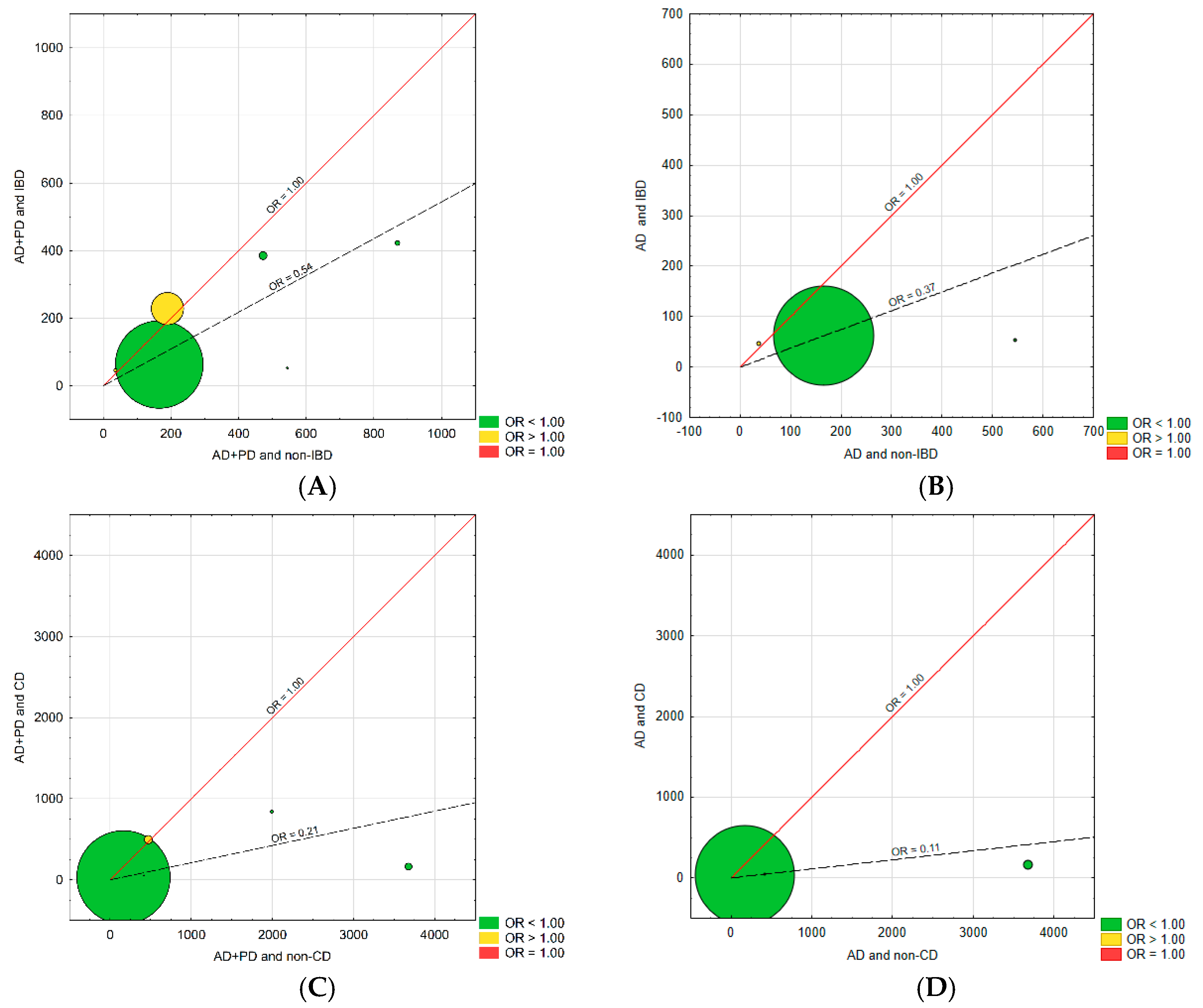
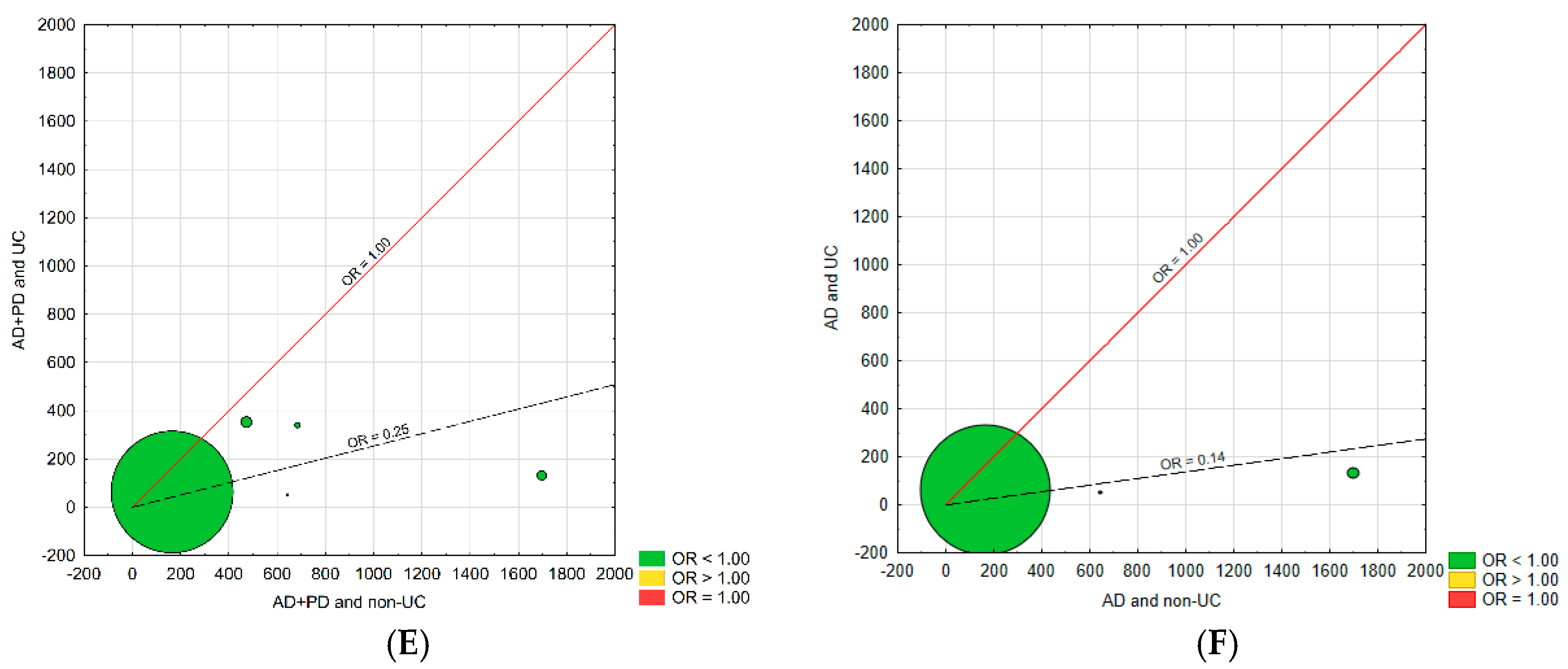
3.5. Heterogeneity Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Neish, A.S. Microbes in gastrointestinal health and disease. Gastroenterology 2009, 136, 65–80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al Bander, Z.; Nitert, M.D.; Mousa, A.; Naderpoor, N. The gut microbiota and inflammation: An overview. Int. J. Environ. Res. Public Health 2020, 17, 7618. [Google Scholar] [CrossRef] [PubMed]
- Góralska, K.; Dzikowiec, M. Role of microbiota in maintaining the homeostasis in the human body. Post. Mikrobiol. 2018, 57, 5–11. [Google Scholar] [CrossRef]
- Amoroso, C.; Perillo, F.; Strati, F.; Fantini, M.; Caprioli, F.; Facciotti, F. The role of gut microbiota biomodulators on mucosal immunity and intestinal inflammation. Cells 2020, 9, 1234. [Google Scholar] [CrossRef]
- Sartor, R.B.; Wu, G.D. Roles for intestinal bacteria, viruses, and fungi in pathogenesis of inflammatory bowel diseases and therapeutic approaches. Gastroenterology 2017, 152, 327–339. [Google Scholar] [CrossRef] [Green Version]
- Szandruk-Bender, M.; Rutkowska, M.; Merwid-Ląd, A.; Wiatrak, B.; Szeląg, A.; Dzimira, S.; Sobieszczańska, B.; Krzystek-Korpacka, M.; Kucharska, A.Z.; Matuszewska, A.; et al. Cornelian cherry iridoid-polyphenolic extract improves mucosal epithelial barrier integrity in rat experimental colitis and exerts antimicrobial and antiadhesive activities in vitro. Oxidative Med. Cell. Longev. 2020, 2020, 7697851. [Google Scholar] [CrossRef]
- Schirmer, M.; Garner, A.; Vlamakis, H.; Xavier, R.J. Microbial genes and pathways in inflammatory bowel disease. Nat. Rev. Microbiol. 2019, 17, 497–511. [Google Scholar] [CrossRef]
- Dinan, T.G.; Cryan, J.F. Gut instincts: Microbiota as a key regulator of brain development, ageing and neurodegeneration. J. Physiol. 2016, 595, 489–503. [Google Scholar] [CrossRef]
- Burokas, A.; Moloney, R.D.; Dinan, T.G.; Cryan, J.F. Microbiota regulation of the Mammalian gut-brain axis. Adv. Appl. Microbiol. 2015, 91, 1–62. [Google Scholar]
- Wiatrak, B.; Balon, K.; Jawień, P.; Bednarz, D.; Jęśkowiak, I.; Szeląg, A. The role of the microbiota-gut-brain axis in the development of Alzheimer’s disease. Int. J. Mol Sci. 2022, 23, 4862. [Google Scholar] [CrossRef]
- Villain, N.; Dubois, B. Alzheimer’s disease including focal presentations. Semin. Neurol. 2019, 39, 213–226. [Google Scholar] [CrossRef] [PubMed]
- Lebouvier, T.; Chaumette, T.; Paillusson, S.; Duyckaerts, C.; Bruley des Varannes, S.; Neunlist, M.; Derkinderen, P. The second brain and Parkinson’s disease. Eur. J. Neurosci. 2009, 30, 735–741. [Google Scholar] [CrossRef] [PubMed]
- Scheltens, P.; Blennow, K.; Breteler, M.M.B.; de Strooper, B.; Frisoni, G.B.; Salloway, S.; Van der Flier, W.M. Alzheimer’s disease. Lancet 2016, 388, 505–517. [Google Scholar] [CrossRef]
- Wang, Q.; Liu, Y.; Zhou, J. Neuroinflammation in Parkinson’s disease and its potential as therapeutic target. Transl. Neurodegener. 2015, 4, 19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Westfall, S.; Lomis, N.; Kahouli, I.; Dia, S.Y.; Singh, S.P.; Prakash, S. Microbiome, probiotics and neurodegenerative diseases: Deciphering the gut brain axis. Cell. Mol. Life Sci. 2017, 74, 3769–3787. [Google Scholar] [CrossRef]
- Houser, M.C.; Tansey, M.G. The gut-brain axis: Is intestinal inflammation a silent driver of Parkinson’s disease pathogenesis? NPJ Parkinsons Dis. 2017, 3, 3. [Google Scholar] [CrossRef]
- Zhu, F.; Li, C.; Gong, J.; Zhu, W.; Gu, L.; Li, N. The risk of Parkinson’s disease in inflammatory bowel disease: A systematic review and meta-analysis. Dig. Liver Dis. 2019, 51, 38–42. [Google Scholar] [CrossRef]
- Zhu, Y.; Yuan, M.; Liu, Y.; Yang, F.; Chen, W.Z.; Xu, Z.Z.; Xiang, Z.B.; Xu, R.S. Association between inflammatory bowel diseases and Parkinson’s disease: Systematic review and meta-analysis. Neural Regen. Res. 2021, 17, 344–353. [Google Scholar]
- Pistollato, F.; Cano, S.S.; Elio, I.; Vergara, M.M.; Giampieri, F.; Battino, M. Role of gut microbiota and nutrients in amyloid formation and pathogenesis of Alzheimer disease. Nutr. Rev. 2016, 74, 624–634. [Google Scholar] [CrossRef] [Green Version]
- Erny, D.; Hrabě de Angelis, A.L.; Jaitin, D.; Wieghofer, P.; Staszewski, O.; David, E.; Keren-Shaul, H.; Mahlakoiv, T.; Jakobshagen, K.; Buch, T.; et al. Host microbiota constantly control maturation and function of microglia in the CNS. Nat. Neurosci. 2015, 18, 965–977. [Google Scholar] [CrossRef]
- Ghaisas, S.; Maher, J.; Kanthasamy, A. Gut microbiome in health and disease: Linking the microbiome–gut–brain axis and environmental factors in the pathogenesis of systemic and neurodegenerative diseases. Pharmacol. Ther. 2016, 158, 52–62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Babulal, G.M.; Quiroz, Y.T.; Albensi, B.C.; Arenaza-Urquijo, E.; Astell, A.J.; Babiloni, C.; Bahar-Fuchs, A.; Bell, J.; Bowman, G.L.; Brickman, A.M.; et al. Perspectives on ethnic and racial disparities in Alzheimer’s disease and related dementias: Update and areas of immediate need. Alzheimers Dement. 2019, 15, 292–312. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. J. Clin. Epidemiol. 2009, 62, 1006–1012. [Google Scholar] [CrossRef] [PubMed]
- Cleophas, T.J.; Zwinderman, A.H. Modern Meta-Analysis; Springer International Publishing: Cham, Switzerland, 2017. [Google Scholar]
- Stang, A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur. J. Epidemiol. 2010, 25, 603–605. [Google Scholar] [CrossRef] [Green Version]
- Herzog, R.; Álvarez-Pasquin, M.J.; Díaz, C.; del Barrio, J.L.; Estrada, J.M.; Gil, A. Are healthcare workers intentions to vaccinate related to their knowledge, beliefs and attitudes? A systematic review. BMC Public Health 2013, 13, 154. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, X.; Kong, L.; Li, F.; Chen, C.; Xu, R.; Wang, H.; Peng, S.; Zhou, M.; Li, B. Association between psoriasis and chronic obstructive pulmonary disease: A systematic review and meta-analysis. PLoS ONE 2015, 10, e0145221. [Google Scholar] [CrossRef] [Green Version]
- Von Hippel, P.T. The heterogeneity statistic I(2) can be biased in small meta-analyses. BMC Med. Res. Methodol. 2015, 15, 35. [Google Scholar] [CrossRef] [Green Version]
- Song, F. Exploring heterogeneity in meta-analysis: Is the L’Abbé plot useful? J. Clin. Epidemiol. 1999, 52, 725–730. [Google Scholar] [CrossRef]
- Dregan, A.; Chowienczyk, P.; Gulliford, M.C. Are inflammation and related therapy associated with all-cause dementia in a primary care population? J. Alzheimers Dis. 2015, 46, 1039–1047. [Google Scholar] [CrossRef]
- Villumsen, M.; Aznar, S.; Pakkenberg, B.; Jess, T.; Brudek, T. Inflammatory bowel disease increases the risk of Parkinson’s disease: A Danish nationwide cohort study 1977–2014. Gut 2018, 68, 18–24. [Google Scholar] [CrossRef]
- Weimers, P.; Halfvarson, J.; Sachs, M.C.; Saunders-Pullman, R.; Ludvigsson, J.F.; Peter, I.; Burisch, J.; Olén, O. Inflammatory Bowel disease and Parkinson’s disease: A Nationwide Swedish cohort study. Inflamm. Bowel Dis. 2018, 25, 111–123. [Google Scholar] [CrossRef] [PubMed]
- Park, S.; Kim, J.; Chun, J.; Han, K.; Soh, H.; Kang, E.A.; Lee, H.J.; Im, J.P.; Kim, J.S. Patients with inflammatory Bowel disease are at an increased risk of Parkinson’s disease: A South Korean Nationwide population-based study. J. Clin. Med. 2019, 8, 1191. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sutton, S.S.; Magagnoli, J.; Cummings, T.; Hardin, J.W. Association between thiopurine medication exposure and Alzheimer’s disease among a cohort of patients with inflammatory bowel disease. Alzheimers Dement. 2019, 5, 809–813. [Google Scholar] [CrossRef] [PubMed]
- Prigent, A.; Chapelet, G.; de Guilhem de Lataillade, A.; Oullier, T.; Durieu, E.; Bourreille, A.; Duchalais, E.; Hardonnière, K.; Neunlist, M.; Noble, W.; et al. Tau accumulates in Crohn’s disease gut. FASEB J. 2020, 34, 9285–9296. [Google Scholar] [CrossRef]
- Zhang, B.; Wang, H.E.; Bai, Y.M.; Tsai, S.J.; Su, T.P.; Chen, T.J.; Wang, Y.-P.; Chen, M.-H. Inflammatory bowel disease is associated with higher dementia risk: A nationwide longitudinal study. Gut 2020, 70, 85–91. [Google Scholar] [CrossRef]
- Zhou, M.; Xu, R.; Kaelber, D.C.; Gurney, M.E. Tumor Necrosis Factor (TNF) blocking agents are associated with lower risk for Alzheimer’s disease in patients with rheumatoid arthritis and psoriasis. PLoS ONE 2020, 3, e0229819. [Google Scholar] [CrossRef] [Green Version]
- Zhang, M.N.; Shi, Y.D.; Jiang, H.Y. The risk of dementia in patients with inflammatory bowel disease: A systematic review and meta-analysis. Int. J. Colorectal Dis. 2022, 37, 769–775. [Google Scholar] [CrossRef]
- Mansson, R.; Joffe, M.M.; Sun, W.; Hennessy, S. On the estimation and use of propensity scores in case-control and case-cohort studies. Am. J. Epidemiol. 2007, 166, 332–339. [Google Scholar] [CrossRef] [Green Version]
- Kinney, J.W.; Bemiller, S.M.; Murtishaw, A.S.; Leisgang, A.M.; Lamb, B.T. Inflammation as a central mechanism in Alzheimer’s disease. Alzheimers Dement. 2018, 4, 575–590. [Google Scholar] [CrossRef]
- Pan, W.; Kastin, A.J. TNFalpha transport across the blood-brain barrier is abolished in receptor knockout mice. Exp. Neurol. 2002, 174, 193–200. [Google Scholar] [CrossRef]
- Leylabadlo, H.E.; Ghotaslou, R.; Feizabadi, M.M.; Farajnia, S.; Moaddab, S.Y.; Ganbarov, K.; Khodadadi, E.; Tanomand, A.; Sheykhsaran, E.; Yousefi, B.; et al. The critical role of Faecalibacterium prausnitzii in human health: An overview. Microb. Pathog. 2020, 149, 104344. [Google Scholar] [CrossRef] [PubMed]
- Cattaneo, A.; Cattane, N.; Galluzzi, S.; Provasi, S.; Lopizzo, N.; Festari, C.; Ferrari, C.; Guerra, U.P.; Paghera, B.; Muscio, C.; et al. Association of brain amyloidosis with pro-inflammatory gut bacterial taxa and peripheral inflammation markers in cognitively impaired elderly. Neurobiol. Aging 2017, 49, 60–68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, H.; Chen, Y.; Wang, Z.; Xie, G.; Liu, M.; Yuan, B.; Chai, H.; Wang, W.; Cheng, P. Implications of gut microbiota in neurodegenerative diseases. Front. Immunol. 2022, 13, 785644. [Google Scholar] [CrossRef] [PubMed]
- Romano, S.; Savva, G.M.; Bedarf, J.R.; Charles, I.G.; Hildebrand, F.; Narbad, A. Meta-analysis of the Parkinson’s disease gut microbiome suggests alterations linked to intestinal inflammation. NPJ Parkinsons Dis. 2021, 7, 27. [Google Scholar] [CrossRef]
- Braniste, V.; Al-Asmakh, M.; Kowal, C.; Anuar, F.; Abbaspour, A.; Tóth, M.; Korecka, A.; Bakocevic, N.; Ng, L.G.; Kundu, P.; et al. The gut microbiota influences blood-brain barrier permeability in mice. Sci. Transl. Med. 2014, 6, 263ra158. [Google Scholar] [CrossRef] [Green Version]
- Jiang, C.; Li, G.; Huang, P.; Liu, Z.; Zhao, B. The gut microbiota and Alzheimer’s disease. J. Alzheimers Dis. 2017, 58, 1–15. [Google Scholar] [CrossRef]
- Zhou, Y.; Smith, D.; Leong, B.J.; Brännström, K.; Almqvist, F.; Chapman, M.R. Promiscuous cross-seeding between bacterial amyloids promotes interspecies biofilms. J. Biol. Chem. 2012, 287, 35092–35103. [Google Scholar] [CrossRef] [Green Version]
- Friedland, R.P. Mechanisms of molecular mimicry involving the microbiota in neurodegeneration. J. Alzheimers Dis. 2015, 45, 349–362. [Google Scholar] [CrossRef] [Green Version]
- Brierley, S.M.; Linden, D.R. Neuroplasticity and dysfunction after gastrointestinal inflammation. Nat. Rev. Gastroenterol. Hepatol. 2014, 11, 611–627. [Google Scholar] [CrossRef]
- Lionnet, A.; Wade, M.A.; Corbillé, A.G.; Prigent, A.; Paillusson, S.; Tasselli, M.; Gonzales, J.; Durieu, E.; Rolli-Derkinderen, M.; Coron, E.; et al. Characterisation of tau in the human and rodent enteric nervous system under physiological conditions and in tauopathy. Acta Neuropathol. Commun. 2018, 6, 65. [Google Scholar] [CrossRef]
- Dugger, B.N.; Hoffman, B.R.; Scroggins, A.; Serrano, G.E.; Adler, C.H.; Shill, H.A.; Belden, C.M.; Sabbagh, M.N.; Caviness, J.N.; Dunckley, E.D.; et al. Tau immunoreactivity in peripheral tissues of human aging and select tauopathies. Neurosci. Lett. 2019, 696, 132–139. [Google Scholar] [CrossRef]
- Prigent, A.; Lionnet, A.; Durieu, E.; Chapelet, G.; Bourreille, A.; Neunlist, M.; Rolli-Derkinderen, M.; Derkinderen, P. Enteric alpha-synuclein expression is increased in Crohn’s disease. Acta Neuropathol. 2019, 137, 359–361. [Google Scholar] [CrossRef] [PubMed]
- Fenyi, A.; Leclair-Visonneau, L.; Clairembault, T.; Coron, E.; Neunlist, M.; Melki, R.; Derkinderen, P.; Bousset, L. Detection of alpha-synuclein aggregates in gastrointestinal biopsies by protein misfolding cyclic amplification. Neurobiol. Dis. 2019, 129, 38–43. [Google Scholar] [CrossRef] [PubMed]
- Kim, G.H.; Lee, Y.C.; Kim, T.J.; Kim, E.R.; Hong, S.N.; Chang, D.K.; Kim, Y.-H. Risk of neurodegenerative diseases in patients with inflammatory Bowel disease: A nationwide population-based cohort study. J. Crohn’s Colitis 2022, 16, 436–443. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Study Design | Country, Year | Study Period | AD, PD Cases among Study Participants | Newcastle-Ottawa Scale |
|---|---|---|---|---|---|
| Dregan A. et al. [30] | cohort study | UK, 2015 | 2002–2013 | 47 AD/7705 CD 93 AD/12,335 UC 266 AD/308,843 non-IBD | Selection: 4 Comparability: 2 Outcome/Exposure: 2 |
| Villumsen M. et al. [31] | cohort study | Denmark, 2018 | 1977–2014 | 335 PD/76,477 IBD 39,784 PD/7,548,259 non-IBD | Selection: 4 Comparability: 1 Outcome/Exposure: 3 |
| Weimers P. et al. [32] | cohort study | Sweden, 2018 | 2002–2014 | 23 PD/11,418 CD 69 PD/24,442 UC 103 PD/39,652 IBD 839 PD/396,520 non-IBD | Selection: 4 Comparability: 2 Outcome/Exposure: 3 |
| Park S. et al. [33] | cohort study | Korea, 2019 | 2010–2013 | 92 PD/38,861 IBD 15 PD/12,631 CD 77 PD/26,230 UC 134 PD/116,583 non-IBD 19 PD/37,893 non-CD 115 PD/78,690 non-UC | Selection: 4 Comparability: 2 Outcome/Exposure: 3 |
| Sutton S. et al. [34] | cohort study | USA, 2019 | 2010–2018 | 523 AD/24,057 IBD 1166 AD/42,255 non-IBD | Selection: 4 Comparability: 2 Outcome/Exposure: 2 |
| Prigent A. et al. [35] | cross-sectional study | France, 2020 | na | 12 AD/16 CD 2 AD/16 non-CD | Selection: 2 Comparability: 1 Outcome/Exposure: 2 |
| Zhang B. et al. [36] | cohort study | Taiwan, 2020 | 1995–2010 | 33 AD/1742 IBD 11 AD/584 CD 22 AD/1158 UC 32 AD/17,420 non-IBD 14 AD/5840 non-CD 18 AD/11,580 non-UC | Selection: 4 Comparability: 2 Outcome/Exposure: 3 |
| Zhou M. et al. [37] | case-control study | USA, 2020 | na | 4440 AD/279,040 IBD 6160 AD/201,870 CD 2650 AD/168,870 UC 338,400 AD/55,954,070 non-IBD | Selection: 4 Comparability: 1 Outcome/Exposure: 3 |
| Comparison | Egger’s Test (C.I.l.–C.I.u.) | p-Value |
|---|---|---|
| AD + PD vs. IBD | −16.88–27.89 | 0.49 |
| AD + PD vs. CD | −5.57–5.81 | 0.96 |
| AD + PD vs. UC | −17.66–11.64 | 0.56 |
| AD vs. IBD | −205.36–218.23 | 0.77 |
| AD vs. CD | −8.88–4.18 | 0.34 |
| AD vs. UC | −70.47–51.63 | 0.30 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Szandruk-Bender, M.; Wiatrak, B.; Szeląg, A. The Risk of Developing Alzheimer’s Disease and Parkinson’s Disease in Patients with Inflammatory Bowel Disease: A Meta-Analysis. J. Clin. Med. 2022, 11, 3704. https://doi.org/10.3390/jcm11133704
Szandruk-Bender M, Wiatrak B, Szeląg A. The Risk of Developing Alzheimer’s Disease and Parkinson’s Disease in Patients with Inflammatory Bowel Disease: A Meta-Analysis. Journal of Clinical Medicine. 2022; 11(13):3704. https://doi.org/10.3390/jcm11133704
Chicago/Turabian StyleSzandruk-Bender, Marta, Benita Wiatrak, and Adam Szeląg. 2022. "The Risk of Developing Alzheimer’s Disease and Parkinson’s Disease in Patients with Inflammatory Bowel Disease: A Meta-Analysis" Journal of Clinical Medicine 11, no. 13: 3704. https://doi.org/10.3390/jcm11133704