
Accuracy of Catheter Positioning during Left Subclavian Venous Access: A Randomized Comparison between Radiological and Topographical Landmarks

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design, Ethics Statement and Study Population
2.2. Randomization and Allocation
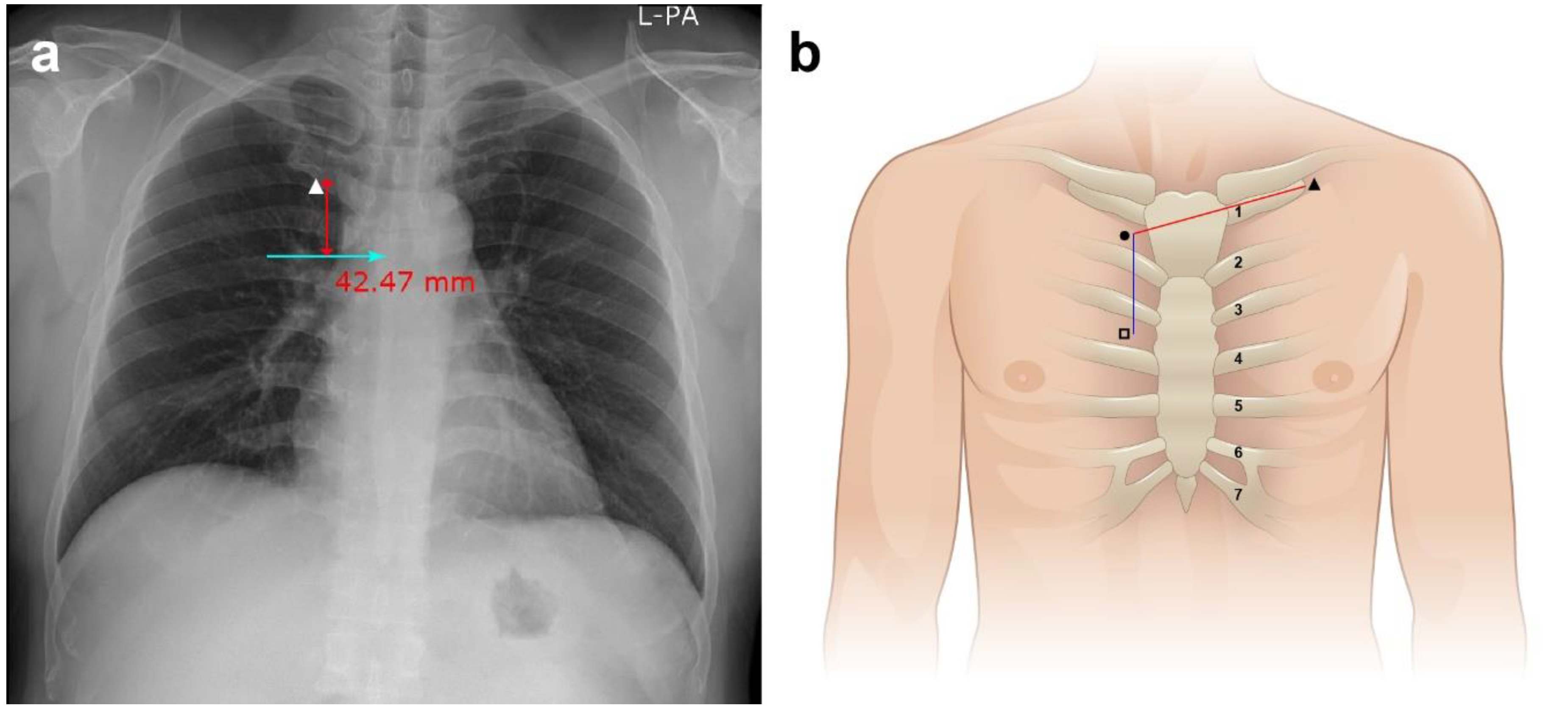
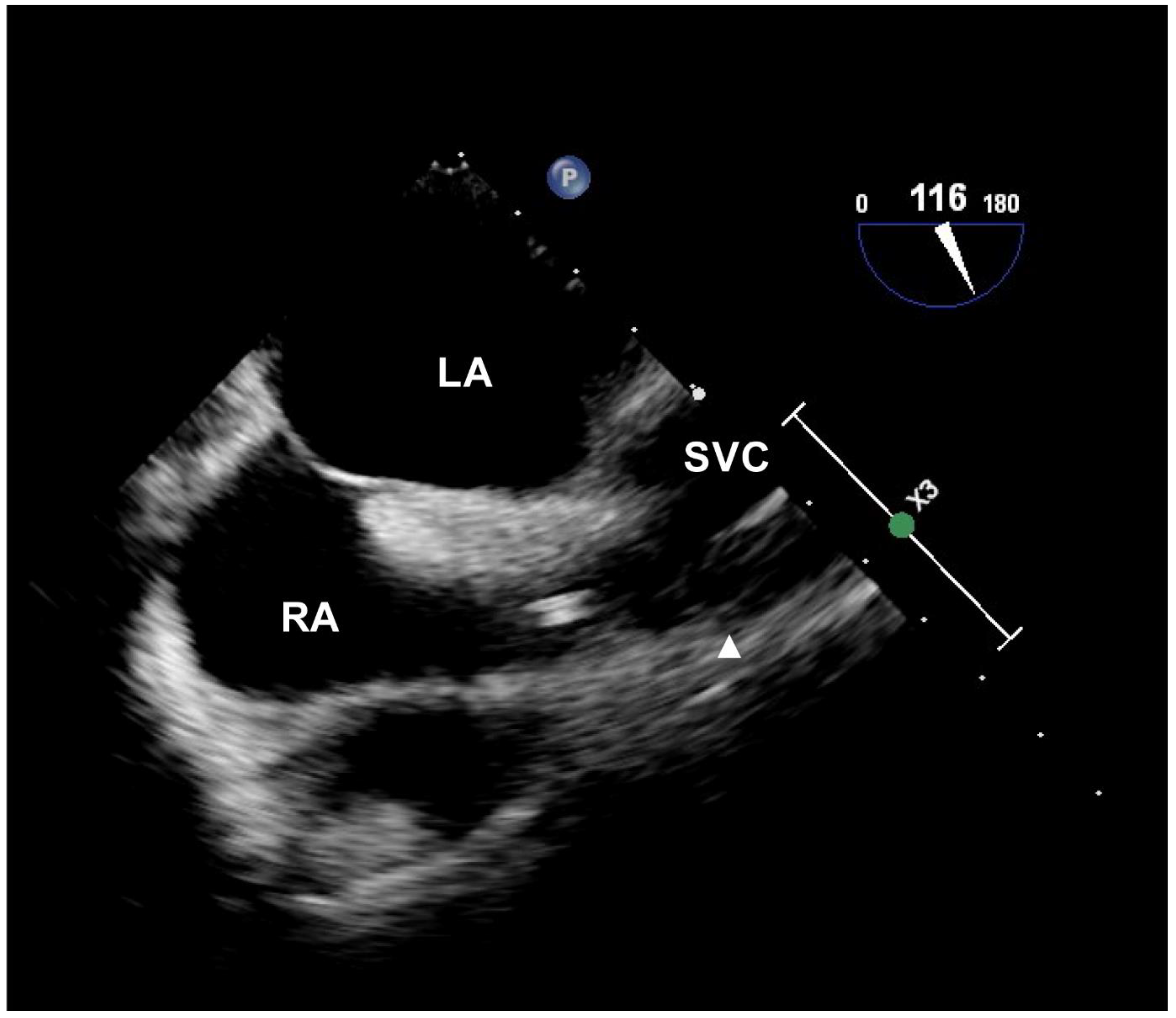
2.3. Procedure and Data Collection
2.4. Statistical Analysis
2.4.1. Sample Size Calculation
2.4.2. Data Analysis
3. Results
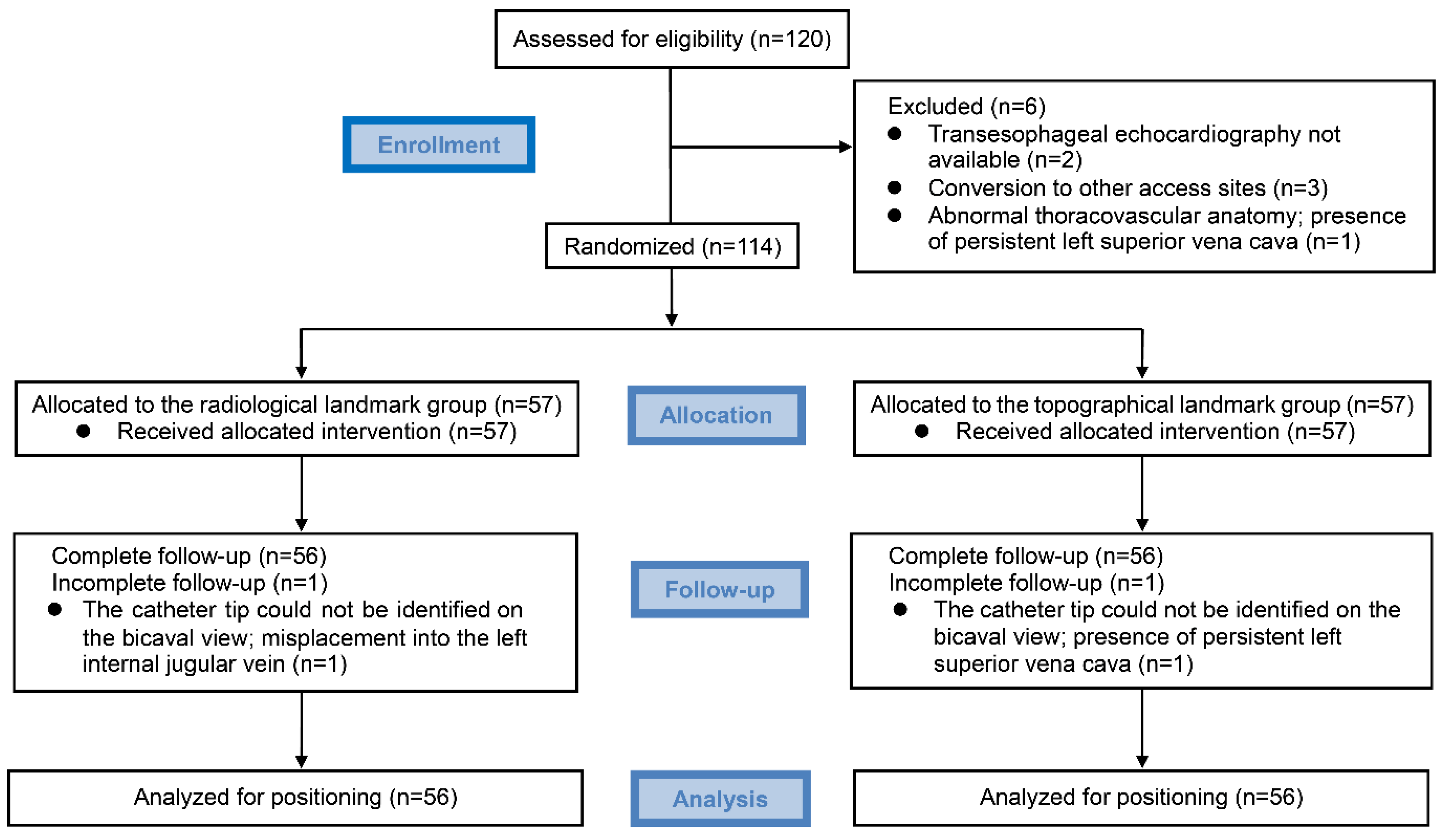
3.1. Participant Enrollment
3.2. Characteristics of the Participants and Measurements
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fletcher, S.J.; Bodenham, A.R. Safe placement of central venous catheters: Where should the tip of the catheter lie? Br. J. Anaesth. 2000, 85, 188–191. [Google Scholar] [CrossRef] [Green Version]
- Vesely, T.M. Central venous catheter tip position: A continuing controversy. J. Vasc. Interv. Radiol. 2003, 14, 527–534. [Google Scholar] [CrossRef] [PubMed]
- Shamir, M.Y.; Bruce, L.J. Central venous catheter-induced cardiac tamponade: A preventable complication. Anesth. Analg. 2011, 112, 1280–1282. [Google Scholar] [CrossRef] [PubMed]
- Cadman, A.; Lawrance, J.A.; Fitzsimmons, L.; Spencer-Shaw, A.; Swindell, R. To clot or not to clot? That is the question in central venous catheters. Clin. Radiol. 2004, 59, 349–355. [Google Scholar] [CrossRef]
- Ballard, D.H.; Samra, N.S.; Gifford, K.M.; Roller, R.; Wolfe, B.M.; Owings, J.T. Distance of the internal central venous catheter tip from the right atrium is positively correlated with central venous thrombosis. Emerg. Radiol. 2016, 23, 269–273. [Google Scholar] [CrossRef]
- Gravenstein, N.; Blackshear, R.H. In vitro evaluation of relative perforating potential of central venous catheters: Comparison of materials, selected models, number of lumens, and angles of incidence to simulated membrane. J. Clin. Monit. 1991, 7, 1–6. [Google Scholar] [CrossRef]
- Stonelake, P.A.; Bodenham, A.R. The carina as a radiological landmark for central venous catheter tip position. Br. J. Anaesth. 2006, 96, 335–340. [Google Scholar] [CrossRef] [Green Version]
- Ahn, J.H.; Kim, I.S.; Yang, J.H.; Lee, I.G.; Seo, D.H.; Kim, S.P. Transoesophageal echocardiographic evaluation of central venous catheter positioning using Peres’ formula or a radiological landmark-based approach: A prospective randomized single-centre study. Br. J. Anaesth. 2017, 118, 215–222. [Google Scholar] [CrossRef] [Green Version]
- Pittiruti, M.; Lamperti, M. Late cardiac tamponade in adults secondary to tip position in the right atrium: An urban legend? A systematic review of the literature. J. Cardiothorac. Vasc. Anesth. 2015, 29, 491–495. [Google Scholar] [CrossRef]
- Shen, X.H.; Su, B.Y.; Liu, J.J.; Zhang, G.M.; Xue, H.D.; Jin, Z.Y.; Mirjalili, S.A.; Ma, C. A reappraisal of adult thoracic and abdominal surface anatomy via CT scan in Chinese population. Clin. Anat. 2016, 29, 165–174. [Google Scholar] [CrossRef]
- Pak, N.; Patel, S.G.; Hashemi Taheri, A.P.; Hashemi, F.; Eftekhari Vaghefi, R.; Naybandi Atashi, S.; Mirjalili, S.A. A reappraisal of adult thoracic and abdominal surface anatomy in Iranians in vivo using computed tomography. Clin. Anat. 2016, 29, 191–196. [Google Scholar] [CrossRef] [PubMed]
- Carrier, G.; Fréchette, E.; Ugalde, P.; Deslauriers, J. Correlative anatomy for the sternum and ribs, costovertebral angle, chest wall muscles and intercostal spaces, thoracic outlet. Thorac. Surg. Clin. 2007, 17, 521–528. [Google Scholar] [CrossRef]
- Andropoulos, D.B.; Stayer, S.A.; Bent, S.T.; Campos, C.J.; Bezold, L.I.; Alvarez, M.; Fraser, C.D. A controlled study of transesophageal echocardiography to guide central venous catheter placement in congenital heart surgery patients. Anesth. Analg. 1999, 89, 65–70. [Google Scholar] [CrossRef] [PubMed]
- Schuster, M.; Nave, H.; Piepenbrock, S.; Pabst, R.; Panning, B. The carina as a landmark in central venous catheter placement. Br. J. Anaesth. 2000, 85, 192–194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ryu, H.G.; Bahk, J.H.; Kim, J.T.; Lee, J.H. Bedside prediction of the central venous catheter insertion depth. Br. J. Anaesth. 2007, 98, 225–227. [Google Scholar] [CrossRef] [Green Version]
- Schummer, W.; Herrmann, S.; Schummer, C.; Funke, F.; Steenbeck, J.; Fuchs, J.; Uhlig, T.; Reinhart, K. Intra-atrial ECG is not a reliable method for positioning left internal jugular vein catheters. Br. J. Anaesth. 2003, 91, 481–486. [Google Scholar] [CrossRef] [Green Version]
- Kim, M.C.; Kim, K.S.; Choi, Y.K.; Kim, D.S.; Kwon, M.I.; Sung, J.K.; Moon, J.Y.; Kang, J.M. An estimation of right- and left-sided central venous catheter insertion depth using measurement of surface landmarks along the course of central veins. Anesth. Analg. 2011, 112, 1371–1374. [Google Scholar] [CrossRef]
- Aslamy, Z.; Dewald, C.L.; Heffner, J.E. MRI of central venous anatomy: Implications for central venous catheter insertion. Chest 1998, 114, 820–826. [Google Scholar] [CrossRef]
- Mahlon, M.A.; Yoon, H.C. CT angiography of the superior vena cava: Normative values and implications for central venous catheter position. J. Vasc. Interv. Radiol. 2007, 18, 1106–1110. [Google Scholar] [CrossRef]
- Ezri, T.; Weisenberg, M.; Sessler, D.I.; Berkenstadt, H.; Elias, S.; Szmuk, P.; Serour, F.; Evron, S. Correct depth of insertion of right internal jugular central venous catheters based on external landmarks: Avoiding the right atrium. J. Cardiothorac. Vasc. Anesth. 2007, 21, 497–501. [Google Scholar] [CrossRef] [Green Version]
- Kim, K.O.; Jo, J.O.; Kim, H.S.; Kim, C.S. Positioning internal jugular venous catheters using the right third intercostal space in children. Acta Anaesthesiol. Scand. 2003, 47, 1284–1286. [Google Scholar] [CrossRef] [PubMed]
- Hsu, J.H.; Wang, S.S.; Lu, D.V.; Cheng, K.I.; Wang, C.K.; Wu, J.R. Optimal skin surface landmark for the SVC-RA junction in cancer patients requiring the implantation of permanent central venous catheters. Anaesthesia 2007, 62, 818–823. [Google Scholar] [CrossRef] [PubMed]
- Mirjalili, S.A.; Hale, S.J.; Buckenham, T.; Wilson, B.; Stringer, M.D. A reappraisal of adult thoracic surface anatomy. Clin. Anat. 2012, 25, 827–834. [Google Scholar] [CrossRef] [PubMed]
- Tarbiat, M.; Manafi, B.; Davoudi, M.; Totonchi, Z. Comparison of the complications between left side and right side subclavian vein catheter placement in patients undergoing coronary artery bypass graft surgery. J. Cardiovasc. Thorac. Res. 2014, 6, 147–151. [Google Scholar] [CrossRef] [Green Version]
- Rossi, U.G.; Rigamonti, P.; Torcia, P.; Mauri, G.; Brunini, F.; Rossi, M.; Gallieni, M.; Cariati, M. Congenital anomalies of superior vena cava and their implications in central venous catheterization. J. Vasc. Access. 2015, 16, 265–268. [Google Scholar] [CrossRef]
- Lee, M.S.; Pande, R.L.; Rao, B.; Landzberg, M.J.; Kwong, R.Y. Cerebral abscess due to persistent left superior vena cava draining into the left atrium. Circulation 2011, 124, 2362–2364. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Radiological Group (n = 56) | Topographical Group (n = 56) | p |
|---|---|---|---|
| Male sex | 36 (64.3) | 39 (69.6) | 0.547 |
| Age (years) | 65.0 [58.0–71.8] | 67.0 [59.3–75.0] | 0.230 |
| Height (cm) | 163.0 [153.3–166.0] | 164.0 [158.0–169.0] | 0.079 |
| Weight (kg) | 64.0 [55.0–71.8] | 63.0 [56.0–69.8] | 0.818 |
| BMI (kg/m2) | 24.3 [21.9–26.5] | 23.6 [21.7–26.2] | 0.317 |
| Variable | Radiological Group (n = 56) | Topographical Group (n = 56) | p |
|---|---|---|---|
| Catheter insertion depth (cm) | 19.5 [18.6–20.4] | 19.8 [18.8–20.2] | 0.645 |
| Actual distance to junction (cm) | 20.5 [19.6–21.0] | 20.4 [19.5–21.0] | 0.802 |
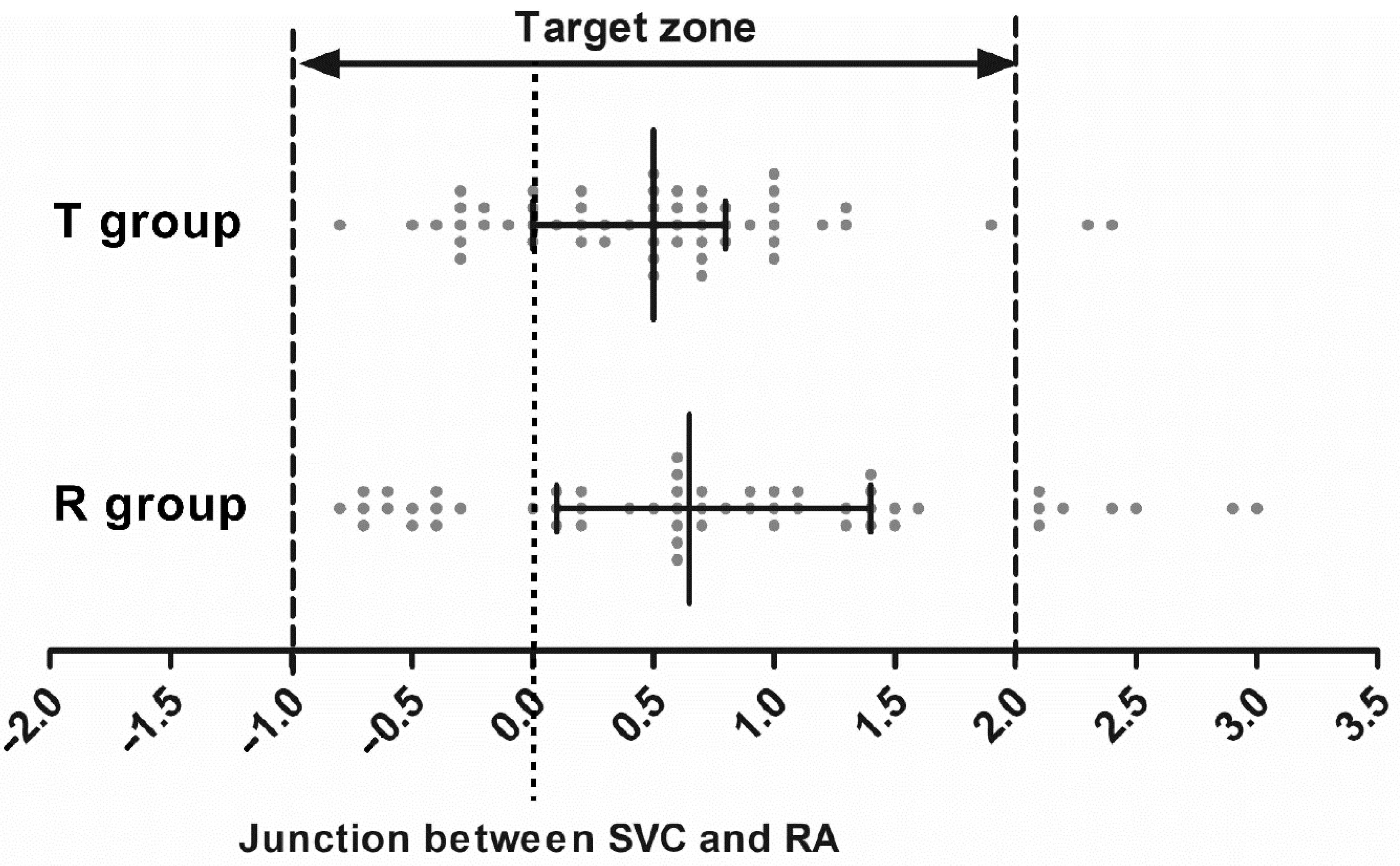
| Difference between measurements (cm) | 0.7 [0.1–1.4] | 0.5 [0–0.8] | 0.171 |
| Acceptable positioning | 48 (85.7) | 54 (96.4) | 0.047 * |
| Position above target zone | 8 (14.3) | 2 (3.6) | 0.047 * |
| Position below target zone | 0 | 0 | |
| Angle of tip (>40°) to the SVC | 0 | 0 | |
| Abutment with the SVC | 1 (1.8) | 0 | 0.315 |
| Flow streams hitting vascular wall | 1 (1.8) | 1 (1.8) | 1.000 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, S.K.; Ahn, J.H.; Lee, Y.K.; Hwang, B.Y.; Lee, M.K.; Kim, I.S. Accuracy of Catheter Positioning during Left Subclavian Venous Access: A Randomized Comparison between Radiological and Topographical Landmarks. J. Clin. Med. 2022, 11, 3692. https://doi.org/10.3390/jcm11133692
Kim SK, Ahn JH, Lee YK, Hwang BY, Lee MK, Kim IS. Accuracy of Catheter Positioning during Left Subclavian Venous Access: A Randomized Comparison between Radiological and Topographical Landmarks. Journal of Clinical Medicine. 2022; 11(13):3692. https://doi.org/10.3390/jcm11133692
Chicago/Turabian StyleKim, Sun Key, Jung Hwan Ahn, Yoon Kyung Lee, Bo Young Hwang, Min Kyung Lee, and Il Seok Kim. 2022. "Accuracy of Catheter Positioning during Left Subclavian Venous Access: A Randomized Comparison between Radiological and Topographical Landmarks" Journal of Clinical Medicine 11, no. 13: 3692. https://doi.org/10.3390/jcm11133692