
Admission Severity of Atrial-Fibrillation-Related Acute Ischemic Stroke in Patients under Anticoagulation Treatment: A Systematic Review and Meta-Analysis





 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Literature Research
2.2. Data Extraction
2.3. Study Selection and Quality Assessment
2.4. Statistical Analysis
3. Results
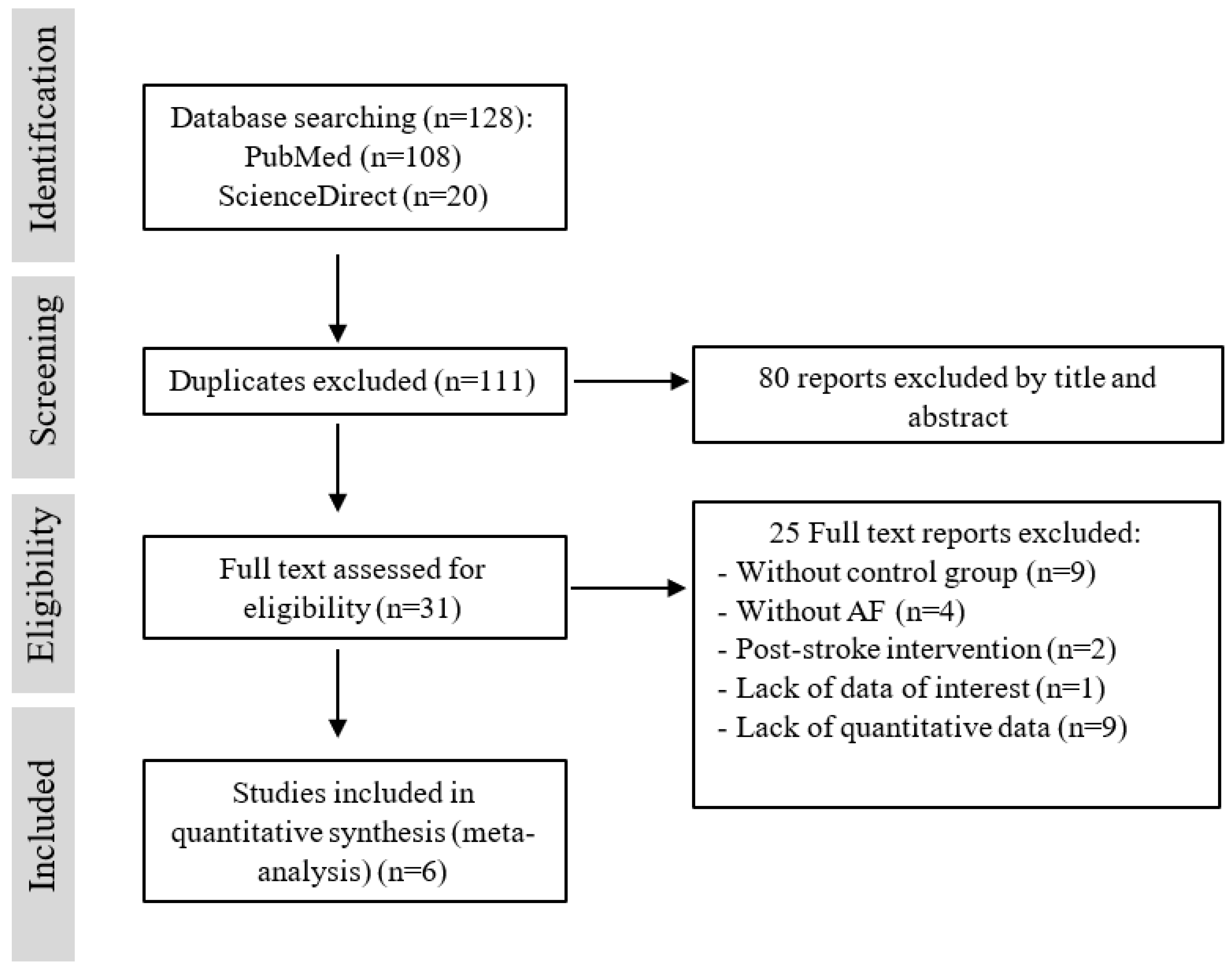
3.1. Study Selection
3.2. Study Characteristics
3.3. Quality Assessment
3.4. General Sociodemographic and Risk Factors
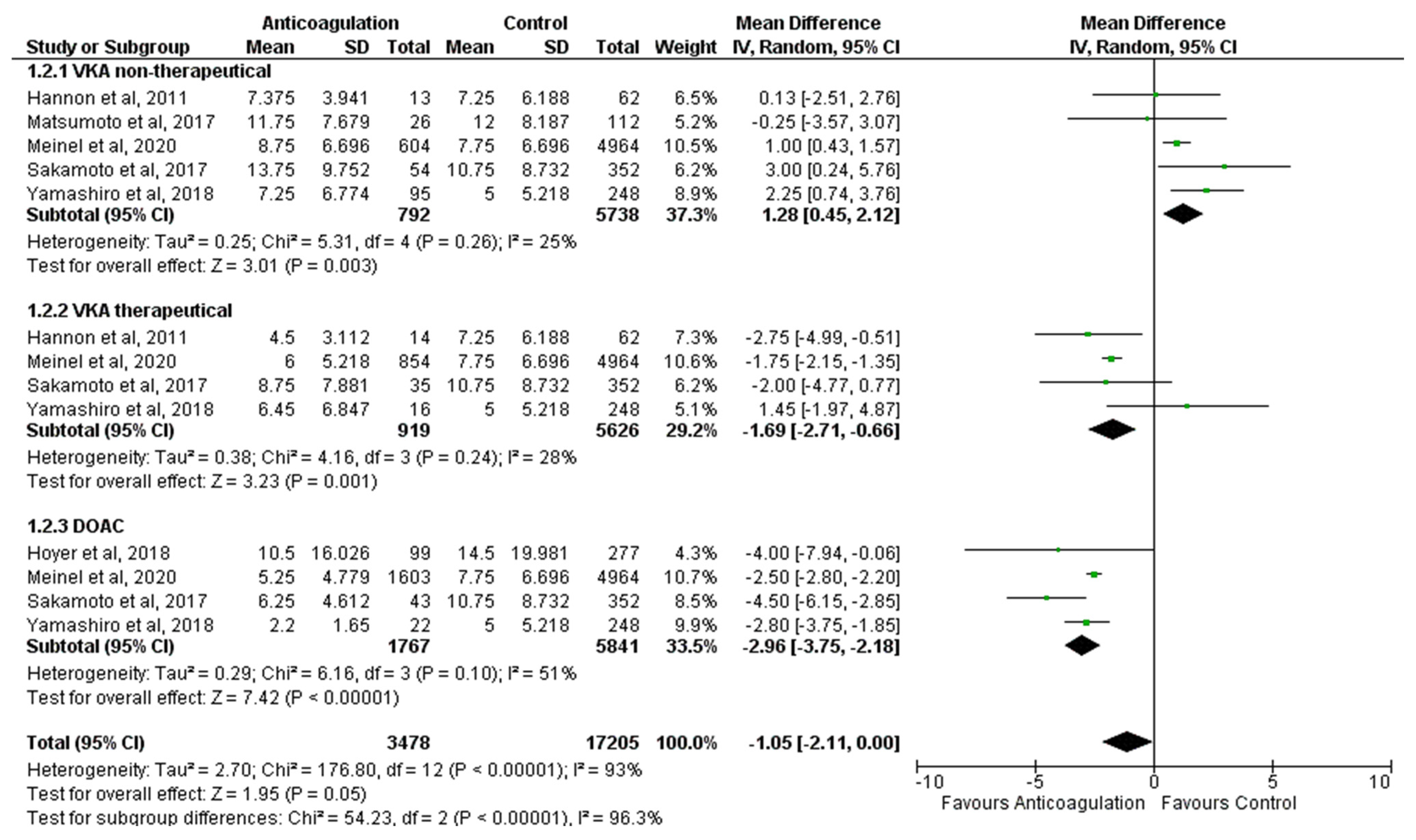
3.5. Stroke Severity
3.6. VKA Non-Therapeutical
3.7. VKA Therapeutical
3.8. DOAC
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| A | B | C | D | Risk of Bias | |||
|---|---|---|---|---|---|---|---|
| Meinel et al., 2020 [13] | Low | A | Confounding bias | ||||
| Sakamoto et al., 2017 [27] | Moderate | B | Selection bias | ||||
| Yamashiro et al., 2018 [28] | Low | C | Information bias | ||||
| Hoyer et al., 2018 [12] | Low | D | Reporting bias | ||||
| Hannon et al., 2011 [29] | Low | ||||||
| Matsumoto et al., 2017 [30] | Low | Low | |||||
| Some concerns | |||||||
| High |
References
- Yi, X.; Lin, J.; Han, Z.; Luo, H.; Shao, M.; Fan, D.; Qiang, Z. Preceding Antithrombotic Treatment is Associated With Acute Ischemic Stroke Severity and Functional Outcome at 90 Days Among Patients With Atrial Fibrillation. J. Stroke Cerebrovasc. Dis. 2019, 28, 2003–2010. [Google Scholar] [CrossRef] [PubMed]
- Jung, Y.H.; Choi, H.Y.; Lee, K.Y.; Cheon, K.; Han, S.W.; Park, J.H.; Cho, H.J.; Park, H.J.; Nam, H.S.; Heo, J.H.; et al. Stroke Severity in Patients on Non-Vitamin K Antagonist Oral Anticoagulants with a Standard or Insufficient Dose. Thromb. Haemost. 2018, 118, 2145–2151. [Google Scholar] [CrossRef]
- Hellwig, S.; Grittner, U.; Audebert, H.; Endres, M.; Haeusler, K.G. Non-Vitamin K-dependent oral anticoagulants have a positive impact on ischaemic stroke severity in patients with atrial fibrillation. EP Europace 2018, 20, 569–574. [Google Scholar] [CrossRef] [PubMed]
- January, C.T.; Wann, L.S.; Calkins, H.; Chen, L.Y.; Cigarroa, J.E.; Cleveland, J.C.; Ellinor, P.T.; Ezekowitz, M.D.; Field, M.E.; Furie, K.L.; et al. 2019 AHA/ACC/HRS Focused Update of the 2014 AHA/ACC/HRS Guideline for the Management of Patients With Atrial Fibrillation: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. Circulation 2019, 140, e125–e151. [Google Scholar] [CrossRef] [PubMed]
- Boursier-Bossy, V.; Zuber, M.; Emmerich, J. Ischemic stroke and non-valvular atrial fibrillation: When to introduce anticoagulant therapy? J. Med. Vasc. 2020, 45, 72–80. [Google Scholar] [CrossRef] [PubMed]
- Wolf, P.A.; Abbott, R.D.; Kannel, W.B. Atrial fibrillation as an independent risk factor for stroke: The framingham study. Stroke 1991, 22, 983–988. [Google Scholar] [CrossRef] [Green Version]
- Lip, G.Y.; Lane, D.A. Stroke prevention in atrial fibrillation: A systematic review. JAMA J. Am. Med. Assoc. 2015, 313, 1950–1962. [Google Scholar] [CrossRef]
- Wodchis, W.P.; Bhatia, R.S.; Leblanc, K.; Meshkat, N.; Morra, D. A review of the cost of atrial fibrillation. Value Health 2012, 15, 240–248. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tziomalos, K.; Giampatzis, V.; Bouziana, S.D.; Spanou, M.; Kostaki, S.; Papadopoulou, M.; Dourliou, V.; Sofogianni, A.; Savopoulos, C.; Hatzitolios, A.I. Adequacy of preadmission oral anticoagulation with vitamin K antagonists and ischemic stroke severity and outcome in patients with atrial fibrillation. J. Thromb. Thrombolysis 2015, 41, 336–342. [Google Scholar] [CrossRef] [PubMed]
- Tavares, S.F.; Ferreira, I.; Chaves, V.; Flores, L.; Correia, C.; Almeida, J.; Fonseca, L.; Chaves, P.C. Acute Ischemic Stroke Outcome and Preceding Anticoagulation: Direct Oral Anticoagulants Versus Vitamin K Antagonists. J. Stroke Cerebrovasc. Dis. 2020, 29, 104691. [Google Scholar] [CrossRef] [PubMed]
- Fernandes, L.; Sargento-Freitas, J.; Milner, J.; Silva, A.; Novo, A.; Gonçalves, T.; Marinho, A.V.; Pego, G.M.; Cunha, L.; António, N. Ischemic stroke in patients previously anticoagulated for non-valvular atrial fibrillation: Why does it happen? Rev. Port. Cardiol. 2019, 38, 117–124. [Google Scholar] [CrossRef] [PubMed]
- Hoyer, C.; Filipov, A.; Neumaier-Probst, E.; Szabo, K.; Ebert, A.; Alonso, A. Impact of pre-admission treatment with non-vitamin K oral anticoagulants on stroke severity in patients with acute ischemic stroke. J. Thromb. Thrombolysis 2018, 45, 529–535. [Google Scholar] [CrossRef] [PubMed]
- Meinel, T.R.; Branca, M.; Marchis, G.M.; Nedeltchev, K.; Kahles, T.; Bonati, L.; Arnold, M.; Heldner, M.R.; Jung, S.; Carrera, E.; et al. Prior Anticoagulation in Patients with Ischemic Stroke and Atrial Fibrillation. Ann. Neurol. 2021, 89, 42–53. [Google Scholar] [CrossRef] [PubMed]
- Seiffge, D.J.; Marchis, G.D.; Koga, M.; Paciaroni, M.; Wilson, D.; Capellari, M.; Md, K.M.; Tsivgoulis, G.; Ambler, G.; Arihiro, S.; et al. Ischemic stroke despite oral anticoagulant therapy in patients with atrial fibrillation. Ann. Neurol. 2020, 87, 677–687. [Google Scholar] [CrossRef] [Green Version]
- Xian, Y.; O’Brien, E.C.; Liang, L.; Xu, H.; Schwamm, L.; Fonarow, G.; Bhatt, D.L.; Smith, E.E.; Olson, D.M.; Maisch, L.; et al. Association of preceding antithrombotic treatment with acute ischemic stroke severity and in-hospital outcomes among patients with atrial fibrillation. JAMA J. Am. Med. Assoc. 2017, 317, 1057–1067. [Google Scholar] [CrossRef] [PubMed]
- Jame, S.; Barnes, G. Stroke and thromboembolism prevention in atrial fibrillation. Heart 2020, 106, 10–17. [Google Scholar] [CrossRef]
- Aguilar, M.I.; Hart, R.; Pearce, L.A. Oral anticoagulants versus antiplatelet therapy for preventing stroke in patients with non-valvular atrial fibrillation and no history of stroke or transient ischemic attacks (Review). Cochrane Database Syst. Rev. 2007, 3, CD006186. [Google Scholar] [CrossRef]
- Hindricks, G.; Potpara, T.; Dagres, N.; Arbelo, E.; Bax, J.; Blomström-Lundqvist, C.; Boriani, G.; Castella, M.; Dan, G.A.; Dilaveris, P.E.; et al. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS). Eur. Heart J. 2021, 42, 373–498. [Google Scholar] [CrossRef]
- Adachi, T.; Hoshino, H.; Takagi, M.; Fujioka, S. Volume and Characteristics of Intracerebral Hemorrhage with Direct Oral Anticoagulants in Comparison with Warfarin. Cerebrovasc. Dis. Extra. 2017, 7, 62–71. [Google Scholar] [CrossRef] [Green Version]
- Bakhai, A.; Petri, H.; Vahidnia, F.; Wolf, C.; Ding, Y.; Foskett, N.; Sculpher, M. Real-world data on the incidence, mortality, and cost of ischaemic stroke and major bleeding events among non-valvular atrial fibrillation patients in England. J. Eval. Clin. Pract. 2021, 27, 119–133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shamseer, L.; Moher, D.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred reporting items for systematic review and meta-analysis protocols (prisma-p) 2015: Elaboration and explanation. Br. Med. J. 2015, 349, g7647. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Donato, H.; Donato, M. Stages for undertaking a systematic review. Acta Médica Portuguesa. 2019, 32, 227–235. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V. Cochrane Handbook for Systematic Reviews of Interventions Version 6.2. Available online: www.training.cochrane.org/handbook (accessed on 6 May 2021).
- Hozo, S.P.; Djulbegovic, B.; Hozo, I. Estimating the mean and variance from the median, range, and the size of a sample. BMC Med. Res. Methodol. 2005, 5, 13. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.T.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef] [PubMed]
- Sousa-Pinto, B.; Azevedo, L. Avaliação Crítica de uma Revisão Sistemática e Meta-Análise: Da Execução da Meta-análise à Exploração da Heterogeneidade. Rev. Soc. Port. Anestesiol. 2019, 28, 187–191. [Google Scholar] [CrossRef]
- Sakamoto, Y.; Okubo, S.; Nito, C.; Suda, S.; Matsumoto, N.; Abe, A.; Aoki, J.; Shimoyama, T.; Takayama, Y.; Suzuki, K.; et al. The relationship between stroke severity and prior direct oral anticoagulant therapy in patients with acute ischaemic stroke and non-valvular atrial fibrillation. Eur. J. Neurol. 2017, 24, 1399–1406. [Google Scholar] [CrossRef] [PubMed]
- Yamashiro, K.; Kurita, N.; Tanaka, R.; Ueno, Y.; Miyamoto, N.; Hira, K.; Nakajima, S.; Urabe, T.; Hattori, N. Adequate Adherence to Direct Oral Anticoagulant is Associated with Reduced Ischemic Stroke Severity in Patients with Atrial Fibrillation. J. Stroke Cerebrovasc. Dis. 2018, 28, 1773–1780. [Google Scholar] [CrossRef] [PubMed]
- Hannon, N.; Callaly, E.; Moore, A.; Chróinín, D.N.; Sheehan, O.; Marnane, M.; Merwick, A.; Kyne, L.; Duggan, J.; McCormack, P.M.E.; et al. Improved late survival and disability after stroke with therapeutic anticoagulation for atrial fibrillation: A population study. Stroke 2011, 42, 2503–2508. [Google Scholar] [CrossRef] [Green Version]
- Matsumoto, M.; Sakaguchi, M.; Okazaki, S.; Hashikawa, K.; Takahashi, T.; Matsumoto, M.; Ohtsuki, T.; Shimazu, T.; Yoshimine, T.; Mochizuki, H.; et al. Relationship between infarct volume and prothrombin time-international normalized ratio in ischemic stroke patients with nonvalvular atrial fibrillation. Circ. J. 2017, 81, 391–396. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Königsbrügge, O.; Weigel, G.; Quehenberger, P.; Pabinger, I.; Ay, C. Plasma clot formation and clot lysis to compare effects of different anticoagulation treatments on hemostasis in patients with atrial fibrillation. Clin. Exp. Med. 2018, 18, 325–336. [Google Scholar] [CrossRef] [Green Version]
- Ay, H.; Arsava, E.M.; Gungor, L.; Greer, D.; Singhal, A.B.; Furie, K.L.; Koroshetz, W.J.; Sorensen, A.G. Admission international normalized ratio and acute infarct volume in ischemic stroke. Ann. Neurol. 2008, 64, 499–506. [Google Scholar] [CrossRef] [PubMed]
- Yavasoglu, N.G.; Eren, Y.; Tatar, I.G.; Yalcinkaya, I. Infarct volumes of patients with acute ischemic stroke receiving direct oral anticoagulants due to non-valvular atrial fibrillation. Ann. Indian Acad. Neurol. 2021, 24, 27–31. [Google Scholar] [CrossRef] [PubMed]
- Hannon, N.; Arsava, E.M.; Audebert, H.J.; Ay, H.; Crowe, M.; Chróinín, D.N.; Furie, K.; McGorrian, C.; Molshatzki, N.; Murphy, S.; et al. Antithrombotic treatment at onset of stroke with atrial fibrillation, functional outcome, and fatality: A systematic review and meta-analysis. Int. J. Stroke 2015, 10, 808–814. [Google Scholar] [CrossRef] [PubMed]
- Takano, K.; Iino, K.; Ibayashi, S.; Tagawa, K.; Sadoshima, S.; Fujishima, M. Hypercoagulable state under low-intensity warfarin anticoagulation assessed with hemostatic markers in cardiac disorders. Am. J. Cardiol. 1994, 74, 935–939. [Google Scholar] [CrossRef]
- Chen, A.; Stecker, E.A.; Warden, B. Direct Oral Anticoagulant Use: A Practical Guide to Common Clinical Challenges. J. Am. Heart Assoc. 2020, 9, e017559. [Google Scholar] [CrossRef] [PubMed]
- Wańkowicz, P.; Nowacki, P.; Gołąb-Janowska, M. Risk factors for ischemic stroke in patients with non-valvular atrial fibrillation and therapeutic international normalized ratio range. Arch Med. Sci. 2019, 15, 1217–1222. [Google Scholar] [CrossRef] [PubMed]


| Study | Year | Type of Study | Inclusion Criteria | Exposure | Outcomes | Risk of Bias | |||
|---|---|---|---|---|---|---|---|---|---|
| Without OAC | DOAC | Therapeutical VKA | Non-Therapeutical VKA | ||||||
| Meinel et al. [13] | 2020 | Observational retrospective | AIS patients with AF (AF diagnosed either before or after stroke onset) aged ≥18 years | n = 4964 | n = 1603 | INR > 1.7 n = 854 | INR < 1.7 n = 604 | NIHSS at admission | Low |
| Sakamoto et al. [27] | 2017 | Observational retrospective | Patients with AIS or TIA with known AF | n = 352 | n = 43 | n = 35 | n = 54 | NIHSS at admission | Moderate |
| Yamashiro et al. [28] | 2018 | Observational retrospective | Patients with AF who developed AIS or TIA | n = 248 | n = 22 | INR ≥ 2 n = 16 | INR < 2 n = 95 | NIHSS at admission | Low |
| Hoyer et al. [12] | 2018 | Observational retrospective | Patients with newly detected AF or known AF admitted for AIS | n = 277 | n = 99 | - | NIHSS at admission | Low | |
| Hannon et al. [29] | 2011 | Observational prospective | Patients with new stroke events and AF (known or new) | n = 62 | - | INR 2–3 n = 14 | INR < 2 or > 3 n = 13 | NIHSS < 72 h | Low |
| Matsumoto et al. [30] | 2017 | Observational retrospective | AF patients who suffered AIS | n = 112 | - | - | n = 26 | NIHSS at admission | Low |
| DOAC | VKA Therapeutical | VKA Non-Therapeutical | Control Group | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Meinel et al. [13] | Sakamoto et al. [27] | Yamashiro et al. [28] | Hoyer et al. [12] | Meinel et al. [13] | Sakamoto et al. [27] | Yamashiro et al. [28] | Hannon et al. [29] | Meinel et al. [13] | Sakamoto et al. [27] | Yamashiro et al. [28] | Matsumoto et al. [30] | Hannon et al. [29] | Meinel et al. [13] | Sakamoto et al. [27] | Yamashiro et al. [28] | Matsumoto et al. [30] | Hoyer et al. [12] | Hannon et al. [29] | |
| Mean age, y | 79.8 | - | - | 79.2 | 80.7 | - | - | - | 82.1 | - | - | 76 | - | 79.4 | - | - | 76 | 79.4 | - |
| Median age, y | - | 78 (71–82) | 71 (63–81) | - | - | 80 (74-88) | 80 (73–84) | 77 (70–80) | - | 79 (75–86) | 80 (72–85) | - | 76 (69–80) | - | 78 (70–85) | 74 (67–82) | - | - | 77 (66–83) |
| Sex, (% female) | 46% | 49% | 40.6% | 52.5% | 44% | 54% | 31.3% | 64.3% | 54% | 41% | 39% | 45% | 46% | 49% | 42% | 36.7% | 49% | 54.5% | 50% |
| Hypertension (%) | 87% | 74% | 77.3% | 86.9% | 87% | 69% | 87.5% | 71.4% | 90% | 67% | 67.4% | 86% | 38.5% | 82% | 61% | 64.9% | 73% | 85.6% | 53% |
| Diabetes mellitus (%) | 25% | 26% | 45.5% | 28.3% | 28% | 17% | 37.5% | 21.4% | 27% | 20% | 35.8% | 24% | 23.1% | 21% | 16% | 20.2% | 27% | 31.8% | 3.3% |
| Hyperlipidemia (%) | 66% | 33% | 45.5% | 30.3% | 67% | 54% | 43.8% | 71.4% | 64% | 29% | 39% | 41% | 46.2% | 60% | 29% | 36.7% | 35% | 27.1% | 29.5% |
| Smokers (%) | 12% | 5% | 10.5% | 1% | 10% | 6% | 28.6% | 42.9% | 8% | 15% | 25.6% | 22% | 61.5% | 13% | 17% | 24.3% | 30% | 51% | 57.9% |
| CHADS2 score | - | 3 (2–4) | 2 (1–3.3) | - | - | 3 (2–4) | 3 (2.3–4) | - | - | 3 (2–4) | 2 (2–3) | 3.1 ± 1.5 | - | - | 2 (1–3) | 2 (1–2) | 2.8 ± 1.4 | - | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Garcia, C.; Silva, M.; Araújo, M.; Henriques, M.; Margarido, M.; Vicente, P.; Nzwalo, H.; Macedo, A. Admission Severity of Atrial-Fibrillation-Related Acute Ischemic Stroke in Patients under Anticoagulation Treatment: A Systematic Review and Meta-Analysis. J. Clin. Med. 2022, 11, 3563. https://doi.org/10.3390/jcm11123563
Garcia C, Silva M, Araújo M, Henriques M, Margarido M, Vicente P, Nzwalo H, Macedo A. Admission Severity of Atrial-Fibrillation-Related Acute Ischemic Stroke in Patients under Anticoagulation Treatment: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2022; 11(12):3563. https://doi.org/10.3390/jcm11123563
Chicago/Turabian StyleGarcia, Catarina, Marcelo Silva, Mariana Araújo, Mariana Henriques, Marta Margarido, Patrícia Vicente, Hipólito Nzwalo, and Ana Macedo. 2022. "Admission Severity of Atrial-Fibrillation-Related Acute Ischemic Stroke in Patients under Anticoagulation Treatment: A Systematic Review and Meta-Analysis" Journal of Clinical Medicine 11, no. 12: 3563. https://doi.org/10.3390/jcm11123563