
Functional Magnetic Resonance Imaging and Obesity—Novel Ways to Seen the Unseen


{kind=link}
Abstract
:1. Introduction
2. Methodology
3. Hunger and Satiety—Physiological Mechanisms
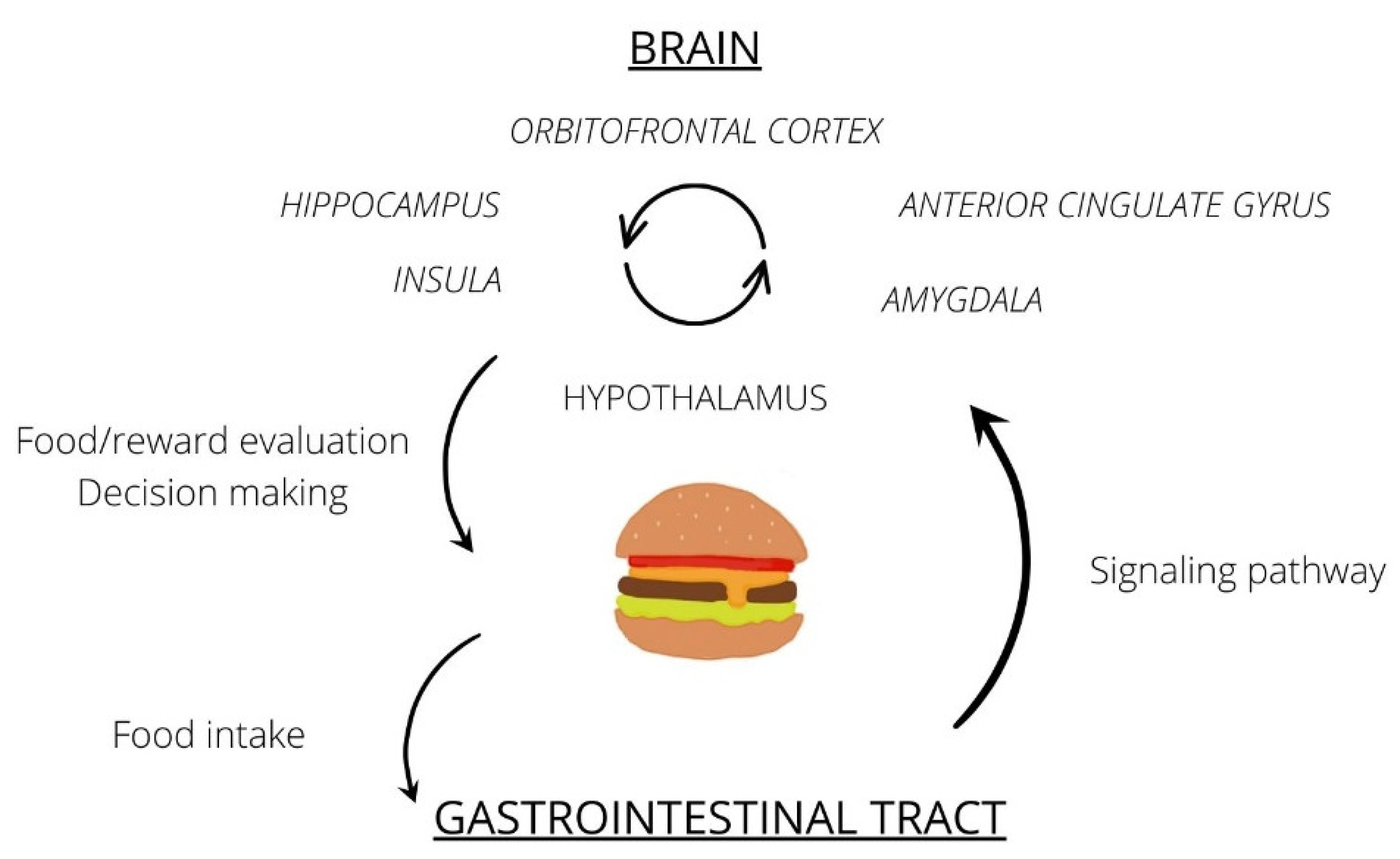
3.1. Food Intake Process
3.2. The Role of the Reward System in Food Consumption
3.3. Other Areas of the Brain Involved in Food Processing
4. Discussion
4.1. Food Intake in the Light of fMRI
4.2. The Influence of Obesity on the Brain
4.3. Altered Reward Circuit in Obesity
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Obesity and Overweight. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 8 February 2022).
- Hales, C.M.; Carroll, M.D.; Fryar, C.D.; Ogden, C.L. Prevalence of Obesity and Severe Obesity Among Adults: United States, 2017–2018 Key Findings Data from the National Health and Nutrition Examination Survey. 2017. Available online: https://www.cdc.gov/nchs/products/index.htm (accessed on 8 February 2022).
- Zhou, Y.; Chi, J.; Lv, W.; Wang, Y. Obesity and diabetes as high-risk factors for severe coronavirus disease 2019 (COVID-19). Diabetes/Metabolism. Res. Rev. 2020, 37, e3377. [Google Scholar] [CrossRef] [PubMed]
- Sinha, R. Role of addiction and stress neurobiology on food intake and obesity. Biol. Psychol. 2017, 131, 5–13. [Google Scholar] [CrossRef] [PubMed]
- Alonso-Alonso, M.; Woods, S.C.; Pelchat, M.; Grigson, P.; Stice, E.; Farooqi, S.; Khoo, C.S.; Mattes, R.D.; Beauchamp, G.K. Food reward system: Current perspectives and future research needs. Nutr. Rev. 2015, 73, 296–307. [Google Scholar] [CrossRef] [PubMed]
- Leigh, S.-J.; Morris, M.J. The role of reward circuitry and food addiction in the obesity epidemic: An update. Biol. Psychol. 2018, 131, 31–42. [Google Scholar] [CrossRef] [PubMed]
- Gendelis, S.; Inbar, D.; Inbar, K.; Mesner, S.; Kupchik, Y.M. Metaplasticity in the Ventral Pallidum as a Potential Marker for the Propensity to Gain Weight in Chronic High-Calorie Diet. J. Neurosci. 2020, 40, 9725–9735. [Google Scholar] [CrossRef]
- Farr, O.M.; Li, C.-S.R.; Mantzoros, C.S. Central nervous system regulation of eating: Insights from human brain imaging. Metabolism 2016, 65, 699–713. [Google Scholar] [CrossRef] [Green Version]
- Woods, S.C.; D’Alessio, D.A. Central Control of Body Weight and Appetite. J. Clin. Endocrinol. Metab. 2008, 93, s37–s50. [Google Scholar] [CrossRef] [Green Version]
- Hopkins, M.; Blundell, J.; Halford, J.; King, N.; Finlayson, G. The Regulation of Food Intake in Humans. Endotext. March 2016. Available online: https://www.ncbi.nlm.nih.gov/books/NBK278931/ (accessed on 8 February 2022).
- Alhabeeb, H.; AlFaiz, A.; Kutbi, E.; AlShahrani, D.; Alsuhail, A.; AlRajhi, S.; Alotaibi, N.; Alotaibi, K.; AlAmri, S.; Alghamdi, S.; et al. Gut Hormones in Health and Obesity: The Upcoming Role of Short Chain Fatty Acids. Nutrients 2021, 13, 481. [Google Scholar] [CrossRef]
- Denis, R.G.; Joly-Amado, A.; Webber, E.; Langlet, F.; Schaeffer, M.; Padilla, S.L.; Cansell, C.; Dehouck, B.; Castel, J.; Delbès, A.-S.; et al. Palatability Can Drive Feeding Independent of AgRP Neurons. Cell Metab. 2015, 22, 646–657. [Google Scholar] [CrossRef] [Green Version]
- Michaud, A.; Vainik, U.; Garcia-Garcia, I.; Dagher, A. Overlapping Neural Endophenotypes in Addiction and Obesity. Front. Endocrinol. 2017, 8, 127. [Google Scholar] [CrossRef] [Green Version]
- Maayan, L.; Hoogendoorn, C.; Sweat, V.; Convit, A. Disinhibited Eating in Obese Adolescents Is Associated With Orbitofrontal Volume Reductions and Executive Dysfunction. Obesity 2011, 19, 1382–1387. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Wen, B.; Cheng, J.; Li, H. Brain Structural Differences between Normal and Obese Adults and their Links with Lack of Perseverance, Negative Urgency, and Sensation Seeking. Sci. Rep. 2017, 7, 40595. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- García-García, I.; Kube, J.; Morys, F.; Schrimpf, A.; Kanaan, A.S.; Gaebler, M.; Villringer, A.; Dagher, A.; Horstmann, A.; Neumann, J. Liking and left amygdala activity during food versus nonfood processing are modulated by emotional context. Cogn. Affect. Behav. Neurosci. 2019, 20, 91–102. [Google Scholar] [CrossRef] [PubMed]
- Riederer, J.W.; Shott, M.E.; DeGuzman, M.; Pryor, T.L.; Frank, G.K.W. Understanding Neuronal Architecture in Obesity through Analysis of White Matter Connection Strength. Front. Hum. Neurosci. 2016, 10, 271. [Google Scholar] [CrossRef] [Green Version]
- Gómez-Apo, E.; Mondragón-Maya, A.; Ferrari-Díaz, M.; Silva-Pereyra, J. Structural Brain Changes Associated with Overweight and Obesity. J. Obes. 2021, 2021, 1–18. [Google Scholar] [CrossRef]
- Mier, W.; Mier, D. Advantages in functional imaging of the brain. Front. Hum. Neurosci. 2015, 9, 249. [Google Scholar] [CrossRef] [Green Version]
- Althubeati, S.; Avery, A.; Tench, C.R.; Lobo, D.N.; Salter, A.; Eldeghaidy, S. Mapping brain activity of gut-brain signaling to appetite and satiety in healthy adults: A systematic review and functional neuroimaging meta-analysis. Neurosci. Biobehav. Rev. 2022, 136, 104603. [Google Scholar] [CrossRef]
- Kroll, D.S.; Feldman, D.E.; Biesecker, C.L.; McPherson, K.L.; Manza, P.; Joseph, P.V.; Volkow, N.D.; Wang, G.-J. Neuroimaging of Sex/Gender Differences in Obesity: A Review of Structure, Function, and Neurotransmission. Nutrients 2020, 12, 1942. [Google Scholar] [CrossRef]
- Prickett, C.; Brennan, L.; Stolwyk, R. Examining the relationship between obesity and cognitive function: A systematic literature review. Obes. Res. Clin. Pr. 2015, 9, 93–113. [Google Scholar] [CrossRef]
- Livingston, G.; Sommerlad, A.; Orgeta, V.; Costafreda, S.G.; Huntley, J.; Ames, D.; Ballard, C.; Banerjee, S.; Burns, A.; Cohen-Mansfield, J.; et al. Dementia prevention, intervention, and care. Lancet 2017, 390, 2673–2734. [Google Scholar] [CrossRef] [Green Version]
- Raji, C.A.; Ho, A.J.; Parikshak, N.; Becker, J.; Lopez, O.L.; Kuller, L.H.; Hua, X.; Leow, A.D.; Toga, A.W.; Thompson, P.M. Brain structure and obesity. Hum. Brain Mapp. 2009, 31, 353–364. [Google Scholar] [CrossRef]
- Kim, A.-Y.; Shim, J.-H.; Choi, H.J.; Baek, H.-M. Comparison of volumetric and shape changes of subcortical structures based on 3-dimensional image between obesity and normal-weighted subjects using 3.0 T MRI. J. Clin. Neurosci. 2020, 73, 280–287. [Google Scholar] [CrossRef]
- Nguyen, J.C.D.; Killcross, A.S.; Jenkins, T.A. Obesity and cognitive decline: Role of inflammation and vascular changes. Front. Neurosci. 2014, 8, 375. [Google Scholar] [CrossRef] [PubMed]
- Sewaybricker, L.E.; Schur, E.A.; Melhorn, S.J.; Campos, B.; Askren, M.K.; Nogueira, G.A.S.; Zambon, M.P.; Antonio, M.A.R.G.M.; Cendes, F.; Velloso, L.A.; et al. Initial evidence for hypothalamic gliosis in children with obesity by quantitative T2 MRI and implications for blood oxygen-level dependent response to glucose ingestion. Pediatr. Obes. 2018, 14, e12486. [Google Scholar] [CrossRef] [PubMed]
- Guillemot-Legris, O.; Muccioli, G.G. Obesity-Induced Neuroinflammation: Beyond the Hypothalamus. Trends Neurosci. 2017, 40, 237–253. [Google Scholar] [CrossRef] [PubMed]
- Veronese, N.; Facchini, S.; Stubbs, B.; Luchini, C.; Solmi, M.; Manzato, E.; Sergi, G.; Maggi, S.; Cosco, T.; Fontana, L. Weight loss is associated with improvements in cognitive function among overweight and obese people: A systematic review and meta-analysis. Neurosci. Biobehav. Rev. 2017, 72, 87–94. [Google Scholar] [CrossRef] [PubMed]
- Van Opstal, A.M.; Wijngaarden, M.A.; Van Der Grond, J.; Pijl, H. Changes in brain activity after weight loss. Obes. Sci. Pr. 2019, 5, 459–467. [Google Scholar] [CrossRef] [Green Version]
- Patriarca, L.; Magerowski, G.; Alonso-Alonso, M. Functional neuroimaging in obesity. Curr. Opin. Endocrinol. Diabetes Obes. 2017, 24, 154–159. [Google Scholar] [CrossRef]
- Puzziferri, N.; Zigman, J.M.; Thomas, B.P.; Mihalakos, P.; Gallagher, R.; Lutter, M.; Carmody, T.; Lu, H.; Tamminga, C.A. Brain imaging demonstrates a reduced neural impact of eating in obesity. Obesity 2016, 24, 829–836. [Google Scholar] [CrossRef] [Green Version]
- Wijngaarden, M.; Veer, I.; Rombouts, S.; van Buchem, M.; van Dijk, K.W.; Pijl, H.; van der Grond, J. Obesity is marked by distinct functional connectivity in brain networks involved in food reward and salience. Behav. Brain Res. 2015, 287, 127–134. [Google Scholar] [CrossRef]
- Stopyra, M.A.; Friederich, H.-C.; Lavandier, N.; Mönning, E.; Bendszus, M.; Herzog, W.; Simon, J.J. Homeostasis and food craving in obesity: A functional MRI study. Int. J. Obes. 2021, 45, 2464–2470. [Google Scholar] [CrossRef] [PubMed]
- Lee, P.C.; Dixon, J.B. Food for Thought: Reward Mechanisms and Hedonic Overeating in Obesity. Curr. Obes. Rep. 2017, 6, 353–361. [Google Scholar] [CrossRef] [PubMed]
- Rothemund, Y.; Preuschhof, C.; Bohner, G.; Bauknecht, H.-C.; Klingebiel, R.; Flor, H.; Klapp, B.F. Differential activation of the dorsal striatum by high-calorie visual food stimuli in obese individuals. NeuroImage 2007, 37, 410–421. [Google Scholar] [CrossRef] [PubMed]
- Demos, K.E.; Heatherton, T.F.; Kelley, W.M. Individual Differences in Nucleus Accumbens Activity to Food and Sexual Images Predict Weight Gain and Sexual Behavior. J. Neurosci. 2012, 32, 5549–5552. [Google Scholar] [CrossRef]
- Langguth, B.; Schecklmann, M.; Lehner, A.; Landgrebe, M.; Poeppl, T.B.; Kreuzer, P.M.; Schlee, W.; Weisz, N.; Vanneste, S.; De Ridder, D. Neuroimaging and Neuromodulation: Complementary Approaches for Identifying the Neuronal Correlates of Tinnitus. Front. Syst. Neurosci. 2012, 6, 15. [Google Scholar] [CrossRef] [Green Version]
- Murdaugh, D.L.; Cox, J.E.; Cook, E.W., III; Weller, R.E. fMRI reactivity to high-calorie food pictures predicts short- and long-term outcome in a weight-loss program. NeuroImage 2011, 59, 2709–2721. [Google Scholar] [CrossRef] [Green Version]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Drelich-Zbroja, A.; Matuszek, M.; Kaczor, M.; Kuczyńska, M. Functional Magnetic Resonance Imaging and Obesity—Novel Ways to Seen the Unseen. J. Clin. Med. 2022, 11, 3561. https://doi.org/10.3390/jcm11123561
Drelich-Zbroja A, Matuszek M, Kaczor M, Kuczyńska M. Functional Magnetic Resonance Imaging and Obesity—Novel Ways to Seen the Unseen. Journal of Clinical Medicine. 2022; 11(12):3561. https://doi.org/10.3390/jcm11123561
Chicago/Turabian StyleDrelich-Zbroja, Anna, Małgorzata Matuszek, Michał Kaczor, and Maryla Kuczyńska. 2022. "Functional Magnetic Resonance Imaging and Obesity—Novel Ways to Seen the Unseen" Journal of Clinical Medicine 11, no. 12: 3561. https://doi.org/10.3390/jcm11123561