
Usefulness of Hospital Admission Chest X-ray Score for Predicting Mortality and ICU Admission in COVID-19 Patients


Abstract
:1. Introduction
2. Materials and Methods
3. Results
- Clinical characteristics of study population
- CXR score as a reliable measurement of lung lesions in COVID-19 patients
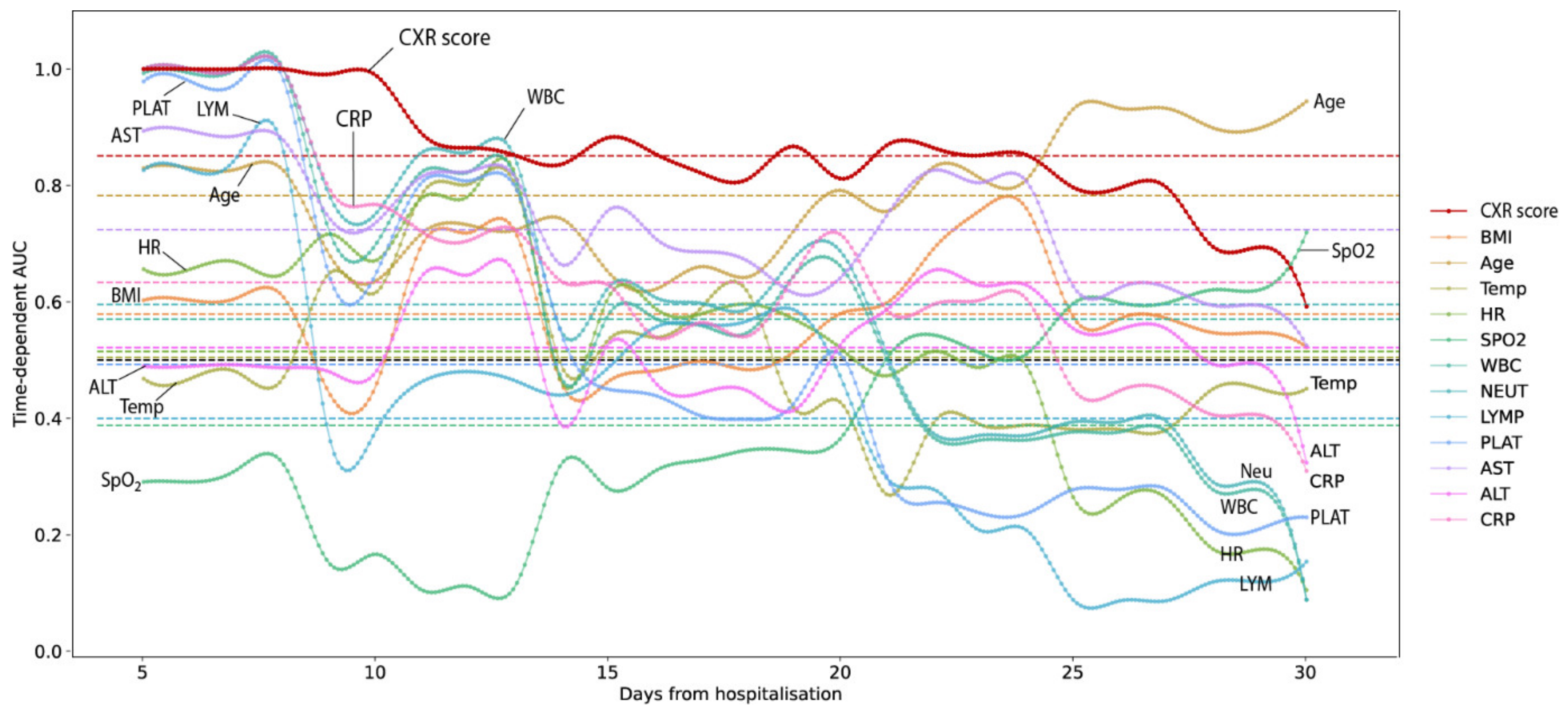
- CXR score as a predictor for the risk of mortality and ICU admission events
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lộc, H.; Mai, X.; Thịnh, N.; Hòa, M. NÓNG: TP.HCM Phát Hiện ca Dương Tính lần 1, Khoanh Yùng Một Block Chung cư ở Thủ Đức. Available online: https://tuoitre.vn/nong-tp-hcm-phat-hien-ca-duong-tinh-lan-1-khoanh-vung-mot-block-chung-cu-o-thu-duc-2021051810493121.htm (accessed on 20 April 2022).
- Anh, L. Bài Học Gì Từ đợt Dịch Thứ 4 Nhiều đau Thương? 2021. Available online: https://tuoitre.vn/bai-hoc-gi-tu-dot-dich-thu-4-nhieu-dau-thuong-20211118222229185.htm (accessed on 20 April 2022).
- Diễn Biến Dịch. 2021. Available online: https://ncov.moh.gov.vn/ (accessed on 20 April 2022).
- Worldometers.info. Available online: https://www.worldometers.info/ (accessed on 20 April 2022).
- Kim, H.W.; Capaccione, K.M.; Li, G.; Luk, L.; Widemon, R.S.; Rahman, O.; Beylergil, V.; Mitchell, R.; D’Souza, B.M.; Leb, J.S.; et al. The role of initial chest X-ray in triaging patients with suspected COVID-19 during the pandemic. Emerg. Radiol. 2020, 27, 617–621. [Google Scholar] [CrossRef] [PubMed]
- Schiaffino, S.; Tritella, S.; Cozzi, A.; Carriero, S.; Blandi, L.; Ferraris, L.; Sardanelli, F. Diagnostic Performance of Chest X-Ray for COVID-19 Pneumonia During the SARS-CoV-2 Pandemic in Lombardy, Italy. J. Thorac. Imaging 2020, 35, W105–W106. [Google Scholar] [CrossRef] [PubMed]
- Cozzi, A.; Schiaffino, S.; Arpaia, F.; Della Pepa, G.; Tritella, S.; Bertolotti, P.; Menicagli, L.; Monaco, C.G.; Carbonaro, L.A.; Spairani, R.; et al. Chest X-ray in the COVID-19 pandemic: Radiologists’ real-world reader performance. Eur. J. Radiol. 2020, 132, 109272. [Google Scholar] [CrossRef] [PubMed]
- Zanardo, M.; Schiaffino, S.; Sardanelli, F. Bringing radiology to patient’s home using mobile equipment: A weapon to fight COVID-19 pandemic. Clin. Imaging 2020, 68, 99–101. [Google Scholar] [CrossRef]
- Franquet, T.; Jeong, Y.J.; Lam, H.Y.S.; Wong, H.Y.F.; Chang, Y.-C.; Chung, M.J.; Lee, K.S. Imaging findings in coronavirus infections: SARS-CoV, MERS-CoV, and SARS-CoV-2. Br. J. Radiol. 2020, 93, 20200515. [Google Scholar] [CrossRef]
- Orsi, M.A.; Oliva, G.; Toluian, T.; Pittino, C.V.; Panzeri, M.; Cellina, M. Feasibility, Reproducibility, and Clinical Validity of a Quantitative Chest X-Ray Assessment for COVID-19. Am. J. Trop. Med. Hyg. 2020, 103, 822–827. [Google Scholar] [CrossRef]
- Wong, H.Y.F.; Lam, H.Y.S.; Fong, A.H.-T.; Leung, S.T.; Chin, T.W.-Y.; Lo, C.S.Y.; Lui, M.M.-S.; Lee, J.C.Y.; Chiu, K.W.-H.; Chung, T.W.-H.; et al. Frequency and Distribution of Chest Radiographic Findings in Patients Positive for COVID-19. Radiology 2020, 296, E72–E78. [Google Scholar] [CrossRef] [Green Version]
- Vancheri, S.G.; Savietto, G.; Ballati, F.; Maggi, A.; Canino, C.; Bortolotto, C.; Valentini, A.; Dore, R.; Stella, G.M.; Corsico, A.G.; et al. Radiographic findings in 240 patients with COVID-19 pneumonia: Time-dependence after the onset of symptoms. Eur. Radiol. 2020, 30, 6161–6169. [Google Scholar] [CrossRef]
- Guan, W.J.; Ni, Z.Y.; Hu, Y.; Liang, W.H.; Qu, C.Q.; He, J.X.; Liu, L.; Shan, H.; Lei, C.L.; Hui, D.S.C.; et al. Clinical Characteristics of Coronavirus Disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef]
- Cozzi, D.; Albanesi, M.; Cavigli, E.; Moroni, C.; Bindi, A.; Luvarà, S.; Lucarini, S.; Busoni, S.; Mazzoni, L.N.; Miele, V. Chest X-ray in new Coronavirus Disease 2019 (COVID-19) infection: Findings and correlation with clinical outcome. Radiol. Med. 2020, 125, 730–737. [Google Scholar] [CrossRef]
- Liang, W.; Liang, H.; Ou, L.; Chen, B.; Chen, A.; Li, C.; Li, Y.; Guan, W.; Sang, L.; Lu, J.; et al. Development and Validation of a Clinical Risk Score to Predict the Occurrence of Critical Illness in Hospitalized Patients With COVID-19. JAMA Intern. Med. 2020, 180, 1081–1089. [Google Scholar] [CrossRef]
- Gatti, M.; Calandri, M.; Barba, M.; Biondo, A.; Geninatti, C.; Gentile, S.; Greco, M.; Morrone, V.; Piatti, C.; Santonocito, A.; et al. Baseline chest X-ray in coronavirus disease 19 (COVID-19) patients: Association with clinical and laboratory data. Radiol. Med. 2020, 125, 1271–1279. [Google Scholar] [CrossRef]
- Reeves, R.A.; Pomeranz, C.; Gomella, A.A.; Gulati, A.; Metra, B.; Hage, A.; Lange, S.; Parekh, M.; Donuru, A.; Lakhani, P.; et al. Performance of a Severity Score on Admission Chest Radiography in Predicting Clinical Outcomes in Hospitalized Patients with Coronavirus Disease (COVID-19). Am. J. Roentgenol. 2021, 217, 623–632. [Google Scholar] [CrossRef]
- Yushkevich, P.A.; Piven, J.; Hazlett, H.C.; Smith, R.G.; Ho, S.; Gee, J.C.; Gerig, G. User-guided 3D active contour segmentation of anatomical structures: Significantly improved efficiency and reliability. NeuroImage 2006, 31, 1116–1128. [Google Scholar] [CrossRef] [Green Version]
- Kendall, M.G.; Gibbons, J.D. Rank Correlation Methods; Oxford University Press: New York, NY, USA, 1990. [Google Scholar]
- Kaplan, E.L.; Meier, P. Nonparametric Estimation from Incomplete Observations. J. Am. Stat. Assoc. 1958, 53, 457–481. [Google Scholar] [CrossRef]
- Cox, D.R. Note on Grouping. J. Am. Stat. Assoc. 1957, 52, 543–547. [Google Scholar] [CrossRef]
- T. pandas development team. Pandas-dev/Pandas: Pandas; Zenodo: New York, NY, USA, 2020. [Google Scholar] [CrossRef]
- Virtanen, P.; Gommers, R.; Oliphant, T.E.; Haberland, M.; Reddy, T.; Cournapeau, D.; Burovski, E.; Peterson, P.; Weckesser, W.; Bright, J.; et al. SciPy 1.0: Fundamental Algorithms for Scientific Computing in Python. Nat. Methods 2020, 17, 261–272. [Google Scholar] [CrossRef] [Green Version]
- Davidson-Pilon, C. Lifelines: Survival analysis in Python. J. Open Source Softw. 2019, 4, 1317. [Google Scholar] [CrossRef] [Green Version]
- Hunter, J.D. Matplotlib: A 2D graphics environment. Comput. Sci. Eng. 2007, 9, 90–95. [Google Scholar] [CrossRef]
- Pedregosa, F.; Varoquaux, G.; Gramfort, A.; Michel, V.; Thirion, B. Scikit-learn: Machine Learning in Python. J. Mach. Learn. Res. 2011, 12, 2825–2830. [Google Scholar]
- Toussie, D.; Voutsinas, N.; Finkelstein, M.; Cedillo, M.A.; Manna, S.; Maron, S.Z.; Jacobi, A.; Chung, M.; Bernheim, A.; Eber, C.; et al. Clinical and Chest Radiography Features Determine Patient Outcomes in Young and Middle-aged Adults with COVID-19. Radiology 2020, 297, E197–E206. [Google Scholar] [CrossRef] [PubMed]
- Borghesi, A.; Zigliani, A.; Masciullo, R.; Golemi, S.; Maculotti, P.; Farina, D.; Maroldi, R. Radiographic severity index in COVID-19 pneumonia: Relationship to age and sex in 783 Italian patients. Radiol. Med. 2020, 125, 461–464. [Google Scholar] [CrossRef]
- Borghesi, A.; Zigliani, A.; Golemi, S.; Carapella, N.; Maculotti, P.; Farina, D.; Maroldi, R. Chest X-ray severity index as a predictor of in-hospital mortality in coronavirus disease 2019: A study of 302 patients from Italy. Int. J. Infect. Dis. 2020, 96, 291–293. [Google Scholar] [CrossRef]
- Hui, T.C.H.; Khoo, H.W.; Young, B.E.; Mohideen, S.M.H.; Lee, Y.S.; Lim, C.J.; Leo, Y.S.; Kaw, G.J.L.; Lye, D.C.; Tan, C.H. Clinical utility of chest radiography for severe COVID-19. Quant. Imaging Med. Surg. 2020, 10, 1540–1550. [Google Scholar] [CrossRef]
- Ralph, A.P.; Ardian, M.; Wiguna, A.; Maguire, G.P.; Becker, N.G.; Drogumuller, G.; Wilks, M.J.; Waramori, G.; Tjitra, E.; Sandjaja; et al. A simple, valid, numerical score for grading chest X-ray severity in adult smear-positive pulmonary tuberculosis. Thorax 2010, 65, 863–869. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taylor, E.; Haven, K.; Reed, P.; Bissielo, A.; Harvey, D.; McArthur, C.; Bringans, C.; Freundlich, S.; Ingram, R.J.H.; Perry, D. A chest radiograph scoring system in patients with severe acute respiratory infection: A validation study. BMC Med. Imaging. 2015, 15, 61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Warren, M.A.; Zhao, Z.; Koyama, T.; Bastarache, J.A.; Shaver, C.M.; Semler, M.W.; Rice, T.W.; Matthay, M.A.; Calfee, C.S.; Ware, L.B. Severity scoring of lung oedema on the chest radiograph is associated with clinical outcomes in ARDS. Thorax 2018, 73, 840–846. [Google Scholar] [CrossRef]
- Borghesi, A.; Maroldi, R. COVID-19 outbreak in Italy: Experimental chest X-ray scoring system for quantifying and monitoring disease progression. Radiol. Med. 2020, 125, 509–513. [Google Scholar] [CrossRef]
- Sun, D.; Li, X.; Guo, D.; Wu, L.; Chen, T.; Fang, Z.; Chen, L.; Zeng, W.; Yang, R. CT Quantitative Analysis and Its Relationship with Clinical Features for Assessing the Severity of Patients with COVID-19. Korean J. Radiol. 2020, 21, 859–868. [Google Scholar] [CrossRef]
- Li, K.; Fang, Y.; Li, W.; Pan, C.; Qin, P.; Zhong, Y.; Liu, X.; Huang, M.; Liao, Y.; Li, S. CT image visual quantitative evaluation and clinical classification of coronavirus disease (COVID-19). Eur. Radiol. 2020, 30, 4407–4416. [Google Scholar] [CrossRef] [Green Version]
- Francone, M.; Iafrate, F.; Masci, G.M.; Coco, S.; Cilia, F.; Manganaro, L.; Panebianco, V.; Andreoli, C.; Colaiacomo, M.C.; Zingaropoli, M.A.; et al. Chest CT score in COVID-19 patients: Correlation with disease severity and short-term prognosis. Eur. Radiol. 2020, 30, 6808–6817. [Google Scholar] [CrossRef]
- Sng, L.; Arlany, L.; Toh, L.; Loo, T.; Ilzam, N.; Wong, B.; Lanca, L. Initial data from an experiment to implement a safe procedure to perform PA erect chest radiographs for COVID-19 patients with a mobile radiographic system in a ‘clean’ zone of the hospital ward. Radiography 2021, 27, 48–53. [Google Scholar] [CrossRef]
- Rai, A.; Ditkofsky, N.; Hunt, B.; Dubrawski, M.; Deva, D.; Mathur, S. Portable Chest Radiography Through Glass During COVID-19 Pandemic-Initial Experience in a Tertiary Care Center. Can. Assoc. Radiol. J. 2021, 72, 175–179. [Google Scholar] [CrossRef]
- Rorat, M.; Zińczuk, A.; Szymański, W.; Simon, K.; Guziński, M. Usefulness of a portable chest radiograph in the initial diagnosis of coronavirus disease 2019. Pol. Arch. Intern. Med. 2020, 130, 906–909. [Google Scholar] [CrossRef]
- Pare, J.R.; Camelo, I.; Mayo, K.C.; Leo, M.M.; Dugas, J.N.; Nelson, K.P.; Baker, W.E.; Shareef, F.; Mitchell, P.M.; Schechter-Perkins, E.M. Point-of-care Lung Ultrasound Is More Sensitive than Chest Radiograph for Evaluation of COVID-19. West. J. Emerg. Med. 2020, 21, 771–778. [Google Scholar] [CrossRef]
- Knight, S.R.; Ho, A.; Pius, R.; Buchan, I.; Carson, G.; Drake, T.M.; Dunning, J.; Fairfield, C.J.; Gamble, C.; Green, C.A.; et al. Risk stratification of patients admitted to hospital with COVID-19 using the ISARIC WHO Clinical Characterisation Protocol: Development and validation of the 4C Mortality Score. BMJ 2020, 370, m3339. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variable | Pooled Data | Survival Outcome Subgroups | ||
|---|---|---|---|---|
| Survived | Died | p Value * | ||
| Number of patients | 219 | 191 | 28 | |
| Age, year | 57.77 (18.11–81.29) | 52.72 (17.07–78.73) | 69.15 (52.77–83.86) | <0.00001 |
| Male gender: freq (%) | 111/219 (50.68) | 97/191 (50.75) | 14/28 (50.00) | 1.0 |
| Body mass index, kg/m2 | 23.44 (17.86–30.04) | 23.31 (17.8–29.78) | 24.09 (19.77–29.52) | 0.04 |
| Admission measures | ||||
| - Temperature, °C | 37.0 (36.5–38.5) | 37.0 (36.5–38.5) | 37.00 (36.4–38.6) | 0.41 |
| - Respiratory rate, breaths/min | 20.0 (18–31.75) | 20.0 (18–29) | 26.00 (20–41.4) | <0.00001 |
| - Heart rate, beats/min | 88.0 (68.95–115) | 88.0 (68.55–113.9) | 90.5 (71.35–120) | 0.149485 |
| - Pulse oxygen saturation (SpO2) % | 96.0 (83.4–98.0) | 96.0 (86.4–98) | 89.0 (70–97) | <0.00001 |
| Oxygen support within first 24 h | ||||
| Room air | 90 (41.10%) | 90 | 0 | <0.0001 |
| Canula | 69 (31.51%) | 67 | 2 | |
| HFNC | 27 (12.33%) | 18 | 9 | |
| Mask | 23 (10.05%) | 14 | 9 | |
| NIV | 6 (2.7%) | 1 | 5 | |
| Mechanical ventilation/Tracheal intubation | 4 (1.8%) | 1 | 3 | |
| Blood test and other biomarkers | ||||
| White blood cell count, 109/L | 6.4 (3.71–14.09) | 6.10 (1.9–10.63) | 9.10 (3.31–21.17) | <0.01 |
| Neutrophil count, 109/L | 4.6 (1.9–12.8) | 4.30 (1.9–10.66) | 8.50 (3.31–21.17) | <0.0001 |
| Lymphocyte count, 109/L | 1.0 (0.3–2.4) | 1.10 (0.325–2.5) | 0.60 (0.2–1.57) | <0.0001 |
| Platelet count, 109/L | 204 (115–401) | 202.0 (115.3–383.7) | 205.0 (96–431.5) | 0.486075 |
| Hemoglobin, g/dL | 13.20 (10.2–15.9) | 13.25 (10.13–15.96) | 13.10 (11.13–15.62) | 0.296964 |
| Aspartate Aminotransferase, U/L | 39.0 (17.55–137.35) | 34.55 (16.96–118.98) | 83.70 (36.73–213.88) | <0.00001 |
| Alanine Aminotransferase, U/L | 37.45 (12.37–132.03) | 33.20 (11.54–121.38) | 67.20 (26.87–212.29) | <0.0001 |
| C reactive protein, mg/L | 23.52 (0.93– 161.75) | 18.40 (0.84–150.62) | 86.71 (26.81–169.26) | <0.0001 |
| Comorbidities | ||||
| Diabetes | 79/219 (36.07) | 66/191 | 13/28 | <0.001 |
| Hypertension | 75/219 | 60/191 | 15/28 | 0.09 |
| Cardiovascular disease | 15/219 | 10/191 | 5/28 | 0.04 |
| Antiviral treatment | ||||
| 154/219 | 129/191 | 25/28 | 0.042 | |
| Remdecivir | 152 | 127 | 25 | |
| Molnupiravir | 2 | 2 | 0 | |
| COVID–19 vaccination | ||||
| Dose 1 | 107/219 | 98/191 | 9/28 | 0.163838 |
| Dose 2 | 6/219 | 6/191 | 0/28 | 0.518534 |
| Severity degree on admission | ||||
| 1 | 90 (41.10%) | 90 | 0 | <0.0001 |
| 2 | 61 (27.85%) | 57 | 4 | |
| 3 | 65 (29,68%) | 43 | 22 | |
| 4 | 3 (1.37%) | 1 | 2 | |
| Most severe degree during hospitalization | ||||
| 1 | 68 (31.05%) | 68 | 0 | <0.0001 |
| 2 | 63 (28.77%) | 63 | 0 | |
| 3 | 53 (24.20%) | 53 | 1 | |
| 4 | 34 (15.53%) | 7 | 27 | |
| Intensive care unit admission, | 34 (15.28%) | 8/191 | 26/28 | <0.00001 |
| - Mechanical ventilation | 29 | 7 | 22 | <0.00001 |
| - CRRT | 16 | 1 | 15 | <0.0001 |
| - ECMO | 3 | 0 | 3 | 0.0002 |
| Length of symptom onset, day | 16.0 (9–51.6) | 15 (9–35.5) | 27.5 (12.7–56) | <0.00001 |
| Length of stay, day | 10.0 (4–35.9) | 10.0 (4–28) | 19.5 (7.7–46.95) | <0.00001 |
| Pooled Data | Survival Outcome | |||
|---|---|---|---|---|
| Survival | Died | p Value * | ||
| Size | 219 | 191 | 28 | |
| CXR score | 9.33 (12.33) | 7.33 (11.33) | 19.67 (2.33) | <0.0001 |
| Extent Q1 | 3.0 (6.0) | 3.0 (5.0) | 9.0 (1.5) | <0.0001 |
| Extent Q2 | 4.0 (6.0) | 3.0 (6.0) | 9.0 (1.0) | <0.0001 |
| Extent Q3 | 2.0 (5.0) | 2.0 (4.0) | 7.0 (7.0) | <0.0001 |
| Extent Q4 | 4.0 (7.0) | 3.0 (6.0) | 9.0 (1.0) | <0.0001 |
| Severity Q1 | 3.0 (4.0) | 3.0 (3.0) | 6.0 (1.0) | <0.0001 |
| Severity Q2 | 4.0 (4.0) | 3.0 (4.0) | 6.0 (0.0) | <0.0001 |
| Severity Q3 | 2.0 (3.5) | 2.0 (4.0) | 6.0 (2.0) | <0.0001 |
| Severity Q4 | 3.50 (5.0) | 3.0 (4.0) | 6.0 (1.0) | <0.0001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hoang-Thi, T.-N.; Tran, D.-T.; Tran, H.-D.; Tran, M.-C.; Ton-Nu, T.-M.; Trinh-Le, H.-M.; Le-Huu, H.-N.; Le-Thi, N.-M.; Tran, C.-T.; Le-Dong, N.-N.; et al. Usefulness of Hospital Admission Chest X-ray Score for Predicting Mortality and ICU Admission in COVID-19 Patients. J. Clin. Med. 2022, 11, 3548. https://doi.org/10.3390/jcm11123548
Hoang-Thi T-N, Tran D-T, Tran H-D, Tran M-C, Ton-Nu T-M, Trinh-Le H-M, Le-Huu H-N, Le-Thi N-M, Tran C-T, Le-Dong N-N, et al. Usefulness of Hospital Admission Chest X-ray Score for Predicting Mortality and ICU Admission in COVID-19 Patients. Journal of Clinical Medicine. 2022; 11(12):3548. https://doi.org/10.3390/jcm11123548
Chicago/Turabian StyleHoang-Thi, Trieu-Nghi, Duc-Tuan Tran, Hai-Dang Tran, Manh-Cuong Tran, Tra-My Ton-Nu, Hong-Minh Trinh-Le, Hanh-Nhi Le-Huu, Nga-My Le-Thi, Cong-Trinh Tran, Nhat-Nam Le-Dong, and et al. 2022. "Usefulness of Hospital Admission Chest X-ray Score for Predicting Mortality and ICU Admission in COVID-19 Patients" Journal of Clinical Medicine 11, no. 12: 3548. https://doi.org/10.3390/jcm11123548