
Unexplained Left Ventricular Hypertrophy with Symptomatic High-Grade Atrioventricular Block in Elderly Patients: A Case Report


Abstract
:1. Introduction
2. Case Presentation
3. Discussion
3.1. Differential Diagnosis of Elderly LVH
3.2. Diagnosis of FD
3.3. Management of FD
3.4. Management of FD with Symptomatic High-Grade AV Block
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| FD | Fabry disease |
| LVH | Left ventricular hypertrophy |
| HCM | Hypertrophic cardiomyopathy |
| AV | Atrioventricular |
| ECG | Electrocardiogram |
| TTE | Transthoracic echocardiography |
| RV | Right ventricular |
| LV | Left ventricular |
| EF | Ejection fraction |
| PICMOPD | Pacing-induced cardiomyopathyOutpatient department |
| SCD | Sudden cardiac death |
| ATTRwt | Wild-type transthyretin amyloidosis |
| α-Gal A | α-galactosidase A |
| Gb3 | Globotriaosylceramide |
| Lyso-Gb3 | Globotriaosylsphingosine |
| CMR | Cardiac magnetic resonance imaging |
| OT | Outflow tract |
| ERT | Enzyme replacement therapy |
References
- Geske, J.B.; Ommen, S.R.; Gersh, B.J. Hypertrophic Cardiomyopathy: Clinical Update. JACC Heart Fail. 2018, 6, 364–375. [Google Scholar] [CrossRef]
- Arad, M.; Maron, B.J.; Gorham, J.M.; Johnson, W.H.; Saul, J.P.; Perez-Atayde, A.R.; Spirito, P.; Wright, G.B.; Kanter, R.J.; Seidman, C.E.; et al. Glycogen Storage Diseases Presenting as Hypertrophic Cardiomyopathy. N. Engl. J. Med. 2005, 352, 362–372. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yousef, Z.; Elliott, P.; Cecchi, F.; Escoubet, B.; Linhart, A.; Monserrat, L.; Namdar, M.; Weidemann, F. Left ventricular hypertrophy in Fabry disease: A practical approach to diagnosis. Eur. Heart J. 2012, 34, 802–808. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Linhart, A.; Germain, D.P.; Olivotto, I.; Akhtar, M.M.; Anastasakis, A.; Hughes, D.; Namdar, M.; Pieroni, M.; Hagège, A.; Cecchi, F.; et al. An expert consensus document on the management of cardiovascular manifestations of Fabry disease. Eur. J. Heart Fail. 2020, 22, 1076–1096. [Google Scholar] [CrossRef] [PubMed]
- Pieroni, M.; Moon, J.C.; Arbustini, E.; Barriales-Villa, R.; Camporeale, A.; Vujkovac, A.C.; Elliott, P.M.; Hagege, A.; Kuusisto, J.; Linhart, A.; et al. Cardiac Involvement in Fabry Disease: Jacc Review Topic of the Week. J. Am. Coll. Cardiol. 2021, 77, 922–936. [Google Scholar] [CrossRef]
- Hagège, A.; Réant, P.; Habib, G.; Damy, T.; Barone-Rochette, G.; Soulat, G.; Donal, E.; Germain, D.P. Fabry disease in cardiology practice: Literature review and expert point of view. Arch. Cardiovasc. Dis. 2019, 112, 278–287. [Google Scholar] [CrossRef]
- Hwu, W.L.; Chien, Y.H.; Lee, N.C.; Chiang, S.C.; Dobrovolny, R.; Huang, A.C.; Yeh, H.Y.; Chao, M.C.; Lin, S.J.; Kitagawa, T.; et al. Newborn Screening for Fabry Disease in Taiwan Reveals a High Incidence of the Later-Onset Gla Mutation C.936+919g>a (Ivs4+919g>a). Hum. Mutat. 2009, 30, 1397–1405. [Google Scholar] [CrossRef] [Green Version]
- Tarnopolsky, M.; Katzberg, H.; Petrof, B.J.; Sirrs, S.; Sarnat, H.B.; Myers, K.; Dupré, N.; Dodig, D.; Genge, A.; Venance, S.L.; et al. Pompe Disease: Diagnosis and Management. Evidence-Based Guidelines from a Canadian Expert Panel. Can. J. Neurol. Sci. 2016, 43, 472–485. [Google Scholar] [CrossRef] [Green Version]
- Adam, R.D.; Coriu, D.; Jercan, A.; Bădeliţă, S.; Popescu, B.A.; Damy, T.; Jurcuţ, R. Progress and challenges in the treatment of cardiac amyloidosis: A review of the literature. ESC Heart Fail. 2021, 8, 2380–2396. [Google Scholar] [CrossRef]
- Perugini, E.; Guidalotti, P.L.; Salvi, F.; Cooke, R.M.; Pettinato, C.; Riva, L.; Leone, O.; Farsad, M.; Ciliberti, P.; Bacchi-Reggiani, L.; et al. Noninvasive Etiologic Diagnosis of Cardiac Amyloidosis Using 99mtc-3,3-Diphosphono-1,2-Propanodicarboxylic Acid Scintigraphy. J. Am. Coll. Cardiol. 2005, 46, 1076–1084. [Google Scholar] [CrossRef] [Green Version]
- Hsu, T.R.; Hung, S.C.; Chang, F.P.; Yu, W.C.; Sung, S.H.; Hsu, C.L.; Dzhagalov, I.; Yang, C.F.; Chu, T.H.; Lee, H.J.; et al. Later Onset Fabry Disease, Cardiac Damage Progress in Silence: Experience with a Highly Prevalent Mutation. J. Am. Coll. Cardiol. 2016, 68, 2554–2563. [Google Scholar] [CrossRef] [PubMed]
- Fan, Y.; Chan, T.-N.; Chow, J.; Kam, K.; Chi, W.-K.; Chan, J.; Fung, E.; Tong, M.; Wong, J.; Choi, P.; et al. High Prevalence of Late-Onset Fabry Cardiomyopathy in a Cohort of 499 Non-Selective Patients with Left Ventricular Hypertrophy: The Asian Fabry Cardiomyopathy High-Risk Screening Study (Asian-Fame). J. Clin. Med. 2021, 10, 2160. [Google Scholar] [CrossRef] [PubMed]
- Esposito, R.; Santoro, C.; Mandoli, G.E.; Cuomo, V.; Sorrentino, R.; La Mura, L.; Pastore, M.C.; Bandera, F.; D’Ascenzi, F.; Malagoli, A.; et al. Cardiac Imaging in Anderson-Fabry Disease: Past, Present and Future. J. Clin. Med. 2021, 10, 1994. [Google Scholar] [CrossRef] [PubMed]
- Vardarli, I.; Weber, M.; Rischpler, C.; Führer, D.; Herrmann, K.; Weidemann, F. Fabry Cardiomyopathy: Current Treatment and Future Options. J. Clin. Med. 2021, 10, 3026. [Google Scholar] [CrossRef] [PubMed]
- Yim, J.; Yau, O.; Yeung, D.; Tsang, T. Fabry Cardiomyopathy: Current Practice and Future Directions. Cells 2021, 10, 1532. [Google Scholar] [CrossRef] [PubMed]
- Germain, D.P.; Elliott, P.; Falissard, B.; Fomin, V.V.; Hilz, M.J.; Jovanovic, A.; Kantola, I.; Linhart, A.; Mignani, R.; Namdar, M.; et al. The effect of enzyme replacement therapy on clinical outcomes in male patients with Fabry disease: A systematic literature review by a European panel of experts. Mol. Genet. Metab. Rep. 2019, 19, 100454. [Google Scholar] [CrossRef]
- Miller, J.J.; Kanack, A.J.; Dahms, N.M. Progress in the understanding and treatment of Fabry disease. Biochim. Biophys. Acta (BBA) Gen. Subj. 2020, 1864, 129437. [Google Scholar] [CrossRef]
- Kusumoto, F.M.; Schoenfeld, M.H.; Barrett, C.; Edgerton, J.R.; Ellenbogen, K.A.; Gold, M.R.; Goldschlager, N.F.; Hamilton, R.M.; Joglar, J.A.; Kim, R.J.; et al. 2018 Acc/Aha/Hrs Guideline on the Evaluation and Management of Patients with Bradycardia and Cardiac Conduction Delay: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. Circulation 2019, 140, e382–e482. [Google Scholar]
- Merchant, F.M.; Mittal, S. Pacing Induced Cardiomyopathy. J. Cardiovasc. Electrophysiol. 2020, 31, 286–292. [Google Scholar] [CrossRef]
- Khurshid, S.; Obeng-Gyimah, E.; Supple, G.E.; Schaller, R.; Lin, D.; Owens, A.T.; Epstein, A.E.; Dixit, S.; Marchlinski, F.E.; Frankel, D.S. Reversal of Pacing-Induced Cardiomyopathy Following Cardiac Resynchronization Therapy. JACC Clin. Electrophysiol. 2017, 4, 168–177. [Google Scholar] [CrossRef]
- Slotwiner, D.J.; Raitt, M.H.; Munoz, F.D.-C.; Mulpuru, S.K.; Nasser, N.; Peterson, P.N. Impact of Physiologic Pacing Versus Right Ventricular Pacing Among Patients With Left Ventricular Ejection Fraction Greater Than 35%: A Systematic Review for the 2018 ACC/AHA/HRS Guideline on the Evaluation and Management of Patients With Bradycardia and Cardiac Conduction Delay: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. J. Am. Coll. Cardiol. 2019, 74, 988–1008. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Year | Age | Symptoms | Evaluation | Management |
|---|---|---|---|---|
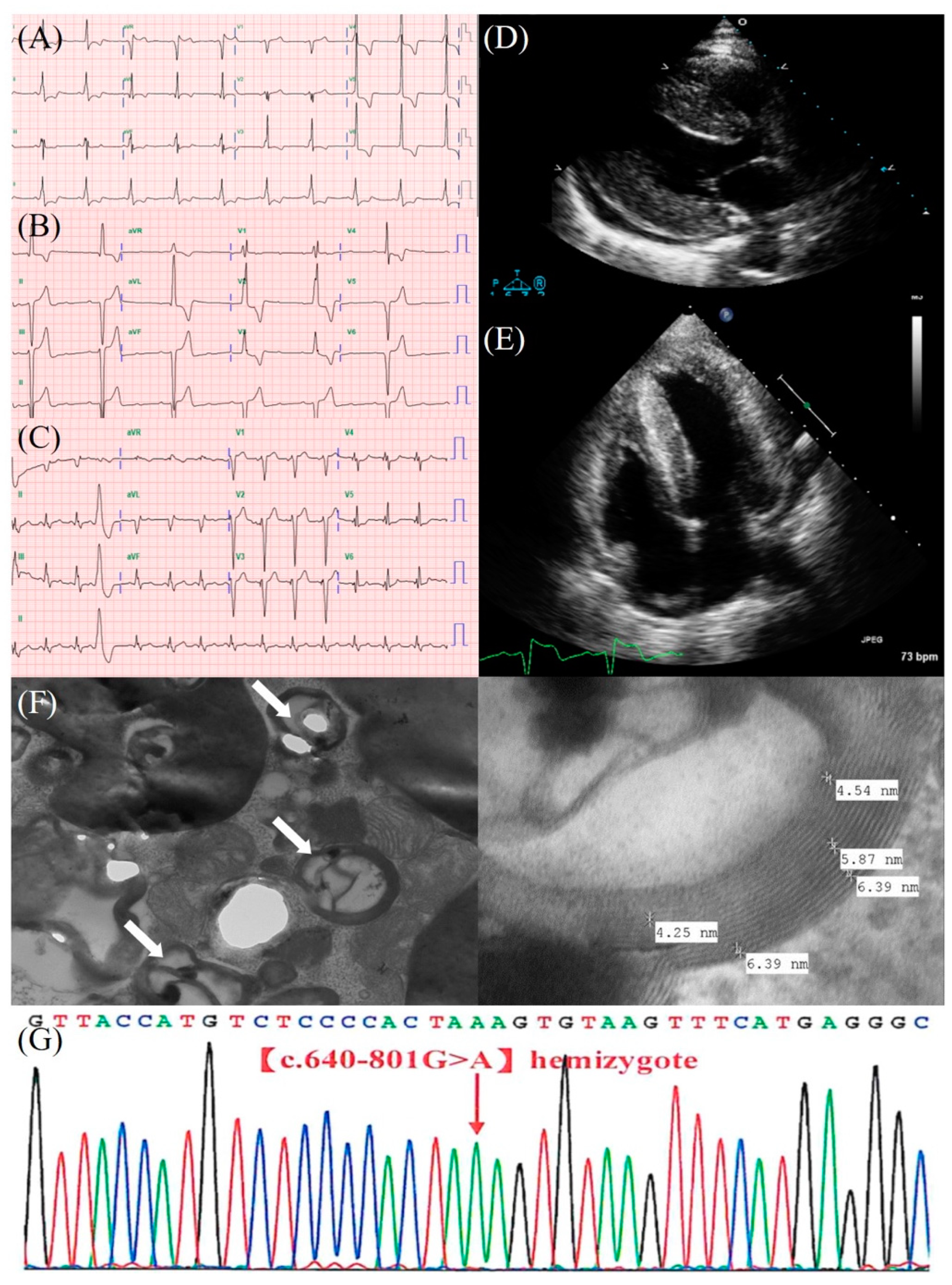
| 2008 | 63 | Palpitation | ECG: Sinus rhythm, ventricular preexcitation, LVH (Figure 1A) Holter: Normal TTE: Concentric LVH, impaired LV relaxation (Figure 1D,E) | OPD follow-up |
| 2011 | 66 | Palpitation and chest tightness | ECG: Sinus rhythm, ventricular preexcitation, LVH Holter: Normal | OPD follow-up |
| 2015 | 70 | Palpitation and chest tightness | Holter: Normal TTE: Concentric LVH, LV diastolic dysfunction, adequate LV systolic function, LVEF = 76%, E/e′: 20.2, LV mass index: 273.0 g/m2 Treadmill test: Positive for ischemia | PCI, OPD follow-up |
| 2016 | 71 | Dizziness | ECG: 3:1 AV block (Figure 1B) | PPM (DDDR), OPD follow-up |
| 2017 | 72 | X | ECG: Ventricular pacing rhythm, QRS = 180 ms | OPD follow-up |
| 2019 | 74 | DOE | ECG: Ventricular pacing rhythm, QRS = 180 ms TTE: Concentric LVH, apical LV hypokinesis, borderline LV systolic function, LVEF = 53%, E/e′: 17.0, LV mass index: 292.9 g/m2 | HF drugs, OPD follow-up |
| 2021 | 76 | Aggravated DOE | ECG: Ventricular pacing rhythm, QRS = 200 ms ECG (s/p CRT): Biventricular pacing rhythm, QRS = 160 ms (Figure 1C) TTE: Concentric LVH, large apical LV akinesis, impaired LV systolic function, LVEF = 20%, E/e′: 21.4, LV mass index: 160.0 g/m2 TTE (s/p CRT): Concentric LVH, apical LV hypokinesis, LVEF = 35%, E/e′: 11.9, LV mass index: 214.5 g/m2 | CRT, HF drugs, ERT, OPD follow-up |
| Examination | Results | Reference Value |
|---|---|---|
| α-Gal A activity | 1.17 μmol/h (borderline) | N > 1.5 Borderline: 0.6~1.5 (μmol/h) |
| Plasma Lyso-Gb3 | 11.95 ng/mL (elevated) | N < 0.8 (ng/mL) |
| Endomyocardial biopsy | Cardiomyocytes are focally vacuolated with a lace-like appearance. The electron microscope showed laminated lysosomal inclusions (zebra bodies) (Figure 1F). | Compatible with FD |
| Genetic sequencing | Genotype: c.640-801G>A (Figure 1G) | Also known as IVS4+919G>A and c.936+919G>A, Cardiac variant of FD [7] |
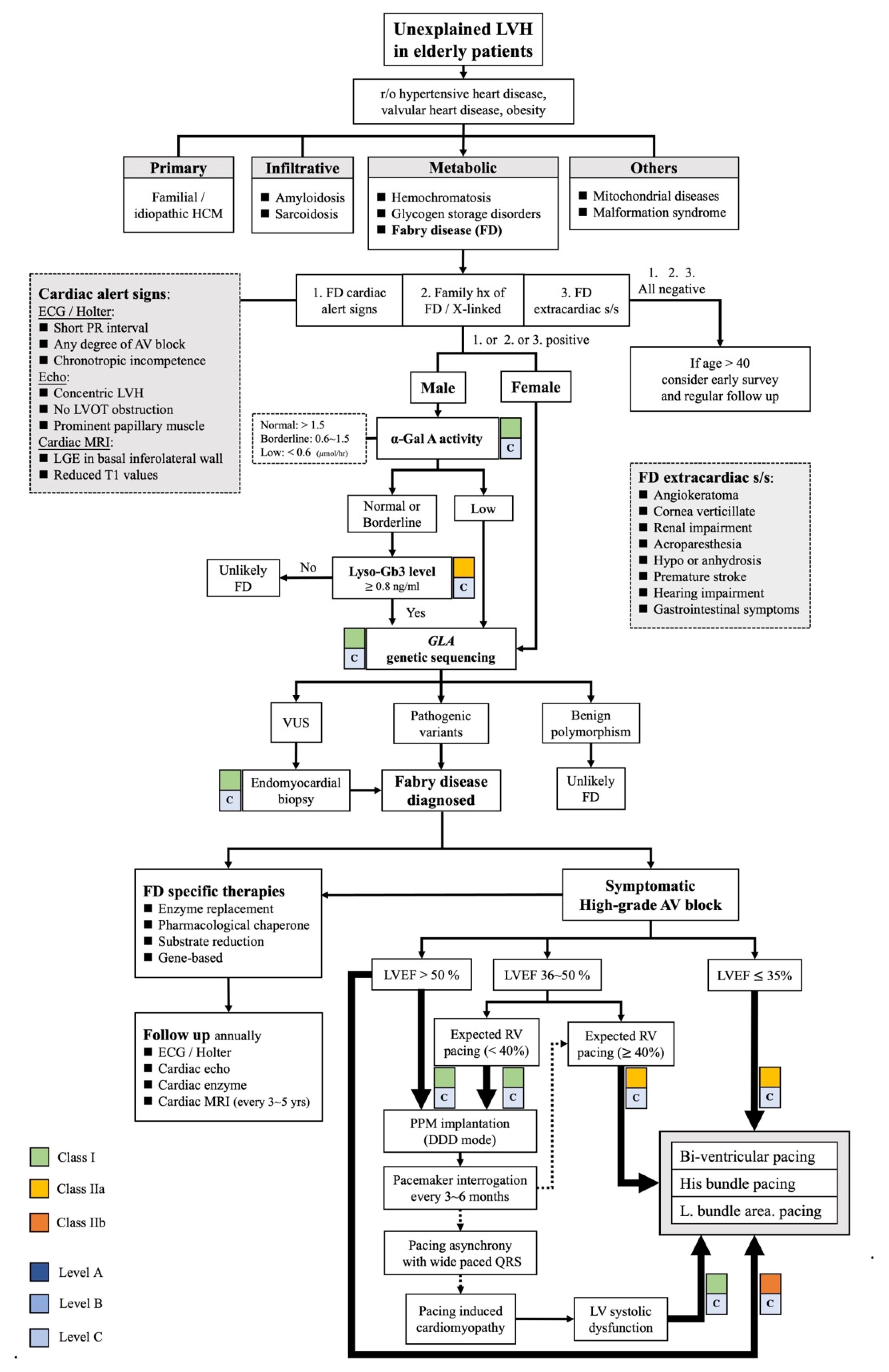
| Cardiac Imaging | Cardiac Alert Signs [4,13] |
| ECG | Short PR interval, AV block, chronotropic incompetence |
| 2D-Echocardiography | Concentric LVH, prominent papillary muscles, diastolic dysfunction |
| CMR | LGE in the basal inferolateral wall, reduced T1 values |
| Diagnostic examinations | Diagnostic criteria [3,4,7,12] |
| α-Gal A activity | N > 1.5, borderline: 0.6~1.5 (μmol/h) |
| Plasma Lyso-Gb3 | N < 0.8 (ng/mL) |
| Endomyocardial biopsy | General: diffuse vacuolization with lace-like appearance. The electron microscope: laminated lysosomal inclusions (zebra bodies), focal loss of myofilaments. |
| Genetic sequencing (Pathogenic variants) | Classical phenotype: more than 840 private mutations, e.g., p.R227X, p.R220X, p.R342X Late-onset phenotype: p.R301Q, p.R363H, p.F113L, p.N215S, IVS4+919G>A |
| Disease-specific therapies | Detailed information [4,14,15] |
| ERT | IV agalsidase alpha and beta (approved), pegunigalsidase alfa (ongoing trials) |
| Pharmacological chaperone | Oral Miglastat (approved) |
| SRT | Oral lucerastat, venglustat (ongoing trials) |
| Gene-based therapy | Gene transfer, mRNA (ongoing trials) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yu, T.-P.; Chen, J.-Y. Unexplained Left Ventricular Hypertrophy with Symptomatic High-Grade Atrioventricular Block in Elderly Patients: A Case Report. J. Clin. Med. 2022, 11, 3522. https://doi.org/10.3390/jcm11123522
Yu T-P, Chen J-Y. Unexplained Left Ventricular Hypertrophy with Symptomatic High-Grade Atrioventricular Block in Elderly Patients: A Case Report. Journal of Clinical Medicine. 2022; 11(12):3522. https://doi.org/10.3390/jcm11123522
Chicago/Turabian StyleYu, Tzu-Ping, and Ju-Yi Chen. 2022. "Unexplained Left Ventricular Hypertrophy with Symptomatic High-Grade Atrioventricular Block in Elderly Patients: A Case Report" Journal of Clinical Medicine 11, no. 12: 3522. https://doi.org/10.3390/jcm11123522