
Vascular Alterations Preceding Arterial Wall Thickening in Overweight and Obese Children

 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Subjects
2.2. Anthropometric Data
2.3. Laboratory Test
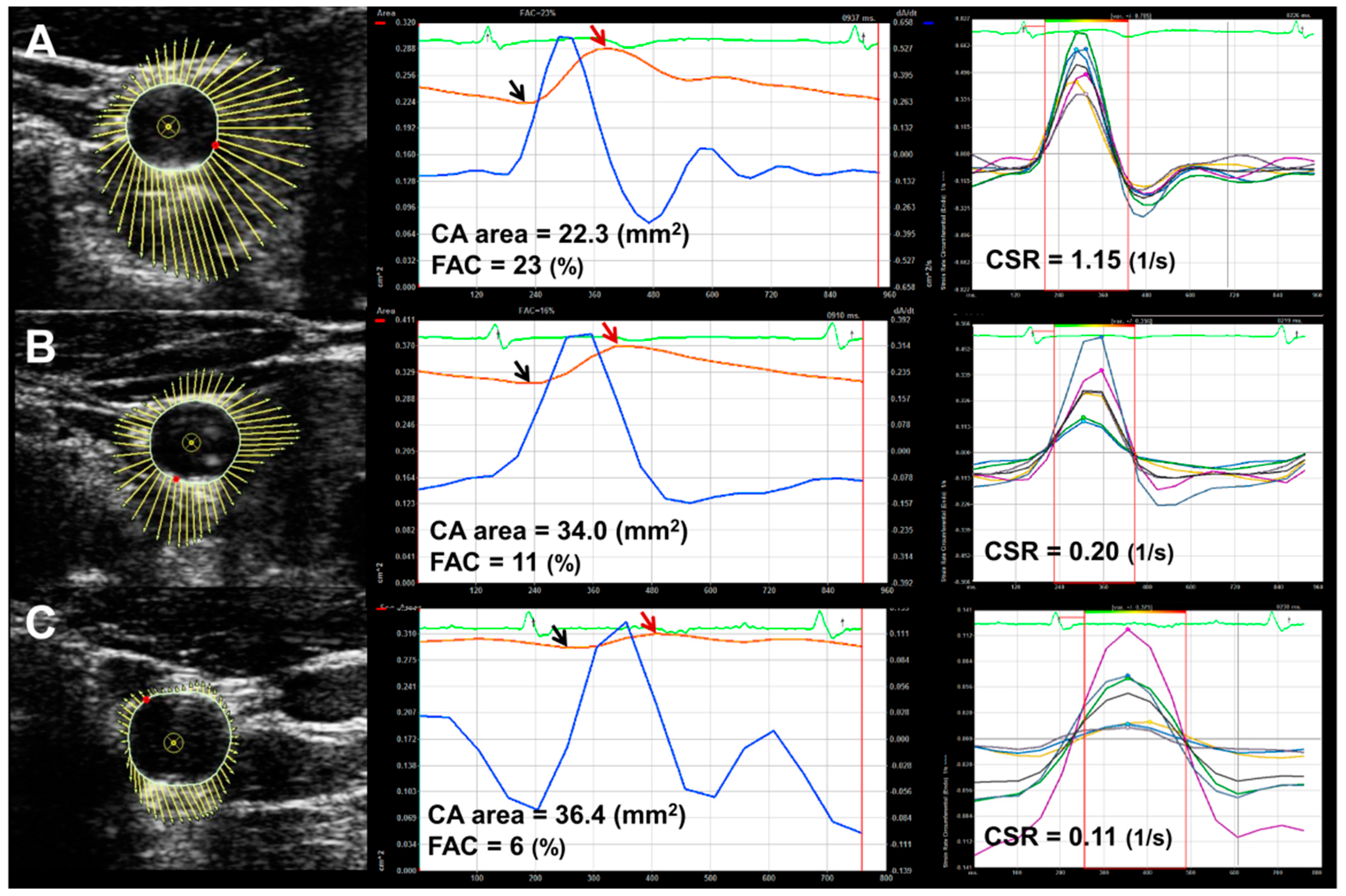
2.4. Carotid Ultrasound and Vascular Parameters
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kass, D.A. Ventricular arterial stiffening: Integrating the pathophysiology. Hypertension 2005, 46, 185–193. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salas, X.R.; Buoncristiano, M.; Williams, J.; Kebbe, M.; Spinelli, A.; Nardone, P.; Rito, A.; Duleva, V.; Milanović, S.M.; Kunesova, M.; et al. Parental Perceptions of Children’s Weight Status in 22 Countries: The WHO European Childhood Obesity Surveillance Initiative: COSI 2015/2017. Obes Facts 2021, 14, 658–674. [Google Scholar] [CrossRef] [PubMed]
- Franks, P.W.; Hanson, R.L.; Knowler, W.C.; Sievers, M.L.; Bennett, P.H.; Looker, H.C. Childhood obesity, other cardiovascu-lar risk factors, and premature death. N. Engl. J. Med. 2010, 362, 485–493. [Google Scholar] [CrossRef] [PubMed]
- Twig, G.; Yaniv, G.; Levine, H.; Leiba, A.; Goldberger, N.; Derazne, E.; Shor, D.B.-A.; Tzur, D.; Afek, A.; Shamiss, A.; et al. Body-Mass Index in 2.3 Million Adolescents and Cardiovascular Death in Adulthood. N. Engl. J. Med. 2016, 374, 2430–2440. [Google Scholar] [CrossRef] [PubMed]
- Freedman, D.S.; Dietz, W.H.; Tang, R.; Mensah, G.; Bond, M.G.; Urbina, E.M.; Srinivasan, S.; Berenson, G.S. The relation of obesity throughout life to carotid intima-media thickness in adulthood: The Bogalusa Heart Study. Int. J. Obes. 2003, 28, 159–166. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koskinen, J.; Kähönen, M.; Viikari, J.S.; Taittonen, L.; Laitinen, T.; Rönnemaa, T.; Lehtimäki, T.; Hutri-Kähönen, N.; Pie-tikäinen, M.; Jokinen, E.; et al. Conventional cardiovascular risk factors and metabolic syndrome in predicting carotid intima media thickness progression in young adults: The Cardiovascular Risk in Young Finns Study. Circulation 2009, 120, 229–236. [Google Scholar] [CrossRef] [PubMed]
- Juonala, M.; Magnussen, C.G.; Berenson, G.S.; Venn, A.; Burns, T.L.; Sabin, M.A.; Srinivasan, S.R.; Daniels, S.R.; Davis, P.H.; Chen, W.; et al. Childhood adiposity, adult adiposity, and cardiovascular risk factors. N. Engl. J. Med. 2011, 365, 1876–1885. [Google Scholar] [CrossRef] [Green Version]
- Lorenz, M.W.; Markus, H.S.; Bots, M.L.; Rosvall, M.; Sitzer, M. Prediction of clinical cardiovascular events with carotid inti-ma-media thickness: A systematic review and meta-analysis. Circulation 2007, 115, 459–467. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iannuzzi, A.; Licenziati, M.R.; Acampora, C.; Salvatore, V.; Auriemma, L.; Romano, M.L.; Panico, S.; Rubba, P.; Trevisan, M. Increased Carotid Intima-Media Thickness and Stiffness in Obese Children. Diabetes Care 2004, 27, 2506–2508. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lamotte, C.; Iliescu, C.; Libersa, C.; Gottrand, F. Increased intima-media thickness of the carotid artery in childhood: A systematic review of observational studies. Eur. J. Pediatr. 2011, 170, 719–729. [Google Scholar] [CrossRef] [PubMed]
- Tounian, P.; Aggoun, Y.; Dubern, B.; Varille, V.; Guy-Grand, B.; Sidi, D.; Girardet, J.-P.; Bonnet, D. Presence of increased stiffness of the common carotid artery and endothelial dysfunction in severely obese children: A prospective study. Lancet 2001, 358, 1400–1404. [Google Scholar] [CrossRef]
- Yilmazer, M.M.; Tavli, V.; Carti, U.; Mese, T.; Guven, B.; Aydın, B.; Devrim, I.; Tavli, T.; Tavlı, T.; Aydin, B. Cardiovascular risk factors and noninvasive assessment of arterial structure and function in obese Turkish children. Eur. J. Pediatr. 2010, 169, 1241–1248. [Google Scholar] [CrossRef]
- Whincup, P.H.; Gilg, J.A.; Donald, A.E.; Katterhorn, M.; Oliver, C.; Cook, D.G.; Deanfield, J.E. Arterial distensibility in adolescents: The influence of adiposity, the metabolic syndrome, and classic risk factors. Circulation 2005, 112, 1789–1797. [Google Scholar] [CrossRef]
- Dangardt, F.; Osika, W.; Volkmann, R.; Gan, L.M.; Friberg, P. Obese children show increased intimal wall thickness and de creased pulse wave velocity. Clin. Physiol. Funct. Imaging 2008, 28, 287–293. [Google Scholar] [CrossRef]
- Niboshi, A.; Hamaoka, K.; Sakata, K.; Inoue, F. Characteristics of brachial–ankle pulse wave velocity in Japanese children. Eur. J. Pediatr. 2006, 165, 625–629. [Google Scholar] [CrossRef]
- Kim, S.-A.; Lee, K.H.; Won, H.-Y.; Park, S.; Chung, J.H.; Jang, Y.; Ha, J.-W. Quantitative Assessment of Aortic Elasticity With Aging Using Velocity-Vector Imaging and Its Histologic Correlation. Arter. Thromb. Vasc. Biol. 2013, 33, 1306–1312. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, S.-A.; Park, S.-H.; Jo, S.-H.; Park, K.-H.; Kim, H.-S.; Han, S.-J.; Park, W.-J.; Ha, J.-W. Alterations of carotid arterial mechanics preceding the wall thickening in patients with hypertension. Atherosclerosis 2016, 248, 84–90. [Google Scholar] [CrossRef] [PubMed]
- Moon, J.S.; Lee, S.Y.; Nam, C.M.; Choi, J.M.; Choe, B.K.; Seo, J.W.; Oh, K.; Jang, M.J.; Hwang, S.S.; Yoo, M.H.; et al. 2007 Korean National Growth Charts: Review of developmental process and an outlook. Korean J. Pediatr. 2008, 51. [Google Scholar] [CrossRef]
- Styne, D.M.; Arslanian, S.A.; Connor, E.L.; Farooqi, I.S.; Murad, M.H.; Silverstein, J.H.; Yanovski, J.A. Pediatric Obesity-Assessment, Treatment, and Prevention: An Endocrine Society Clinical Practice Guideline. J. Clin. Endocrinol. Metab. 2017, 102, 709–757. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hayashi, K.; Handa, H.; Nagasawa, S.; Okumura, A.; Moritake, K. Stiffness and elastic behavior of human intracranial and extracranial arteries. J. Biomech. 1980, 13, 175–184. [Google Scholar] [CrossRef]
- O’Rourke, M. Arterial stiffness, systolic blood pressure, and logical treatment of arterial hypertension. Hypertension 1990, 15, 339–347. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Leary, D.H.; Polak, J.F.; Kronmal, R.A.; Manolio, T.A.; Burke, G.L.; Wolfson, S.K., Jr. Carotid-artery intima and media thickness as a risk factor for myocardial infarction and stroke in older adults. N. Engl. J. Med. 1999, 340, 14–22. [Google Scholar] [CrossRef] [PubMed]
- Park, J.; Kim, S.H.; Cho, G.Y.; Baik, I.; Kim, N.H.; Lim, H.E.; Kim, E.J.; Park, C.G.; Lim, S.Y.; Kim, Y.H.; et al. Obesity phenotype and cardiovascular changes. J. Hypertens. 2011, 29, 1765–1772. [Google Scholar] [CrossRef] [PubMed]
- Blaha, M.J.; Rivera, J.J.; Budoff, M.J.; Blankstein, R.; Agatston, A.; O’Leary, D.H.; Cushman, M.; Lakoski, S.; Criqui, M.H.; Szklo, M.; et al. Association between obesity, high-sensitivity c-reactive protein ≥ 2mg/L, and subclinical atherosclerosis: Implications of JUPITER from the Multi-Ethnic Study of Atherosclerosis. Arteriosclerosis, thrombosis. Vasc. Biol. 2011, 31, 1430–1438. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reed, D.; Dwyer, K.M.; Dwyer, J.H. Abdominal obesity and carotid artery wall thickness. The Los Angeles Atherosclerosis Study. Int. J. Obes. 2003, 27, 1546–1551. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Juonala, M.; Raitakari, M.; Viikari, J.S.; Raitakari, O.T. Obesity in youth is not an independent predictor of carotid IMT in adulthood: The Cardiovascular Risk in Young Finns Study. Atherosclerosis 2006, 185, 388–393. [Google Scholar] [CrossRef] [PubMed]
- Freedman, D.S.; Patel, D.A.; Srinivasan, S.R.; Chen, W.; Tang, R.; Bond, M.G.; Berenson, G.S. The contribution of childhood obesity to adult carotid intima-media thick ness: The Bogalusa Heart Study. Int. J. Obes. 2008, 32, 749–756. [Google Scholar] [CrossRef] [Green Version]
- Ayer, J.G.; Harmer, J.A.; Nakhla, S.; Xuan, W.; Ng, M.K.; Raitakari, O.T.; Marks, G.B.; Celermajer, D.S. HDL-Cholesterol, Blood Pressure, and Asymmetric Dimethylarginine Are Significantly Associated With Arterial Wall Thickness in Children. Arter. Thromb. Vasc. Biol. 2009, 29, 943–949. [Google Scholar] [CrossRef]
- Geerts, C.C.; Evelein, A.M.; Bots, M.L.; van der Ent, C.K.; Grobbee, D.E.; Uiterwaal, C.S. Body fat distribution and early arterial changes in healthy 5-year-old children. Ann. Med. 2012, 44, 350–359. [Google Scholar] [CrossRef] [PubMed]
- Whincup, P.H.; Nightingale, C.M.; Rapala, A.; Joysurry, D.; Prescott, M.; Donald, A.E.; Ellins, E.; Donin, A.; Masi, S.; Owen, C.G.; et al. 66 Ethnic differences in carotid intimal medial thickness and carotid-femoral pulse wave velocity are present in UK children. Heart 2011, 97, A41. [Google Scholar] [CrossRef] [Green Version]
- Elkiran, O.; Yilmaz, E.; Koc, M.; Kamanli, A.; Ustundag, B.; Ilhan, N. The association between intima media thickness, central obesity and diastolic blood pressure in obese and owerweight children: A cross-sectional school-based study. Int. J. Cardiol. 2013, 165, 528–532. [Google Scholar] [CrossRef] [PubMed]
- Ozguven, I.; Ersoy, B.; Ozguven, A.; Ozkol, M.; Onur, E. Factors affecting carotid intima media thickness predicts early atherosclerosis in overweight and obese adolescents. Obesity Res. Clin. Pract. 2010, 4, e1–e82. [Google Scholar] [CrossRef] [PubMed]
- Caserta, C.A.; Pendino, G.M.; Alicante, S.; Amante, A.; Amato, F.; Fiorillo, M.; Messineo, A.; Polito, I.; Surace, M.; Surace, P.; et al. Body Mass Index, Cardiovascular Risk Factors, and Carotid Intima-Media Thickness in a Pediatric Population in Southern Italy. J. Pediatr. Gastroenterol. Nutr. 2010, 51, 216–220. [Google Scholar] [CrossRef] [PubMed]
- Woo, K.S.; Chook, P.; Yu, C.; Sung, R.Y.T.; Qiao, M.; Leung, S.S.F.; Lam, C.W.K.; Metreweli, C.; Celermajer, D.S. Overweight in children is associated with arterial endothelial dysfunction and intima-media thickening. Int. J. Obes. 2004, 28, 852–857. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Urbina, E. Noninvasive assessment of target organ injury in children with the metabolic syndrome. J. CardioMetabolic Syndr. 2006, 1, 277–281. [Google Scholar] [CrossRef] [Green Version]
- Gao, Z.; Khoury, P.R.; McCoy, C.E.; Shah, A.S.; Kimball, T.R.; Dolan, L.M.; Urbina, E.M. Adiposity has no direct effect on carotid intima-media thickness in adolescents and young adults: Use of structural equation modeling to elucidate indirect & direct pathways. Atherosclerosis 2015, 246, 29–35. [Google Scholar] [CrossRef] [Green Version]
- Osiniri, I.; Sitjar, C.; Soriano-Rodríguez, P.; Prats-Puig, A.; Casas-Satre, C.; Mayol, L.; de Zegher, F.; Ibánez, L.; Bassols, J.; López-Bermejo, A. Carotid Intima-Media Thickness at 7 Years of Age: Relationship to C-Reactive Protein Rather than Adiposity. J. Pediatr. 2012, 160, 276–280.e1. [Google Scholar] [CrossRef]
- Giannattasio, C.; Failla, M.; Capra, A.; Scanziani, E.; Amigoni, M.; Boffi, L.; Whistock, C.; Gamba, P.; Paleari, F.; Mancia, G. Increased Arterial Stiffness in Normoglycemic Normotensive Offspring of Type 2 Diabetic Parents. Hypertension 2008, 51, 182–187. [Google Scholar] [CrossRef] [Green Version]
- Aronson, D. Cross-linking of glycated collagen in the pathogenesis of arterial and myocardial stiffening of aging and diabetes. J. Hypertens. 2003, 21, 3–12. [Google Scholar] [CrossRef]
- Ozcetin, M.; Celikyay, Z.R.; Celik, A.; Yilmaz, R.; Yerli, Y.; Erkorkmaz, U. The importance of carotid artery stiffness and in-creased intima-media thickness in obese children. S. Afr. Med. J. 2012, 102, 295–299. [Google Scholar] [CrossRef] [Green Version]
- Şen, H.; Bakiler, A.R.; Aydoğdu, S.A.; Ünüvar, T.; Yenisey, Ç.; Özer, E.A. The mechanical properties and stiffness of aorta in obese children. Turk. J. Pediatr. 2013, 55, 309–314. [Google Scholar] [PubMed]
- Charakida, M.; Jones, A.; Falaschetti, E.; Khan, T.; Finer, N.; Sattar, N.; Hingorani, A.; Lawlor, D.A.; Smith, G.D.; Deanfield, J.E. Childhood Obesity and Vascular Phenotypes: A Population Study. J. Am. Coll. Cardiol. 2012, 60, 2643–2650. [Google Scholar] [CrossRef] [PubMed]
- Fonck, E.; Prod’Hom, G.; Roy, S.; Augsburger, L.; Rufenacht, D.A.; Stergiopulos, N. Effect of elastin degradation on carotid wall mechanics as assessed by a constituent-based biomechanical model. Am. J. Physiol. Circ. Physiol. 2007, 292, H2754–H2763. [Google Scholar] [CrossRef] [Green Version]
- Eberth, J.; Gresham, V.C.; Reddy, A.K.; Popovic, N.; Wilson, E.; Humphrey, J.D. Importance of pulsatility in hypertensive carotid artery growth and remodeling. J. Hypertens. 2009, 27, 2010–2021. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Normal Weight | Over Weight | Obese | p Value | |
|---|---|---|---|---|
| Age, year | 10.5 ± 2.4 | 10.5 ± 2.0 | 10.8 ± 2.1 | 0.685 |
| Male, % | 58 | 53 | 59 | 0.840 |
| Height, cm | 143 ± 13 | 145 ± 10 | 152 ± 12 **,‡ | <0.001 |
| Weight, kg | 38.2 ± 11.8 | 49.9 ± 10.2 ** | 68.7 ± 18.1 **,‡ | <0.001 |
| BMI, kg/m2 | 18.0 ± 2.4 | 23.3 ± 1.8 ** | 28.9 ± 4.1 **,‡ | <0.001 |
| BMI z-score | −0.13 ± 0.76 | 1.45 ± 0.17 ** | 2.38 ± 0.44 **,‡ | <0.001 |
| WC, cm | 60.0 ± 7.3 | 74.7 ± 7.2 ** | 89.3 ± 10.6 **,‡ | <0.001 |
| HC, cm | 78.3 ± 7.9 | 87.0 ± 6.7 ** | 98.3 ± 10.4 **,‡ | <0.001 |
| Systolic BP, mmHg | 104 ± 11 | 107 ± 8.7 | 114 ± 9.6 **,‡ | <0.001 |
| Diastolic BP, mmHg | 60 ± 6.0 | 63 ± 6.0 | 65 ± 8.0 ** | 0.003 |
| Mean BP, mmHg | 75 ± 6.8 | 78 ± 5.8 | 82 ± 7.5 **,† | <0.001 |
| Heart rate, bpm | 80 ± 11 | 79 ± 10 | 80 ± 12 | 0.909 |
| Hemoglobin, mg/dL | 13.9 ± 0.9 | 13.9 ± 0.8 | 13.7 ± 0.8 | 0.477 |
| Creatinine, mg/dL | 0.55 ± 0.13 | 0.53 ± 0.06 | 0.54 ± 0.10 | 0.729 |
| Glucose, mg/dL | 82 ± 10 | 86 ± 9.9 | 88 ± 7.6 ** | 0.001 |
| AST, IU/L | 27 ± 23 | 23 ± 8.5 | 27 ± 18 | 0.446 |
| ALT, IU/L | 16 ± 18 | 21 ± 21 | 37 ± 40 * | 0.003 |
| HOMA-IR | 1.35 ± 0.75 | 2.89 ± 1.80 ** | 4.80 ± 2.79 **,‡ | <0.001 |
| hsCRP, mg/dL | 0.47 ± 0.31 | 0.94 ± 0.83 | 2.17 ± 2.11 **,‡ | <0.001 |
| TG, mg/dL | 78 ± 38 | 104 ± 51 | 114 ± 56 ** | 0.002 |
| HDL-C, mg/dL | 60 ± 13 | 56 ± 14 | 49 ± 11 **,‡ | <0001 |
| LDL-C, mg/dL | 94 ± 20 | 105 ± 23 | 110 ± 25 ** | 0.003 |
| Adiponectin, ug/mL | 10.2 ± 4.0 | 9.4 ± 4.1 | 8.4 ± 3.2 ** | 0.012 |
| Normal Weight | Over Weight | Obese | p Value | |
|---|---|---|---|---|
| M-mode-derived parameters | ||||
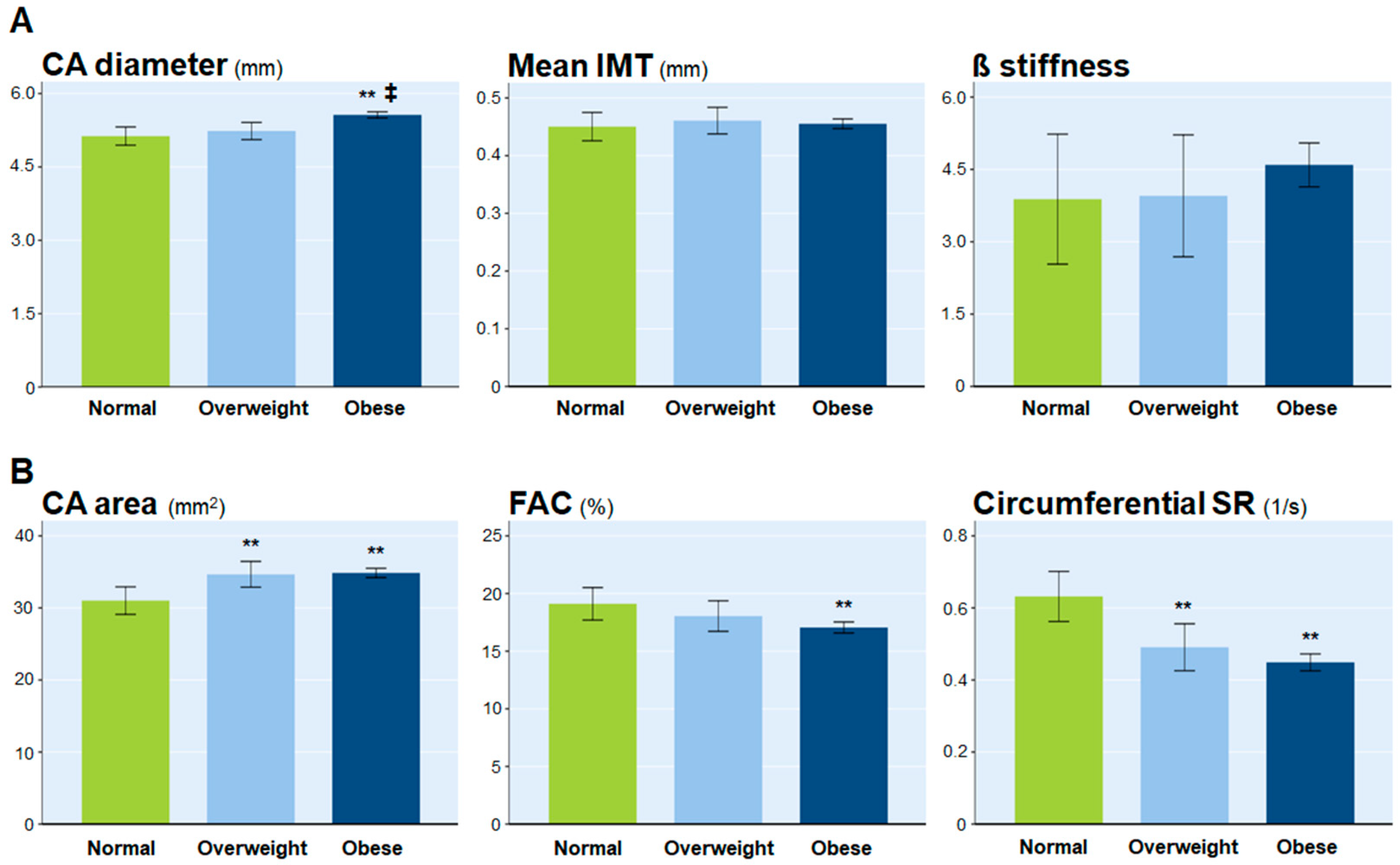
| Mean IMT, mm | 0.44 ± 0.04 | 0.45 ± 0.05 | 0.45 ± 0.06 | 0.277 |
| CA diameter, mm | 5.05 ± 0.49 | 5.16 ± 0.51 | 5.58 ± 0.53 **,‡ | <0.001 |
| ß stiffness | 4.15 ± 1.30 | 4.13 ± 1.77 | 4.53 ± 3.77 | 0.735 |
| YEM, 102 × kPa/mm | 5.45 ± 1.65 | 5.51 ± 2.44 | 6.34 ± 5.05 ‡ | 0.443 |
| VVI parameters | ||||
| CA area, mm2 | 30.3 ± 5.0 | 34.0 ± 5.1 * | 35.0 ± 5.6 ** | <0.001 |
| FAC, % | 19.1 ± 4.2 | 17.9 ± 3.3 | 17.0 ± 3.6 ** | 0.007 |
| Circumferential strain, % | 6.50 ± 2.45 | 5.74 ± 1.64 | 5.67 ± 1.94 | 0.090 |
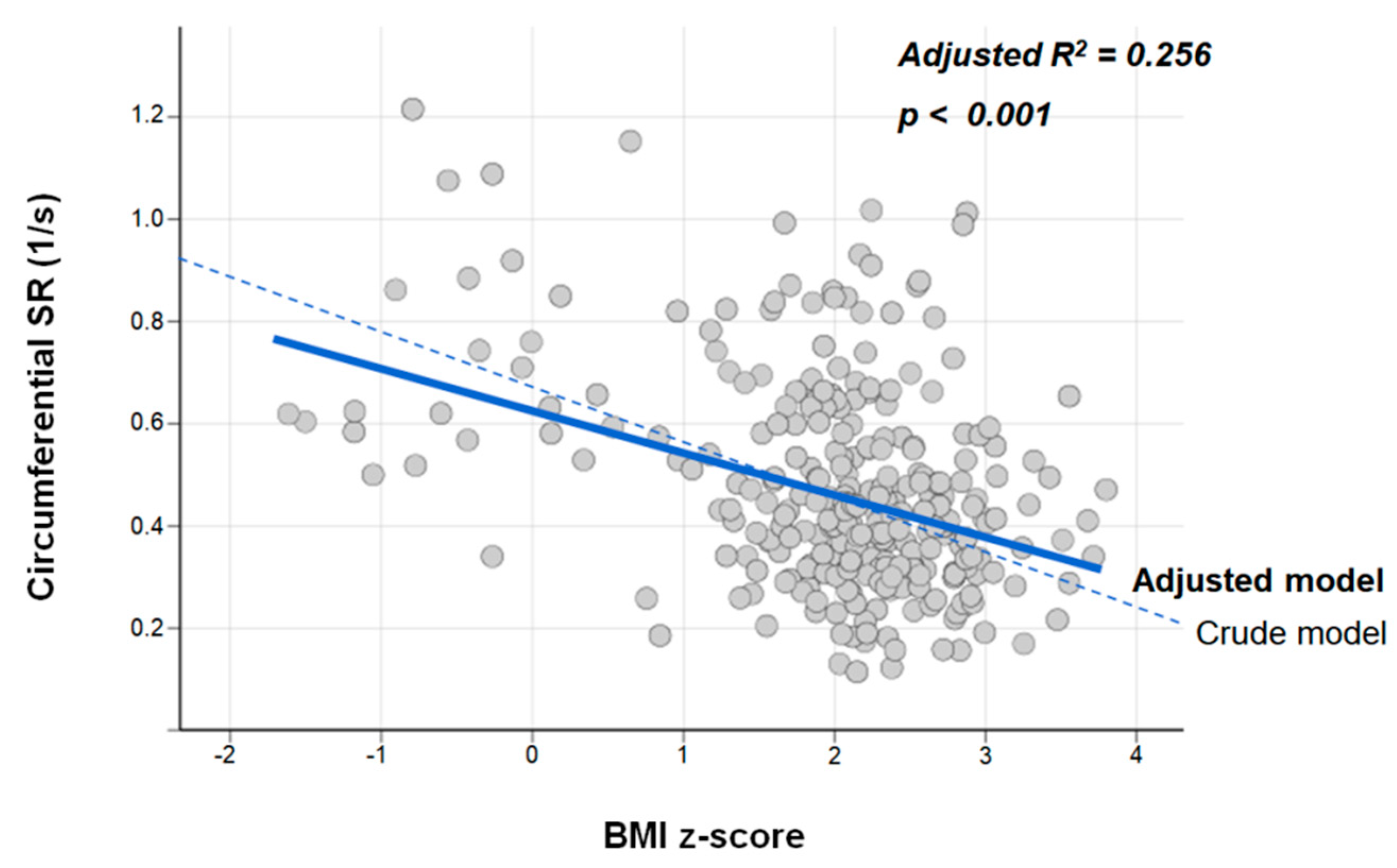
| Circumferential SR, 1/s | 0.68 ± 0.24 | 0.51 ± 0.21 ** | 0.44 ± 0.18 ** | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, S.-A.; Park, K.H.; Woo, S.; Kim, Y.M.; Lim, H.J.; Park, W.-J. Vascular Alterations Preceding Arterial Wall Thickening in Overweight and Obese Children. J. Clin. Med. 2022, 11, 3520. https://doi.org/10.3390/jcm11123520
Kim S-A, Park KH, Woo S, Kim YM, Lim HJ, Park W-J. Vascular Alterations Preceding Arterial Wall Thickening in Overweight and Obese Children. Journal of Clinical Medicine. 2022; 11(12):3520. https://doi.org/10.3390/jcm11123520
Chicago/Turabian StyleKim, Sung-Ai, Kyung Hee Park, Sarah Woo, Yoon Myung Kim, Hyun Jung Lim, and Woo-Jung Park. 2022. "Vascular Alterations Preceding Arterial Wall Thickening in Overweight and Obese Children" Journal of Clinical Medicine 11, no. 12: 3520. https://doi.org/10.3390/jcm11123520