
Magnesium Sulfate and Cerebral Oxygen Saturation in Mild Traumatic Brain Injury: A Randomized, Double-Blind, Controlled Trial

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study
2.2. Patients
2.3. Anesthesia and Monitoring
2.4. Intervention Protocol
2.5. Assessment of Outcomes
2.6. Sample Size Calculation
2.7. Statistical Analysis
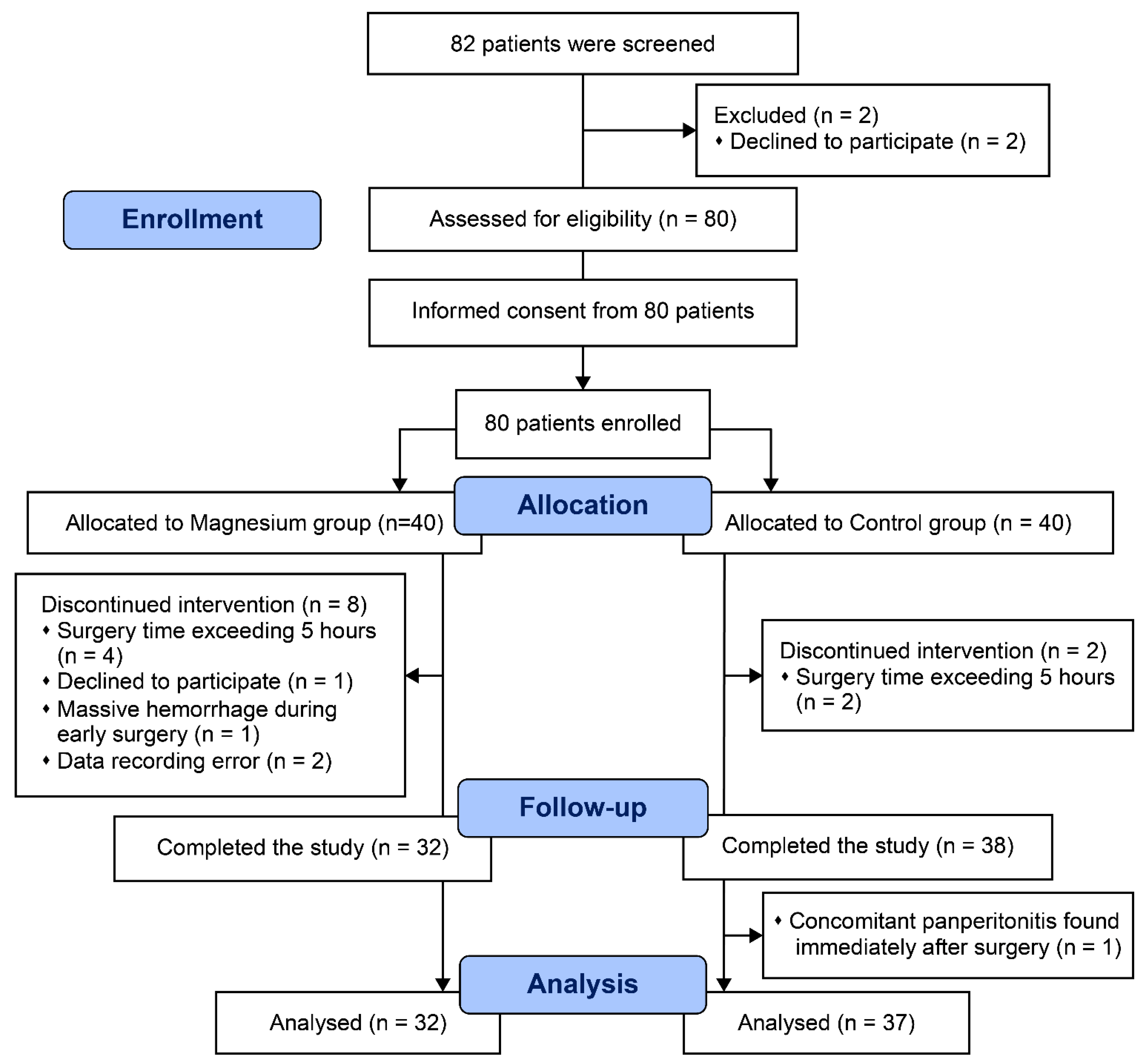
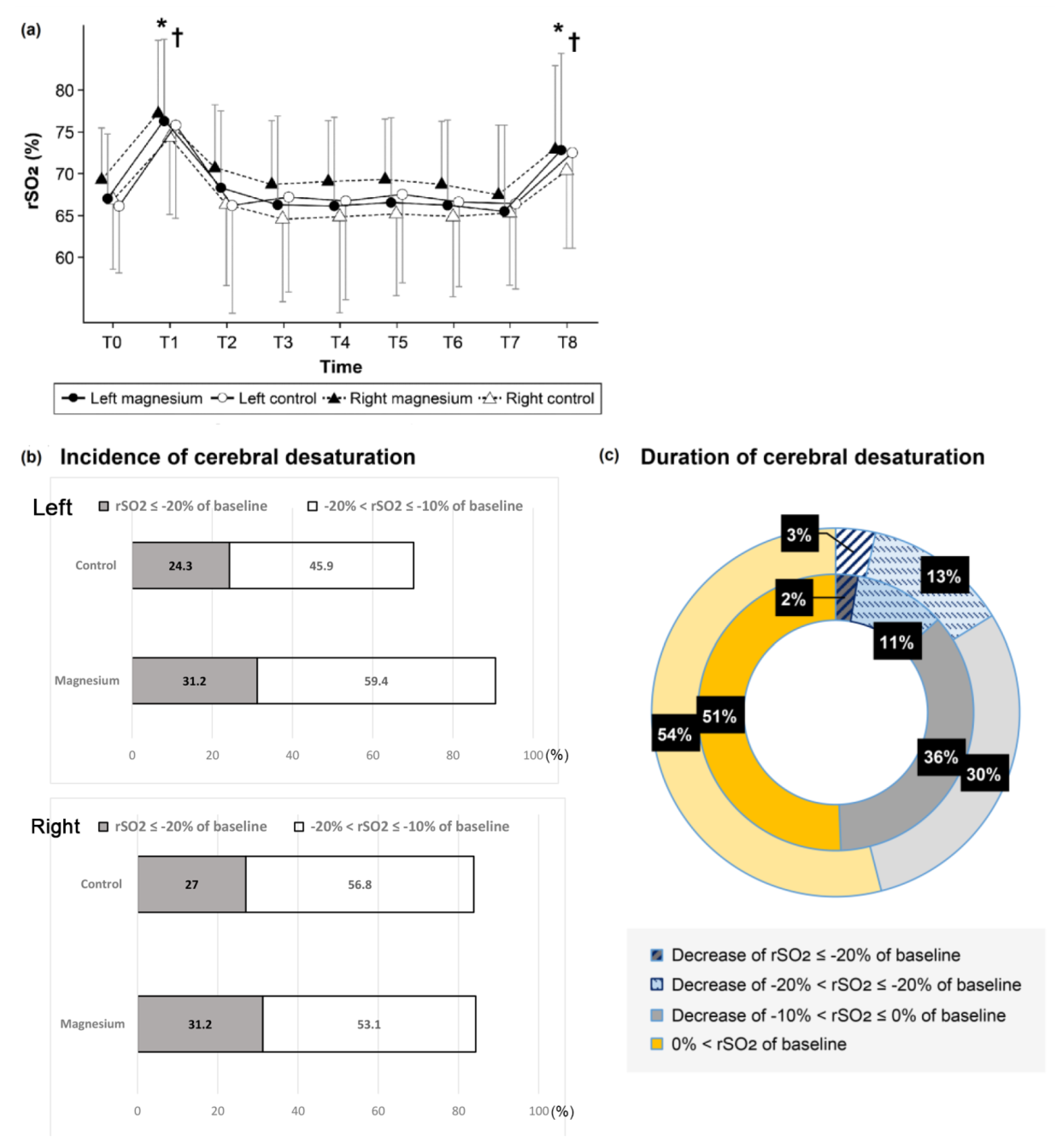
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Werner, C.; Engelhard, K. Pathophysiology of traumatic brain injury. Br. J. Anaesth. 2007, 99, 4–9. [Google Scholar] [CrossRef] [PubMed]
- Mathieu, F.; Khellaf, A.; Ku, J.C.; Donnelly, J.; Thelin, E.P.; Zeiler, F.A. Continuous near-infrared spectroscopy monitoring in adult traumatic brain injury: A systematic review. J. Neurosurg. Anesthesiol. 2020, 32, 288–299. [Google Scholar] [CrossRef] [PubMed]
- Nelson, L.D.; Temkin, N.R.; Dikmen, S.; Barber, J.; Giacino, J.T.; Yuh, E.; Levin, H.S.; McCrea, M.A.; Stein, M.B.; Mukherjee, P.; et al. Recovery after mild traumatic brain injury in patients presenting to US level I trauma centers: A transforming research and clinical knowledge in traumatic brain injury (TRACK-TBI) study. JAMA Neurol. 2019, 76, 1049–1059. [Google Scholar] [CrossRef] [PubMed]
- Curry, P.; Viernes, D.; Sharma, D. Perioperative management of traumatic brain injury. Int. J. Crit. Illn. Inj. Sci. 2011, 1, 27–35. [Google Scholar]
- Lumba-Brown, A.; Yeates, K.O.; Sarmiento, K.; Breiding, M.J.; Haegerich, T.M.; Gioia, G.A.; Turner, M.; Benzel, E.C.; Suskauer, S.J.; Giza, C.C.; et al. Centers for Disease Control and Prevention guideline on the diagnosis and management of mild traumatic brain injury among children. JAMA Pediatr. 2018, 172, e182853. [Google Scholar] [CrossRef]
- Silverberg, N.D.; Duhaime, A.C.; Iaccarino, M.A. Mild traumatic brain injury in 2019–2020. JAMA 2020, 323, 177–178. [Google Scholar] [CrossRef]
- Albrecht, E.; Kirkham, K.R.; Liu, S.S.; Brull, R. Peri-operative intravenous administration of magnesium sulphate and postoperative pain: A meta-analysis. Anaesthesia 2013, 68, 79–90. [Google Scholar] [CrossRef]
- Do, S.H. Magnesium: A versatile drug for anesthesiologists. Korean J. Anesthesiol. 2013, 65, 4–8. [Google Scholar] [CrossRef]
- Sohn, H.M.; Jheon, S.H.; Nam, S.; Do, S.H. Magnesium sulphate improves pulmonary function after video-assisted thoracoscopic surgery: A randomised double-blind placebo-controlled study. Eur. J. Anaesthesiol. 2017, 34, 508–514. [Google Scholar] [CrossRef]
- Chang, J.J.; Mack, W.J.; Saver, J.L.; Sanossian, N. Magnesium: Potential roles in neurovascular disease. Front. Neurol. 2014, 5, 52. [Google Scholar] [CrossRef]
- Kemp, P.A.; Gardiner, S.M.; March, J.E.; Rubin, P.C.; Bennett, T. Assessment of the effects of endothelin-1 and magnesium sulphate on regional blood flows in conscious rats, by the coloured microsphere reference technique. Br. J. Pharmacol. 1999, 126, 621–626. [Google Scholar] [CrossRef]
- Arango, M.F.; Bainbridge, D. Magnesium for acute traumatic brain injury. Cochrane Database Syst. Rev. 2008, 4, CD005400. [Google Scholar] [CrossRef]
- Iseri, L.T.; French, J.H. Magnesium: Nature’s physiologic calcium blocker. Am. Heart J. 1984, 108, 188–193. [Google Scholar] [CrossRef]
- Temkin, N.R.; Anderson, G.D.; Winn, H.R.; Ellenbogen, R.G.; Britz, G.W.; Schuster, J.; Lucas, T.; Newell, D.W.; Mansfield, P.N.; Machamer, J.E.; et al. Magnesium sulfate for neuroprotection after traumatic brain injury: A randomised controlled trial. Lancet Neurol. 2007, 6, 29–38. [Google Scholar] [CrossRef]
- Vink, R.; McIntosh, T.K.; Demediuk, P.; Weiner, M.W.; Faden, A.I. Decline in intracellular free Mg2+ is associated with irreversible tissue injury after brain trauma. J. Biol. Chem. 1988, 263, 757–761. [Google Scholar] [CrossRef]
- Lozada-Martinez, I.D.; Padilla-Durán, T.J.; González-Monterroza, J.J.; Aguilar-Espinosa, D.A.; Molina-Perea, K.N.; Camargo-Martinez, W.; Llamas-Medrano, L.; Hurtado-Pinillos, M.; Guerrero-Mejía, A.; Janjua, T.; et al. Basic considerations on magnesium in the management of neurocritical patients. J. Neurocrit. Care 2021, 14, 78–87. [Google Scholar] [CrossRef]
- Behrouz, R.; Hafeez, S.; Mutgi, S.A.; Zakaria, A.; Miller, C.M. Hypomagnesemia in intracerebral hemorrhage. World Neurosurg. 2015, 84, 1929–1932. [Google Scholar] [CrossRef]
- Weigl, W.; Milej, D.; Janusek, D.; Wojtkiewicz, S.; Sawosz, P.; Kacprzak, M.; Gerega, A.; Maniewski, R.; Liebert, A. Application of optical methods in the monitoring of traumatic brain injury: A review. J. Cereb. Blood Flow Metab. 2016, 36, 1825–1843. [Google Scholar]
- Deschamps, A.; Hall, R.; Grocott, H.; Mazer, C.D.; Choi, P.T.; Turgeon, A.F.; de Medicis, E.; Bussières, J.S.; Hudson, C.; Syed, S.; et al. Cerebral oximetry monitoring to maintain normal cerebral oxygen saturation during high-risk cardiac surgery: A randomized controlled feasibility trial. Anesthesiology 2016, 124, 826–836. [Google Scholar] [CrossRef]
- Stocchetti, N.; Zanier, E.R. Chronic impact of traumatic brain injury on outcome and quality of life: A narrative review. Crit. Care 2016, 20, 148. [Google Scholar] [CrossRef]
- Hogue, C.W.; Levine, A.; Hudson, A.; Lewis, C. Clinical applications of near-infrared spectroscopy monitoring in cardiovascular surgery. Anesthesiology 2021, 134, 784–791. [Google Scholar] [CrossRef] [PubMed]
- Goyal, N.; Tsivgoulis, G.; Malhotra, K.; Houck, A.L.; Khorchid, Y.M.; Pandhi, A.; Inoa, V.; Alsherbini, K.; Alexandrov, A.V.; Arthur, A.S.; et al. Serum magnesium levels and outcomes in patients with acute spontaneous intracerebral hemorrhage. J. Am. Heart Assoc. 2018, 7, e008698. [Google Scholar] [CrossRef] [PubMed]
- Sen, A.P.; Gulati, A. Use of magnesium in traumatic brain injury. Neurotherapeutics 2010, 7, 91–99. [Google Scholar] [CrossRef] [PubMed]
- Polderman, K.H.; Bloemers, F.W.; Peerdeman, S.M.; Girbes, A.R. Hypomagnesemia and hypophosphatemia at admission in patients with severe head injury. Crit. Care Med. 2000, 28, 2022–2025. [Google Scholar] [CrossRef]
- Heath, D.L.; Vink, R. Improved motor outcome in response to magnesium therapy received up to 24 h after traumatic diffuse axonal brain injury in rats. J. Neurosurg. 1999, 90, 504–509. [Google Scholar] [CrossRef]
- Jo, Y.Y.; Shim, J.K.; Soh, S.; Suh, S.; Kwak, Y.L. Association between cerebral oxygen saturation with outcome in cardiac surgery: Brain as an index organ. J. Clin. Med. 2020, 9, 840. [Google Scholar] [CrossRef]
- Davie, S.; Mutch, W.A.C.; Monterola, M.; Fidler, K.; Funk, D.J. The incidence and magnitude of cerebral desaturation in traumatic brain injury: An observational cohort study. J. Neurosurg. Anesthesiol. 2021, 33, 258–262. [Google Scholar] [CrossRef]
- Subramanian, B.; Nyman, C.; Fritock, M.; Klinger, R.Y.; Sniecinski, R.; Roman, P.; Huffmyer, J.; Parish, M.; Yenokyan, G.; Hogue, C.W. A multicenter pilot study assessing regional cerebral oxygen desaturation frequency during cardiopulmonary bypass and responsiveness to an intervention algorithm. Anesth. Analg. 2016, 122, 1786–1793. [Google Scholar] [CrossRef]
- Anastasian, Z.H. Anaesthetic management of the patient with acute ischaemic stroke. Br. J. Anaesth. 2014, 113 (Suppl. 2), ii9–ii16. [Google Scholar] [CrossRef]
- Gardner, C.J.; Lee, K. Hyperperfusion syndromes: Insight into the pathophysiology and treatment of hypertensive encephalopathy. CNS Spectr. 2007, 12, 35–42. [Google Scholar] [CrossRef]
- Sohn, H.M.; Kim, B.Y.; Bae, Y.K.; Seo, W.S.; Jeon, Y.T. Magnesium sulfate enables patient immobilization during moderate block and ameliorates the pain and analgesic requirements in spine surgery, which can not be achieved with opioid-only protocol: A randomized double-blind placebo-controlled study. J. Clin. Med. 2021, 10, 4289. [Google Scholar] [CrossRef]
- Gan, T.J. Poorly controlled postoperative pain: Prevalence, consequences, and prevention. J. Pain Res. 2017, 10, 2287–2298. [Google Scholar] [CrossRef]
- Loftus, R.W.; Yeager, M.P.; Clark, J.A.; Brown, J.R.; Abdu, W.A.; Sengupta, D.K.; Beach, M.L. Intraoperative ketamine reduces perioperative opiate consumption in opiate-dependent patients with chronic back pain undergoing back surgery. Anesthesiology 2010, 113, 639–646. [Google Scholar] [CrossRef]
- Bohl, D.D.; Louie, P.K.; Shah, N.; Mayo, B.C.; Ahn, J.; Kim, T.D.; Massel, D.H.; Modi, K.D.; Long, W.W.; Buvanendran, A.; et al. Multimodal versus patient-controlled analgesia after an anterior cervical decompression and fusion. Spine 2016, 41, 994–998. [Google Scholar] [CrossRef]
- Rodriguez-Rubio, L.; Nava, E.; Del Pozo, J.S.G.; Jordan, J. Influence of the perioperative administration of magnesium sulfate on the total dose of anesthetics during general anesthesia. a systematic review and meta-analysis. J. Clin. Anesth. 2017, 39, 129–138. [Google Scholar] [CrossRef]
- Vilke, A.; Bilskiene, D.; Saferis, V.; Gedminas, M.; Bieliauskaitė, D.; Tamašauskas, A.; Macas, A. Predictive value of early near-infrared spectroscopy monitoring of patients with traumatic brain injury. Medicina 2014, 50, 263–268. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Magnesium Group (n = 32) | Control Group (n = 37) | p Value | |
|---|---|---|---|
| Sex (Male/Female) | 25/7 | 32/5 | 0.361 |
| Age (year) | 49.5 ± 15.2 | 50.1 ± 14.9 | 0.879 |
| Height (cm) | 168.5 ± 7.2 | 167.9 ± 8.1 | 0.749 |
| Weight (kg) | 71.9 ± 11.6 | 69.9 ± 11.4 | 0.479 |
| ASA (I/II/III) | 3/18/11 | 3/28/6 | 0.211 |
| Mechanism of Injury, n (%) | 0.642 | ||
| Fall | 11 (34.4%) | 11 (29.7%) | |
| Transportation accident | 20 (62.5%) | 26 (70.3%) | |
| Explosion | 1 (3.1%) | 0 (0%) | |
| Days after injury (days) (range) | 4.5 ± 3.7 (6 h–13 day) | 5.1 ± 4.7 (6 h–21 day) | 0.569 |
| Surgery, Orthopedic | 0.315 | ||
| Upper extremity | 11 (34.4%) | 9 (24.3%) | |
| Lower extremity | 12 (37.5%) | 15 (40.5%) | |
| Hip | 4 (12.5%) | 4 (10.8%) | |
| Other parts | 4 (12.5%) | 6 (16.2%) | |
| Combined op | 1 (3.1%) | 3 (8.1%) | |
| Magnesium at admission (normal range: 1.6–2.6) (mg/dL) | 1.96 ± 0.41 | 2.03 ± 0.20 | 0.361 |
| Duration of surgery (min) | 81.1 ± 43.0 | 99.6 ± 63.3 | 0.167 |
| Duration of anesthesia (min) | 126.4 ± 49.0 | 143.1 ± 66.7 | 0.247 |
| Aldrete score * | 10 (n = 20) | 10 (n = 25) | |
| PACU stay time (min) * | 34.6 ± 7.7 (n = 20) | 37.8 ± 9.9 (n = 25) | 0.239 |
| Magnesium Group (n = 32) | Control Group (n = 37) | p Value | |
|---|---|---|---|
| TBI, Symptom, n (%) | |||
| Loss of consciousness at the time of injury | 24 (75.0%) | 33 (89.2%) | 0.121 |
| Headache | 6 (18.8%) | 8 (21.6%) | 0.767 |
| Dizziness | 3 (9.4%) | 6 (16.2%) | 0.489 |
| Nausea/vomiting | 5 (15.6%) | 5 (13.5%) | 0.804 |
| Memory impairment | 5 (15.6%) | 6 (16.2%) | 0.947 |
| Sleeping tendency | 10 (31.3%) | 13 (35.1%) | 0.733 |
| TBI, Severity, n (%) immediately before surgery | |||
| Mild (GCS 15/14) | 31/1 | 34/3 | 0.618 |
| Moderate | 0 | 0 | |
| Severe | 0 | 0 | |
| Brain CT, n (%) * | |||
| Subarachnoid hemorrhage | 8 (25.0%) | 5 (13.5%) | 0.224 |
| Subdural hemorrhage | 6 (18.8%) | 4 (10.8%) | 0.350 |
| Epidural hemorrhage | 4 (12.5%) | 2 (5.4%) | 0.349 |
| Intracerebral hemorrhage | 0 (0%) | 1 (2.7%) | 0.279 |
| Cerebral Contusion | 2 (6.3%) | 4 (10.8%) | 0.503 |
| Skull fracture | 7 (21.9%) | 3 (8.1%) | 0.105 |
| Scalp/soft tissue swelling | 8 (25.0%) | 14 (37.8%) | 0.254 |
| Midline shift > 5 mm, n (%) | 0 | 0 | |
| The others | 4 (12.5%) | 3 (8.1%) | 0.547 |
| No intracranial hemorrhage or bony skull fracture | 16 (50.5%) | 17 (51.5%) | 0.737 |
| TBI site (Left/Right/Both/non-specific/none) | (3/9/4/0/16) | (4/4/4/8/17) | |
| Preoperative antiepileptic prescription | 10 (31.3%) | 6 (16.2%) | 0.140 |
| GCS at the time of entering trauma-bay | 14.16 ± 2.02 | 14.62 ± 0.83 | 0.210 |
| 15/14/13–11/less than 11, n | 24/6/1/1 | 21/11/4/1 | |
| GCS at the time of leaving trauma-bay | 14.62 ± 0.73 | 14.74 ± 0.56 | 0.451 |
| 15/14/13–11/less than 11, n | 26/3/0/3 | 23/8/4/2 | |
| Invasive ICP monitoring, n | 0 | 0 | |
| Evacuation of brain mass lesion, n | 0 | 0 | |
| ISS score | |||
| Median (range, IQR) | 22 (5–43, 17–23) | 19 (9–43, 17–22) | |
| Mean ± SD | 21.2 ± 6.7 | 22.0 ± 9.3 | 0.691 |
| Magnesium Group (n = 32) | Control Group (n = 37) | p Value | |
|---|---|---|---|
| PCA fentanyl consumption | n = 17 (53.1%) | n = 24 (64.9%) | 0.322 |
| postoperative 6 h (mcg) | 201.9 ± 134.1 * | 302.8 ± 140.4 | 0.026 |
| postoperative 24 h (mcg) | 574.7 ± 380.7 | 598.6 ± 264.9 | 0.814 |
| postoperative 48 h (mcg) | 762.8 ± 464.4 | 853.8 ± 357.4 | 0.482 |
| Fentanyl bolus iv until 6 h postoperatively (mcg) | n = 12 (37.5%) 75.0 ± 26.1 | n = 11 (29.7%) 95.8 ± 54.2 | 0.495 0.243 |
| Nefopam consumption | n = 23 (71.9%) | n = 31 (83.8%) | 0.232 |
| postoperative 6 h (mg) | 21.6 ± 2.3 | 21.9 ± 2.5 | 0.700 |
| postoperative 24 h (mg) | 70.6 ± 8.5 | 71.9 ± 5.4 | 0.519 |
| postoperative 48 h (mg) | 86.2 ± 23.6 | 93.4 ± 8.1 | 0.137 |
| NSAIDs use, number (%) | |||
| postoperative 6 h | 5 (15.6%) * | 14 (37.8%) | 0.039 |
| postoperative 24 h | 6 (18.8%) | 8 (21.6%) | 0.767 |
| postoperative 48 h | 8 (25.0%) | 6 (16.2%) | 0.366 |
| Tramadol consumption | n = 29 (90.6%) | n = 36 (97.3%) | 0.330 |
| postoperative 6 h (mg) | 56.3 ± 50.4 | 49.3 ± 47.3 | 0.558 |
| postoperative 24 h (mg) | 120.3 ± 71.9 | 104.1 ± 76.7 | 0.370 |
| postoperative 48 h (mg) | 116.4 ± 65.6 | 127.0 ± 74.9 | 0.536 |
| Pain scores (NRS) | |||
| postoperative 6 h | 6.8 ± 2.8 * | 8.2 ± 2.0 | 0.017 |
| postoperative 24 h | 5.1 ± 2.5 | 5.4 ± 2.3 | 0.660 |
| postoperative 48 h | 3.3 ± 2.2 | 3.2 ± 2.6 | 0.839 |
| Satisfaction scores (NRS) | |||
| postoperative 6 h | 66.1 ± 28.9 * | 47.1 ± 27.6 | 0.007 |
| postoperative 24 h | 71.8 ± 21.1 | 65.7 ± 20.6 | 0.226 |
| postoperative 48 h | 78.3 ± 21.3 | 73.4 ± 24.6 | 0.389 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sohn, H.-M.; Ahn, H.; Seo, W.-S.; Yi, I.K.; Park, J.Y. Magnesium Sulfate and Cerebral Oxygen Saturation in Mild Traumatic Brain Injury: A Randomized, Double-Blind, Controlled Trial. J. Clin. Med. 2022, 11, 3388. https://doi.org/10.3390/jcm11123388
Sohn H-M, Ahn H, Seo W-S, Yi IK, Park JY. Magnesium Sulfate and Cerebral Oxygen Saturation in Mild Traumatic Brain Injury: A Randomized, Double-Blind, Controlled Trial. Journal of Clinical Medicine. 2022; 11(12):3388. https://doi.org/10.3390/jcm11123388
Chicago/Turabian StyleSohn, Hye-Min, Hyoeun Ahn, Won-Seok Seo, In Kyong Yi, and Jun Yeong Park. 2022. "Magnesium Sulfate and Cerebral Oxygen Saturation in Mild Traumatic Brain Injury: A Randomized, Double-Blind, Controlled Trial" Journal of Clinical Medicine 11, no. 12: 3388. https://doi.org/10.3390/jcm11123388