
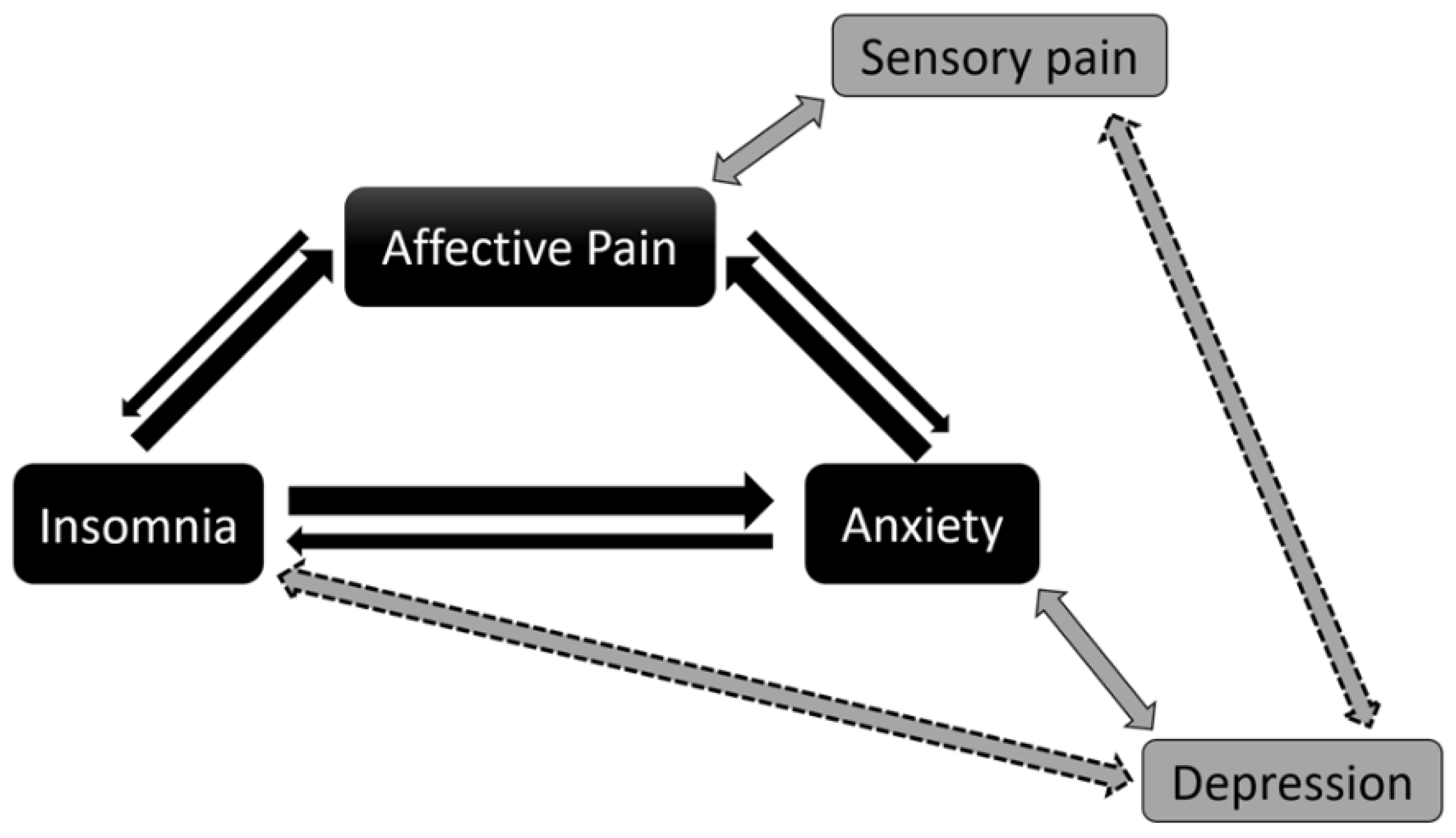
The Affective Dimension of Pain Appears to Be Determinant within a Pain–Insomnia–Anxiety Pathological Loop in Fibromyalgia: A Case-Control Study

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Ethics
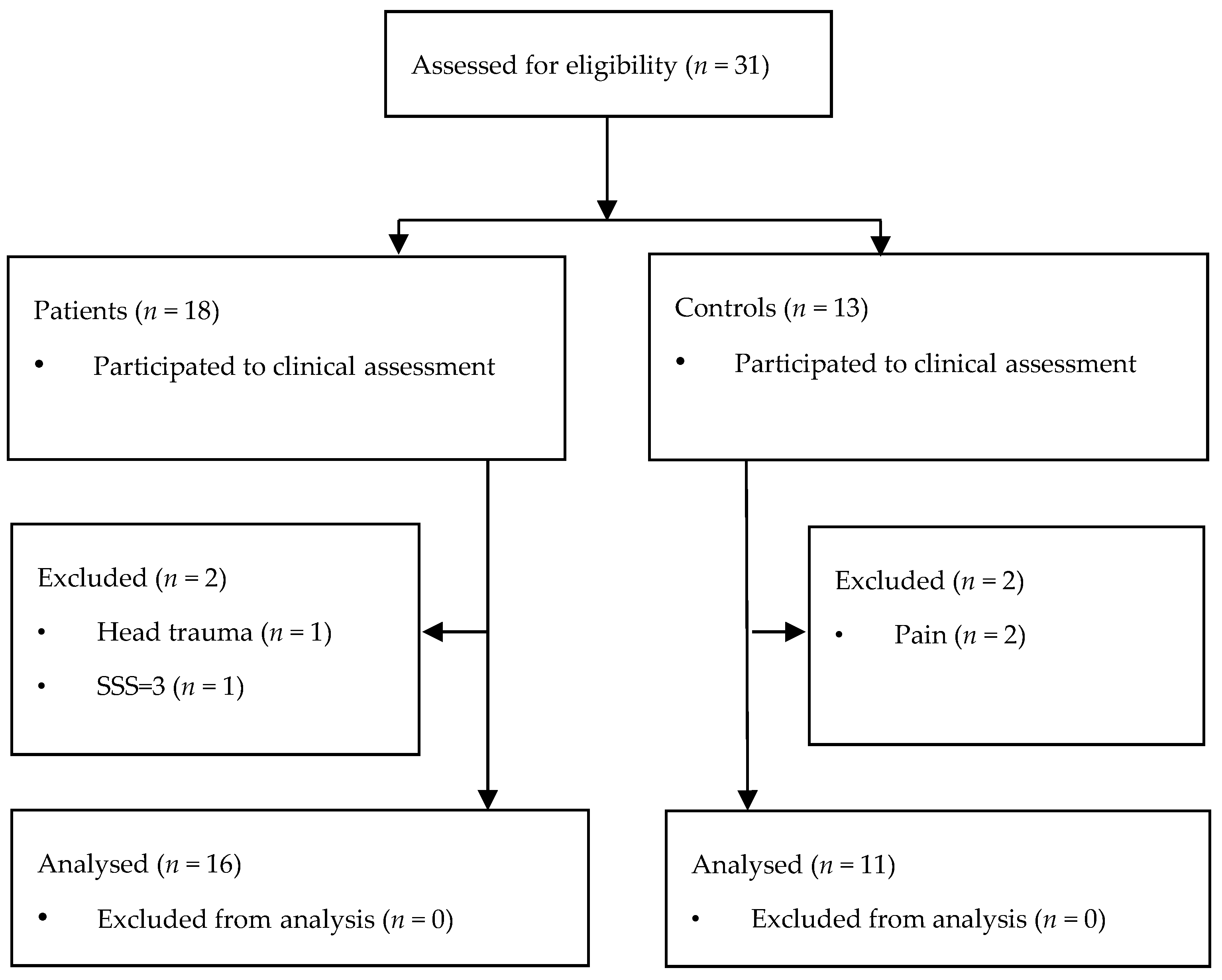
2.2. Participants
2.3. Data Collection
2.4. Data Analysis
2.4.1. FM Diagnosis and Classifications of Clinical Scores
2.4.2. Statistical Analysis
3. Results
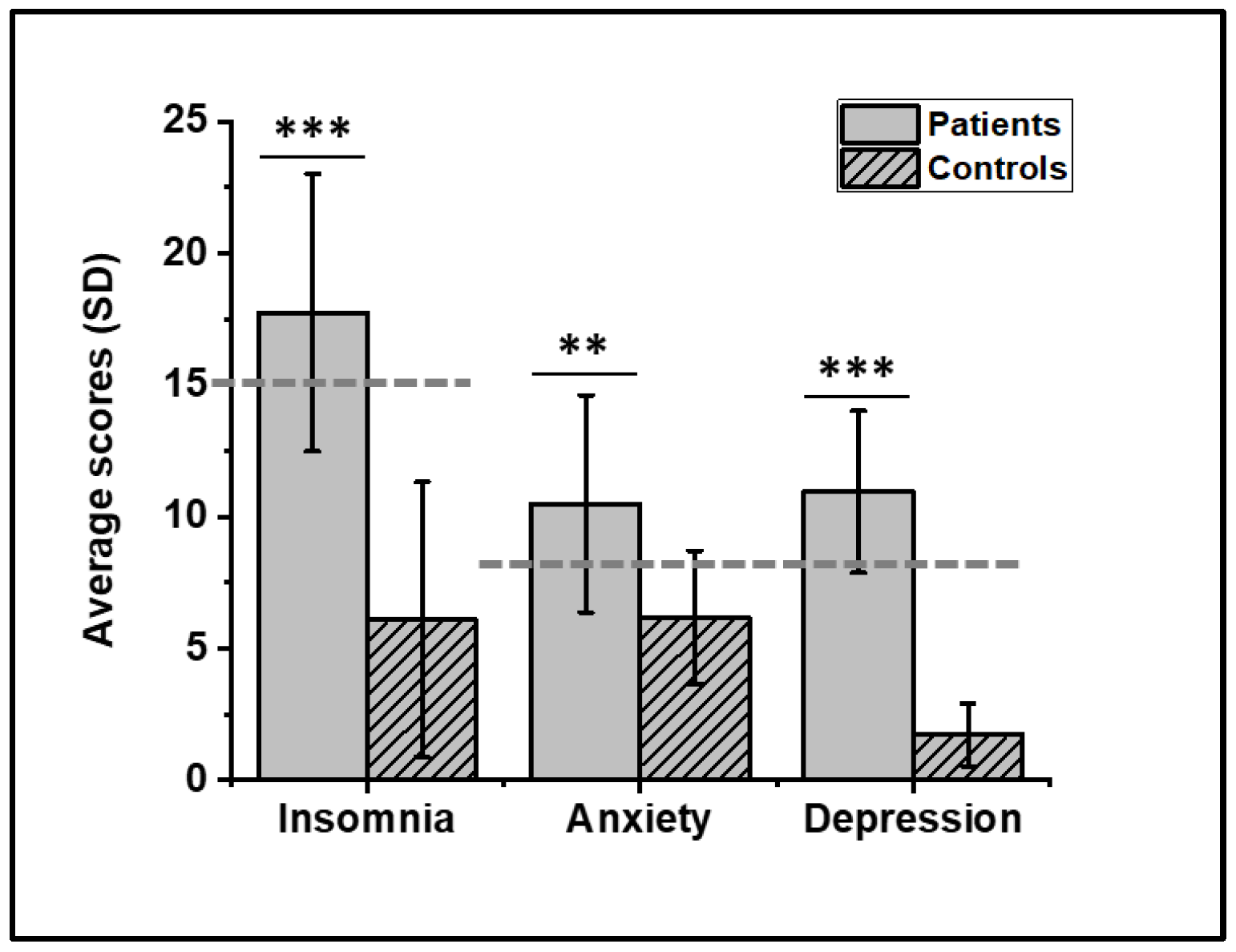
3.1. General Data
3.2. Associations between Pain Indicators
3.3. Associations between Mood, Sleep, and Pain Descriptors
3.4. Impact of Ongoing Pain
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hauser, W.; Ablin, J.; Fitzcharles, M.A.; Littlejohn, G.; Luciano, J.V.; Usui, C.; Walitt, B. Fibromyalgia. Nat. Rev. Dis. Primers 2015, 1, 15022. [Google Scholar] [CrossRef] [PubMed]
- Chinn, S.; Caldwell, W.; Gritsenko, K. Fibromyalgia Pathogenesis and Treatment Options Update. Curr. Pain Headache Rep. 2016, 20, 25. [Google Scholar] [CrossRef] [PubMed]
- Marques, A.P.; Santo, A.; Berssaneti, A.A.; Matsutani, L.A.; Yuan, S.L.K. Prevalence of fibromyalgia: Literature review update. Rev. Bras. Reumatol. Engl. Ed. 2017, 57, 356–363. [Google Scholar] [CrossRef] [PubMed]
- Choy, E.H. The role of sleep in pain and fibromyalgia. Nat. Rev. Rheumatol. 2015, 11, 513–520. [Google Scholar] [CrossRef]
- Bigatti, S.M.; Hernandez, A.M.; Cronan, T.A.; Rand, K.L. Sleep disturbances in fibromyalgia syndrome: Relationship to pain and depression. Arthritis Rheum. 2008, 59, 961–967. [Google Scholar] [CrossRef] [Green Version]
- Andrade, A.; Vilarino, G.T.; Sieczkowska, S.M.; Coimbra, D.R.; Bevilacqua, G.G.; Steffens, R.A.K. The relationship between sleep quality and fibromyalgia symptoms. J. Health Psychol. 2020, 25, 1176–1186. [Google Scholar] [CrossRef]
- van den Berg, B.; Hijma, H.J.; Koopmans, I.; Doll, R.J.; Zuiker, R.; Groeneveld, G.J.; Buitenweg, J.R. Simultaneous measurement of intra-epidermal electric detection thresholds and evoked potentials for observation of nociceptive processing following sleep deprivation. Exp. Brain Res. 2022, 240, 631–649. [Google Scholar] [CrossRef]
- Smith, M.T.; Edwards, R.R.; McCann, U.D.; Haythornthwaite, J.A. The effects of sleep deprivation on pain inhibition and spontaneous pain in women. Sleep 2007, 30, 494–505. [Google Scholar] [CrossRef]
- Haack, M.; Scott-Sutherland, J.; Santangelo, G.; Simpson, N.S.; Sethna, N.; Mullington, J.M. Pain sensitivity and modulation in primary insomnia. Eur. J. Pain 2012, 16, 522–533. [Google Scholar] [CrossRef] [Green Version]
- Husak, A.J.; Bair, M.J. Chronic Pain and Sleep Disturbances: A Pragmatic Review of Their Relationships, Comorbidities, and Treatments. Pain Med. 2020, 21, 1142–1152. [Google Scholar] [CrossRef]
- Herrero Babiloni, A.; De Koninck, B.P.; Beetz, G.; De Beaumont, L.; Martel, M.O.; Lavigne, G.J. Sleep and pain: Recent insights, mechanisms, and future directions in the investigation of this relationship. J. Neural. Transm. 2020, 127, 647–660. [Google Scholar] [CrossRef]
- Diaz-Piedra, C.; Di Stasi, L.L.; Baldwin, C.M.; Buela-Casal, G.; Catena, A. Sleep disturbances of adult women suffering from fibromyalgia: A systematic review of observational studies. Sleep Med. Rev. 2015, 21, 86–99. [Google Scholar] [CrossRef]
- Rizzi, M.; Radovanovic, D.; Santus, P.; Airoldi, A.; Frassanito, F.; Vanni, S.; Cristiano, A.; Masala, I.F.; Sarzi-Puttini, P. Influence of autonomic nervous system dysfunction in the genesis of sleep disorders in fibromyalgia patients. Clin. Exp. Rheumatol. 2017, 35 (Suppl. 105), 74–80. [Google Scholar] [CrossRef]
- Fietta, P.; Fietta, P.; Manganelli, P. Fibromyalgia and psychiatric disorders. Acta Biomed. 2007, 78, 88–95. [Google Scholar]
- Hadlandsmyth, K.; Dailey, D.L.; Rakel, B.A.; Zimmerman, M.B.; Vance, C.G.; Merriwether, E.N.; Chimenti, R.L.; Geasland, K.M.; Crofford, L.J.; Sluka, K.A. Somatic symptom presentations in women with fibromyalgia are differentially associated with elevated depression and anxiety. J. Health Psychol. 2020, 25, 819–829. [Google Scholar] [CrossRef]
- Galvez-Sanchez, C.M.; Montoro, C.I.; Duschek, S.; Reyes Del Paso, G.A. Depression and trait-anxiety mediate the influence of clinical pain on health-related quality of life in fibromyalgia. J. Affect Disord. 2020, 265, 486–495. [Google Scholar] [CrossRef]
- Consoli, G.; Marazziti, D.; Ciapparelli, A.; Bazzichi, L.; Massimetti, G.; Giacomelli, C.; Rossi, A.; Bombardieri, S.; Dell’Osso, L. The impact of mood, anxiety, and sleep disorders on fibromyalgia. Compr. Psychiatry 2012, 53, 962–967. [Google Scholar] [CrossRef]
- Paul-Savoie, E.; Marchand, S.; Morin, M.; Bourgault, P.; Brissette, N.; Rattanavong, V.; Cloutier, C.; Bissonnette, A.; Potvin, S. Is the deficit in pain inhibition in fibromyalgia influenced by sleep impairments? Open Rheumatol. J. 2012, 6, 296–302. [Google Scholar] [CrossRef] [Green Version]
- Michaelides, A.; Zis, P. Depression, anxiety and acute pain: Links and management challenges. Postgrad. Med. 2019, 131, 438–444. [Google Scholar] [CrossRef]
- Rainville, P. Brain mechanisms of pain affect and pain modulation. Curr. Opin. Neurobiol. 2002, 12, 195–204. [Google Scholar] [CrossRef]
- Krause, A.J.; Prather, A.A.; Wager, T.D.; Lindquist, M.A.; Walker, M.P. The Pain of Sleep Loss: A Brain Characterization in Humans. J. Neurosci. 2019, 39, 2291–2300. [Google Scholar] [CrossRef] [Green Version]
- Melzack, R. Pain and the neuromatrix in the brain. J. Dent. Educ. 2001, 65, 1378–1382. [Google Scholar] [CrossRef]
- Salaffi, F.; Sarzi-Puttini, P.; Atzeni, F. How to measure chronic pain: New concepts. Best Pract. Res. Clin. Rheumatol. 2015, 29, 164–186. [Google Scholar] [CrossRef]
- Di Tella, M.; Ghiggia, A.; Tesio, V.; Romeo, A.; Colonna, F.; Fusaro, E.; Torta, R.; Castelli, L. Pain experience in Fibromyalgia Syndrome: The role of alexithymia and psychological distress. J. Affect Disord. 2017, 208, 87–93. [Google Scholar] [CrossRef] [Green Version]
- Wiech, K.; Tracey, I. The influence of negative emotions on pain: Behavioral effects and neural mechanisms. Neuroimage 2009, 47, 987–994. [Google Scholar] [CrossRef]
- Liu, J.H.; Wei, C.Z.; Huang, L.Y.; Wang, W.; Lei, Z.J.; Liang, D.H.; Wang, F.; Wang, X.Y.; Liu, K.; Hou, X.J.; et al. Study on the prevalence of snoring and obstructive sleep apnea-hypopnea syndrome in Guangxi, China. Zhonghua Liu Xing Bing Xue Za Zhi 2007, 28, 115–118. [Google Scholar]
- Talbot, K.; Madden, V.J.; Jones, S.L.; Moseley, G.L. The sensory and affective components of pain: Are they differentially modifiable dimensions or inseparable aspects of a unitary experience? A systematic review. Br. J. Anaesth. 2019, 123, e263–e272. [Google Scholar] [CrossRef]
- Price, D.D. Psychological and neural mechanisms of the affective dimension of pain. Science 2000, 288, 1769–1772. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boggero, I.A.; Carlson, C.R. Somatosensory and affective contributions to emotional, social, and daily functioning in chronic pain patients. Pain Med. 2015, 16, 341–347. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rainville, P.; Bao, Q.V.; Chretien, P. Pain-related emotions modulate experimental pain perception and autonomic responses. Pain 2005, 118, 306–318. [Google Scholar] [CrossRef] [PubMed]
- Giesecke, T.; Gracely, R.H.; Williams, D.A.; Geisser, M.E.; Petzke, F.W.; Clauw, D.J. The relationship between depression, clinical pain, and experimental pain in a chronic pain cohort. Arthritis Rheum. 2005, 52, 1577–1584. [Google Scholar] [CrossRef] [Green Version]
- Bushnell, M.C.; Ceko, M.; Low, L.A. Cognitive and emotional control of pain and its disruption in chronic pain. Nat. Rev. Neurosci. 2013, 14, 502–511. [Google Scholar] [CrossRef] [Green Version]
- Gracely, R.H.; Ceko, M.; Bushnell, M.C. Fibromyalgia and depression. Pain Res. Treat. 2012, 2012, 486590. [Google Scholar] [CrossRef] [Green Version]
- Xiao, X.; Zhang, Y.Q. A new perspective on the anterior cingulate cortex and affective pain. Neurosci. Biobehav. Rev. 2018, 90, 200–211. [Google Scholar] [CrossRef]
- Teixeira, M.; Mancini, C.; Wicht, C.A.; Maestretti, G.; Kuntzer, T.; Cazzoli, D.; Mouthon, M.; Annoni, J.M.; Chabwine, J.N. Beta Electroencephalographic Oscillation Is a Potential GABAergic Biomarker of Chronic Peripheral Neuropathic Pain. Front. Neurosci. 2021, 15, 594536. [Google Scholar] [CrossRef]
- Ichesco, E.; Schmidt-Wilcke, T.; Bhavsar, R.; Clauw, D.J.; Peltier, S.J.; Kim, J.; Napadow, V.; Hampson, J.P.; Kairys, A.E.; Williams, D.A.; et al. Altered resting state connectivity of the insular cortex in individuals with fibromyalgia. J. Pain 2014, 15, 815–826.e811. [Google Scholar] [CrossRef] [Green Version]
- Fillingim, R.B.; King, C.D.; Ribeiro-Dasilva, M.C.; Rahim-Williams, B.; Riley, J.L., 3rd. Sex, gender, and pain: A review of recent clinical and experimental findings. J. Pain 2009, 10, 447–485. [Google Scholar] [CrossRef] [Green Version]
- Kowalczyk, W.J.; Evans, S.M.; Bisaga, A.M.; Sullivan, M.A.; Comer, S.D. Sex differences and hormonal influences on response to cold pressor pain in humans. J. Pain 2006, 7, 151–160. [Google Scholar] [CrossRef]
- Menzies, V. CE: Fibromyalgia Syndrome: Current Considerations in Symptom Management. AJN Am. J. Nurs. 2016, 116, 24–32. [Google Scholar] [CrossRef] [Green Version]
- Morin, C.M.; Belleville, G.; Belanger, L.; Ivers, H. The Insomnia Severity Index: Psychometric indicators to detect insomnia cases and evaluate treatment response. Sleep 2011, 34, 601–608. [Google Scholar] [CrossRef] [Green Version]
- Zigmond, A.S.; Snaith, R.P. The hospital anxiety and depression scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef] [Green Version]
- Perrot, S.; Bouhassira, D.; Fermanian, J.; Cercle d’Etude de la Douleur en, R. Development and validation of the Fibromyalgia Rapid Screening Tool (FiRST). Pain 2010, 150, 250–256. [Google Scholar] [CrossRef]
- Collins, S.L.; Moore, R.A.; McQuay, H.J. The visual analogue pain intensity scale: What is moderate pain in millimetres? Pain 1997, 72, 95–97. [Google Scholar] [CrossRef]
- Bouhassira, D.; Attal, N.; Alchaar, H.; Boureau, F.; Brochet, B.; Bruxelle, J.; Cunin, G.; Fermanian, J.; Ginies, P.; Grun-Overdyking, A.; et al. Comparison of pain syndromes associated with nervous or somatic lesions and development of a new neuropathic pain diagnostic questionnaire (DN4). Pain 2005, 114, 29–36. [Google Scholar] [CrossRef] [PubMed]
- Dworkin, R.H.; Turk, D.C.; Revicki, D.A.; Harding, G.; Coyne, K.S.; Peirce-Sandner, S.; Bhagwat, D.; Everton, D.; Burke, L.B.; Cowan, P.; et al. Development and initial validation of an expanded and revised version of the Short-form McGill Pain Questionnaire (SF-MPQ-2). Pain 2009, 144, 35–42. [Google Scholar] [CrossRef] [PubMed]
- Cleeland, C.S.; Ryan, K.M. Pain assessment: Global use of the Brief Pain Inventory. Ann. Acad. Med. Singap. 1994, 23, 129–138. [Google Scholar] [PubMed]
- Wolfe, F.; Clauw, D.J.; Fitzcharles, M.A.; Goldenberg, D.L.; Katz, R.S.; Mease, P.; Russell, A.S.; Russell, I.J.; Winfield, J.B.; Yunus, M.B. The American College of Rheumatology preliminary diagnostic criteria for fibromyalgia and measurement of symptom severity. Arthritis Care Res. 2010, 62, 600–610. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Čeko, M.; Frangos, E.; Gracely, J.; Richards, E.; Wang, B.; Schweinhardt, P.; Catherine Bushnell, M. Default mode network changes in fibromyalgia patients are largely dependent on current clinical pain. NeuroImage 2020, 216, 116877. [Google Scholar] [CrossRef]
- Myles, P.S.; Myles, D.B.; Galagher, W.; Boyd, D.; Chew, C.; MacDonald, N.; Dennis, A. Measuring acute postoperative pain using the visual analog scale: The minimal clinically important difference and patient acceptable symptom state. Br. J. Anaesth. 2017, 118, 424–429. [Google Scholar] [CrossRef] [Green Version]
- Mantha, S.; Thisted, R.; Foss, J.; Ellis, J.E.; Roizen, M.F. A proposal to use confidence intervals for visual analog scale data for pain measurement to determine clinical significance. Anesth. Analg. 1993, 77, 1041–1047. [Google Scholar] [CrossRef]
- Hawker, G.A.; Mian, S.; Kendzerska, T.; French, M. Measures of adult pain: Visual Analog Scale for Pain (VAS Pain), Numeric Rating Scale for Pain (NRS Pain), McGill Pain Questionnaire (MPQ), Short-Form McGill Pain Questionnaire (SF-MPQ), Chronic Pain Grade Scale (CPGS), Short Form-36 Bodily Pain Scale (SF-36 BPS), and Measure of Intermittent and Constant Osteoarthritis Pain (ICOAP). Arthritis Care Res. 2011, 63 (Suppl. 11), S240–S252. [Google Scholar] [CrossRef]
- Kruschke, J.K.; Liddell, T.M. Bayesian data analysis for newcomers. Psychon. Bull. Rev. 2018, 25, 155–177. [Google Scholar] [CrossRef] [Green Version]
- Melzack, R. The short-form McGill Pain Questionnaire. Pain 1987, 30, 191–197. [Google Scholar] [CrossRef]
- DelVentura, J.L.; Terry, E.L.; Bartley, E.J.; Rhudy, J.L. Emotional modulation of pain and spinal nociception in persons with severe insomnia symptoms. Ann. Behav. Med. 2014, 47, 303–315. [Google Scholar] [CrossRef] [Green Version]
- Schiel, J.E.; Holub, F.; Petri, R.; Leerssen, J.; Tamm, S.; Tahmasian, M.; Riemann, D.; Spiegelhalder, K. Affect and Arousal in Insomnia: Through a Lens of Neuroimaging Studies. Curr. Psychiatry Rep. 2020, 22, 44. [Google Scholar] [CrossRef]
- Burgmer, M.; Pogatzki-Zahn, E.; Gaubitz, M.; Wessoleck, E.; Heuft, G.; Pfleiderer, B. Altered brain activity during pain processing in fibromyalgia. Neuroimage 2009, 44, 502–508. [Google Scholar] [CrossRef]
- Berna, C.; Leknes, S.; Holmes, E.A.; Edwards, R.R.; Goodwin, G.M.; Tracey, I. Induction of depressed mood disrupts emotion regulation neurocircuitry and enhances pain unpleasantness. Biol. Psychiatry 2010, 67, 1083–1090. [Google Scholar] [CrossRef]
- Zhuo, M. Neural Mechanisms Underlying Anxiety-Chronic Pain Interactions. Trends Neurosci. 2016, 39, 136–145. [Google Scholar] [CrossRef]
- Dunietz, G.L.; Swanson, L.M.; Jansen, E.C.; Chervin, R.D.; O’Brien, L.M.; Lisabeth, L.D.; Braley, T.J. Key insomnia symptoms and incident pain in older adults: Direct and mediated pathways through depression and anxiety. Sleep 2018, 41, zsy125. [Google Scholar] [CrossRef] [Green Version]
- Ravyts, S.G.; Dzierzewski, J.M.; Grah, S.C.; Buman, M.P.; Aiken-Morgan, A.T.; Giacobb, P.R., Jr.; Roberts, B.L.; Marsiske, M.; McCrae, C.S. Sleep and Pain in Mid- to Late-Life: An Exploration of Day-to-Day Pain Inconsistency. Clin. Gerontol. 2018, 41, 123–129. [Google Scholar] [CrossRef] [Green Version]
- McCrae, C.S.; Williams, J.; Roditi, D.; Anderson, R.; Mundt, J.M.; Miller, M.B.; Curtis, A.F.; Waxenberg, L.B.; Staud, R.; Berry, R.B.; et al. Cognitive behavioral treatments for insomnia and pain in adults with comorbid chronic insomnia and fibromyalgia: Clinical outcomes from the SPIN randomized controlled trial. Sleep 2019, 42, zsy234. [Google Scholar] [CrossRef]
- Prados, G.; Miro, E.; Martinez, M.P.; Sanchez, A.I.; Lami, M.J.; Caliz, R. Combined cognitive-behavioral therapy for fibromyalgia: Effects on polysomnographic parameters and perceived sleep quality. Int. J. Clin. Health Psychol. 2020, 20, 232–242. [Google Scholar] [CrossRef]
- Finan, P.H.; Goodin, B.R.; Smith, M.T. The association of sleep and pain: An update and a path forward. J. Pain 2013, 14, 1539–1552. [Google Scholar] [CrossRef] [Green Version]
- Meeus, M.; Nijs, J. Central sensitization: A biopsychosocial explanation for chronic widespread pain in patients with fibromyalgia and chronic fatigue syndrome. Clin. Rheumatol. 2007, 26, 465–473. [Google Scholar] [CrossRef] [Green Version]
- Nijs, J.; Mairesse, O.; Neu, D.; Leysen, L.; Danneels, L.; Cagnie, B.; Meeus, M.; Moens, M.; Ickmans, K.; Goubert, D. Sleep Disturbances in Chronic Pain: Neurobiology, Assessment, and Treatment in Physical Therapist Practice. Phys. Ther. 2018, 98, 325–335. [Google Scholar] [CrossRef]
- Clark, J.R.; Nijs, J.; Yeowell, G.; Holmes, P.; Goodwin, P.C. Trait Sensitivity, Anxiety, and Personality Are Predictive of Central Sensitization Symptoms in Patients with Chronic Low Back Pain. Pain Pract. 2019, 19, 800–810. [Google Scholar] [CrossRef]
- Eysenck, M.W.; Fajkowska, M. Anxiety and depression: Toward overlapping and distinctive features. Cogn. Emot. 2018, 32, 1391–1400. [Google Scholar] [CrossRef]
- Manchikanti, L.; Pampati, V.; Beyer, C.; Damron, K. Do number of pain conditions influence emotional status? Pain Physician 2002, 5, 200–205. [Google Scholar] [CrossRef] [PubMed]
- Hauser, W.; Sarzi-Puttini, P.; Fitzcharles, M.A. Fibromyalgia syndrome: Under-, over- and misdiagnosis. Clin. Exp. Rheumatol. 2019, 37 (Suppl. 116), 90–97. [Google Scholar] [PubMed]
- Basu, N.; Kaplan, C.M.; Ichesco, E.; Larkin, T.; Harris, R.E.; Murray, A.; Waiter, G.; Clauw, D.J. Neurobiologic Features of Fibromyalgia Are Also Present Among Rheumatoid Arthritis Patients. Arthritis Rheumatol. 2018, 70, 1000–1007. [Google Scholar] [CrossRef] [PubMed]
- Boomershine, C.S. Fibromyalgia: The prototypical central sensitivity syndrome. Curr. Rheumatol. Rev. 2015, 11, 131–145. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Neurological Symptoms | Type of Symptoms | n/16 |
| Negative symptoms * | 7 | |
| Positive symptoms ** | 4 | |
| Normal | 5 | |
| Treatment | Type of Treatment | n/16 |
| NSAID | 7 | |
| Antidepressants | 7 | |
| Physical and alternative | 5 | |
| Antimigrainous | 4 | |
| Benzodiazepines | 3 | |
| Opiates | 2 | |
| Other drugs | 5 | |
| None | 3 |
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | |
|---|---|---|---|---|---|---|---|---|---|---|
| 1. ISI | - | |||||||||
| 2. HADanx | 0.59 a* | - | ||||||||
| (0.84 a**) | ||||||||||
| 3. HADdep | 0.41 | 0.56 a* | - | |||||||
| (0.67 b*) | (0.68 b*) | |||||||||
| 4. MPQaff | 0.48 b | 0.44 b | 0.14 | - | ||||||
| (0.45) | (0.36) | (0.49) | ||||||||
| 5. MPQsen | 0.33 | 0.16 | 0.01 | 0.64 a** | - | |||||
| (0.29) | (0.39) | (0.73 a*) | (0.69 b*) | |||||||
| 6. VASd | −0.37 | −0.29 | −0.19 | −0.11 | 0.24 | |||||
| (0.27) | (0.43) | (0.26) | (0.61 b) | (0.53 b) | ||||||
| 7. VASgen | −0.00 | 0.02 | 0.15 | 0.29 | 0.62 a* | 0.39 | - | |||
| (0.27) | (−0.07) | (0.41) | (0.47) | (0.55 b) | (0.18) | |||||
| 8. BPIsev | 0.22 | 0.15 | 0.07 | 0.51 b* | 0.71 a** | 0.44 b | 0.66 a** | - | ||
| (0.40) | (0.33) | (0.50) | (0.68 b*) | (0.63 b) | (0.77 a*) | (0.66 b*) | ||||
| 9. BPIint | 0.63 a** | 0.47 b | 0.39 | 0.64 a** | 0.29 | −0.41 | −0.03 | 0.26 | - | |
| (0.55 b) | (0.38) | (0.69 b*) | (0.72 a*) | (0.43) | (0.15) | (0.36) | (0.44) | |||
| 10. WPI | −0.22 | −0.07 | −0.36 | −0.36 | 0.01 | 0.57 a* | 0.22 | 0.18 | −0.40 | - |
| (0.29) | (0.42) | (0.55) | (−0.46) | (−0.58 b) | (0.02) | (−0.66 b) | (−0.35) | (−0.38) | ||
| 11. DN4 | −0.10 | −0.02 | 0.12 | 0.55 b* | 0.71 a** | 0.34 | 0.69 a** | 0.63 a** | 0.20 | −0.10 |
| (0.35) | (0.04) | (0.65 b) | (0.47) | (0.67 b*) | (0.11) | (0.90 a**) | (0.59 b) | (0.47) | (−0.66 b) |
| N | Mean ± SD | F | p-Value | ||
|---|---|---|---|---|---|
| Affective pain | |||||
| No insomnia | 5 | 3.00 ± 1.59 | 13.36 | 0.003 | |
| Insomnia | 11 | 7.18 ± 2.30 | |||
| No anxiety | 6 | 3.58 ± 2.31 | 9.71 | 0.008 | |
| Anxiety | 10 | 7.25 ± 2.26 | |||
| Sensory pain | |||||
| No insomnia | 5 | 4.11 ± 2.03 | 1.99 | 0.180 | |
| Insomnia | 11 | 5.83 ± 2.34 | |||
| No anxiety | 6 | 4.40 ± 2.11 | 1.45 | 0.248 | |
| Anxiety | 10 | 5.83 ± 2.39 | |||
| Current pain intensity | |||||
| No anxiety | 6 | 5.17 ± 2.18 | 0.20 | 0.665 | |
| Anxiety | 10 | 4.5 ± 3.26 | |||
| No insomnia | 5 | 5.90 ± 2.22 | 1.21 | 0.290 | |
| Insomnia | 11 | 4.23 ± 3.03 | |||
| General pain intensity | |||||
| No anxiety | 6 | 6.08 ± 2.51 | 0.17 | 0.683 | |
| Anxiety | 10 | 6.55 ± 1.94 | |||
| No insomnia | 5 | 6.00 ± 2.21 | 0.22 | 0.647 | |
| Insomnia | 11 | 6.54 ± 2.14 | |||
| Insomnia | |||||
| No anxiety | 6 | 14.83 ± 5.67 | 3.41 | 0.086 | |
| Anxiety | 10 | 19.50 ± 4.40 | |||
| Anxiety | |||||
| No insomnia | 5 | 6.60 ± 1.82 | 10.80 | 0.005 | |
| Insomnia | 11 | 12.27 ± 3.61 | |||
| Depression | |||||
| No insomnia | 5 | 9.20 ± 2.95 | 2.58 | 0.130 | |
| Insomnia | 11 | 11.73 ± 2.90 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mory, L.-N.; de Oliveira Fernandes, D.; Mancini, C.; Mouthon, M.; Chabwine, J.N. The Affective Dimension of Pain Appears to Be Determinant within a Pain–Insomnia–Anxiety Pathological Loop in Fibromyalgia: A Case-Control Study. J. Clin. Med. 2022, 11, 3296. https://doi.org/10.3390/jcm11123296
Mory L-N, de Oliveira Fernandes D, Mancini C, Mouthon M, Chabwine JN. The Affective Dimension of Pain Appears to Be Determinant within a Pain–Insomnia–Anxiety Pathological Loop in Fibromyalgia: A Case-Control Study. Journal of Clinical Medicine. 2022; 11(12):3296. https://doi.org/10.3390/jcm11123296
Chicago/Turabian StyleMory, Lliure-Naima, Daniel de Oliveira Fernandes, Christian Mancini, Michael Mouthon, and Joelle Nsimire Chabwine. 2022. "The Affective Dimension of Pain Appears to Be Determinant within a Pain–Insomnia–Anxiety Pathological Loop in Fibromyalgia: A Case-Control Study" Journal of Clinical Medicine 11, no. 12: 3296. https://doi.org/10.3390/jcm11123296