
Uterine Septum with or without Hysteroscopic Metroplasty: Impact on Fertility and Obstetrical Outcomes—A Systematic Review and Meta-Analysis of Observational Research


 , , , ,
, , , ,
Abstract
:1. Introduction
2. Material and Methods
2.1. Study Design and Protocol Registration
2.2. Eligibility Criteria
- Type of study: Case-control studies, cohort studies or case series.
- Period of publication: no restriction.
- Language: English.
- Comparators: (i) Women with untreated uterine septum versus women without septum (controls); (ii) Women with treated uterine septum versus women with untreated septum (controls); (iii) Women before and after septum removal.
- Outcomes: Pregnancy rate; live birth rate; spontaneous abortion rate; preterm delivery rate.
- Outcome definitions: Pregnancy rate (PR—defined as the presence of a gestational sac on transvaginal ultrasound; Live birth rate (LBR—defined as the delivery of one or more living and viable infants). Spontaneous abortion rate (SA—defined as fetal loss prior to the completed 23th week of gestation; Preterm labour (PL—defined as a delivery before 37 weeks of gestation).
2.3. Information Sources and Search Strategies
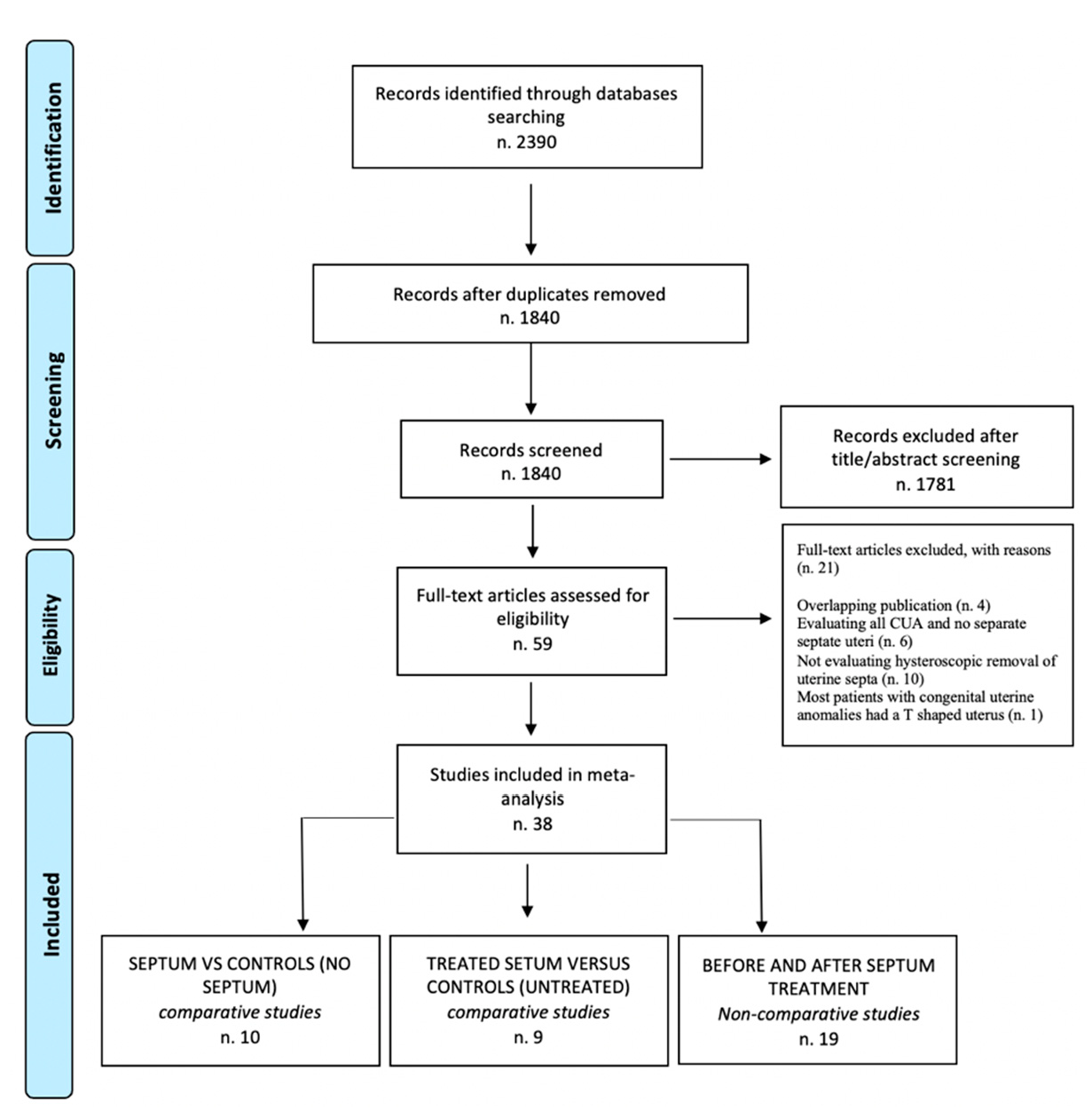
2.4. Study Selection
2.5. Risk of Bias
2.6. Statistical Analysis
3. Results
Study Selection
4. Research Findings
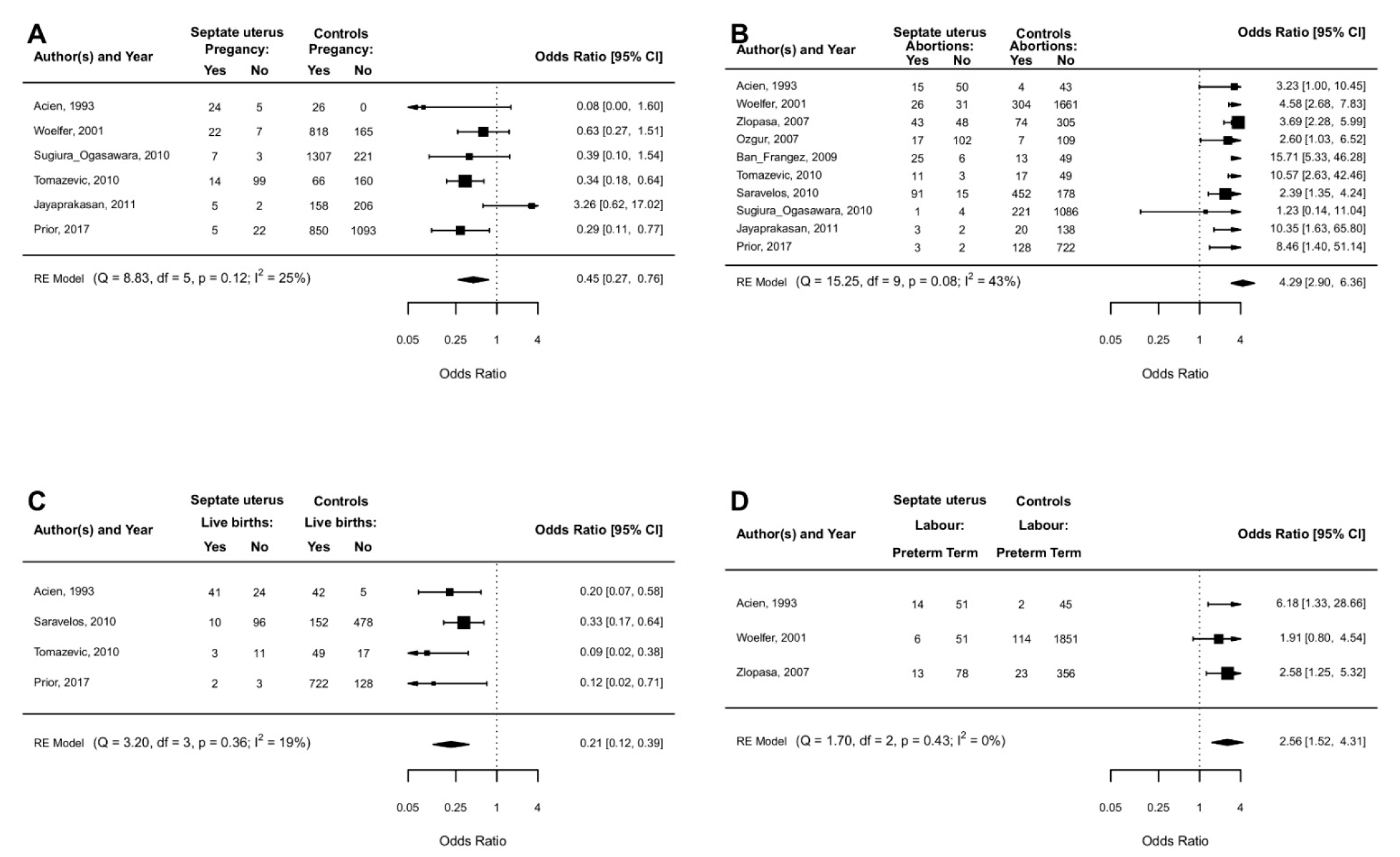
4.1. Uterine Septum vs. Controls (No Septum)
4.2. Pregnancy Rate
4.2.1. Subgroup Analysis
4.2.2. Sensitivity Analysis
4.3. Live Birth Rate
4.3.1. Subgroup Analysis
4.3.2. Sensitivity Analysis
4.4. Spontaneous Abortions in I-II Trimesters
4.4.1. Subgroup Analysis
4.4.2. Sensitivity Analysis
4.4.3. Spontaneous Abortion during the First Trimester of Pregnancy
4.4.4. Spontaneous Abortions during the Second Trimester of Pregnancy
4.5. Preterm Labor
4.5.1. Subgroup Analysis
4.5.2. Sensitivity Analysis
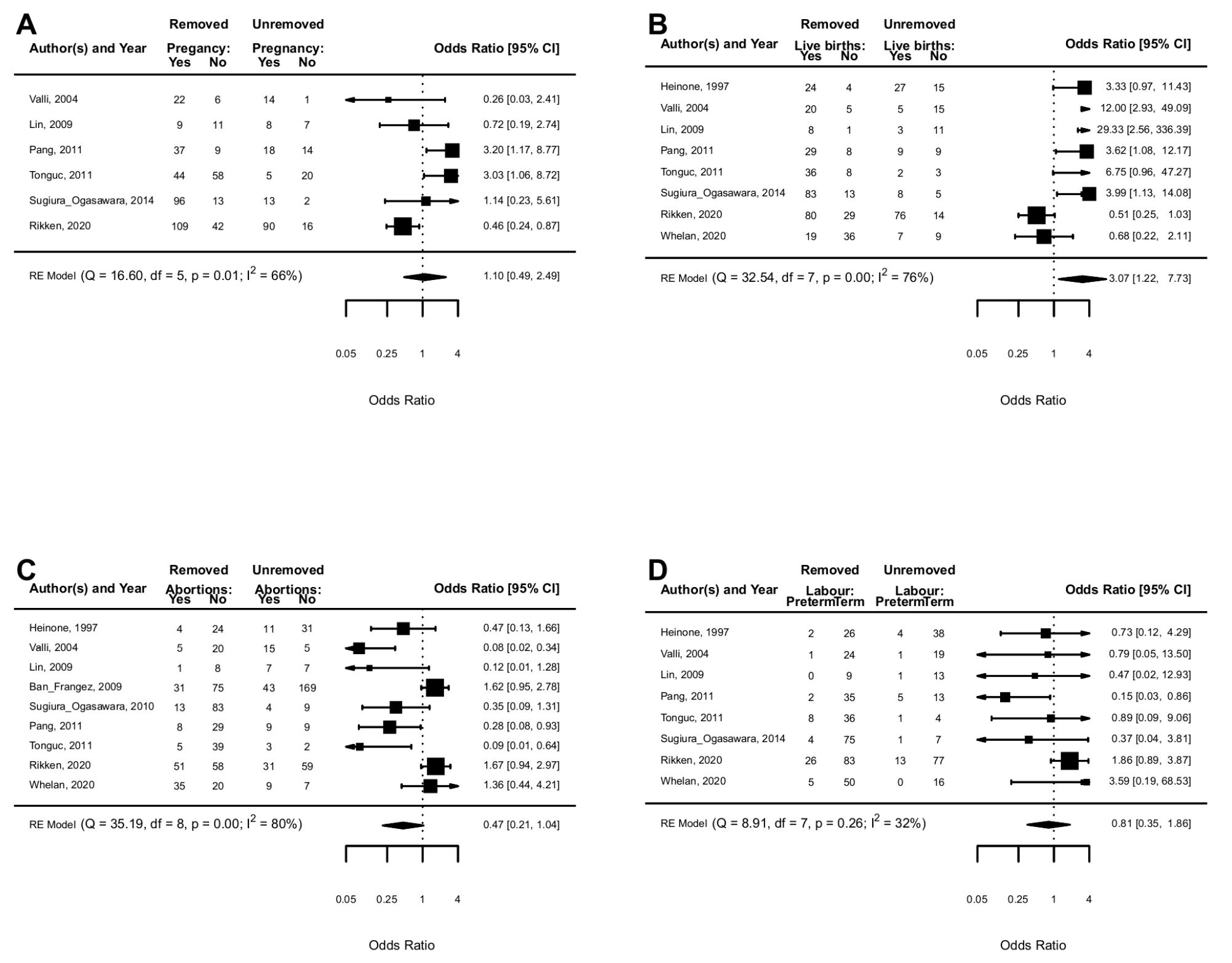
4.6. Treated Uterine Septum versus Untreated Uterine Septum
4.7. Pregnancy Rate
4.7.1. Subgroup Analysis
4.7.2. Sensitivity Analysis
4.8. Live Birth Rate
4.8.1. Subgroup Analysis
4.8.2. Sensitivity Analysis
4.9. Spontaneous Abortions during the First and Second Trimesters
4.9.1. Subgroup Analysis
4.9.2. Sensitivity Analysis
4.10. Preterm Labor
4.10.1. Subgroup Analysis
4.10.2. Sensitivity Analysis
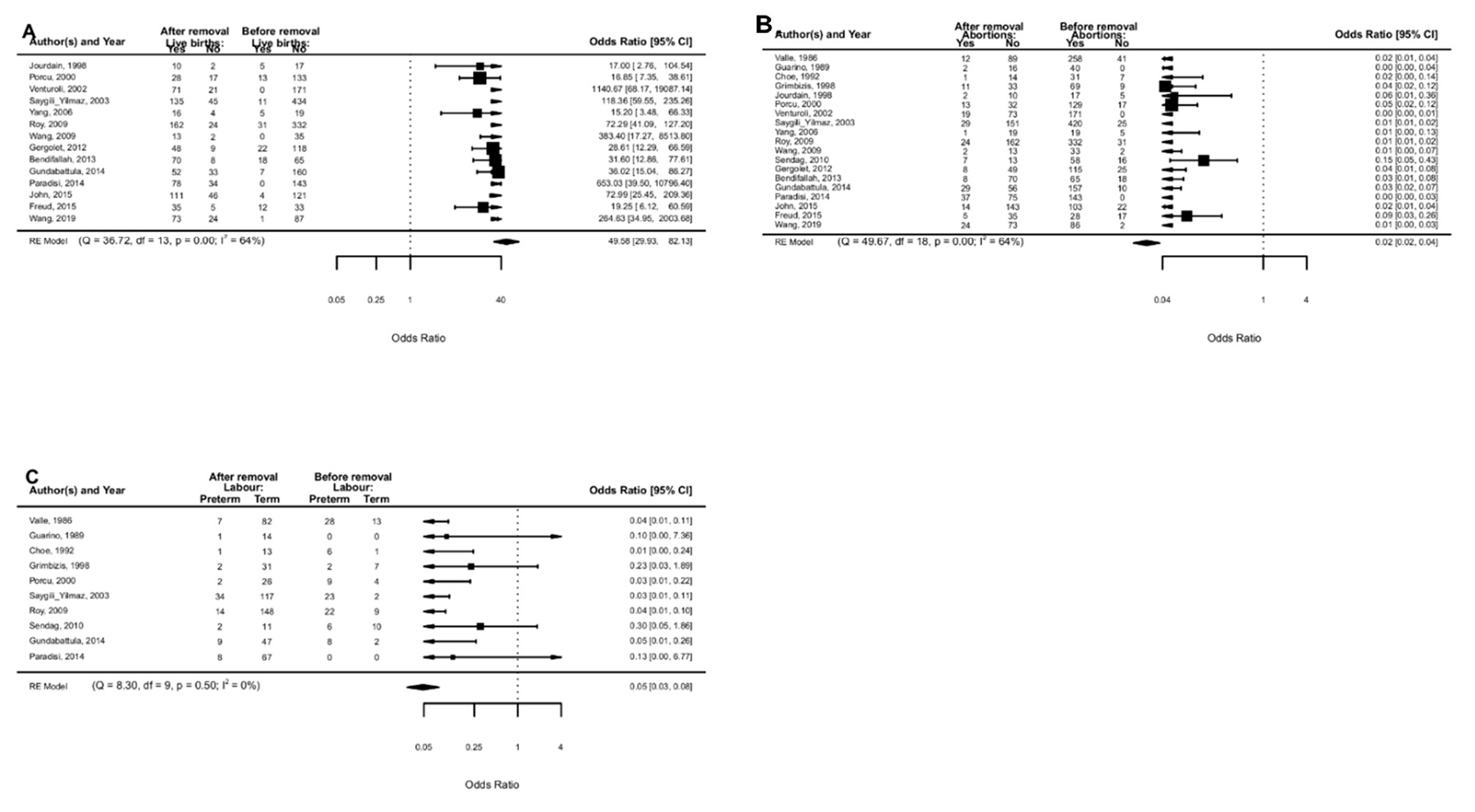
5. Before and after Septum Removal
5.1. Live Birth Rate
5.1.1. Subgroup Analysis
5.1.2. Sensitivity Analysis
5.2. Spontaneous Abortions during the First and Second Trimesters of Pregnancy
5.2.1. Sub-Analyses
5.2.2. Sensitivity Analysis
5.3. Preterm Labor
5.3.1. Subgroup-Analyses
5.3.2. Sensitivity Analysis
6. Surgical Complications
7. Risk Bias Assessment
8. Discussion
9. Main Findings and Implications
9.1. Uterine Septum versus Controls (No Septum)
9.2. Treated Uterine Septum versus Untreated Septum
9.3. Before and after Septum Removal
10. Surgical Complications
11. Biological Rationale
12. Strengths and Limitations
13. Conclusions and Future Research
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Paradisi, R.; Barzanti, R.; Natali, F.; Battaglia, C.; Venturoli, S. Metroplasty in a large population of women with septate uterus. J. Minim. Invasive Gynecol. 2011, 18, 449–454. [Google Scholar] [CrossRef] [PubMed]
- Acien, P.; Acien, M. Evidence-based management of recurrent miscarriage. Surg. Manag. 2004, 1, 335–342. [Google Scholar]
- Grimbizis, G.F.; Camus, M.; Tarlatzis, B.C.; Bontis, J.N.; Devroey, P. Clinical implications of uterine malformations and hysteroscopic treatment results. Hum. Reprod. Update 2001, 7, 161–174. [Google Scholar] [CrossRef]
- Hollett-Caines, J.; Vilos, G.A.; Abu-Rafea, B.; Ahmad, R. Fertility and pregnancy outcomes following hysteroscopic septum division. J. Obstet. Gynaecol. Can. 2006, 28, 156–159. [Google Scholar] [CrossRef]
- American Fertility Society. The American Fertility Society classifications of adnexal adhesions, distal tubal occlusion, tubal occlusion secondary to tubal ligation, tubal pregnancies, müllerian anomalies and intrauterine adhesions. Fertil. Steril. 1988, 49, 944–955. [Google Scholar] [CrossRef]
- Practice Committee of the American Society for Reproductive Medicine. Uterine septum: A guideline. Fertil. Steril. 2016, 106, 530–540. [Google Scholar] [CrossRef] [Green Version]
- Grimbizis, G.F.; Gordts, S.; Di Spiezio Sardo, A.; Brucker, S.; De Angelis, C.; Gergolet, M.; Li, T.-C.; Tanos, V.; Brölmann, H.; Gianaroli, L.; et al. The ESHRE/ESGE consensus on the classification of female genital tract congenital anomalies. Hum. Reprod. 2013, 28, 2032–2044. [Google Scholar] [CrossRef] [Green Version]
- Ludwin, A.; Martins, W.P.; Nastri, C.O.; Ludwin, I.; Coelho Neto, M.A.; Leitão, V.M.; Acién, M.; Alcazar, J.L.; Benacerraf, B.; Condous, H.; et al. Congenital Uterine Malformation by Experts (CUME): Better criteria for distinguishing between normal/arcuate and septate uterus? Ultrasound Obstet. Gynecol. 2018, 51, 101–109. [Google Scholar] [CrossRef]
- Hua, M.; Odibo, A.O.; Longman, R.E.; Macones, G.A.; Roehl, K.A.; Cahill, A.G. Congenital uterine anomalies and adverse pregnancy outcomes. Am. J. Obstet. Gynecol. 2011, 205, 558.e1–558.e5. [Google Scholar] [CrossRef]
- Prior, M.; Richardson, A.; Asif, S.; Polanski, L.; Parris-Larkin, M.; Chandler, J.; Fogg, L.; Jassal, P.; Thornton, J.G.; Raine-Fenning, N.J. Outcome of assisted reproduction in women with congenital uterine anomalies: A prospective observational study. Ultrasound Obstet. Gynecol. 2018, 51, 110–117. [Google Scholar] [CrossRef] [Green Version]
- Valle, R.F.; Ekpo, G.E. Hysteroscopic metroplasty for the septate uterus: Review and meta-analysis. J. Minim. Invasive Gynecol. 2013, 20, 22–42. [Google Scholar] [CrossRef] [PubMed]
- Saygili-Yilmaz, E.; Yildiz, S.; Erman-Akar, M.; Akyuz, G.; Yilmaz, Z. Reproductive outcome of septate uterus after hysteroscopic metroplasty. Arch. Gynecol. Obstet. 2003, 268, 289–292. [Google Scholar] [CrossRef] [PubMed]
- Venetis, C.A.; Papadopoulos, S.P.; Campo, R.; Gordts, S.; Tarlatzis, B.C.; Grimbizis, G.F. Clinical implications of congenital uterine anomalies: A meta-analysis of comparative studies. Reprod. Biomed. Online 2014, 29, 665–683. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Acién, P. Reproductive performance of women with uterine malformations. Hum. Reprod. 1993, 8, 122–126. [Google Scholar] [CrossRef] [PubMed]
- Maneschi, F.; Zupi, E.; Marconi, D.; Valli, E.; Romanini, C.; Mancuso, S. Hysteroscopically detected asymptomatic müllerian anomalies. Prevalence and reproductive implications. J. Reprod. Med. 1995, 40, 684–688. [Google Scholar] [PubMed]
- Raga, F.; Bauset, C.; Remohi, J.; Bonilla-Musoles, F.; Simón, C.; Pellicer, A. Reproductive impact of congenital Müllerian anomalies. Hum. Reprod. 1997, 12, 2277–2281. [Google Scholar] [CrossRef] [PubMed]
- Mollo, A.; De Franciscis, P.; Colacurci, N.; Cobellis, L.; Perino, A.; Venezia, R.; Alviggi, C.; De Placido, G. Hysteroscopic resection of the septum improves the pregnancy rate of women with unexplained infertility: A prospective controlled trial. Fertil. Steril. 2009, 91, 2628–2631. [Google Scholar] [CrossRef]
- Shokeir, T.; Abdelshaheed, M.; El-Shafie, M.; Sherif, L.; Badawy, A. Determinants of fertility and reproductive success after hysteroscopic septoplasty for women with unexplained primary infertility: A prospective analysis of 88 cases. Eur. J. Obstet. Gynecol. Reprod. Biol. 2011, 155, 54–57. [Google Scholar] [CrossRef]
- Tonguc, E.A.; Var, T.; Batioglu, S. Hysteroscopic metroplasty in patients with a uterine septum and otherwise unexplained infertility. Int. J. Gynaecol. Obstet. 2011, 113, 128–130. [Google Scholar] [CrossRef]
- Sparac, V.; Kupesic, S.; Ilijas, M.; Zodan, T.; Kurjak, A. Histologic architecture and vascularization of hysteroscopically excised intrauterine septa. J. Am. Assoc. Gynecol. Laparosc. 2001, 8, 111–116. [Google Scholar] [CrossRef]
- Rikken, J.; Leeuwis-Fedorovich, N.E.; Letteboer, S.; Emanuel, M.H.; Limpens, J.; van der Veen, F.; Goddijn, M.; van Wely, M. The pathophysiology of the septate uterus: A systematic review. BJOG Int. J. Obstet. Gynaecol. 2019, 126, 1192–1199. [Google Scholar] [CrossRef] [PubMed]
- Rikken, J.F.W.; Kowalik, C.R.; Emanuel, M.H.; Bongers, M.Y.; Spinder, T.; Jansen, F.W.; Mulders, A.G.M.G.J.; Padmehr, R.; Clark, T.J.; van Vliet, H.A.; et al. Septum resection versus expectant management in women with a septate uterus: An international multicentre open label randomized controlled trial. Hum. Reprod. 2021, 36, 1260–1267. [Google Scholar] [CrossRef]
- Stroup, D.F.; Berlin, J.A.; Morton, S.C.; Olkin, I.; Williamson, G.D.; Rennie, D.; Moher, D.; Becker, B.J.; Sipe, T.A.; Thacker, S.B. Meta-analysis of observational studies in epidemiology: A proposal for reporting. Meta-analysis Of Observational Studies in Epidemiology (MOOSE) group. JAMA 2000, 283, 2008–2012. [Google Scholar] [CrossRef]
- Jarcho, J. Malformations of the uterus. Am. J. Surg. 1946, 71, 106–166. [Google Scholar] [CrossRef]
- Buttram, V.C., Jr.; Gibbons, W.E. Müllerian anomalies: A proposed classification. (An analysis of 144 cases). Fertil. Steril. 1979, 32, 40–46. [Google Scholar] [CrossRef]
- Woelfer, B.; Salim, R.; Banerjee, S.; Elson, J.; Regan, L.; Jurkovic, D. Reproductive outcomes in women with congenital uterine anomalies detected by three-dimensional ultrasound screening. Obstet. Gynecol. 2001, 98, 1099–1103. [Google Scholar] [CrossRef] [PubMed]
- Ozgur, K.; Isikoglu, M.; Donmez, L.; Oehninger, S. Is hysteroscopic correction of an incomplete uterine septum justified prior to IVF? Reprod. Biomed. Online 2007, 14, 335–340. [Google Scholar] [CrossRef]
- Zlopasa, G.; Skrablin, S.; Kalafatić, D.; Banović, V.; Lesin, J. Uterine anomalies and pregnancy outcome following resectoscope metroplasty. Int. J. Gynaecol. Obstet. 2007, 98, 129–133. [Google Scholar] [CrossRef]
- Ban-Frangez, H.; Tomazevic, T.; Virant-Klun, I.; Verdenik, I.; Ribic-Pucelj, M.; Bokal, E.V. The outcome of singleton pregnancies after IVF/ICSI in women before and after hysteroscopic resection of a uterine septum compared to normal controls. Eur. J. Obstet. Gynecol. Reprod. Biol. 2009, 146, 184–187. [Google Scholar] [CrossRef]
- Sugiura-Ogasawara, M.; Ozaki, Y.; Kitaori, T.; Kumagai, K.; Suzuki, S. Midline uterine defect size is correlated with miscarriage of euploid embryos in recurrent cases. Fertil. Steril. 2010, 93, 1983–1988. [Google Scholar] [CrossRef]
- Tomaževič, T.; Ban-Frangež, H.; Virant-Klun, I.; Verdenik, I.; Požlep, B.; Vrtačnik-Bokal, E. Septate, subseptate and arcuate uterus decrease pregnancy and live birth rates in IVF/ICSI. Reprod. Biomed. Online 2010, 21, 700–705. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saravelos, S.H.; Cocksedge, K.A.; Li, T.C. The pattern of pregnancy loss in women with congenital uterine anomalies and recurrent miscarriage. Reprod. Biomed. Online 2010, 20, 416–422. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jayaprakasan, K.; Chan, Y.Y.; Sur, S.; Deb, S.; Clewes, J.S.; Raine-Fenning, N.J. Prevalence of uterine anomalies and their impact on early pregnancy in women conceiving after assisted reproduction treatment. Ultrasound Obstet. Gynecol. 2011, 37, 727–732. [Google Scholar] [CrossRef]
- Heinonen, P.K. Reproductive performance of women with uterine anomalies after abdominal or hysteroscopic metroplasty or no surgical treatment. J. Am. Assoc. Gynecol. Laparosc. 1997, 4, 311–317. [Google Scholar] [CrossRef]
- Valli, E.; Vaquero, E.; Lazzarin, N.; Caserta, D.; Marconi, D.; Zupi, E. Hysteroscopic metroplasty improves gestational outcome in women with recurrent spontaneous abortion. J. Am. Assoc. Gynecol. Laparosc. 2004, 11, 240–244. [Google Scholar] [CrossRef]
- Lin, K.; Zhu, X.; Xu, H.; Liang, Z.; Zhang, X. Reproductive outcome following resectoscope metroplasty in women having a complete uterine septum with double cervix and vagina. Int. J. Gynaecol. Obstet. 2009, 105, 25–28. [Google Scholar] [CrossRef]
- Pang, L.H.; Li, M.J.; Li, M.; Xu, H.; Wei, Z.L. Not every subseptate uterus requires surgical correction to reduce poor reproductive outcome. Int. J. Gynaecol. Obstet. 2011, 115, 260–263. [Google Scholar] [CrossRef]
- Sugiura-Ogasawara, M.; Lin, B.L.; Aoki, K.; Maruyama, T.; Nakatsuka, M.; Ozawa, N.; Sugi, T.; Takeshita, T.; Nishida, M. Does surgery improve live birth rates in patients with recurrent miscarriage caused by uterine anomalies? J. Obstet. Gynaecol. 2015, 35, 155–158. [Google Scholar] [CrossRef]
- Rikken, J.F.W.; Verhorstert, K.W.J.; Emanuel, M.H.; Bongers, M.Y.; Spinder, T.; Kuchenbecker, W.; Jansen, F.W.; van der Steeg, J.W.; Janssen, C.A.H.; Kapiteijn, K.; et al. Septum resection in women with a septate uterus: A cohort study. Hum. Reprod. 2020, 35, 1722. [Google Scholar] [CrossRef]
- Whelan, A.; Burks, C.; Stephenson, M.D. Pregnancy Outcomes in Women With a History of Recurrent Early Pregnancy Loss and a Septate Uterus, With and Without Hysteroscopic Metroplasty. Obstet. Gynecol. 2020, 136, 417–419. [Google Scholar] [CrossRef]
- Valle, R.F.; Sciarra, J.J. Hysteroscopic treatment of the septate uterus. Obstet. Gynecol. 1986, 67, 253–257. [Google Scholar] [CrossRef] [PubMed]
- Guarino, S.; Incandela, S.; Maneschi, M.; Vegna, G.; D’Anna, M.R.; Leone, S.; Maneschi, F. Hysteroscopic treatment of uterine septum. Acta Eur. Fertil. 1989, 20, 321–325. [Google Scholar] [PubMed]
- Choe, J.K.; Baggish, M.S. Hysteroscopic treatment of septate uterus with Neodymium-YAG laser. Fertil. Steril. 1992, 57, 81–84. [Google Scholar] [CrossRef]
- Grimbizis, G.; Camus, M.; Clasen, K.; Tournaye, H.; De Munck, L.; Devroey, P. Hysteroscopic septum resection in patients with recurrent abortions or infertility. Hum. Reprod. 1998, 13, 1188–1193. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jourdain, O.; Dabysing, F.; Harle, T.; Lajus, C.; Roux, D.; Dallay, D. Management of septate uterus by flexible hysteroscopy and Nd:YAG laser. Int. J. Gynaecol. Obstet. 1998, 63, 159–162. [Google Scholar] [CrossRef]
- Porcu, G.; Cravello, L.; D’Ercole, C.; Cohen, D.; Roger, V.; de Montgolfier, R.; Blanc, B. Hysteroscopic metroplasty for septate uterus and repetitive abortions: Reproductive outcome. Eur. J. Obstet. Gynecol. Reprod. Biol. 2000, 88, 81–84. [Google Scholar] [CrossRef]
- Venturoli, S.; Colombo, F.M.; Vianello, F.; Seracchioli, R.; Possati, G.; Paradisi, R. A study of hysteroscopic metroplasty in 141 women with a septate uterus. Arch. Gynecol. Obstet. 2002, 266, 157–159. [Google Scholar] [CrossRef]
- Yang, J.; Yin, T.L.; Xu, W.M.; Xia, L.B.; Li, A.B.; Hu, J. Reproductive outcome of septate uterus after hysteroscopic treatment with neodymium:YAG laser. Photomed. Laser Surg. 2006, 24, 625. [Google Scholar] [CrossRef]
- Wang, J.H.; Xu, K.H.; Lin, J.; Chen, X.Z. Hysteroscopic septum resection of complete septate uterus with cervical duplication, sparing the double cervix in patients with recurrent spontaneous abortions or infertility. Fertil. Steril. 2009, 91, 2643–2649. [Google Scholar] [CrossRef]
- Roy, K.K.; Singla, S.; Baruah, J.; Kumar, S.; Sharma, J.B.; Karmakar, D. Reproductive outcome following hysteroscopic septal resection in patients with infertility and recurrent abortions. Arch. Gynecol. Obstet. 2011, 283, 273–279. [Google Scholar] [CrossRef]
- Sendag, F.; Mermer, T.; Yucebilgin, S.; Oztekin, K.; Bilgin, O. Reproductive outcomes after hysteroscopic metroplasty for uterine septum. Clin. Exp. Obstet. Gynecol. 2010, 37, 287–289. [Google Scholar] [PubMed]
- Gergolet, M.; Campo, R.; Verdenik, I.; Kenda Suster, N.; Gordts, S.; Gianaroli, L. No clinical relevance of the height of fundal indentation in subseptate or arcuate uterus: A prospective study. Reprod. Biomed. Online 2012, 24, 576–582. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bendifallah, S.; Faivre, E.; Legendre, G.; Deffieux, X.; Fernandez, H. Metroplasty for AFS Class V and VI septate uterus in patients with infertility or miscarriage: Reproductive outcomes study. J. Minim. Invasive Gynecol. 2013, 20, 178–184. [Google Scholar] [CrossRef]
- Gundabattula, S.R.; Joseph, E.; Marakani, L.R.; Dasari, S.; Nirmalan, P.K. Reproductive outcomes after resection of intrauterine septum. J. Obstet. Gynaecol. 2014, 34, 235–237. [Google Scholar] [CrossRef] [PubMed]
- Paradisi, R.; Barzanti, R.; Natali, F.; Guerrini, M.; Battaglia, C.; Seracchioli, R.; Venturoli, S. Hysteroscopic metroplasty: Reproductive outcome in relation to septum size. Arch. Gynecol. Obstet. 2014, 289, 671–676. [Google Scholar] [CrossRef]
- John, B.M.; Mathew, S.; Suresh, A. Reproductive Outcome Analysis of 286 Women Who Underwent Hysteroscopic Septum Resection for Complete and Partial Septum of the Uterus. J. Minim. Invasive Gynecol. 2015, 22 (Suppl. S6), S110–S111. [Google Scholar] [CrossRef] [PubMed]
- Freud, A.; Harlev, A.; Weintraub, A.Y.; Ohana, E.; Sheiner, E. Reproductive outcomes following uterine septum resection. J. Matern. Fetal Neonatal Med. 2015, 28, 2141–2144. [Google Scholar] [CrossRef]
- Wang, X.; Hou, H.; Yu, Q. Fertility and pregnancy outcomes following hysteroscopic metroplasty of different sized uterine septa: A retrospective cohort study protocol. Medicine 2019, 98, e16623. [Google Scholar] [CrossRef]
- Slim, K.; Nini, E.; Forestier, D.; Kwiatkowski, F.; Panis, Y.; Chipponi, J. Methodological index for non-randomized studies (minors): Development and validation of a new instrument. ANZ J. Surg. 2003, 73, 712–716. [Google Scholar] [CrossRef] [PubMed]
- Viechtbauer, W. Conducting meta-analyses in R with the metafor package. J. Stat. Softw. 2010, 36, 1–48. [Google Scholar] [CrossRef] [Green Version]
- R Core Team. R: A language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2020. [Google Scholar]
- Higgins, J.P.T.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef]
- Duval, S.J.; Tweedie, R.L. Trim and fill: A simple funnel-plot-based method of testing and adjusting for publication bias in meta-analysis. Biometrics 2000, 56, 455–463. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, W.A. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions; Version 6.1 (Updated September 2020); John Wiley & Sons: Hoboken, NJ, USA, 2020; Available online: www.training.cochrane.org/handbook (accessed on 1 September 2020).
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The PRISMA Group. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alonso Pacheco, L.; Ata, B.; Bettocchi, S.; Campo, R.; Carugno, J.; Checa, M.A.; de Angelis, C.; Di Spiezio Sardo, A.; Donnez, J.; Farrugia, M.; et al. Septate uterus and reproductive outcomes: Let’s get serious about this. Hum. Reprod. 2020, 35, 2627–2629. [Google Scholar] [CrossRef] [PubMed]
- Chan, Y.Y.; Jayaprakasan, K.; Tan, A.; Thornton, J.G.; Coomarasamy, A.; Raine-Fenning, N.J. Reproductive outcomes in women with congenital uterine anomalies: A systematic review. Ultrasound Obstet. Gynecol. 2011, 38, 371–382. [Google Scholar] [CrossRef]
- Hume, H.; Chasen, S.T. Trends in timing of prenatal diagnosis and abortion for fetal chromosomal abnormalities. Am. J. Obstet. Gynecol. 2015, 213, 545.e1–545.e4. [Google Scholar] [CrossRef]
- Ambühl, L.M.; Baandrup, U.; Dybkær, K.; Blaakær, J.; Uldbjerg, N.; Sørensen, S. Human Papillomavirus Infection as a Possible Cause of Spontaneous Abortion and Spontaneous Preterm Delivery. Infect. Dis. Obstet. Gynecol. 2016, 2016, 3086036. [Google Scholar] [CrossRef] [Green Version]
- Gupta, S.; Agarwal, A.; Banerjee, J.; Alvarez, J.G. The role of oxidative stress in spontaneous abortion and recurrent pregnancy loss: A systematic review. Obstet. Gynecol. Surv. 2007, 62, 335–347. [Google Scholar] [CrossRef] [Green Version]
- Di Spiezio Sardo, A.; Zizolfi, B.; Bettocchi, S.; Exacoustos, C.; Nocera, C.; Nazzaro, G.; da Cunha Vieira, M.; Nappi, C. Accuracy of Hysteroscopic Metroplasty With the Combination of Presurgical 3-Dimensional Ultrasonography and a Novel Graduated Intrauterine Palpator: A Randomized Controlled Trial. J. Minim. Invasive Gynecol. 2016, 23, 557–566. [Google Scholar] [CrossRef]
- Salazar, C.A.; Isaacson, K.B. Office Operative Hysteroscopy: An Update. J. Minim. Invasive Gynecol. 2018, 25, 199–208. [Google Scholar] [CrossRef]
- Vercellini, P.; Chiaffarino, F.; Parazzini, F. ‘It’s all too much’: The shadow of overtreatment looms over hysteroscopic metroplasty for septate uterus. Hum. Reprod. 2021, 36, 1166–1170. [Google Scholar] [CrossRef] [PubMed]
- Bosteels, J.; van Wessel, S.; Weyers, S.; Broekmans, F.J.; D’Hooghe, T.M.; Bongers, M.Y.; Mol, B.W.J. Hysteroscopy for treating subfertility associated with suspected major uterine cavity abnormalities. Cochrane Database Syst Rev. 2018, 12, CD009461. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krishnan, M.; Narice, B.F.; Ola, B.; Metwally, M. Does hysteroscopic resection of uterine septum improve reproductive outcomes: A systematic review and meta-analysis. Arch. Gynecol. Obstet. 2021, 303, 1131–1142. [Google Scholar] [CrossRef] [PubMed]
- Carrera, M.; Pérez Millan, F.; Alcázar, J.L.; Alonso, L.; Caballero, M.; Carugno, J.; Dominguez, J.A.; Moratalla, E. Effect of Hysteroscopic Metroplasty on Reproductive Outcomes in Women with Septate Uterus: Systematic Review and Meta-Analysis. J. Minim. Invasive Gynecol. 2022, 29, 465–475. [Google Scholar] [CrossRef]
- Homer, H.A.; Li, T.C.; Cooke, I.D. The septate uterus: A review of management and reproductive outcome. Fertil. Steril. 2000, 73, 1–14. [Google Scholar] [CrossRef]
- Candiani, G.B.; Fedele, L.; Zamberletti, D.; De Virgillis, D.; Carinelli, S. Endometrial patterns in malformed uteri. Acta Eur. Fertil. 1983, 14, 311–318. [Google Scholar]
- Fascilla, F.D.; Resta, L.; Cannone, R.; De Palma, D.; Ceci, O.R.; Loizzi, V.; Di Spiezio Sardo, A.; Campo, R.; Cicinelli, E.; Bettocchi, S. Resectoscopic Metroplasty with Uterine Septum Excision: A Histologic Analysis of the Uterine Septum. J. Minim. Invasive Gynecol. 2020, 27, 1287–1294. [Google Scholar] [CrossRef]
- Taylor, H.S. The role of HOX genes in human implantation. Hum. Reprod. Update 2000, 6, 75–79. [Google Scholar] [CrossRef] [Green Version]
- Dabirashrafi, H.; Bahadori, M.; Mohammad, K.; Alavi, M.; Moghadami-Tabrizi, N.; Zandinejad, K. Septate uterus: New idea on the histologic features of the septum in this abnormal uterus. Am. J. Obstet. Gynecol 1995, 172 Pt 1, 105–107. [Google Scholar] [CrossRef]
- Fedele, L.; Bianchi, S.; Marchini, M.; Franchi, D.; Tozzi, L.; Dorta, M. Ultrastructural aspects of endometrium in Infertile women with septate uterus. Fertil. Steril. 1996, 65, 750–752. [Google Scholar] [CrossRef]
- National Institute for Health and Care Excellence. Hysteroscopic Metroplasty of a Uterine Septum for Primary Infertility—Interventional Procedures Guidance; National Institute for Health and Care Excellence: London, UK, 2015. Available online: nice.org.uk/guidance/ipg509 (accessed on 1 May 2022).





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Design | Period | Population | Exclusion Criteria | Cases | Controls | Sample Size; Case/Control | Outcomes | Follow-Up | Mode of Diagnosis | Method of Classification |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Acien et al., 1993, [14] | Retrospective | 1980–1991 | Infertile: if attempts to achieve pregnancy remained unsuccessful for >two years. Recurrent miscarriage Natural conception | Patients with: Rokitansky syndrome, hypoplastic, arcuate, bicornuate, didelphis, unicornuate uterus. | Septate uterus Subseptate uterus | No malformations. | 31/28 | Pregnancy rate Live birth rate Spontaneous abortion Preterm labour | 24 months | Clinical examination, ultrasound hysterosalpingographypyelography. | Jarcho (1946) [24], Buttram and Gibbons (1979) [25] and the AFS (1988) criteria [5] |
| Woelfer et al., 2001, [26] | Prospective | Aug 1997 to Sep 2000 | Infertile Recurrent miscarriage Natural conception | Women ongoing pregnancy, history of infertility or recurrent miscarriage, presence of uterine fibroids that distorted the uterine cavity. | Subseptate uterus | No malformations. | 29/983 | Pregnancy rate Spontaneous abortion Preterm labour | - | 3D TV-US | AFS (1988) criteria [5] |
| Ozgur et al., 2007, [27] | Retrospective | Jan 2002 to June 2004 | Infertile: Male factor Tubal factor Other female factor Unexplained Multifactorial ART conception: IVF | Not reported. | Septate uterus | No malformations. | 119/116 | Spontaneous abortion | - | 2D TV-US HSC | N/A |
| Zlopaša et al., 2007, [28] | Retrospective | 1997–2000 | Recurrent miscarriage: experienced at least two early spontaneous abortions Natural conception | Twin gestations, submucosal myomas, fetal chromosomopathy, IVF; arcuate bicornuate, didelphys, unicornuate uterus. | Septate uterus Subseptate uterus | No malformations. | 31/182 | Spontaneous abortion Preterm labour | - | Surgery hysterosalpingograph sonohysterography laparoscopy HSC | AFS (1988) criteria [5] |
| Ban-Frangez et al., 2009, [29] | Retrospective | 1993–2004. | Infertile: Tubal factor Endometriosis Endocrinologic Male factor Idiopathic ART conception: IVF or ICSI | Extrauterine pregnancies, multiple pregnancies and cases with an empty gestational sac. | Septate uterus | No malformations. | 106/212 | Spontaneous abortion | - | 2D TV-US HSC | AFS (1988) criteria [5] |
| Sugiura-Ogasawara et al., 2010, [30] | Retrospective | 1986–2007. | Recurrent miscarriage: two or more (two–12) consecutive miscarriages whose subsequent pregnancies Natural conception | Patients with chromosome abnormalities, unicornuate, bicornuate, didelphis uterus. | Septate uterus | No malformations. | 10/1528 | Pregnancy rate Spontaneous abortion | - | Laparoscopy Laparotomy MRI | AFS (1988) criteria [5] |
| Tomazevic et al., 2010, [31] | Retrospective | 1993–2005 | Infertile: Tubal factor Endometriosis Endocrinologic Male factor Idiopathic ART conception: IVF or ICSI | Not reported. | Septate uterus | No malformations. | 289 embryo transfers, 1654 embryo transfers as controls. | Pregnancy rate Live birth rate Spontaneous abortion | - | 2D TV-US HSC | AFS (1988) criteria [5] |
| Saravelos et al., 2010, [32] | Retrospective | N/A | Recurrent miscarriage: was defined as three or more consecutive pregnancy losses prior to 24 weeks of gestation Natural conception | Pregnancies in which patients received medical treatment or surgery. | Septate uterus | No malformations. | 29/107 | Live birth rate Spontaneous abortion | - | 2D TV-US Hysterosalpingography | AFS (1988) criteria [5] |
| Jayaprakasan et al., 2011, [33] | Prospective | 2005–2009 | Infertile: Tubal factor Endometriosis Endocrinologic Male factor Idiopathic ART conception: IVF or ICSI | Patients found to have one or more uterine fibroids or polyps distorting the endometrial cavity. | Septate uterus | No malformations. | 7/364 | Pregnancy rate Spontaneous abortion | - | 3D TV-US | AFS (1988) criteria [5] |
| Prior et al., 2017, [10] | Prospective | May 2009 to November 2015 | Infertile: Tubal factor Endometriosis Endocrinologic Male factor Idiopathic ART conception: IVF or ICSI | Patients with a bicornuate uterus Not possible to make a definitive diagnosis for limited views, distortion of endometrial cavity by fibroids, and intrauterine contraceptive device in situ. | Septate uterus Subseptate uterus | No malformations. | 23/1943 | Pregnancy rate Live birth rate Spontaneous abortion | Present but not specified | 3D TV-US | AFS (1988) criteria [5] |
| Study | Design | Period | Population | Exclusion Criteria | Sample Size; Case/Control | Outcomes | Cases | Controls | Follow-Up | Type of Hysetroscopy | Procedure/Metroplasty | Mode of Diagnosis | Method of Classification |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Heinonen et al., 1997, [34] | Retrospective | 1962–1995 | Women who experienced recurrent abortions and/or infertility. Natural conception Recurrent miscarriage: one or more miscarriages | N/A | 19/19 | Pregnancy rate Spontaneous abortion Preterm labour Live birth rate | Women with uterine septum and subseptum who underwent hysteroscopic metroplasty. Septate uterus Subseptate uterus | Septate and subseptate with no treatment matched by age, gravidity and type of uterine anomaly. | Mean nine years (nine months—25 years) | 26-gauge resectoscope (Karl Storz). | Jones procedure and Tompkins procedure respectively in six and 14 cases. | Not reported. | Buttram and Gibbons (1979) [25] criteria |
| Valli et al., 2004, [35] | Prospective | 1990–2001. | Women who experienced recurrent abortions. Recurrent miscarriage: at least two miscarriages. Natural conception | Women with bicornuate uterus. | 28/15 | Pregnancy rate Spontaneous abortion Preterm labour Live birth rate | Women with uterine septum who underwent hysteroscopic metroplasty. Septate uterus | Untreated women. | 36 months | Hamou hysteroscope (Karl Storz). | Resectoscope loop. Septum incision was performed until the underlying myometrial tissue. | HSC | AFS (1988) criteria [5] |
| Ban-Frangez et al., 2009, [29] | Retrospective | 1993–2004. | Women with uterine septum that underwent IVF or ICSI and had a singleton pregnancy (fetal heart activity by ultrasound demonstration) Infertile: Tubal factor Endometriosis Endocrinologic Male factor Idiopathic ART conception: IVF or ICSI | Extrauterine pregnancies, multiple pregnancies and cases with an empty gestational sac. | 106/212 | Spontaneous abortion Preterm labour | Women who had conceived after IVF or ICSI. Septate uterus | Women without uterine anomalies with a singleton pregnancy after IVF or ICSI | - | N/A | N/A | 2D TV-US HSC | AFS (1988) criteria [5] |
| Lin et al., 2009, [36] | Retrospective | 1998–2007. | Complete septum (from fundus to vagina). Infertile: defined as unsuccessfully trying to conceive for at least 1 full year Recurrent miscarriage: at least two miscarriages. Natural conception | Other abnormalities than utero- cervico-vaginal septum. | 21/15 | Pregnancy rate Spontaneous abortion Preterm labour Live birth rate | Vaginal septum removal plus hysteroscopic resection of the uterus septum. Septate uterus | Women that remained untreated. | Mean 18 months (six months—nine years) | N/A | N/A | 3D TV-US hysterosalpingography | N/A |
| Pang et al., 2011, [37] | Prospective | January 2006 to March 2011. | Women with subseptate uterus and who have experienced recurrent spontaneous abortions (two first- trimester abortions). Recurrent miscarriage: at least two first-trimester Natural conception | Only one spontaneous abortion. | 46/32 | Spontaneous abortion Preterm labour Live birth rate | Women with uterine subseptum and who have experienced recurrent spontaneous abortion. Subseptate uterus | Women with subseptate uterus and who have experienced recurrent spontaneous abortion not treated with hysteroscopic metroplasty. | 15 months | N/A | N/A | 3D TV-US | AFS (1988) criteria [5] |
| Tonguc et al., 2011, [19] | Retrospective | January 2006 to January 2009. | Patients with a uterine septum and otherwise unexplained infertility. Infertile Natural conception | Patients who had a history of tuberculosis or endometriosis, endocrinologic problem, abdominal surgery, husband with mild or severe oligospermia at the spermiogram. | 102/25 | Pregnancy rate Spontaneous abortion Preterm labour Live birth rate | Women with uterine septum who underwent hysteroscopic metroplasty. Septate uterus | Patients who rejected the surgery. | 14 months | 26-Fr rigid hysteroscope (Karl Storz). | Incision of the septa at the lower margin and continued upward with a horizontal section from one tubal ostium to the other. | N/A | AFS (1988) criteria [5] |
| Sugiura-Ogasawara et al., 2014, [38] | Prospective | January 2003 to June 2009. | Women with a history of two or more consecutive miscarriages or one stillbirth and septate uterus. Recurrent miscarriage: at least two consecutive miscarriages Natural conception | Patients with a bicornuate uterus. | 109/15 | Pregnancy rate Spontaneous abortion Preterm labour Live birth rate | Women with uterine septum who underwent hysteroscopic metroplasty. Septate uterus | Patients who rejected the surgery. | Present but Not specified | N/A | Transcervical resection (TCR) or a Jones modified metroplasty. | Hysterosalpingography and/or 2D transvaginal ultrasound were used as the initial screening. Laparoscopy/ laparotomy and/or MRI | AFS (1988) criteria [5] |
| Rikken et al., 2020, [39] | Retrospective | January 2000 to August 2018. | Women with a history of subfertility, pregnancy loss or preterm birth. Infertile: defined as the inability to conceive for a minimal period of one year of trying to conceive Recurrent miscarriage: two or more, not necessarily consecutive Natural conception | Women that do not have a wish to conceive at time of diagnosis. | 151/106 | Pregnancy rate Spontaneous abortion Preterm labour Live birth rate | Women with uterine septum who underwent hysteroscopic metroplasty. Septate uterus Subseptate uterus | Women who had expectant management. | Mean 46 months | 73 procedures performed with a Versa point device. 32 with scissors. 12 with electro-surgery. 34 unknown. | Intrauterine septum was completely removed. | Hysterosalpingography, 3D TV-US MRI saline or gel infusion sonohysterography or hysteroscopy combined with laparoscopy. | AFS (1988)[5] and ASMR (2016) [6] criteria |
| Whelan et al., 2020, [40] | Prospective | July 2004 to May 2012 | Women with recurrent early pregnancy loss, uterine septum diagnosed and one subsequent pregnancy. Recurrent miscarriage: two or more documented pregnancy losses before 10 weeks of gestation | N/A | 21/11 | Spontaneous abortion Preterm labour Live birth rate | Women with recurrent early pregnancy loss, uterine septum diagnosed and one subsequent pregnancy who underwent histeroscopic metroplasty. Septate uterus | Women with recurrent early pregnancy loss, uterine septum diagnosed and one subsequent pregnancy untreated. | N/A | N/A | N/A | HSC 3D TV-US | ASMR (2016) criteria [6] |
| Study | Design | Period | Population | Exclusion Criteria | Simple Size | Case | Outcomes | Follow-Up | Type of Hysteroscopic | Procedure/Metroplasty | Mode of Diagnosis | Method of Classification |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Valle et al., 1986, [41] | Retrospective | N/A | Infertile Recurrent miscarriage Natural conception | N/A | 124 | Women with uterine septum who underwent hysteroscopic metroplasty. | Spontaneous abortion Preterm labour | N/A | N/A | N/A | N/A | N/A |
| Guarino et al., 1989, [42] | Retrospective | N/A | Infertile Recurrent miscarriage Natural conception | N/A | 19 | Women with uterine septum who underwent hysteroscopic metroplasty. | Spontaneous abortion Preterm labour | six months | N/A | N/A | N/A | N/A |
| Choe et al., 1992, [43] | Retrospective | August 1986 to April 1990. | Infertile Recurrent miscarriage Natural conception | N/A | 14 | Women with uterine septum who underwent hysteroscopic metroplasty. | Spontaneous abortion Preterm labour | N/A | Nd-YAG laser with an 8-mm operating hysteroscope. | An incision was made from one cornua down the septum, then across the septum. Next, beginning at the opposite cornua, the same procedure was done until each tubal ostium could be seen in the panoramic hysteroscopic view. | Laparoscopy HSC | N/A |
| Grimbizis et al., 1998, [44] | Retrospective | January 1991 to Dec 1996. | Infertile: Tubal factor Endometriosis Endocrinologic Male factor Idiopathic Recurrent miscarriage: two or more previous miscarriages ART conception: IVF or ICSI Natural conception | N/A | 57 | Septate uterus Subseptate uterus | Spontaneous abortion Preterm labour | 34 months | Rigid hysteroscope mounted with a rotatable 9 mm resectoscope. | Resection from the lower margin of the septum and continued upwards with progressive horizontal incisions in the midline until a normal cavity was obtained. | Laparoscopy HSC | AFS (1988) criteria [5] |
| Jourdain et al., 1998, [45] | Retrospective | 1990–1995. | Infertile Recurrent miscarriage: two or more spontaneous first trimester losses or be infertile. Natural conception | N/A | 17 | Septate uterus | Live birth rate Spontaneous abortion | 41 months | Flexible hysteroscope with Nd-YAG laser. | The septum was divided by the laser after exploration of the cavity. | HSC | N/A |
| Porcu et al., 2000, [46] | Retrospective | Feb 1988 to December 1996. | Recurrent miscarriage Natural conception | N/A | 63 | Septate uterus | Live birth rate Spontaneous abortion Preterm labour | 48 months | 55 procedures performed with a 21-Fr resectoscope. Three procedures with endoscopic scissors. Five procedures with Nd-YAG laser. | Electric section performed in 55 cases (87.3%). Section with a pair of endoscopic scissors in three cases (4.8%). A Nd– Yag laser had been used in five cases (9.5%). The method to divide the septum was chosen on an arbitrary decision and not for a specific reason. | Hysterosalpingography TV-US | N/A |
| Venturoli et al., 2002, [47] | Retrospective | January 1993 to December 1997. | Infertile: unexplained infertility of at least two years duration Recurrent miscarriage: two or more miscarriages in the last three years Natural conception ART conception | No endocrine or other disorders. | 141 | Septate uterus | Live birth rate Spontaneous abortion | 36 ± 19.5 months | Rigid hysteroscope with a 26 gauge resectoscope (Karl Storz) | After visualization of the tubal ostia, the resection was started from the lower margin of the septum and continued upwards with a progressive horizontal incision in the midline. | Laparoscopy HSC | AFS (1988) criteria [5] |
| Saygili-Yilmaz et al., 2003, [12] | Retrospective | 1990–2000. | Infertile: primary infertility who failed to achieve pregnancy for over two years Recurrent miscarriage: two or more miscarriage Natural conception | N/A | 361 | Septate uterus Subseptate uterus | Live birth rate Spontaneous abortion Preterm labour | 36 months | Rigid hysteroscope with 26 gaude resectoscope and specific loop electrode (Karl Storz). | After visualization both of the tubal ostias, the incision of septa was started from the lower margin and continued upward with horizontal section until a normal cavity was obtained and both tubal ostia could be visualized. | Hysterosalpingography | AFS (1988) criteria [5] |
| Yang et al., 2006, [48] | Retrospective | N/A | Infertile Recurrent miscarriage Natural conception | N/A | 46 | Septate uterus Subseptate uterus | Live birth rate Spontaneous abortion | 10.2 ± 1.3 months | Rigid hysteroscopy with operating channel into which an optic fiber can be inserted, connected with a Nd-YAG laser. | Incision of the septum between the anterior and posterior uterine walls extending up to the fundus rather into the fundal myometrium. | Laparoscopy HSC | N/A |
| Wang et al., 2009, [49] | Prospective | Sep 2004 to Oct 2007 | Infertile: the inability to conceive after 12 months of unprotected intercourse Recurrent miscarriage: two or more previous spontaneous miscarriages Natural conception | N/A | 25 | Septate uterus | Live birth rate Spontaneous abortion | 17.6 ± 5.4 months | 27-Fr hysteroresectoscope (Olympus, Hangzhou City, Japan) | The resection was performed between the anterior and posterior uterine walls, extending up to the fundus rather than into the fundal myometrium from the lower margin of the septum | 3D TV-US | AFS (1988) criteria [5] |
| Roy et al., 2011, [50] | Retrospective | January 2000 to June 2008 | Infertile Recurrent miscarriage Natural conception | Presence of endocrine disease, uterine myoma, adnexal disease and abnormal semen parameters in the husband | 152 | Septate uterus Subseptate uterus | Live birth rate Spontaneous abortion Preterm labour | 28 months | A 9-mm working element along with sheath and 4-mm 30° telescope (Karl Storz, Germany) equipped with a hysteroscopic monopolar (Collin’s) | The septum was divided in a cephalad direction until both tubal ostia became clearly available. The resection of septa was stopped at the point when hysteroscope could be moved from one cornual end to another without intervening obstruction, and both tubal ostia could be viewed simultaneously | HSC | AFS (1988) criteria [5] |
| Sendag et al., 2010, [51] | Retrospective | N/A | Infertile Recurrent miscarriage Natural conception | N/A | 30 | Septate uterus Subseptate uterus | Spontaneous abortion Preterm labour | N/A | N/A | N/A | N/A | N/A |
| Gergolet et al., 2012, [52] | Prospective | January 2003 to December 2008. | Recurrent miscarriage: one or more miscarriages Natural conception | Anovulatory cycles, polycystic ovary syndrome and those referred to assisted reproduction treatment. | 72 | Subseptate uterus | Live birth rate Spontaneous abortion | N/A | 8-mm Karl Storzmonopolar operative hysteroscope | N/A | 2D/3D TV-US HSC | AFS (1988) criteria [5] |
| Bendifallah et al., 2013, [53] | Retrospective | January 1999 to December 2009. | Infertile: primary infertility for >3 years as defined by inability to conceive. Recurrent miscarriage: at least two consecutive miscarriages before 16 weeks of gestation. Natural conception ART conception: IVF or ICSI | N/A | 128 | Septate uterus | Live birth rate Spontaneous abortion | 38 months | Operative hysteroscope fitted with a monopolar hook (26F resectoscope, 2.9-mm optical lens; Karl Storz GmbH, Tuttlingen, Germany) | the septum was incised equidistant between the anterior and posterior uterine walls, from the lower margin of the septum and continuing upward with progressive horizontal incisions in the midline to the uterine fundus. | HSC | AFS (1988) criteria [5] |
| Gundabattula et al., 2014, [54] | Retrospective | 2003 to 2010. | Infertile: as the inability to conceive aft er 12 months of contraceptive-free intercourse Recurrent miscarriage: 3 or more pregnancy losses before 24 weeks’ gestation Natural conception | N/A | 124 | Septate uterus Subseptate uterus | Live birth rate Spontaneous abortion Preterm labour | 24 months | 26 FR resectoscope with a cutting monopolar electrode or a VersaPoint Hysteroscopy system with a spring-type electrode | The septum was divided in an upward direction until both tubal ostia were visualised in the same plane in a panoramic view of the uterine cavity. | TV-US. Hysterosalpingography | N/A |
| Paradisi et al., 2014, [55] | Retrospective | January 2001 to June 2007. | Infertile Natural conception | Oligo/anovulation and menstrual irregularities | 112 | Subseptate uterus | Live birth rate Spontaneous abortion Preterm labour | N/A | Equatorial semicircular loop, cutting 0° with monopolar energy. | After visualization of the tubal ostia the resection was started from the lower margin of the septum and continued until the muscular component until a normal cavity was obtained and the hysteroscope could be moved freely from one tubal ostium to the other without any intervening obstruction. | HSC 3D TV-US | AFS (1988) criteria [5] |
| John et al. 2015, [56] | Retrospective | 2006 to 2014. | Infertile Natural conception ART conception: IVF or ICSI | N/A | 286 | Septate uterus Subseptate uterus | Live birth rate Spontaneous abortion | N/A | Monopolar cautery loop. | N/A | N/A | N/A |
| Freud et al., 2015, [57] | Retrospective | 2004 to 2011. | Recurrent miscarriage Natural conception ART conception: IVF or ICSI | Multiple pregnancies were excluded from the analysis. | 28 | Septate uterus | Live birth rate Spontaneous abortion | N/A | Bipolar versascope system (Gynecare, Johnson and Johnson, Somerville, NJ, USA) | Septum was divided until complete visualization of both tubal ostia at the same plane was achieved. | HSC 3D TV-US | N/A |
| Wang et al., 2019, [58] | Retrospective | Jul 2006 to January 2017. | Infertile: defined as the inability to conceive for a minimal period of 1 year of trying to conceive Recurrent miscarriage Natural conception | Pelvic lesions, such as endometriosisoligo or anovulation and menstrual irregularities; partners with abnormal semen analysis. | 121 | Septate uterus Subseptate uterus | Live birth rate Spontaneous abortion | 12 | 7 mm rigid hysteroscope (Karl Storz). | Electrosurgical incision in the uterine septum was made equidistantly between the anterior and posterior uterine walls and went up high into the uterine fundus until the presence of a normal-shaped cavity was obtained. | Laparoscopy HSC | AFS (1988) [5] and ASMR (2016) [6] criteria |
| Study | A Clearly Stated Aim | Inclusion of Consecutive Patients | Prospective Collection of Data | Endpoints Appropriate to the Aim of the Study | Unbiased Assessment of the Study Endpoint | Follow-Up Period Appropriate to the Aim of the Study | Loss to Follow Up less than 5% | Prospective Calculation of the Study Size | An Adequate Control Group | Contemporary Groups | Baseline Equivalence of Groups | Adequate Statistical Analyses | Final Score |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Acien et al., 1993. [14] | ** | ** | ** | ** | * | * | ** | * | * | 14 | |||
| Woelfer et al., 2001. [26] | ** | ** | ** | ** | * | * | ** | ** | ** | ** | 18 | ||
| Ozgur et al., 2007. [27] | ** | ** | ** | ** | ** | ** | ** | 14 | |||||
| Zlopaša et al., 2007. [28] | ** | * | * | ** | * | ** | ** | ** | 13 | ||||
| Ban-Frangez et al., 2009. [29] | ** | ** | ** | ** | ** | ** | ** | 14 | |||||
| Sugiura-Ogasawara et al., [30] | ** | ** | ** | * | * | ** | ** | ** | ** | 16 | |||
| Tomazevic et al., 2010. [31] | ** | ** | * | ** | ** | ** | ** | ** | 15 | ||||
| Saravelos et al., 2010. [32] | ** | ** | ** | ** | * | ** | ** | ** | ** | 17 | |||
| Jayaprakasan et al., 2011. [33] | ** | ** | ** | ** | * | * | * | ** | ** | ** | ** | 19 | |
| Prior et al., 2017. [10] | ** | ** | ** | ** | * | * | ** | ** | ** | ** | ** | ** | 22 |
| Study and Year | A clearly stated Aim | Inclusion of Consecutive Patients | Prospective Collection of Data | Endpoints Appropriate to the Aim of the Study | Unbiased Assessment of the Study Endpoint | Follow-Up Period Appropriate to the Aim of the Study | Loss to Follow Up less than 5% | Prospective Calculation of the Study Size | An Adequate Control Group | Contemporary Groups | Baseline Equivalence of Groups | Adequate Statistical Analyses | Final Score |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Heinonen et al., 1997 [34] | ** | * | ** | ** | * | ** | ** | * | ** | * | ** | 18 | |
| Valli et al., 2004 [35] | ** | ** | ** | * | ** | ** | * | ** | ** | ** | ** | 20 | |
| Ban-Frangez et al., 2009 [29] | ** | ** | ** | ** | * | ** | ** | ** | ** | ** | 19 | ||
| Lin et al., 2009 [36] | ** | * | ** | * | * | ** | ** | ** | * | ** | ** | ** | 20 |
| Pang et al., 2011 [37] | ** | ** | ** | ** | * | ** | ** | ** | ** | * | ** | 20 | |
| Tonguc et al., 2011 [19] | ** | ** | ** | ** | ** | ** | * | ** | ** | ** | ** | 21 | |
| Sugiura-Ogasawara et al., 2014 [38] | ** | ** | ** | ** | ** | * | * | * | ** | ** | 17 | ||
| Rikken et al., 2020 [39] | ** | * | ** | ** | * | ** | * | * | ** | ** | ** | 18 | |
| Whelan et al., 2020 [40] | ** | * | * | ** | * | * | * | ** | * | ** | 13 |
| Study and Year | A Clearly Stated Aim | Inclusion of Consecutive Patients | Prospective Collection of Data | Endpoints Appropriate to the Aim of the Study | Unbiased Assessment of the Study Endpoint | Follow-Up Period Appropriate to the Aim of the Study | Loss to Follow Up less than 5% | Prospective Calculation of the Study Size | Final Score |
|---|---|---|---|---|---|---|---|---|---|
| Valle et al., 1986 [41] | ** | * | * | 4 | |||||
| Guarino et al., 1989 [42] | ** | * | ** | 5 | |||||
| Choe et al., 1992 [43] | ** | * | * | * | 5 | ||||
| Grimbizis et al., 1998 [44] | ** | * | ** | ** | * | 8 | |||
| Jourdain et al., 1998 [45] | ** | * | * | ** | * | 7 | |||
| Porcu et al., 2000 [46] | ** | ** | ** | * | 7 | ||||
| Venturoli et al., 2002 [47] | ** | * | ** | * | ** | 8 | |||
| Saygili-Yilmaz et al., 2003 [12] | ** | ** | ** | ** | * | 9 | |||
| Yang et al., 2006 [48] | ** | * | ** | * | * | 7 | |||
| Wang et al., 2009 [49] | ** | ** | ** | ** | * | 9 | |||
| Roy et al., 2011 [50] | ** | ** | ** | ** | ** | 10 | |||
| Sendag et al., 2010 [51] | ** | ** | 4 | ||||||
| Gergolet et al., 2012 [52] | ** | ** | ** | ** | * | * | 10 | ||
| Bendifallah et al., 2013 [53] | ** | ** | ** | ** | * | 9 | |||
| Gundabattula et al., 2014 [54] | ** | ** | ** | * | ** | 9 | |||
| Paradisi et al., 2014 [55] | ** | ** | * | ** | * | 8 | |||
| John et al., 2015 [56] | ** | ** | * | 5 | |||||
| Freud et al., 2015 [57] | ** | ** | ** | 6 | |||||
| Wang et al., 2019 [58] | ** | ** | ** | * | ** | * | 10 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Noventa, M.; Spagnol, G.; Marchetti, M.; Saccardi, C.; Bonaldo, G.; Laganà, A.S.; Cavallin, F.; Andrisani, A.; Ambrosini, G.; Vitale, S.G.; et al. Uterine Septum with or without Hysteroscopic Metroplasty: Impact on Fertility and Obstetrical Outcomes—A Systematic Review and Meta-Analysis of Observational Research. J. Clin. Med. 2022, 11, 3290. https://doi.org/10.3390/jcm11123290
Noventa M, Spagnol G, Marchetti M, Saccardi C, Bonaldo G, Laganà AS, Cavallin F, Andrisani A, Ambrosini G, Vitale SG, et al. Uterine Septum with or without Hysteroscopic Metroplasty: Impact on Fertility and Obstetrical Outcomes—A Systematic Review and Meta-Analysis of Observational Research. Journal of Clinical Medicine. 2022; 11(12):3290. https://doi.org/10.3390/jcm11123290
Chicago/Turabian StyleNoventa, Marco, Giulia Spagnol, Matteo Marchetti, Carlo Saccardi, Giulio Bonaldo, Antonio Simone Laganà, Francesco Cavallin, Alessandra Andrisani, Guido Ambrosini, Salvatore Giovanni Vitale, and et al. 2022. "Uterine Septum with or without Hysteroscopic Metroplasty: Impact on Fertility and Obstetrical Outcomes—A Systematic Review and Meta-Analysis of Observational Research" Journal of Clinical Medicine 11, no. 12: 3290. https://doi.org/10.3390/jcm11123290