
Colistin Monotherapy versus Colistin plus Meropenem Combination Therapy for the Treatment of Multidrug-Resistant Acinetobacter baumannii Infection: A Meta-Analysis



Abstract
:1. Introduction
2. Methods
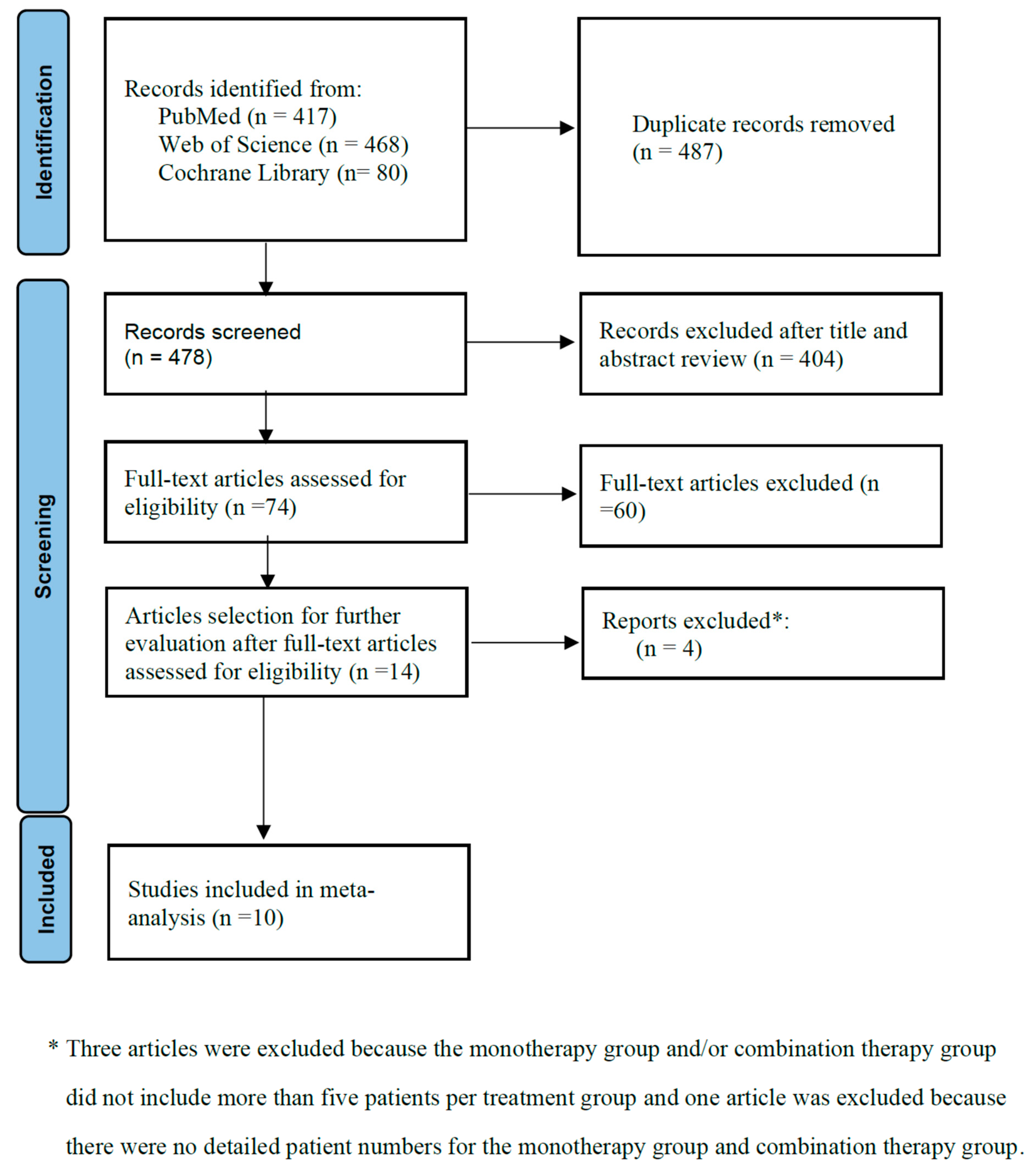
2.1. Data Search
2.2. Inclusion and Exclusion Criteria
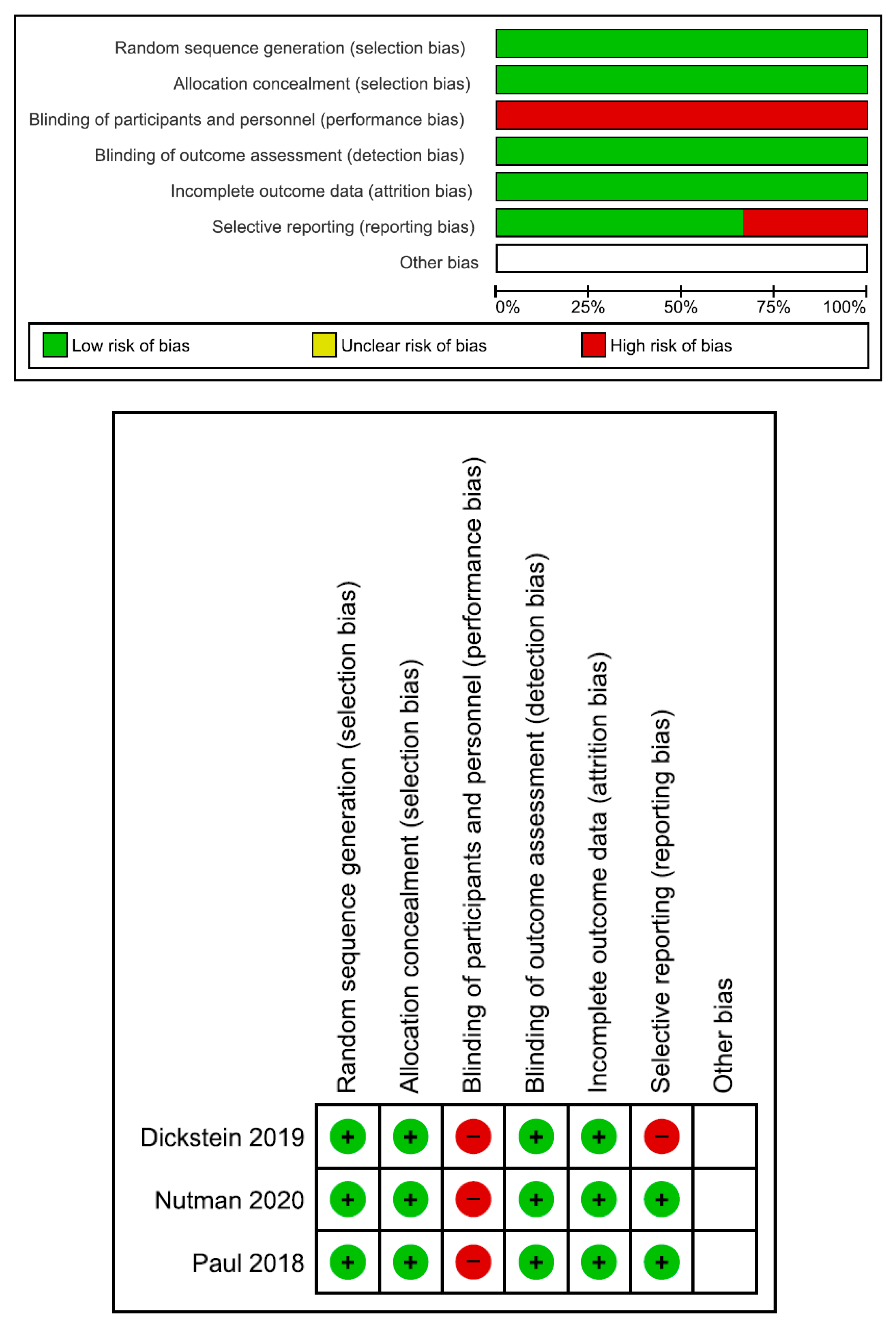
2.3. Quality Assessment
2.4. Statistical Analysis
3. Results
3.1. Characteristics of the Included Trials
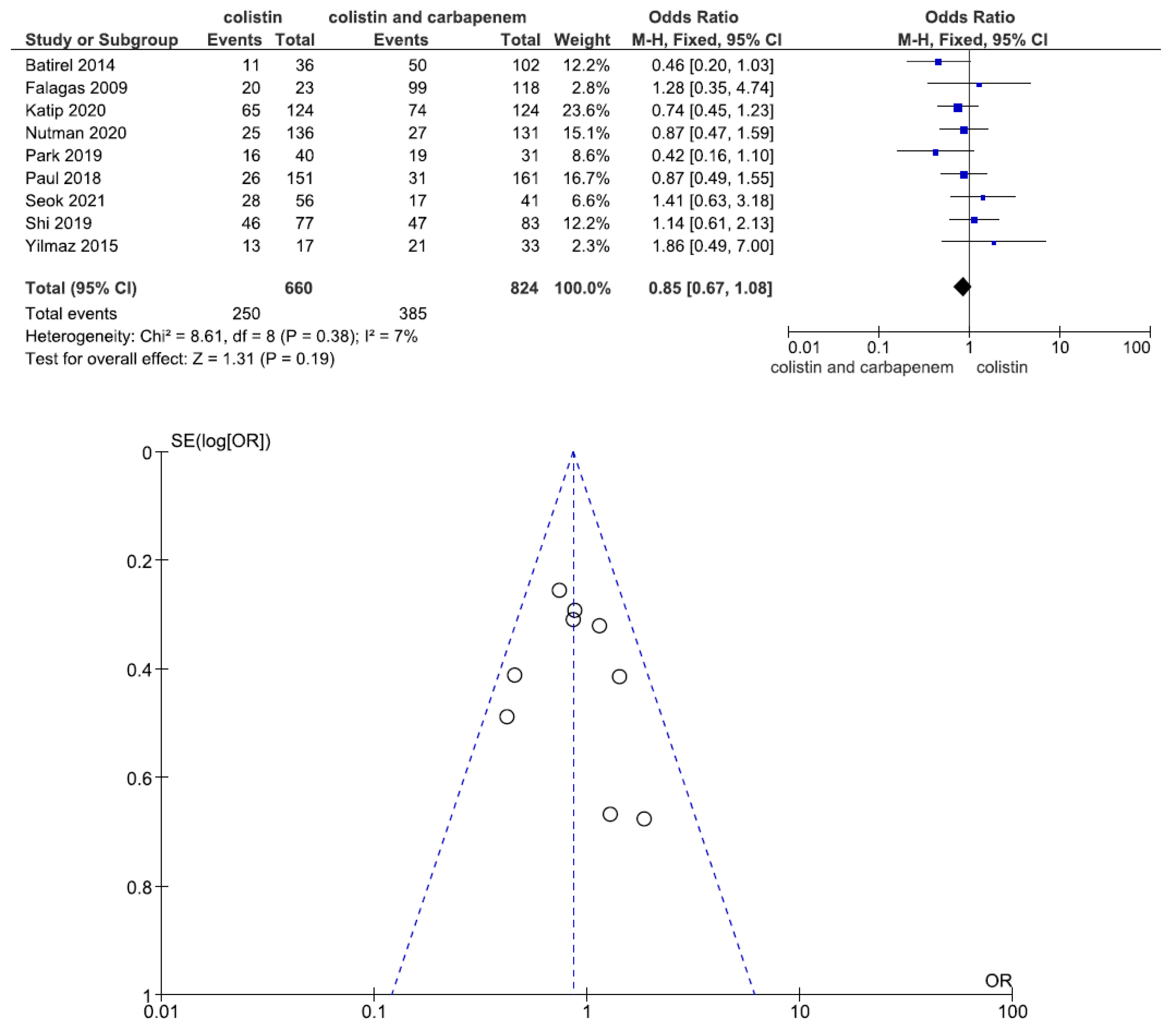
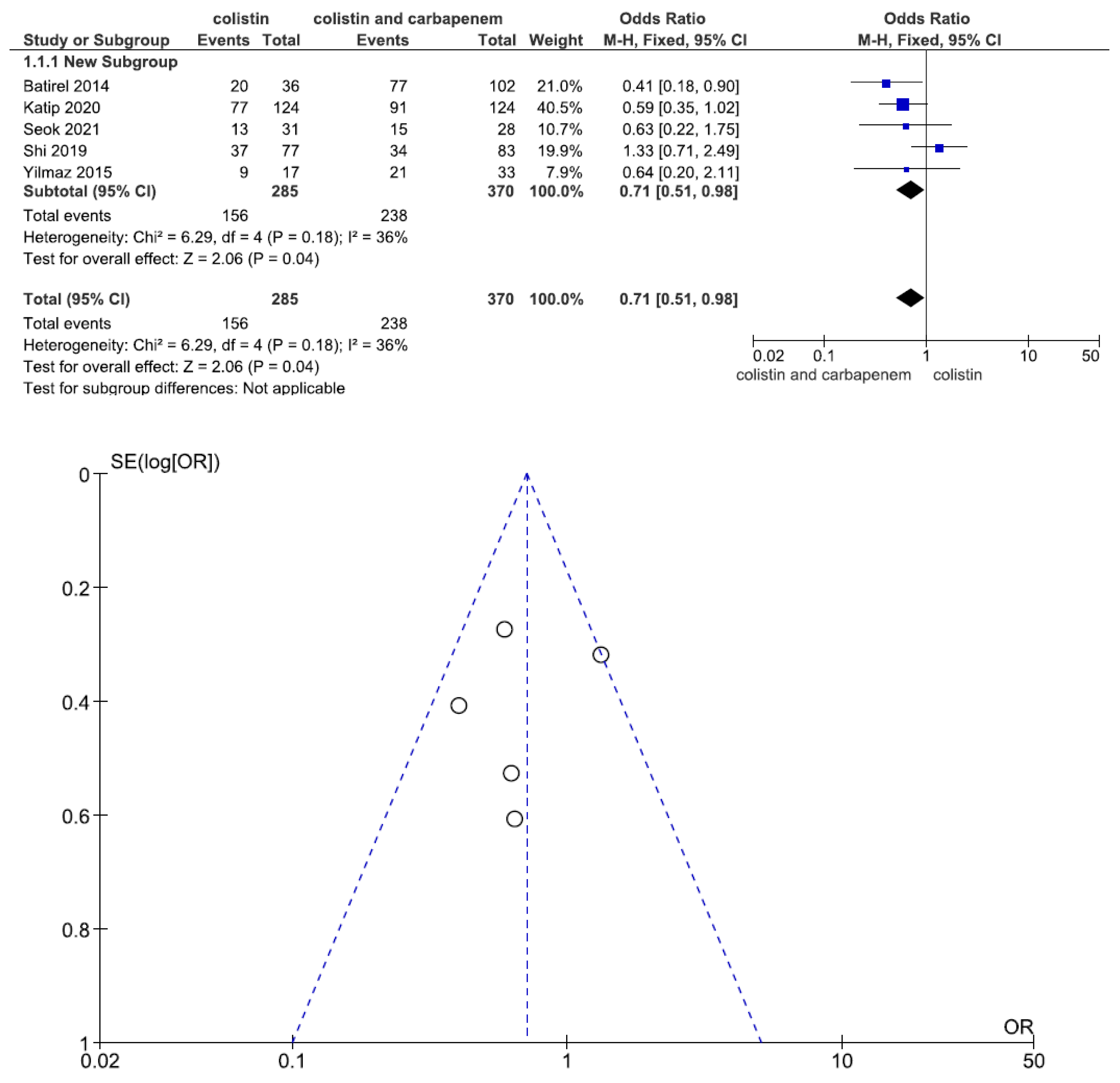
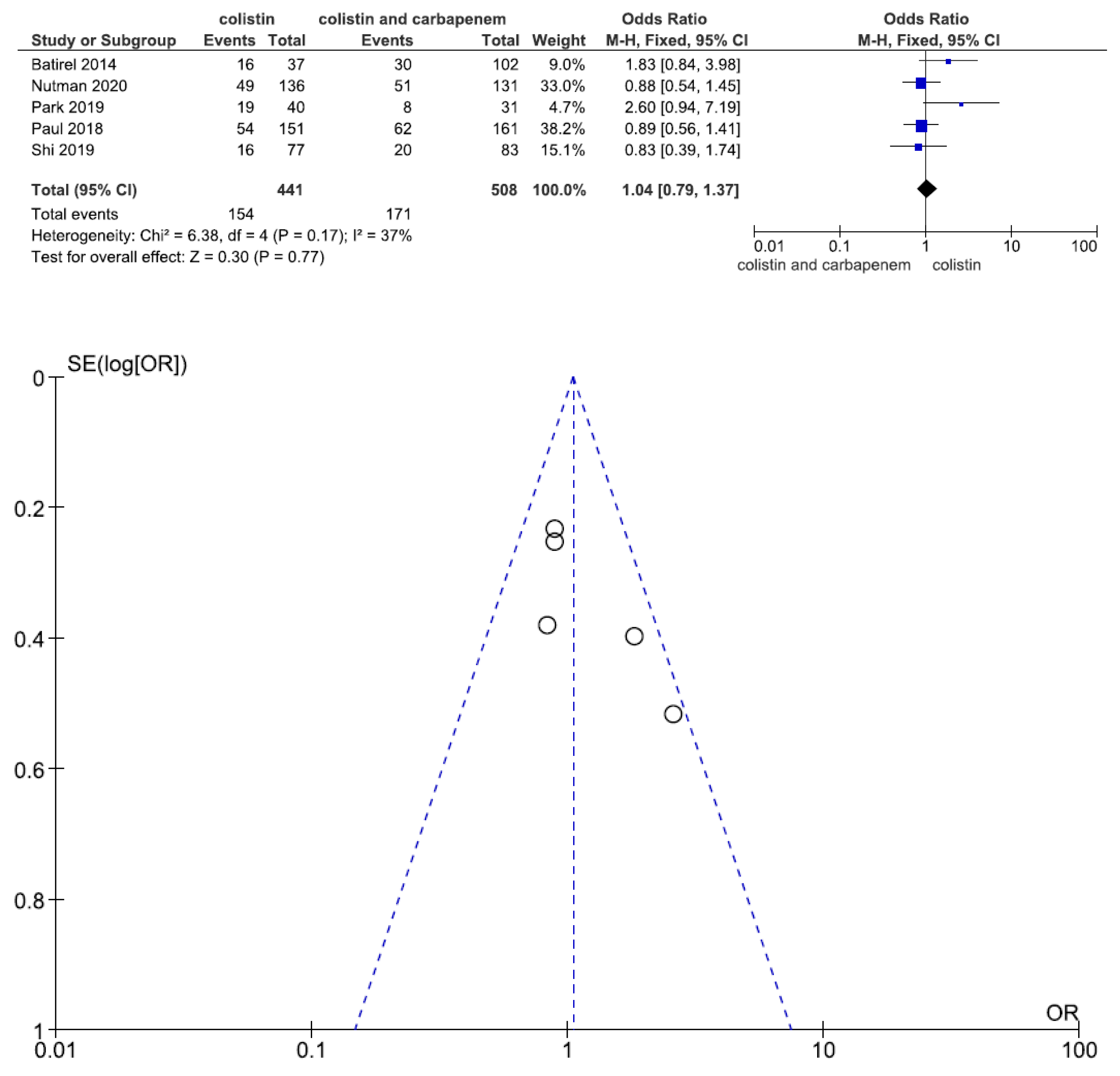
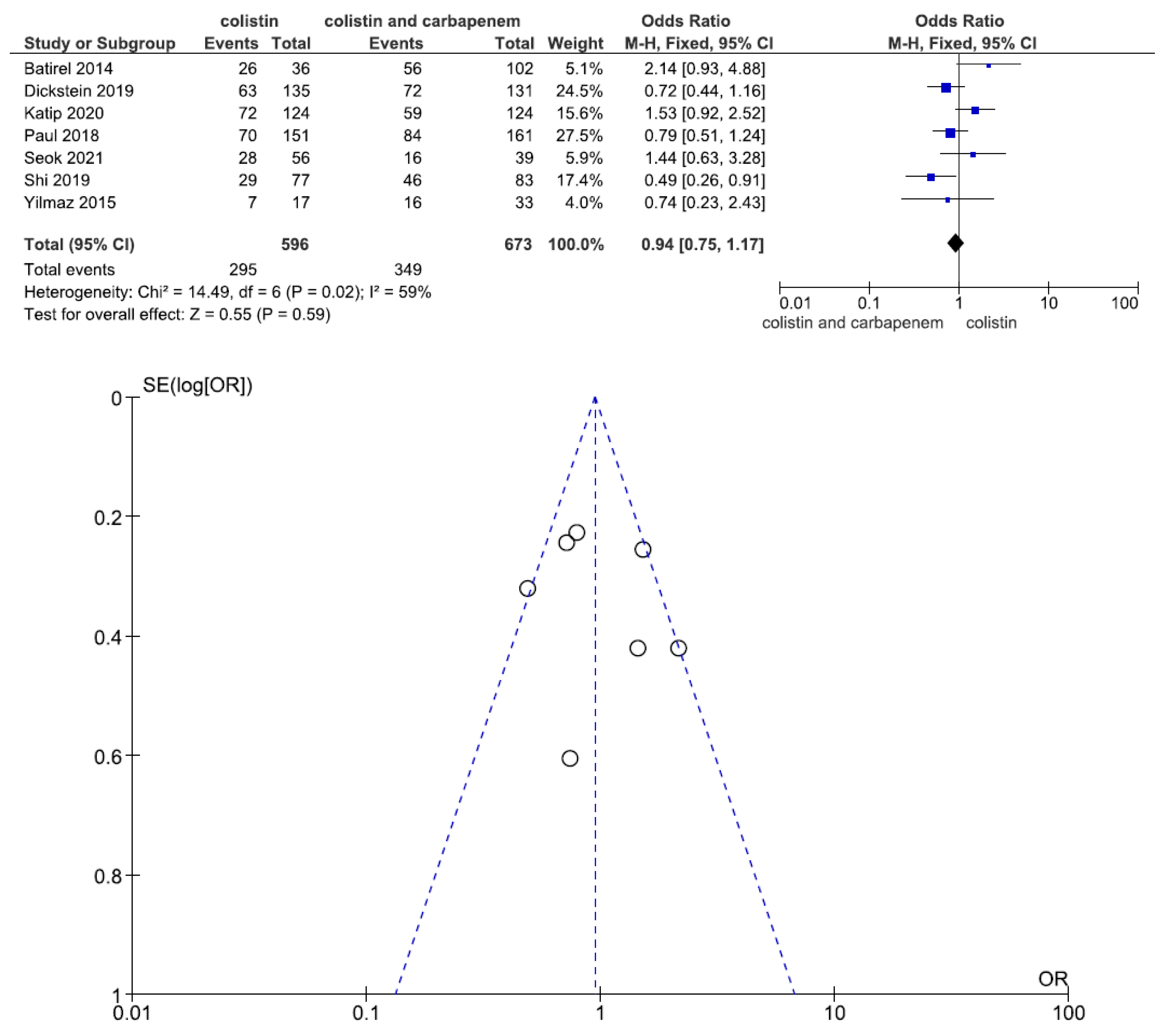
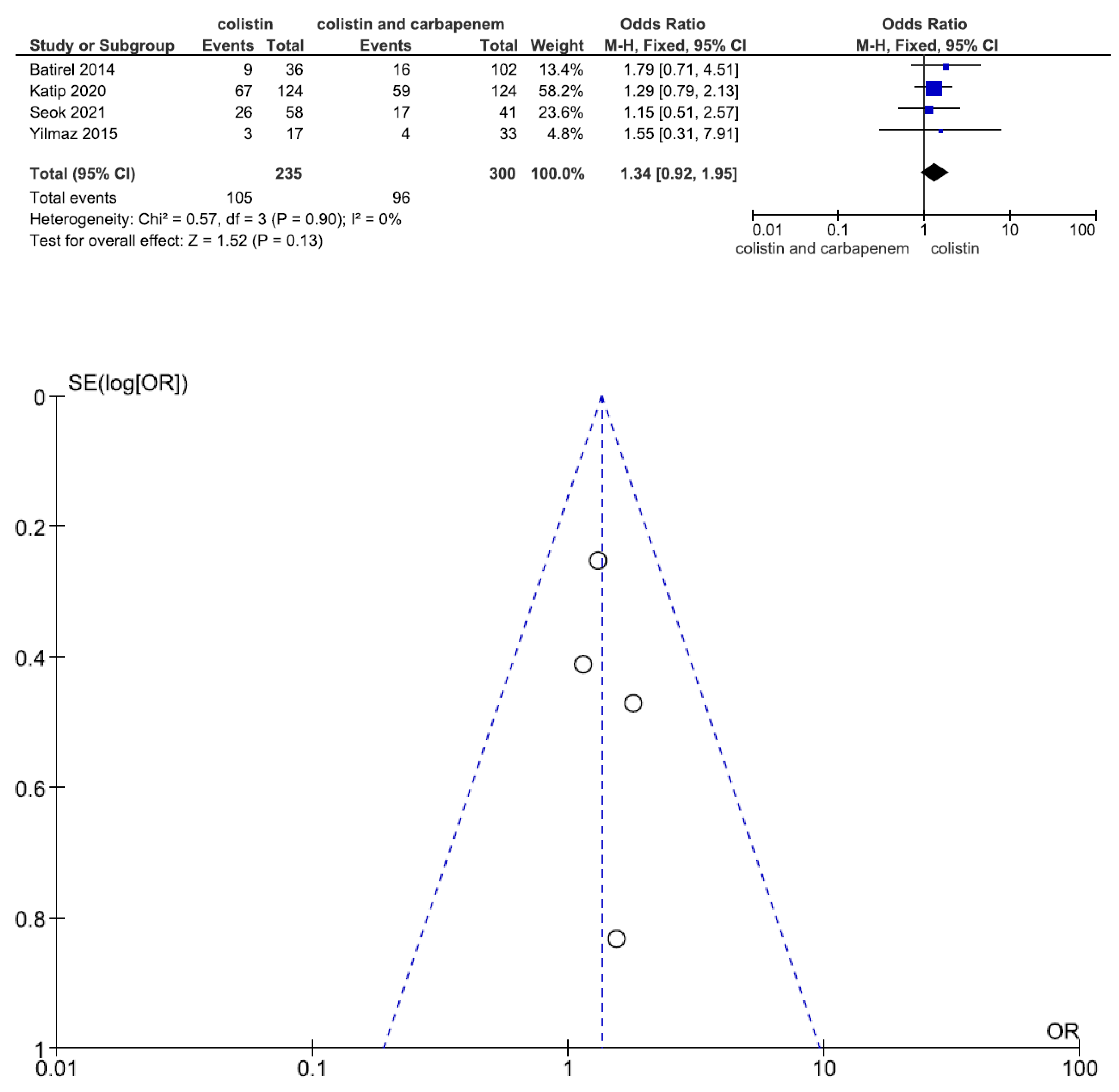
3.2. Efficacy and Safety Outcomes
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pogue, J.M.; Mann, T.; Barber, K.E.; Kaye, K.S. Carbapenem-resistant Acinetobacter baumannii: Epidemiology, surveillance and management. Expert Rev. Anti-Infect. Ther. 2013, 11, 383–393. [Google Scholar] [CrossRef]
- Garnacho-Montero, J.; Amaya-Villar, R. Multiresistant Acinetobacter baumannii infections: Epidemiology and management. Curr. Opin. Infect. Dis. 2010, 23, 332–339. [Google Scholar] [CrossRef]
- Katip, W.; Meechoui, M.; Thawornwittayakom, P.; Chinwong, D.; Oberdorfer, P. Efficacy and Safety of High Loading Dose of Colistin in Multidrug-Resistant Acinetobacter baumannii: A Prospective Cohort Study. J. Intensive Care Med. 2019, 4, 996–1002. [Google Scholar] [CrossRef] [PubMed]
- Katip, W.; Uitrakul, S.; Oberdorfer, P. Clinical outcomes and nephrotoxicity of colistin loading dose for treatment of extensively drug-resistant Acinetobacter baumannii in cancer patients. Infect. Drug Resist. 2017, 10, 293–298. [Google Scholar] [CrossRef] [Green Version]
- Javan, A.O.; Shokouhi, S.; Sahraei, Z.; Salamzadeh, J.; Armaki, S.A. Nephrotoxicity of high and conventional dosing regimens of colistin: A randomized clinical trial. Iran. J. Pharm. Res. 2017, 16, 778–787. [Google Scholar]
- Grégoire, N.; Aranzana-Climent, V.; Magréault, S.; Marchand, S.; Couet, W. Clinical Pharmacokinetics and Pharmacodynamics of Colistin. Clin. Pharmacokinet. 2017, 56, 1441–1460. [Google Scholar] [CrossRef]
- Nowak, J.; Zander, E.; Stefanik, D.; Higgins, P.G.; Roca, I.; Vila, J.; McConnell, M.J.; Cisneros, J.M.; Seifert, H.; MagicBullet Working Group WP4. High incidence of pandrug-resistant Acinetobacter baumannii isolates collected from patients with ventilator-associated pneumonia in Greece, Italy and Spain as part of the MagicBullet clinical trial. J. Antimicrob. Chemother. 2017, 72, 3277–3282. [Google Scholar] [CrossRef]
- Zusman, O.; Avni, T.; Leibovici, L.; Adler, A.; Friberg, L.; Stergiopoulou, T.; Carmeli, Y.; Paul, M. Systematic review and meta-analysis of in vitro synergy of polymyxins and carbapenems. Antimicrob. Agents Chemother. 2013, 57, 5104–5111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leelasupasri, S.; Santimaleeworagun, W. Antimicrobial susceptibility among colistin, sulbactam, and fosfomycin and a synergism study of colistin in combination with sulbactam or fosfomycin against clinical isolates of carbapenem-resistant Acinetobacter baumannii. J. Pathog. 2018, 18, 3893492. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ku, Y.H.; Chen, C.C.; Lee, M.F.; Chuang, Y.C.; Tang, H.J.; Yu, W.L. Comparison of synergism between colistin, fosfomycin and tigecycline against extended-spectrum beta-lactamase-producing Klebsiella pneumoniae isolates or with carbapenem resistance. J. Microbiol. Immunol. Infect. 2017, 50, 931–939. [Google Scholar] [CrossRef]
- Soudeiha, M.A.H.; Dahdouh, E.A.; Azar, E.; Sarkis, D.K.; Daoud, Z. In vitro evaluation of the colistin-carbapenem combination in clinical isolates of A. baumannii using the checkerboard, Etest, and Time-Kill Curve Techniques. Front. Cell. Infect. Microbiol. 2017, 7, 209. [Google Scholar] [CrossRef]
- Petrosillo, N.; Ioannidou, E.; Falagas, M.E. Colistin monotherapy vs. combination therapy: Evidence from microbiological, animal and clinical studies. Clin. Microbiol. Infect. 2008, 14, 816–827. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tamma, P.D.; Cosgrove, S.E.; Maragakis, L.L. Combination therapy for treatment of infections with Gram-negative bacteria. Clin. Microbiol. Rev. 2012, 25, 450–470. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Papst, L.; Beović, B.; Pulcini, C.; Durante-Mangoni, E.; Rodríguez-Baño, J.; Kaye, K.S.; Daikos, G.L.; Raka, L.; Paul, M. Antibiotic treatment of infections caused by carbapenem-resistant Gram-negative bacilli: An international ESCMID cross-sectional survey among infectious diseases specialists practicing in large hospitals. Clin. Microbiol. Infect. 2018, 24, 1070–1076. [Google Scholar] [CrossRef] [Green Version]
- Magiorakos, A.P.; Srinivasan, A.; Carey, R.B.; Carmeli, Y.; Falagas, M.E.; Giske, C.G.; Harbarth, S.; Hindler, J.F.; Kahlmeter, G.; Olsson-Liljequist, B.; et al. Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: An international expert proposal for interim standard definitions for acquired resistance. Clin. Microbiol. Infect. 2012, 18, 268–281. [Google Scholar] [CrossRef] [Green Version]
- Sterne, J.A.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef] [Green Version]
- Atkins, D.; Eccles, M.; Flottorp, S.; Guyatt, G.H.; Henry, D.; Hill, S.; Liberati, A.; O’Connell, D.; Oxman, A.D.; Phillips, B.; et al. Systems for grading the quality of evidence and the strength of recommendations I: Critical appraisal of existing approaches The GRADE Working Group. BMC Health Serv. Res. 2004, 4, 38. [Google Scholar] [CrossRef]
- Guyatt, G.H.; Oxman, A.D.; Vist, G.E.; Kunz, R.; Falck-Ytter, Y.; Alonso-Coello, P.; Schünemann, H.J.; for the GRADE Working Group. GRADE: An emerging consensus on rating quality of evidence and strength of recommendations. BMJ 2008, 336, 924–926. [Google Scholar] [CrossRef] [Green Version]
- Simsek, F.; Gedik, H.; Yildirmak, M.T.; Iris, N.E.; Türkmen, A.; Ersoy, A.; Ersöz, M.; Gücüyener, A. Colistin against colistin-only-susceptible Acinetobacter baumannii-related infections: Monotherapy or combination therapy? Indian J. Med. Microbiol. 2012, 30, 448–452. [Google Scholar] [CrossRef] [PubMed]
- López-Cortés, L.E.; Cisneros, J.M.; Fernández-Cuenca, F.; Bou, G.; Tomás, M.; Garnacho-Montero, J.; Pascual, A.; Martínez-Martínez, L.; Vila, J.; Pachón, J.; et al. Monotherapy versus combination therapy for sepsis due to multidrug-resistant Acinetobacter baumannii: Analysis of a multicentre prospective cohort. J. Antimicrob. Chemother. 2014, 69, 3119–3126. [Google Scholar] [CrossRef] [Green Version]
- Crusio, R.; Rao, S.; Changawala, N.; Paul, V.; Tiu, C.; van Ginkel, J.; Chapnick, E.; Kupfer, Y. Epidemiology and outcome of infections with carbapenem-resistant Gram-negative bacteria treated with polymyxin B-based combination therapy. Scand. J. Infect. Dis. 2014, 46, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Rigatto, M.H.; Vieira, F.J.; Antochevis, L.C.; Behle, T.F.; Lopes, N.T.; Zavascki, A.P. Polymyxin B in Combination with Antimicrobials Lacking In Vitro Activity versus Polymyxin B in Monotherapy in Critically Ill Patients with Acinetobacter baumannii or Pseudomonas aeruginosa Infections. Antimicrob. Agents Chemother. 2015, 59, 6575–6580. [Google Scholar] [CrossRef] [Green Version]
- Falagas, M.E.; Rafailidis, P.I.; Ioannidou, E.; Alexiou, V.G.; Matthaiou, D.K.; Karageorgopoulos, D.E.; Kapaskelis, A.; Nikita, D.; Michalopoulos, A. Colistin therapy for microbiologically documented multidrug-resistant Gram-negative bacterial infections: A retrospective cohort study of 258 patients. Int. J. Antimicrob. Agents 2010, 35, 194–199. [Google Scholar] [CrossRef] [Green Version]
- Batirel, A.; Balkan, I.I.; Karabay, O.; Agalar, C.; Akalin, S.; Alici, O.; Alp, E.; Altay, F.A.; Altin, N.; Arslan, F.; et al. Comparison of colistin-carbapenem, colistin-sulbactam, and colistin plus other antibacterial agents for the treatment of extremely drug-resistant Acinetobacter baumannii bloodstream infections. Eur. J. Clin. Microbiol. Infect. Dis. 2014, 33, 1311–1322. [Google Scholar] [CrossRef]
- Yilmaz, G.R.; Guven, T.; Guner, R.; Kocak Tufan, Z.; Izdes, S.; Tasyaran, M.A.; Acikgoz, Z.C. Colistin alone or combined with sulbactam or carbapenem against A. baumannii in ventilator-associated pneumonia. J. Infect. Dev. Ctries. 2015, 9, 476–485. [Google Scholar] [CrossRef] [Green Version]
- Paul, M.; Daikos, G.L.; Durante-Mangoni, E.; Yahav, D.; Carmeli, Y.; Benattar, Y.D.; Skiada, A.; Andini, R.; Eliakim-Raz, N.; Nutman, A.; et al. Colistin alone versus colistin plus meropenem for treatment of severe infections caused by carbapenem-resistant Gram-negative bacteria: An open-label, randomised controlled trial. Lancet Infect. Dis. 2018, 18, 391–400. [Google Scholar] [CrossRef]
- Park, S.Y.; Si, H.J.; Eom, J.S.; Lee, J.S. Survival of carbapenem-resistant Acinetobacter baumannii bacteremia: Colistin monotherapy versus colistin plus meropenem. J. Int. Med. Res. 2019, 47, 5977–5985. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shi, H.; Lee, J.S.; Park, S.Y.; Ko, Y.; Eom, J.S. Colistin Plus Carbapenem versus Colistin Monotherapy in the Treatment of Carbapenem-Resistant Acinetobacter baumannii Pneumonia. Infect. Drug Resist. 2019, 12, 3925–3934. [Google Scholar] [CrossRef] [Green Version]
- Dickstein, Y.; Lellouche, J.; Ben Dalak Amar, M.; Schwartz, D.; Nutman, A.; Daitch, V.; Yahav, D.; Leibovici, L.; Skiada, A.; Antoniadou, A.; et al. Treatment Outcomes of Colistin- and Carbapenem-resistant Acinetobacter baumannii Infections: An Exploratory Subgroup Analysis of a Randomized Clinical Trial. Clin. Infect. Dis. 2019, 69, 769–776. [Google Scholar] [CrossRef]
- Nutman, A.; Lellouche, J.; Temkin, E.; Daikos, G.; Skiada, A.; Durante-Mangoni, E.; Dishon-Benattar, Y.; Bitterman, R.; Yahav, D.; Daitch, V.; et al. Colistin plus meropenem for carbapenem-resistant Gram-negative infections: In vitro synergism is not associated with better clinical outcomes. Clin. Microbiol. Infect. 2020, 26, 1185–1191. [Google Scholar] [CrossRef]
- Katip, W.; Uitrakul, S.; Oberdorfer, P. A Comparison of Colistin versus Colistin Plus Meropenem for the Treatment of Carbapenem-Resistant Acinetobacter baumannii in Critically Ill Patients: A Propensity Score-Matched Analysis. Antibiotics 2020, 9, 647. [Google Scholar] [CrossRef]
- Seok, H.; Choi, W.S.; Lee, S.; Moon, C.; Park, D.W.; Song, J.Y.; Cheong, H.J.; Kim, J.; Kim, J.Y.; Park, M.N.; et al. What is the optimal antibiotic treatment strategy for carbapenem-resistant Acinetobacter baumannii (CRAB)? A multicentre study in Korea. J. Glob. Antimicrob. Resist. 2021, 24, 429–439. [Google Scholar] [CrossRef]
- Chen, Z.; Chen, Y.; Fang, Y.; Wang, X.; Chen, Y.; Qi, Q.; Huang, F.; Xiao, X. Meta-analysis of colistin for the treatment of Acinetobacter baumannii infection. Sci. Rep. 2015, 5, 17091. [Google Scholar] [CrossRef] [Green Version]
- Zusman, O.; Altunin, S.; Koppel, F.; Dishon Benattar, Y.; Gedik, H.; Paul, M. Polymyxin monotherapy or in combination against carbapenem-resistant bacteria: Systematic review and meta-analysis. J. Antimicrob. Chemother. 2017, 72, 29–39. [Google Scholar] [CrossRef]
- Kengkla, K.; Kongpakwattana, K.; Saokaew, S.; Apisarnthanarak, A.; Chaiyakunapruk, N. Comparative efficacy and safety of treatment options for MDR and XDR Acinetobacter baumannii infections: A systematic review and network meta-analysis. J. Antimicrob. Chemother. 2018, 73, 22–32. [Google Scholar] [CrossRef] [Green Version]
- Vardakas, K.Z.; Mavroudis, A.D.; Georgiou, M.; Falagas, M.E. Intravenous colistin combination antimicrobial treatment vs. monotherapy: A systematic review and meta-analysis. Int. J. Antimicrob. Agents 2018, 51, 535–547. [Google Scholar] [CrossRef] [PubMed]
- Cheng, I.L.; Chen, Y.H.; Lai, C.C.; Tang, H.J. Intravenous Colistin Monotherapy versus Combination Therapy against Carbapenem-Resistant Gram-Negative Bacteria Infections: Meta-Analysis of Randomized Controlled Trials. J. Clin. Med. 2018, 7, 208. [Google Scholar] [CrossRef] [Green Version]
- Wang, J.; Niu, H.; Wang, R.; Cai, Y. Safety and efficacy of colistin alone or in combination in adults with Acinetobacter baumannii infection: A systematic review and meta-analysis. Int. J. Antimicrob. Agents 2019, 53, 383–400. [Google Scholar] [CrossRef] [PubMed]
- Schmid, A.; Wolfensberger, A.; Nemeth, J.; Schreiber, P.W.; Sax, H.; Kuster, S.P. Monotherapy versus combination therapy for multidrug-resistant Gram-negative infections: Systematic Review and Meta-Analysis. Sci. Rep. 2019, 9, 15290. [Google Scholar] [CrossRef]
- Samal, S.; Samir, S.B.; Patra, S.K.; Rath, A.; Dash, A.; Nayak, B.; Mohanty, D. Polymyxin Monotherapy vs. Combination Therapy for the Treatment of Multidrug-resistant Infections: A Systematic Review and Meta-analysis. Indian J. Crit. Care Med. 2021, 25, 199–206. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author/Year | Region | Study Type | Bacteria | Infection Type | No. of Patients (M) | No. of Patients (C) |
|---|---|---|---|---|---|---|
| Falagas, M.E., 2009 [23] | Greece | RETS | MDR AB (65.9%) | Mixed * | 23 | 118 |
| Batirel, A., 2014 [24] | Turkey | RETM | XRD AB | BSI | 36 | 102 |
| Yilmaz, G.R., 2015 [25] | Turkey | RETS | MDR AB XRD AB | VAP | 17 | 33 |
| Paul, M., 2018 [26] | Israel | RCTM | CR AB | BSI, VAP, HAP, UTI | 151 | 161 |
| Park, S.Y., 2019 [27] | Korea | RETS | CR AB | BSI | 40 | 31 |
| Shi, H., 2019 [28] | Korea | RETS | CR AB | Pneumonia | 77 | 83 |
| Dickstein, Y., 2019 [29] | Israel | RCTM | CR AB | BSI, VAP, HAP, UTI | 135 | 131 |
| Nutman, A., 2020 [30] | Israel | RCTM | CR AB | BSI, VAP, HAP, UTI | 136 | 131 |
| Katip, W., 2020 [31] | Thailand | RETS | CR AB | BSI, pneumonia, UTI, surgical site infection | 124 | 124 |
| Seok, H., 2021 [32] | Korea | RETM | CR AB | BSI, UTI, Pneumonia | 58 | 41 |
| Author/Year | CST Loading Dose | CST Maintain Dose | Meropenem Maintain Dose | Duration of Treatment | ||
| Falagas, M.E., 2009 [23] | No data | No data | No data | 17.9 days | ||
| Batirel, A., 2014 [24] | No loading dose | 5 mg/kg/day | 1.0 gm q8h | No data | ||
| Yilmaz, G.R., 2015 [25] | No data | 4.5 MU q12 h | 1.0 gm q8h | M:12.3 days C: 11.7 days | ||
| Paul, M., 2018 [26] | 9.0 MU | 4.5 MU q12 h | 2.0 gm q8h | No data | ||
| Park, S.Y., 2019 [27] | No data | 4.5 MU q12h | 1.0 gm q8h | M: 8.88 days C: 8.22 days | ||
| Shi, H., 2019 [28] | No data | 4.5 MU q12h | 2–3 gm/day | M: 12 days C: 14 days | ||
| Dickstein, Y., 2019 [29] | No data | No data | No data | No data | ||
| Nutman, A., 2020 [30] | 9.0 MU | 4.5 MU q12h | 2.0 gm q8h | No data | ||
| Katip, W., 2020 [31] | 9.0 MU | 4.5 MU q12h | 1.0 gm q8h | No data | ||
| Seok, H., 2021 [32] | No data | No data | No data | No data |
| Author/Year | Confounding | Selection | Interventions Classification | Interventions Deviations | Missing Data | Measurement of Outcomes | Selective Results |
|---|---|---|---|---|---|---|---|
| Flagas, M.E., 2009 [23] | serious risk | serious risk | serious risk | serious risk | low risk | serious risk | serious risk |
| Batirel, A., 2014 [24] | serious risk | serious risk | serious risk | serious risk | low risk | serious risk | low risk |
| Yilmaz, G.R., 2015 [25] | serious risk | serious risk | serious risk | moderate risk | low risk | serious risk | low risk |
| Park, S.Y., 2019 [27] | serious risk | serious risk | serious risk | serious risk | low risk | serious risk | low risk |
| Shi, H., 2019 [28] | serious risk | serious risk | serious risk | low risk | low risk | serious risk | low risk |
| Katip, W., 2020 [31] | serious risk | moderate risk | low risk | low risk | low risk | moderate risk | low risk |
| Seok, H., 2021 [32] | serious risk | moderate risk | low risk | low risk | low risk | moderate risk | low risk |
| Author/Pathogen | Clinical Improvement | Microbiological Response | 14-Day Mortality | * Hospital Mortality | Nephro-Toxicity | Combination Antibiotics |
|---|---|---|---|---|---|---|
| Chen/AB | No | Yes | No data | No | No data | RIF, SUL, CAR, TGC UNA, CPZ, AMG, TZA MIN, TMP |
| Zusman, O.,/GNB1 [34] | No data | No data | No data | No | No data | CAR, TGC, RIF, AMG, SUL, VAN, TZA, FOS |
| Kengkla, K.,/AB [35] | No | Yes % | No data | No | No | RIF, TGC, CAR, SUL, AMG, CPZ, UNA, FOS, MIN, TMP, TZA, |
| Vardakas, K.Z.,/GNB1 [36] | No data | No data | No data | No | No data | RIF, CAR, AMG, TGC, FOS, SUL, CIP |
| Cheng, I.L.,/GNB2 [37] | No data | No | No data | No | No | RIF, FOS, MPM, UNA |
| Wang, J.,/AB [38] | No | Yes | No data | No | No | CAR or/and Sul (subgroup analysis) |
| Schmid, A.,/AB [39] | No | No data | No data | No | No data | RIF, SUL, CAR, TGC UNA, AMG, TZA, RIF, |
| Samal, S.,/GNB1 [40] | No data | No data | No data | No | No data | RIF, VAN, TGC, CAR, SUL, AMG, CPZ, UNA, TAZ, FOS, MIN, TMP. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huang, C.; Chen, I.; Tang, T. Colistin Monotherapy versus Colistin plus Meropenem Combination Therapy for the Treatment of Multidrug-Resistant Acinetobacter baumannii Infection: A Meta-Analysis. J. Clin. Med. 2022, 11, 3239. https://doi.org/10.3390/jcm11113239
Huang C, Chen I, Tang T. Colistin Monotherapy versus Colistin plus Meropenem Combination Therapy for the Treatment of Multidrug-Resistant Acinetobacter baumannii Infection: A Meta-Analysis. Journal of Clinical Medicine. 2022; 11(11):3239. https://doi.org/10.3390/jcm11113239
Chicago/Turabian StyleHuang, Chienhsiu, Ihung Chen, and Tiju Tang. 2022. "Colistin Monotherapy versus Colistin plus Meropenem Combination Therapy for the Treatment of Multidrug-Resistant Acinetobacter baumannii Infection: A Meta-Analysis" Journal of Clinical Medicine 11, no. 11: 3239. https://doi.org/10.3390/jcm11113239