
New Generation Pulse Modulation in Holmium:YAG Lasers: A Systematic Review of the Literature and Meta-Analysis

 , , ,
, , ,
Abstract
:1. Introduction
2. Objectives
3. Evidence Acquisition
3.1. Protocol
3.2. Search Strategy
3.3. Eligibility Criteria
- (P): All in-vitro and in-vivo studies investigating the use of Holmium-laser lithotripsy performance employing any new pulse modulation settings: Moses and Moses 2.0 for Lumenis® 120 W, Vapor Tunnel, Bubble Blast, and Virtual Basket (Quanta System, Samarate, Italy); Advanced Mode (Dornier MedTech, Munich, Germany) and Stabilization Mode (Olympus, Tokyo, Japan);
- (I): Performance of different pulse modulation settings in Ho:YAG laser lithotripsy;
- (C): Comparative and non-comparative studies;
- (O): In-vivo outcomes: stone-free rate, fragmentation. and operative time; in-vitro outcomes: ablation ability, fragmentation efficacy, retropulsion, and laser tip degradation;
- (S) Both prospective and retrospective studies were included.
3.4. Study Selection
3.5. Data Extraction
- -
- For in-vitro studies: first author’s name, publication year, type of laser and fiber size, pulse modulation, energy and frequency settings, fiber-stone distance, stone composition and hardness, experimental conditions, compared variables, and summarized results;
- -
- For in-vivo studies: first author’s name, publication year, study design, intervention, type of laser and fiber size, pulse modulation, energy and frequency settings, population, median stone size, stone Hounsfield units, operative time, fragmentation time, retropulsion, SFR, and complications.
3.6. Assessment of Risk of Bias of Included Studies
3.7. Meta-Analyses for In-Vivo Studies
4. Results
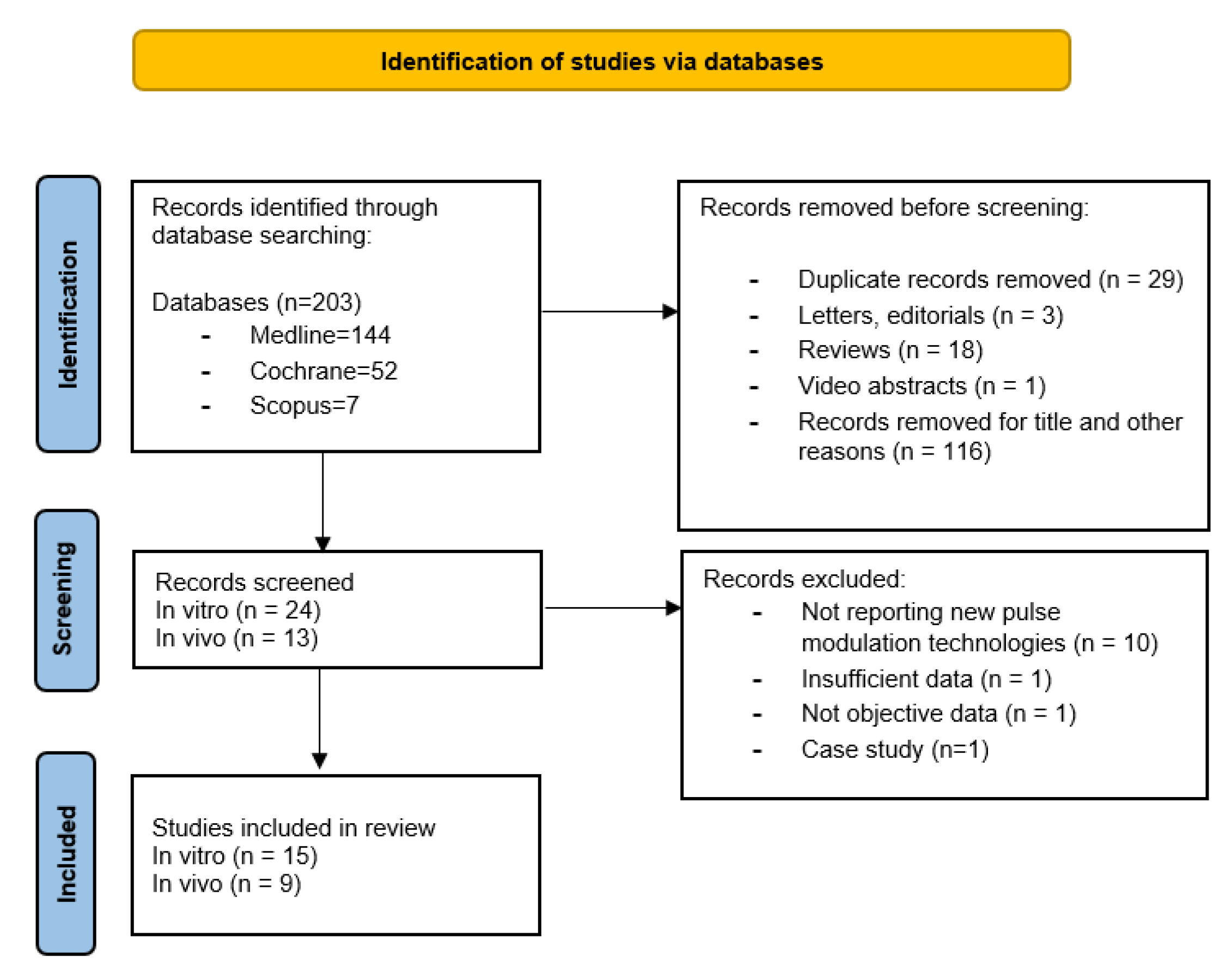
4.1. Literature Search and Inclusion Studies
4.2. Description of the Studies
4.2.1. In-Vitro Studies
4.2.2. In-Vivo Studies
4.3. Risk of Bias of Included Studies
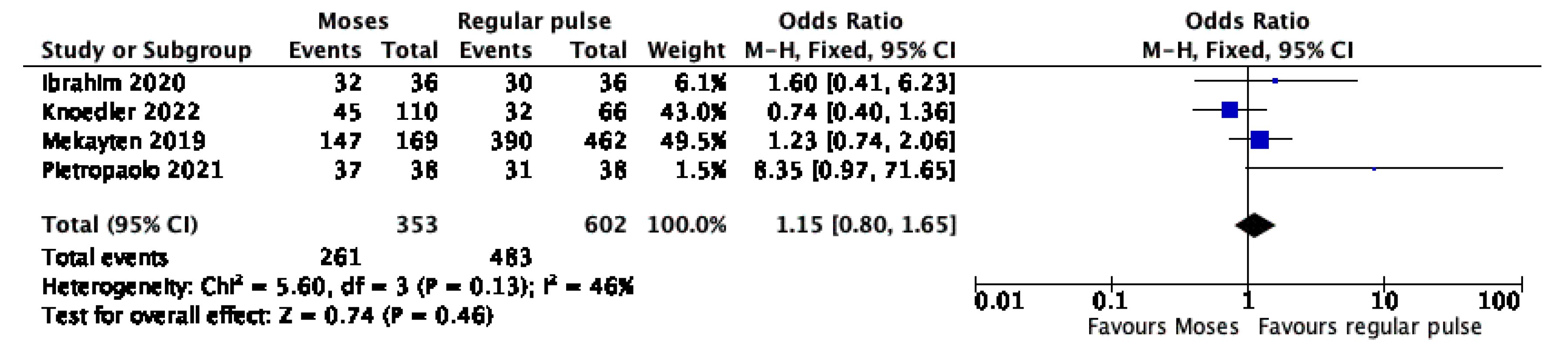
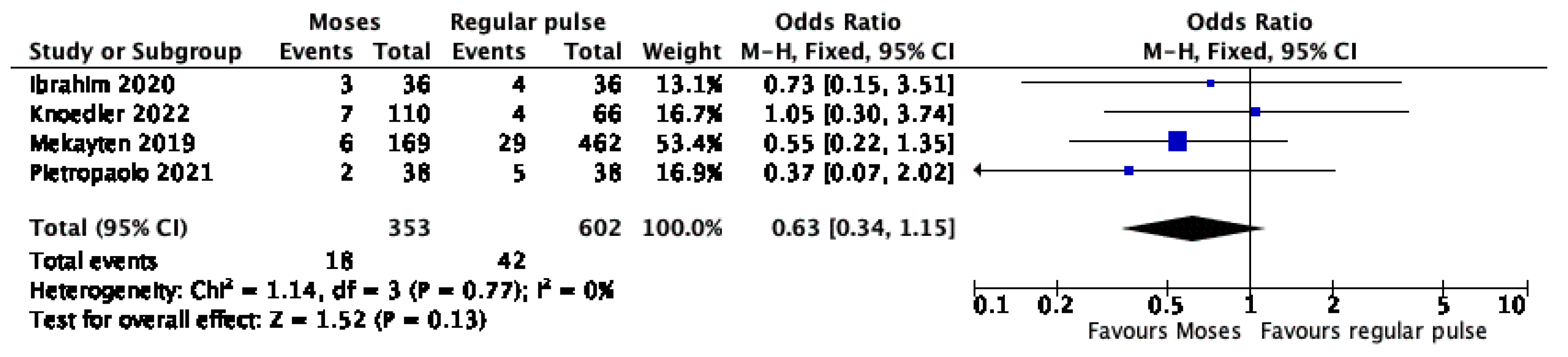
4.4. Meta-Analyses
5. Discussion
Strengths and Limitations
6. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Scales, C.D.; Smith, A.C.; Hanley, J.M.; Saigal, C.S. Prevalence of Kidney Stones in the United States. Eur. Urol. 2012, 62, 160–165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Trinchieri, A. Epidemiology of urolithiasis: An update. Clin. Cases Min. Bone Metab 2008, 5, 101–106. [Google Scholar]
- Gross, A.J.; Herrmann TR, W. History of lasers. World J. Urol. 2007, 25, 217–220. [Google Scholar] [CrossRef]
- Johnson, D.E.; Cromeens, D.M.; Price, R.E. Use of the Holmium:YAG Laser in Urology. Lasers Surg. Med. 1992, 12, 353–363. [Google Scholar] [CrossRef] [PubMed]
- Turney, B.W.; Reynard, J.M.; Noble, J.G.; Keoghane, S.R. Trends in urological stone disease. BJU Int 2012, 109, 1082–1087. [Google Scholar] [CrossRef] [PubMed]
- Khoder, W.Y.; Bader, M.; Sroka, R.; Stief, C.; Waidelich, R. Efficacy and safety of Ho:YAG Laser Lithotripsy for ureteroscopic removal of proximal and distal ureteral calculi. BMC Urol 2014, 14, 62. [Google Scholar] [CrossRef] [Green Version]
- Oberlin, D.T.; Flum, A.S.; Bachrach, L.; Matulewicz, R.S.; Flury, S.C. Contemporary Surgical Trends in the Management of Upper Tract Calculi. J. Urol. 2015, 193, 880–884. [Google Scholar] [CrossRef] [PubMed]
- Teichman, J.M.H.; Vassar, G.J.; Bishoff, J.T.; Bellman, G.C. Holmium: YAG lithotripsy yields smaller fragments than lithoclast, pulsed dye laser or elecrohydraulic lithotripsy. J. Urol. 1998, 159, 17–23. [Google Scholar] [CrossRef] [Green Version]
- Keller, E.X.; de Coninck, V.; Audouin, M.; Doizi, S.; Bazin, D.; Daudon, M.; Traxer, O. Fragments and Dust after Holmium Laser Lithotripsy with or without “Moses Technology”: How are they different? J. Biophotonics 2019, 12, e201800227. [Google Scholar] [CrossRef] [PubMed]
- Kronenberg, P.; Traxer, O. The Truth About Laser Fiber Diameters. Urology 2014, 84, 1301–1307. [Google Scholar] [CrossRef]
- Kronenberg, P.; Traxer, O. Update on lasers in urology 2014: Current assessment on holmium: Yttrium—Aluminum—Garnet (Ho: YAG) laser lithotripter settings and laser fibers. World J. Urol. 2015, 33, 463–469. [Google Scholar] [CrossRef] [PubMed]
- Gilling, P.J.; Cass, C.B.; Cresswell, M.D.; Fraundorfer, M.R. Holmium Laser Resection of the prostate: Preliminary results of a new method for the treatment of benign prostatic hyperplasia. Urology 1996, 47, 48–51. [Google Scholar] [CrossRef]
- Bach, T.; Muschter, R.; Sroka, R.; Gravas, S.; Skolarikos, A.; Herrmann, T.R.; Bayer, T.; Knoll, T.; Abbou, C.-C.; Janetschek, G.; et al. Laser Treatment of Benign Prostatic Obstruction: Basics and Physical Differences. Eur. Urol. 2012, 61, 317–325. [Google Scholar] [CrossRef]
- Chan, K.F.; Vassar, G.J.; Pfefer, T.J.; Teichman, J.M.; Glickman, R.D.; Weintraub, S.T.; Welch, A.J. Holmium:YAG Laser Lithotripsy: A Dominant Photothermal Ablative Mechanism With Chemical Decomposition of Urinary Calculi. Lasers Surg. Med. 1999, 25, 22–37. [Google Scholar] [CrossRef]
- Ventimiglia, E.; Traxer, O. What is Moses effect: An historical perspective. J. Endourol. 2019, 33, 353–357. [Google Scholar] [CrossRef] [PubMed]
- Elhilali, M.M.; Badaan, S.; Ibrehim, A.; Andonian, S. Use of the Moses Technology to Improve Holmium Laser Lithotripsy Outcomes: A Preclinical Study. J. Endourol. 2017, 31, 598–604. [Google Scholar] [CrossRef]
- Terry, R.S.; Ho, D.S.; Scialabba, D.M.; Whelan, P.S.; Qi, R.; Ketterman, B.T.; Preminger, G.M.; Zhong, P.; Lipkin, M.E. Comparison of Different Pulse Modulation Modes for Holmium:Yttrium–Aluminum–Garnet Laser Lithotripsy Ablation in a Benchtop Model. J. Endourol. 2022, 36, 29–37. [Google Scholar] [CrossRef] [PubMed]
- Ibrahim, A.; Elhilali, M.M.; Fahmy, N.; Carrier, S.; Andonian, S. Double-Blind Prospective Randomized Clinical Trial Comparing Regular and Moses Modes of Holmium Laser Lithotripsy. J. Endourol. 2020, 34, 624–628. [Google Scholar] [CrossRef]
- Wang, M.; Shao, Q.; Zhu, X.; Wang, Z.; Zheng, A. Efficiency and Clinical Outcomes of Moses Technology with Flexible Ureteroscopic Laser Lithotripsy for Treatment of Renal Calculus. Urol. Int. 2021, 157, 587–593. [Google Scholar] [CrossRef]
- Slim, K.; Nini, E.; Forestier, D.; Kwiatkowski, F.; Panis, Y.; Chipponi, J. Assessing the Quality of Reports of Randomized Clinical Trials: Is Blinding Necessary? Control. Clin. Trials 1996, 17, 1–12. [Google Scholar]
- Slim, K.; Nini, E.; Forestier, D.; Kwiatkowski, F.; Panis, Y.; Chipponi, J. Methodological index for non-randomized studies (minors): Development and validation of a new instrument. ANZ J. Surg. 2003, 73, 712–716. [Google Scholar] [CrossRef] [PubMed]
- King, J.B.; Katta, N.; Teichman JM, H.; Tunnell, J.W.; Milner, T.E. Mechanisms of Pulse Modulated Holmium: YAG Lithotripsy. J. Endourol. 2021, 35, S29–S36. [Google Scholar] [CrossRef] [PubMed]
- Aldoukhi, A.H.; Roberts, W.W.; Hall, T.L.; Ghani, K.R. Watch your distance: The role of laser fiber working distance on fragmentation when altering pulse width or modulation. J. Endourol. 2019, 33, 120–126. [Google Scholar] [CrossRef] [PubMed]
- Winship, B.; Wollin, D.A.; Carlos, E.C.; Li, M.J.; Peters, M.C.; Simmons, W.N.; Preminger, G.M.; Lipkin, M.E. Dusting Efficiency of the Moses Holmium Laser: An Automated In Vitro Assessment. J. Endourol. 2018, 32, 1131–1135. [Google Scholar] [CrossRef] [PubMed]
- Aldoukhi, A.H.; Black, K.M.; Hall, T.L.; Roberts, W.W.; Ghani, K.R. Frequency threshold for ablation during holmium laser lithotripsy: How high can you go? J. Endourol. 2020, 34, 1075–1081. [Google Scholar] [CrossRef]
- Black, K.M.; Aldoukhi, A.H.; Teichman, J.M.H.; Majdalany, S.E.; Hall, T.L.; Roberts, W.W.; Ghani, K.R. Pulse modulation with Moses technology improves popcorn laser lithotripsy. World J. Urol. 2020, 39, 1699–1705. [Google Scholar] [CrossRef]
- Ibrahim, A.; Badaan, S.; Elhilali, M.M.; Andonian, S. Moses technology in a stone simulator. Can. Urol. Asso. 2018, 12, 127–130. [Google Scholar] [CrossRef] [Green Version]
- Khajeh, N.R.; Black, K.M.; Daignault-Newton, S.; Hall, T.L.; Roberts, W.W.; Ghani, K.R. Impact of Pulse Mode on Dusting Effect for Holmium Laser Lithotripsy: Oxalate Monohydrate Stones. Urology 2022, 159, 53–58. [Google Scholar] [CrossRef]
- Winship, B.; Terry, R.; Boydston, K.; Carlos, E.; Wollin, D. Holmium:Yttrium-Aluminum-Garnet Laser Pulse Type Affects Irrigation Temperatures in a Benchtop Ureteral Model. J. Endourol. 2019, 33, 896–901. [Google Scholar] [CrossRef]
- Ventimiglia, E.; Doizi, S.; Kovalenko, A.; Andreeva, V.; Traxer, O. Effect of temporal pulse shape on urinary stone phantom retropulsion rate and ablation ef fi ciency using holmium: YAG and super-pulse thulium fi bre lasers. BJU Int. 2020, 126, 159–167. [Google Scholar] [CrossRef]
- Jiang, P.; Peta, A.; Brevik, A.; Arada, R.B.; Ayad, M.; Afyouni, A.S.; Limfueco, L.; Nguyen, N.; Palma, A.; Patel, R.M.; et al. Ex-vivo Renal Stone Dusting: Impact of Laser Modality, Ureteral Access Sheath, and Suction on Total Stone Clearance. J. Endourol. 2022, 36, 499–507. [Google Scholar] [CrossRef] [PubMed]
- Ballesta, B.; Peteinaris, A.; Tsaturyan, A.; Natsos, A.; Koukiou, G.; Vagionis, A.; Pagonis, K.; Obaidat, M.; Liourdi, D.; Vrettos, T.; et al. Stone ablation rates using innovative pulse modulation technology: Vapor tunnel, virtual basket, and bubble blast. An in vitro experimental study. Lasers Surg. Med. 2022, 54, 580–587. [Google Scholar] [CrossRef] [PubMed]
- Ho, D.S.; Scialabba, D.; Terry, R.S.; Ma, X.; Chen, M.J.; Sankin, G.N.; Xiang, G.; Qi, R.; Preminger, G.M.; Lipkin, M.E.; et al. The Role of Cavitation in Energy Delivery and Stone Damage During Laser Lithotripsy. J. Endourol. 2021, 35, 860–870. [Google Scholar] [CrossRef] [PubMed]
- Bozzini, G.; Maltagliati, M.; Berti, L.; Besana, U.; Calori, A.; Pastore, A.L.; Gozen, A.; Govorov, A.; Liatsikos, E.; Micali, S.; et al. “VirtualBasket” Ureteroscopic Holmium laser lithotripsy: Intraoperative and early postoperative outcomes. Minerva Urol. Nephrol. 2022, 74, e1314. [Google Scholar] [CrossRef]
- Knoedler, M.A.; Li, M.S.; Best, S.L.; Hedican, S.P.; Penniston, K.L.; Nakada, S.Y. Clinical Impact of the Institution of Moses Technology on Efficiency During Retrograde Ureteroscopy for Stone Disease: Single-Center Experience. J. Endourol. 2022, 36, 65–70. [Google Scholar] [CrossRef] [PubMed]
- Majdalany, S.E.; Levin, B.A.; Ghani, K.R. The Efficiency of Moses Technology Holmium Laser for Treating Renal Stones During Flexible Ureteroscopy: Relationship Betwen Stone Volume, Time and Energy. J. Endourol. 2021, 35, 14–22. [Google Scholar] [CrossRef]
- Pietropaolo, A.; Hughes, T.; Mani, M.; Somani, B. Outcomes of Ureteroscopy and Laser Stone Fragmentation (URSL) for Kidney Stone Disease (KSD): Comparative Cohort Study Using MOSES Technology 60 W Laser System versus Regular Holmium 20 W Laser. J. Clin. Med. 2021, 10, 2742. [Google Scholar] [CrossRef]
- Mekayten, M.; Lorber, A.; Katafigiotis, I.; Sfoungaristos, S.; Leotsakos, I.; Heifetz, E.M.; Yutkin, V.; Gofrit, O.N.; Dovdevani, M. Will Stone Density Stop Being a Key Factor in Endourology? The Impact of Stone Density on Laser Time Using Lumenis Laser p120w and Standard 20 W Laser: A Comparative Study. J. Endourol. 2019, 33, 585–589. [Google Scholar] [CrossRef]
- Reddy, N.K.; Patil, A.P.; Tak, G.R.; Shah, D.; Singh, A.G.; Ganpule, A.P.; Sabnis, R.B.; Desai, M.R. Size Distribution of Fragments by High-power Holmium Laser Lithotripsy in MiniPCNL with Suction. Curr. Urol. Rep. 2021, 22, 64. [Google Scholar] [CrossRef]
- Leotsakos, I.; Katafigiotis, I.; Lorber, A.; Sfoungaristos, S.; Sabler, I.M.; Yutkin, V.; Gofrit, O.N.; Dovdevani, M. Initial experience in combined ultra-mini percutaneous nephrolithotomy with the use of 120-W laser and the anti-retropulsion “Moses effect”: The future of percutaneous nephrolithotomy? Lasers Med. Sci. 2020, 35, 1961–1966. [Google Scholar] [CrossRef]
- Olympus Online Homepage. Available online: https://www.olympusprofed.com/uro/stone-management/19220/ (accessed on 31 March 2022).
- Dornier MedTech Online Home Page. Available online: https://www.dornier.com/europe/products-item/dornier-medilas-h-solvo-35/ (accessed on 31 March 2022).
- Sroka, R.; Pongratz, T.; Scheib, G.; Khoder, W.; Stief, C.G.; Herrmann, T.; Nagele, U.; Bader, M.J. Impact of pulse duration on Ho:YAG laser lithotripsy: Treatment aspects on the single-pulse level. World J. Urol. 2015, 33, 479–485. [Google Scholar] [CrossRef] [PubMed]
- Kang, H.W.; Lee, H.; Teichman, J.M.H.; Oh, J.; Kim, J.; Welch, A.J. Dependence of Calculus Retropulsion on Pulse Duration During Ho: YAG Laser Lithotripsy. Lasers Surg. Med. 2006, 38, 762–772. [Google Scholar] [CrossRef] [PubMed]
- Wezel, F.; Häcker, A.; Gross, A.J.; Michel, M.S.; Bach, T. Effect of Pulse Energy, Frequency and Length on Holmium: Yttrium-Aluminum-Garnet Laser Fragmentation Efficiency in Non-Floating Artificial Urinary Calculi. J. Endourol. 2010, 24, 1135–1140. [Google Scholar] [CrossRef] [PubMed]
- Bell, J.; Pennistion, K.; Nakada, S. In Vitro Comparison of Stone Fragmentation When Using Various Settings with Modern Variable Pulse Holmium Lasers. J. Endourol. 2017, 31, 1067–1072. [Google Scholar] [CrossRef]
- Finley, D.S.; Kang, H.W.; Lee, H.; Joel, M.H.; Oh, J.; Kim, J.; Ashley, J. Effect of Holmium:YAG Laser Pulse Width on Lithotripsy Retropulsion in Vitro. J. Endourol. 2005, 19, 1041–1044. [Google Scholar] [CrossRef]
- Black, K.M.; Aldoukhi, A.H.; Ghani, K.R. A Users Guide to Holmium Laser Lithotripsy Settings in the Modern Era. Front. Surg. 2019, 14, 48. [Google Scholar] [CrossRef] [Green Version]
- Bader, M.J.; Pongratz, T.; Khoder, W.; Stief, C.G.; Herrmann, T.; Nagele, U.; Sroka, R. Impact of pulse duration on Ho:YAG laser lithotripsy: Fragmentation and dusting performance. World J. Urol. 2015, 33, 471–477. [Google Scholar] [CrossRef]
- Corsini, C.; de Angelis, M.; Villa, L.; Somani, B.K.; Pietropaolo, A.; Montorsi, F.; Goumas, I.K.; Traxer, O.; Salonia, A.; Ventimiglia, E. Holmium:yttrium–aluminum–garnet laser with Moses: Does it make a difference ? Curr. Opin. Urol. 2022, 32, 324–329. [Google Scholar] [CrossRef]
- Takhar, M.; Alshalalfa, M.; Gupta, A.; Prasad, S. Sientific program of 36th World Congress of endourology Programm Book. J. Endourol. 2018, 32, P1-A573. [Google Scholar]
- Bozzini, G.; Berti, L.; Besana, U.; Calori, A.; Maltagliati, M.; Roche, J.B.; Gözen, A.S.; Breda, A.; Pini, G.; Pastore, A.L.; et al. “Vapor Tunnel”: Advantages of a New Setting Option for Urgent Holmium Laser Lithotripsy with Cyber-Ho. VideoUrology 2020, 34, 2. [Google Scholar] [CrossRef] [Green Version]
- Khajeh, N.R.; Majdalany, S.E.; Ghani, K.R. Moses 2.0 for High-Power Ureteroscopic Stone Dusting: Clinical Principles for Step-by-Step Video Technique. J. Endourol. 2021, 35, 22–28. [Google Scholar] [CrossRef] [PubMed]
- Aldoukhi, A.H.; Roberts, W.W.; Hall, T.L.; Ghani, K.R. Holmium Laser Lithotripsy in the New Stone Age: Dust or Bust ? Front. Surg. 2017, 4, 57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Traxer, O.; Keller, E.X. Thulium fiber laser: The new player for kidney stone treatment? A comparison with Holmium:YAG laser. World J. Urol. 2019, 38, 1883–1894. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gao, B.; Bobrowski, A.; Lee, J. A scoping review of the clinical efficacy and safety of the novel thulium fiber laser: The rising star of laser lithotripsy. Can. Urol. Assoc. 2020, 15, 56–66. [Google Scholar] [CrossRef]
- Martov, A.G.; Ergakov, D.V.; Guseynov, M.; Andronov, A.S.; Plekhanova, O.A. Clinical Comparison of Super Pulse Thulium Fiber Laser and High- Power Holmium Laser for Ureteral Stone Management. J. Biophotonics 2020, 5, 795–800. [Google Scholar] [CrossRef]
- Ulvik, Ø.; Sørstrand, M.; Juliebø-jones, P.; Gjengstø, P.; Beisland, C. Thulium Fibre Laser versus Holmium:YAG for Ureteroscopic Lithotripsy: Outcomes from a Prospective Randomised Clinical Trial. Eur. Urol. 2022; in press. [Google Scholar] [CrossRef]
- Darwish, A.E.; Gadelmoula, M.M.; Abdelkawi, I.F.; Abdellatif, A.M.; Abdel-Moneim, A.M.; Hammouda, H.M. Ureteral stricture after ureteroscopy for stones: A prospective study for the incidence and risk factors. Urol. Ann. 2019, 11, 276–281. [Google Scholar]
- Winship, B.; Wollin, D.; Carlos, E.; Peters, C.; Li, J.; Terry, R.; Boydston, K.; Preminger, G.M.; Lipkin, M.E. The Rise and Fall of High Temperatures During Ureteroscopic Holmium Laser Lithotripsy. J. Endourol. 2019, 33, 794–799. [Google Scholar] [CrossRef]
- Liang, H.; Liang, L.; Yu, Y.; Huang, B.; Chen, J.; Wang, C.; Zhu, Z.; Liang, X. Thermal effect of holmium laser during ureteroscopic lithotripsy. BMC Urol. 2020, 20, 69. [Google Scholar] [CrossRef]
- Esch, E.; Simmons, W.N.; Sankin, G.; Cocks, H.F.; Preminger, G.M.; Zhong, P. A simple method for fabricating artificial kidney stones of different physical properties. Urol. Res. 2010, 38, 315–319. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author, Year | Laser Used | Pulse Modulation Setting | Laser Setting (Energy J, Frequency Hz) | Fiber Size (μm) | Fiber-stone Distance (mm) | Stone Composition | Hardness (Plaster: Water) | Experimental Conditions | Compared Variables | Summarized Results |
|---|---|---|---|---|---|---|---|---|---|---|
| King 2021 [22] | Lumenis Pulse™ 120 H (Lumenis) | SP vs. MD | −1 J single pulse −0.5 J two pulses separated by at least 2 s | 200 | 1 | BegoStone and human COM, MAP and UA | Hard BegoStone (15:3) | Static laser activation for crater formation in: (1) Dry stones in air (2) Wet stones in air (3) Wet stones in water | -Crater volume -Energy transmission through 1 mm water -Cavitation bubble collapse pressures | Larger craters with MC and MD than with SP. All PMs had high energy transmission through 1 mm of water. No-Moses PMs generated much higher peak pressures. |
| Aldoukhi 2019 [23] | Lumenis Pulse™ 120 H (Lumenis) | SP vs. LP vs. MC vs. MD | 1 J, 10 Hz | 230 | 0 0.5 1 2 | BegoStone | Hard (15:3) for static crater experiment and soft (15:5) for moving laser cut | Static laser activation for crater formation and automatized moving laser-holding arm performing a 2 cm linear cut | -Ablation crater volume -Ablated mass (difference between phantom weight before and after laser action) | More LSD distance, less ablation. No ablation from 3 mm distance. Greatest ablation was achieved with MD at 1 mm. Greater fragmentation at both 0 and 1 mm compared to other PMs. |
| Winship 2018 [24] | Lumenis Pulse™ 120 H (Lumenis) | SP vs. LP vs. MC vs. MD | 0.4, 70 Hz | 365 | 0 1 2 | BegoStone | Hard (15:3) and soft (15:6) | Automatized moving laser-holding arm performed square lithotripsy in a spiral motion | -Ablated mass -Fiber tip degradation | Less LSD, greater ablation regardless of stone composition and pulse modulations. No ablation difference between PMs on hard stones at any distance. In contact with soft stones, MC produced the greatest ablation. At 1 mm from soft stones, MD produced the greatest ablation. No differences in fiber tip degradation. |
| Aldoukhi 2020 [25] | Lumenis Pulse™ 120 H (Lumenis) | LP vs. MD | 0.5 J, 20/40/80 Hz | 230 | 0 | BegoStone | Soft (15:5) | Automatized moving laser-holding arm cutting phantoms at 1 and 3 mm/s | -Crater depth -Crater area -Ablation volume | Ablation MD > LP, specially at 3 mm/s MD has deeper craters than LP |
| Elhilali 2017 [16] | Lumenis Pulse™ 120 H (Lumenis) | Regular Mode * vs. MC and MD | Fragmentation: 0.8 J, 10 Hz and 1.5 J, 10 Hz | 200 365 | 1 for MC 2 for MD | Plaster of Paris (gypsum) stones and AU 3000 | UA 3000 (4:1) | -Static laser horizontal firing for retropulsion analysis -Automatized moving laser-holding arm performing a linear cut -Human performed RIRS for pyelic stone anesthetized pigs | -Stone retropulsion -Ablation volume -Surgeon subjective retropulsion | Less retropulsion and higher ablation volume in MC and MD compared to regular mode. Biggest difference with low energy with high frequencies (stone dusting regimes) together with larger diameter fibers. Less subjective retropulsion with Moses PMs but no differences regarding lasing and procedural times. |
| Dusting: 0.5 J, 50 Hz | ||||||||||
| Black 2020 [26] | Lumenis Pulse™ 120 H (Lumenis) | SP vs. MD | 1 J, 20 Hz 0.5 J, 40 Hz 1 J, 40 Hz 0.5 J, 80 Hz | 230 | 2 | BegoStone | Hard (15:3) | Static laser pop-corn RIRS model in spherical test tube (repositioning the fiber in the center each 15 s) | -Fragment size distribution -Fragment mass lost in fluid | At 1 J × 20 Hz, MD created smaller fragments than SP. MD created the smallest fragment size distribution for both 20 W and 40 W settings, except for the high frequency 80 Hz |
| Ibrahim 2018 [27] | Lumenis Pulse™ 120 H (Lumenis) | SP vs. MC | For fragmentation: 0.8 J, 10 Hz | 200 | 0 | UA 3000 | Soft (4:1) | Human performed lower pole RIRS in an artificial urinary trat model | -Subjective stone retropulsion -Time to compete dusting -Lasing time -Number of pedal uses -% laser on vs. Off -Total energy required | MC: Less procedural time both in fragmentation and pulverization, less subjective retropulsion, reduced number of times the pedal was pressed and higher percentage of time lasing vs. pausing. |
| For dusting 0.4 J, 50 Hz | ||||||||||
| Keller 2018 [9] | Lumenis Pulse™ 120 H (Lumenis) | LP vs. MC | 0.2 J, 40 Hz | 200 | - | Human COM, COD, UA, CA, MAP CA, MAP, BR and CYS | - | Human performed RIRS model inside a 10 mm diameter glass container | -Morphology of dust and residual fragments | MC: more pronounced disruption of morphological characteristics of COD, MAP and CYS. Areas with hexagonal plate-like surfaces appeared on residual fragments and dust from BR |
| Khajeh 2022 [28] | Lumenis Pulse™ 120 H (Lumenis) | SP vs. LP vs. MC vs. MD | 0.5 J, 30 Hz | 230 | - | Canine COM stones | - | Human performed RIRS model in a 20 mm inner diameter spherical 3D printed calyceal model | -Residual fragment size distribution -Fiber tip degradation | No difference between fragments <0.25 mm rate. MC and MD produced a greater mass of fragments <2 mm compared to LP Less fiber tip degradation with MC and MD than with SP. |
| Winship 2019 [29] | Lumenis Pulse™ 120 H (Lumenis) | SP vs. LP vs. MC vs. MD | 0.6 J, 6 Hz 0.8 J, 8 Hz 1 J, 10 Hz 1 J, 20 Hz 0.2 J, 70 Hz | 365 | - | No stone used | - | Static laser activation inside a UAS (URS model) | -Mean temperature change from a baseline adjusted to 37 °C at 1 s and every 5 s -Cumulative equivalent minutes at 43 °C | At 1/10 Hz no thermal injury threshold was reached. LP generated the greatest temperature increase, but not statistically significant. Only MC at 0.2 J/70 Hz exceed the threshold by a small margin although this was not statistically significant |
| Ventimiglia 2020 [30] | sTFL (Urolase SP) | Regular | 0.2–2 J, 8–80 Hz ~16 W combinations | 200 | 0 | BegoStone | Hard (15:3) | Static laser crater formation | -Retropulsion -Crater volume -Pulse shape | Retropulsion: Lowest with sTFL, highest with SP. LP = Moses Stone ablation: sTFL > Ho:YAG. LP = Moses LP had longer pulse and lower peak power than SP SP mode had the shortest pulse width and highest peak power |
| Dual phase | ||||||||||
| Lumenis Pulse™ 120 H (Lumenis) | SP LP MC | 230 | ||||||||
| Jiang 2021 [31] | sTFL (IPG Photonics) | - | 0.2 J, 80 Hz | 230 | - | Human calcium oxalate stones | - | Human performed pyelic RIRS in a porcine kidney with and without UAS and with or without continuous aspiration | -Stone clearance rate (SCR) -Residual fragment size distribution | Highest SCR with sTFL with UAS and aspiration. Lowest SCR with Ho:YAG laser without UAS and no aspiration. sTFL resulted in smaller stone remnants compared to Ho:YAG and Ho:YAG-MOSES. All groups had similar proportion of stone remnants <100 microns. The use of UAS improved SCR regardless of the type of laser used or use of aspiration |
| Ho and Nd:YAG VersaPulse PowerSuite™ (Lumenis) | Regular Mode * | 0.4 J, 40 Hz | 420 | |||||||
| Lumenis Pulse™ 30 H (Lumenis) | Moses MP * | 0.2 J, 80 Hz | 408 | |||||||
| Terry 2021 [17] | Lumenis Pulse™ 120 H (Lumenis) | SP LP MC MD | 0.4 and 1 J, | 272 | 0.5 1 2 | BegoStone | Soft (15:6) | -Static laser crater formation -Automatized laser-holding moving arm generating a linear cut | -Crater depth -Crater area -Crater volume -Cut volume -Pulse duration | Ablation volume was different in all PMs. Lumenis MD had better lithotripsy performance. Lumenis MC was clearly inferior. VT maintains a much greater proportion of its 0.5 mm ablation efficacy once SD increases to 2 mm. |
| Litho 100 High Power (Quanta System) | SP LP VP | |||||||||
| Ballesta 2021 [32] | Cyber Ho 150 W (Quanta System) | VB | 0.5 J, 20 Hz 1 J, 60 Hz 2 J, 30 Hz | 365 | - | BegoStone | Hard (15:3) and soft (15:6) | Static laser crater formation in saline media | -Ablation rate (difference between stone weight before and after lithotripsy /lithotripsy time -Laser activation time to reach 3 kJ | Greatest ablation rate combination: VB, 2 J, 30 Hz. Lowest ablation rate: VT in hard stones. Ablation rates for VT and BB improved with increasing laser power. For hard stones, VB and BB had better performance with 2 J × 30 Hz than 1 J × 60 Hz. In low-power lithotripsy (10 W= 0.5 J × 20 Hz) ablation rate was higher with VB than VT |
| VT | 0.5 J, 20 Hz | |||||||||
| BB | 1.2 J, 10 Hz 1.2 J, 50 Hz 2 J, 30 Hz | |||||||||
| Ho 2021 [33] | H Solvo 35 W (Dornier MedTech) | FM vs. SM vs. AM | 0.8 J, 10 Hz | 365 | 0.5 1 2 | Human COM and BegoStone | Hard (hCOM) and soft (BegoStone 15:6) | Static laser crater formation in air and saline media | -Crater volume -Maximum crater depth -Crater area -Dynamic of crater formation and its relation with the bubble formation | Longer pulse durations (AM) result in greater laser energy delivery to the stone Shortest PM (FM and RM) had higher crater volumes predominantly by wider craters. Crater depths were comparable among PMs |
| Author, Year | Study Design | Intervention | Laser | Pulse Technology | Fiber (μm) | Laser Setting | Population, n | Median Dimension, mm (HU) | Operative Time, min | p Value | Fragmentation Time, min | p value | Retropulsion (Mean Grade LIKERT Scale 0–3) | p Value | Stone Free Rate Definition | Stone Free Rate, % | p Value | Complications | p Value | Jadad Scale | Minors Scale (0–24) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| (Energy J, Frequency Hz) | |||||||||||||||||||||
| Comparative studies | |||||||||||||||||||||
| Ibrahim 2020 [18] | RCT | URS | Lumenis Pulse™ 120 H | Moses | 200 | Dusting: 0.4 J, 80 Hz | 36 | 1.7 (991) | 41.1 | 0.03 | 14.2 | 0.03 | 0.5 | 0.01 | 3 month | 88.4 | p > 0.05 | 8.3% | >0.05 | 5 | |
| Regular mode | Fragmentation: 1.0 J, 10 Hz | 36 | 1.4 (841) | 50.9 | 21.1 | 1.0 | 83.3 | 11.1% | |||||||||||||
| Bozzini 2021 [34] | Prospective Comparative | RIRS | Quanta System Cyber Ho 100 W | VirtualBasket | 272 | 0.6–1.0 J, 15 Hz | 40 | 15.5 | 52.4 | <0.05 | 19.8 | <0.05 | 0 | - | 1 month | 92.5 | 22 | ||||
| Regular mode | 40 | 16.2 | 67.1 | 28.7 | 3 | 77.5 | |||||||||||||||
| URS | VirtualBasket | 365 | 0.6–1.4 J, 10 Hz | 40 | 11 | 35.7 | <0.05 | 16.1 | <0.05 | 0 | 87.5 | ||||||||||
| Regular mode | 40 | 12 | 49 | 20.4 | 3 | 92.5 | |||||||||||||||
| Knoedler 2022 [35] | Retrospective Comparative | URS/RIRS | Lumenis Pulse™ 120 H | Moses | 200 | Dusting: 0.3 J, 80 Hz | 110 | 11.8 | 49.7 | 0.195 | 20.5 | 0.305 | - | - | 1 month | 52.3 | 0.143 | 6.4% | 0.936 | 13 | |
| Regular mode | Fragmentation: 0.8 J, 8 Hz | 66 | 11.6 | 39 | 17.1 | 65.3 | 6.1% | ||||||||||||||
| Majdalany 2021 [36] | Retrospective comparative | URS | Lumenis Pulse™ 120 H | Moses 1.0 | 230 | 0.5 J, 50–80 Hz | 18 | 0.94 | 32 (not compared) | - | 10.4 | - | - | - | 1 month | 71 | - | 17.2% (not compared) | 12 | ||
| Moses 2.0 | 0.2–0.3 J, 50–120 Hz | 11 | 14.3 | 90 | |||||||||||||||||
| Pietropaolo 2021 [37] | Retrospective Comparative | URS | Lumenis Moses P60 W | Moses | 200 | 0.4–0.8 J, 20–35 Hz | 38 | 10.9 | 51.6 | <0.0001 | - | - | - | - | 2/4 month | 97.3 | 0.05 | 16 | |||
| Lumenis Holmium 20 W | Regular mode | 0.4–0.8 J, 12–18 Hz | 38 | 11.8 | 82.1 | - | 81.6 | ||||||||||||||
| Wang 2021 [19] | Retrospective Comparative | URS | Lumenis Pulse™ 120 H | Moses Contact | 200 | 0.3 J, 60 Hz | 114 | 12 (990.5) | 18.4 | 0.001 | 4.99 | <0.001 | - | - | 1 month | 86.8 | 0.743 | Fever 3.5%, ARF 4.4% | 1.000 | 15 | |
| Long Pulse | 102 | 12 (993.7) | 21.2 | 5.94 | 85.3 | Fever 4.4%, ARF 3.9% | |||||||||||||||
| Mekayten 2019 [38] | Retrospective Compartive | URS | Lumenis Pulse™ 120 H | Moses | 200, 365, 550 | 0.46 J, 62 Hz (mean) | 169 | 1021 | 21.1 | 0.001 | 3.25 | <0.001 | - | - | 1–1.5 month | 87.2 | 0.469 | 3.8% | 0.225 | 15 | |
| Dornier Medilas H20 Ho:YAG | Regular mode | 0.69 J, 13 Hz (mean) | 462 | 1084 | 31.8 | 6.5 | - | 84.5 | 6.2% | ||||||||||||
| Observation non-comparative studies | MINORS scale (0–16) | ||||||||||||||||||||
| Reddy 2021 [39] | Prospective | Mini PCNL | Lumenis Pulse™ 120 H | Moses Contact and Moses Distance | 365 | 0.4–0.6 J, 40–60 Hz | 110 | 17.5 (1140) | 38.6 | - | 7.9 | - | - | - | 1 month | 100 | - | 3.8% | - | 12 | |
| Leotsakos 2020 [40] | Retrospective | Ultra-mini PCNL | Lumenis Pulse™ 120 H | Moses Contact | 550 | 0.6–0.8 J, 80 Hz | 12 | 31.5 (1252) | 93.5 | - | 12.6 | - | - | - | 1 month | 91.7 | - | 0% | - | 9 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sánchez-Puy, A.; Bravo-Balado, A.; Diana, P.; Baboudjian, M.; Piana, A.; Girón, I.; Kanashiro, A.K.; Angerri, O.; Contreras, P.; Eisner, B.H.; et al. New Generation Pulse Modulation in Holmium:YAG Lasers: A Systematic Review of the Literature and Meta-Analysis. J. Clin. Med. 2022, 11, 3208. https://doi.org/10.3390/jcm11113208
Sánchez-Puy A, Bravo-Balado A, Diana P, Baboudjian M, Piana A, Girón I, Kanashiro AK, Angerri O, Contreras P, Eisner BH, et al. New Generation Pulse Modulation in Holmium:YAG Lasers: A Systematic Review of the Literature and Meta-Analysis. Journal of Clinical Medicine. 2022; 11(11):3208. https://doi.org/10.3390/jcm11113208
Chicago/Turabian StyleSánchez-Puy, Antoni, Alejandra Bravo-Balado, Pietro Diana, Michael Baboudjian, Alberto Piana, Irene Girón, Andrés K. Kanashiro, Oriol Angerri, Pablo Contreras, Brian H. Eisner, and et al. 2022. "New Generation Pulse Modulation in Holmium:YAG Lasers: A Systematic Review of the Literature and Meta-Analysis" Journal of Clinical Medicine 11, no. 11: 3208. https://doi.org/10.3390/jcm11113208