
Five Years of Direct Oral Anticoagulants Use in Italy: Adverse Drug Reactions from the Italian National Pharmacovigilance Network

 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Methods
3. Results
4. Discussion
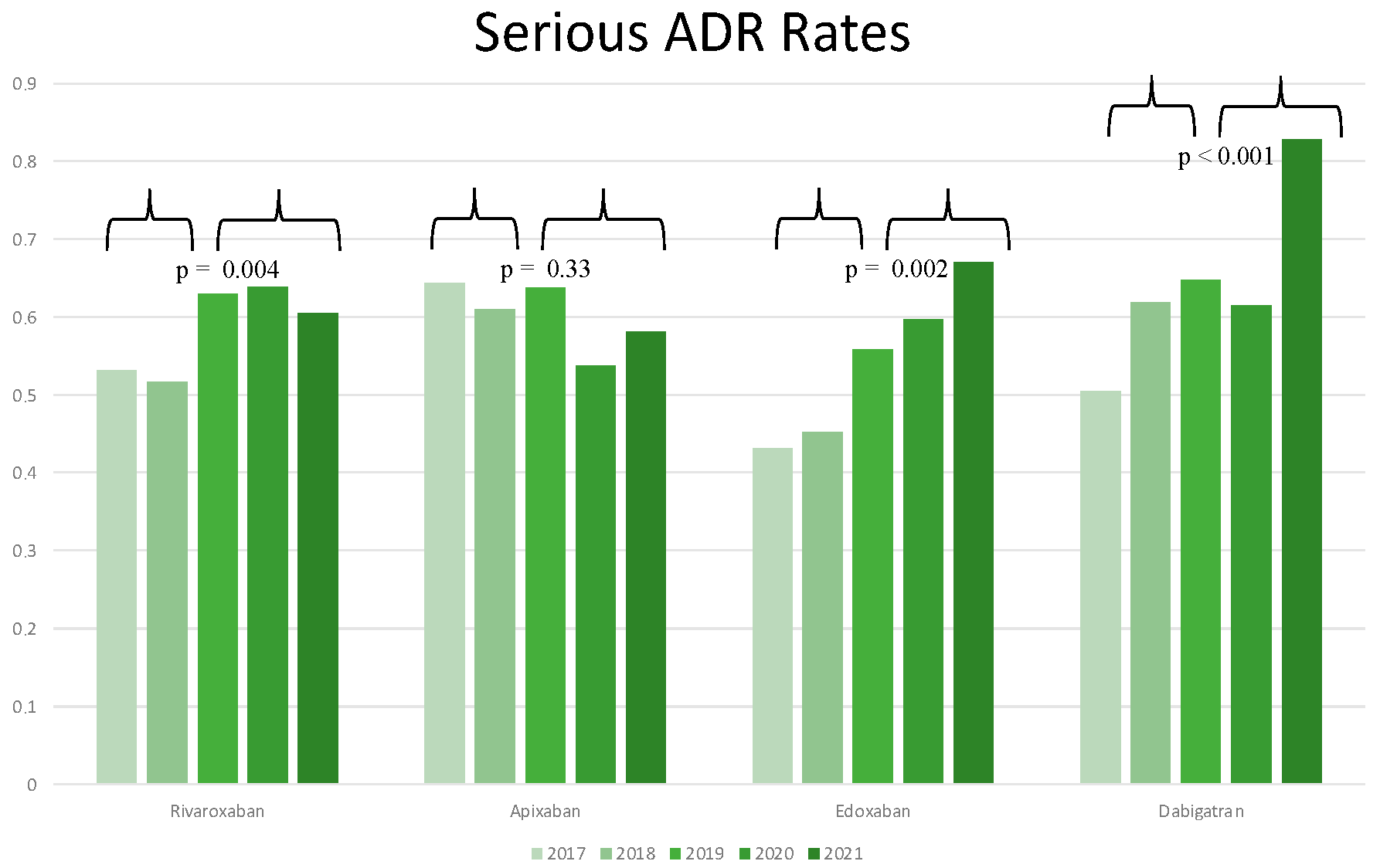
- Rivaroxaban use was associated with consistent and stable low rates of serious ADR, GI ADR, and ICH ADR across the 5-year study period, while fluctuations of ADR rates were recorded for the other molecules (reduction in ICH ADRs for apixaban, increase in serious ADR and ICH ADR for edoxaban and dabigatran).
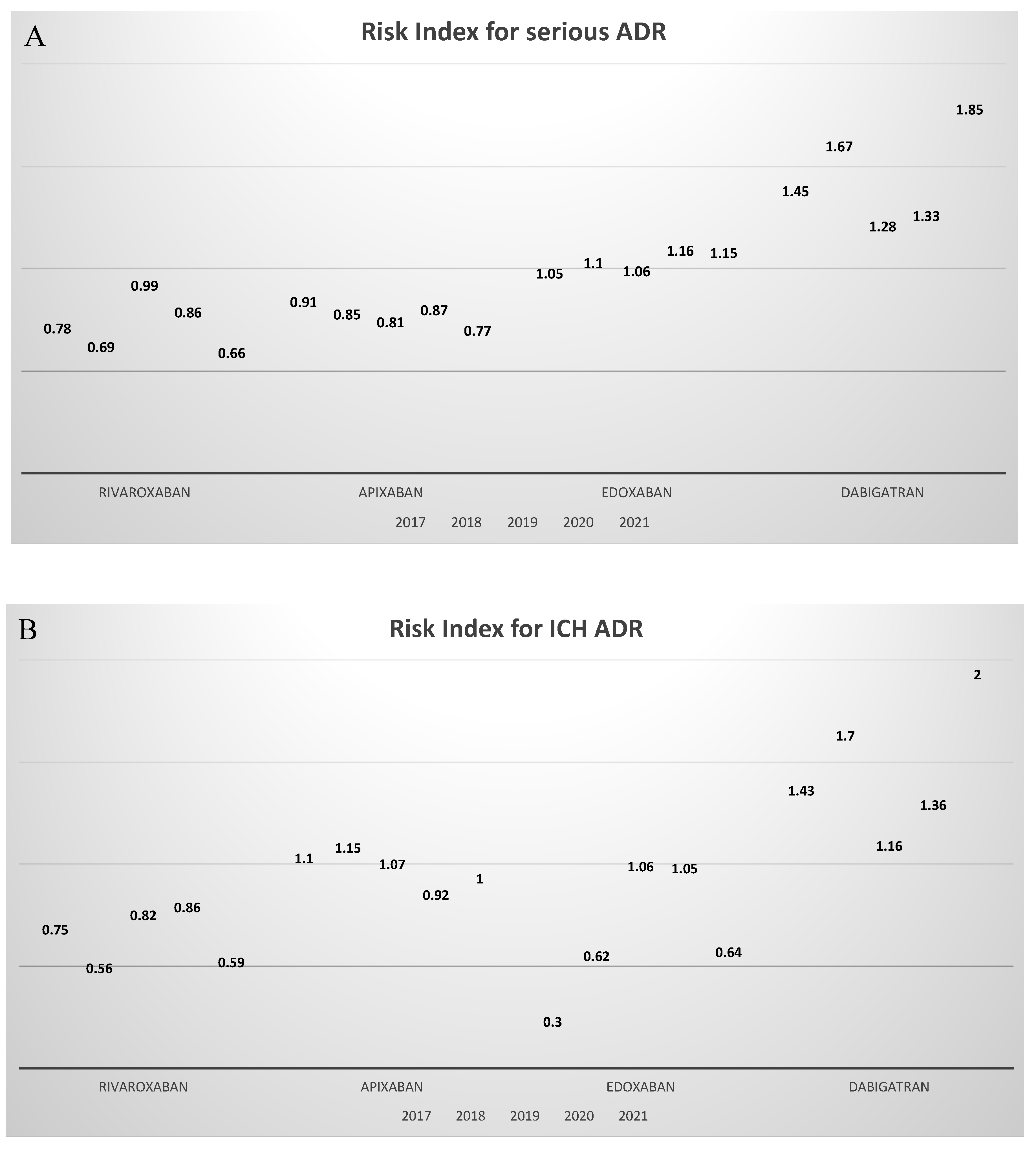
- Rate of serious ADR for rivaroxaban, edoxaban, and dabigatran significantly increased in the period 2019–2021 relative to the period 2017–2018, while no difference was found for apixaban. When normalizing serious ADR rates for usage rates for the same time periods, rivaroxaban showed the lowest risk index for all the study periods but 2019 (RI of 0.99 for rivaroxaban and RI of 0.83 for apixaban).
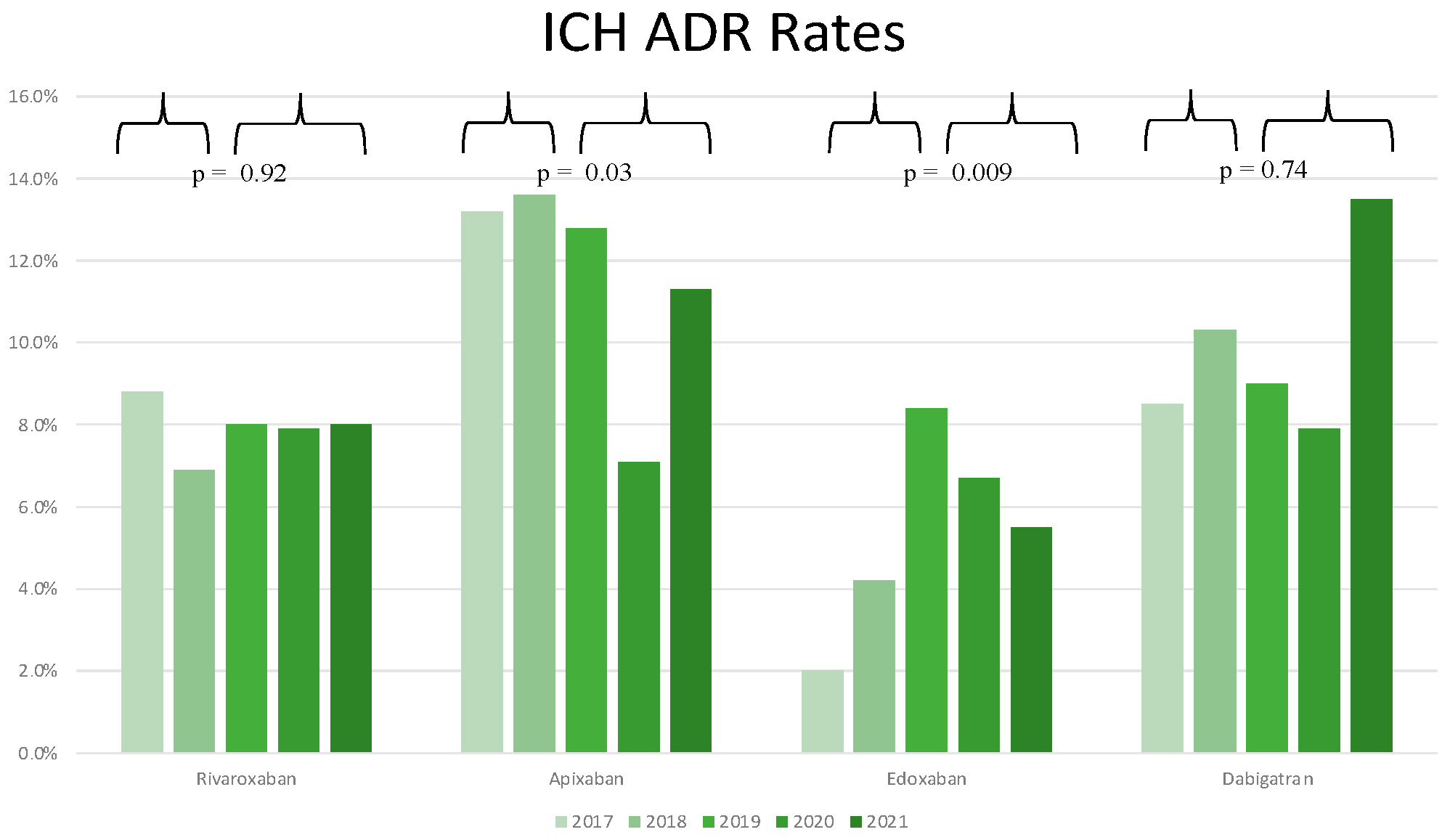
- Rate of ICH ADR for edoxaban significantly increased in the period 2019–2021 relative to the period 2017–2018, and a significant decrease was observed for apixaban, while no difference was found for rivaroxaban and dabigatran. When normalizing ICH ADR rates for usage rates for the same time periods, rivaroxaban constantly showed the lowest risk index for all the study periods, with RI as low as 0.59 in 2021.
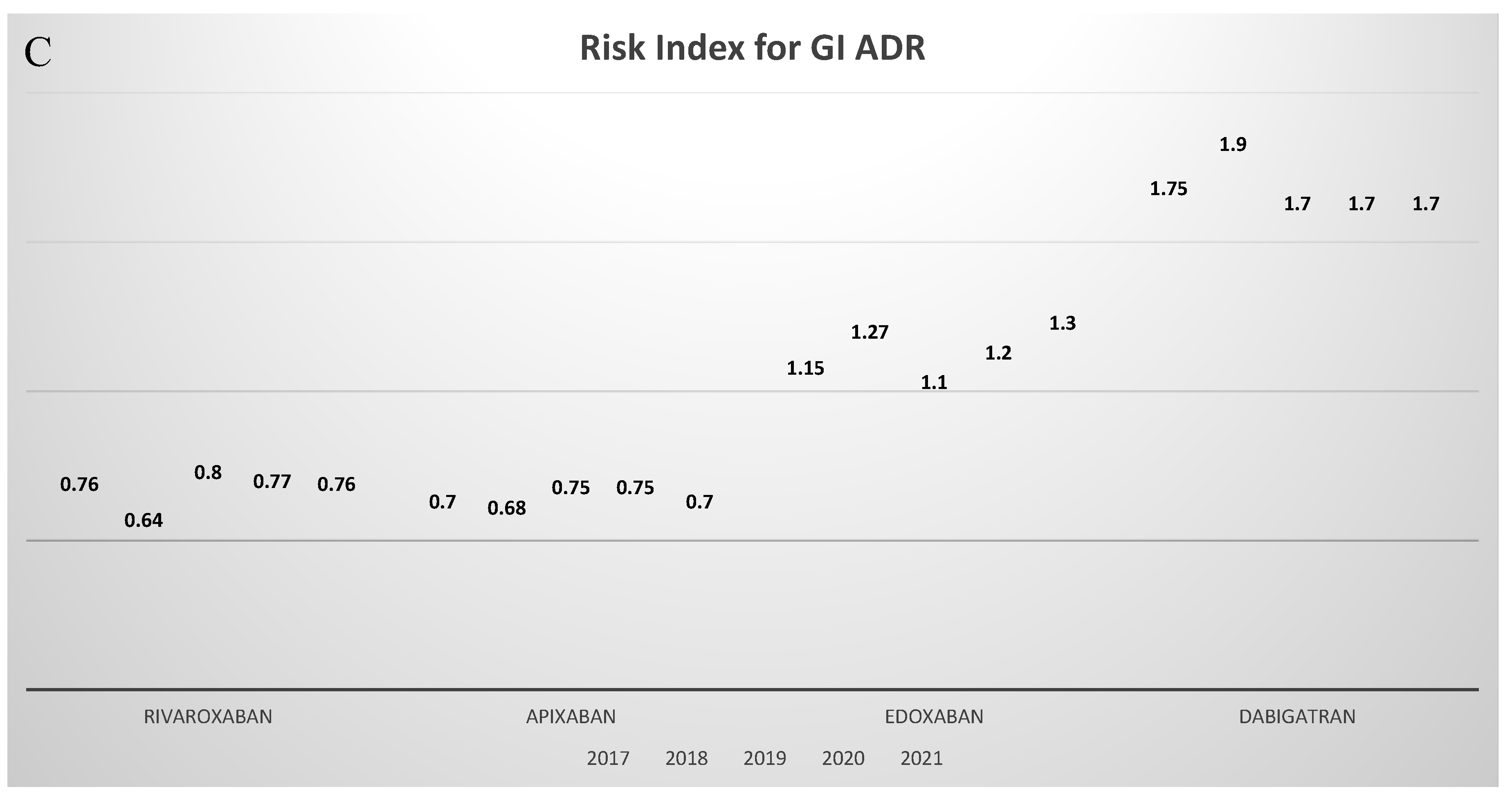
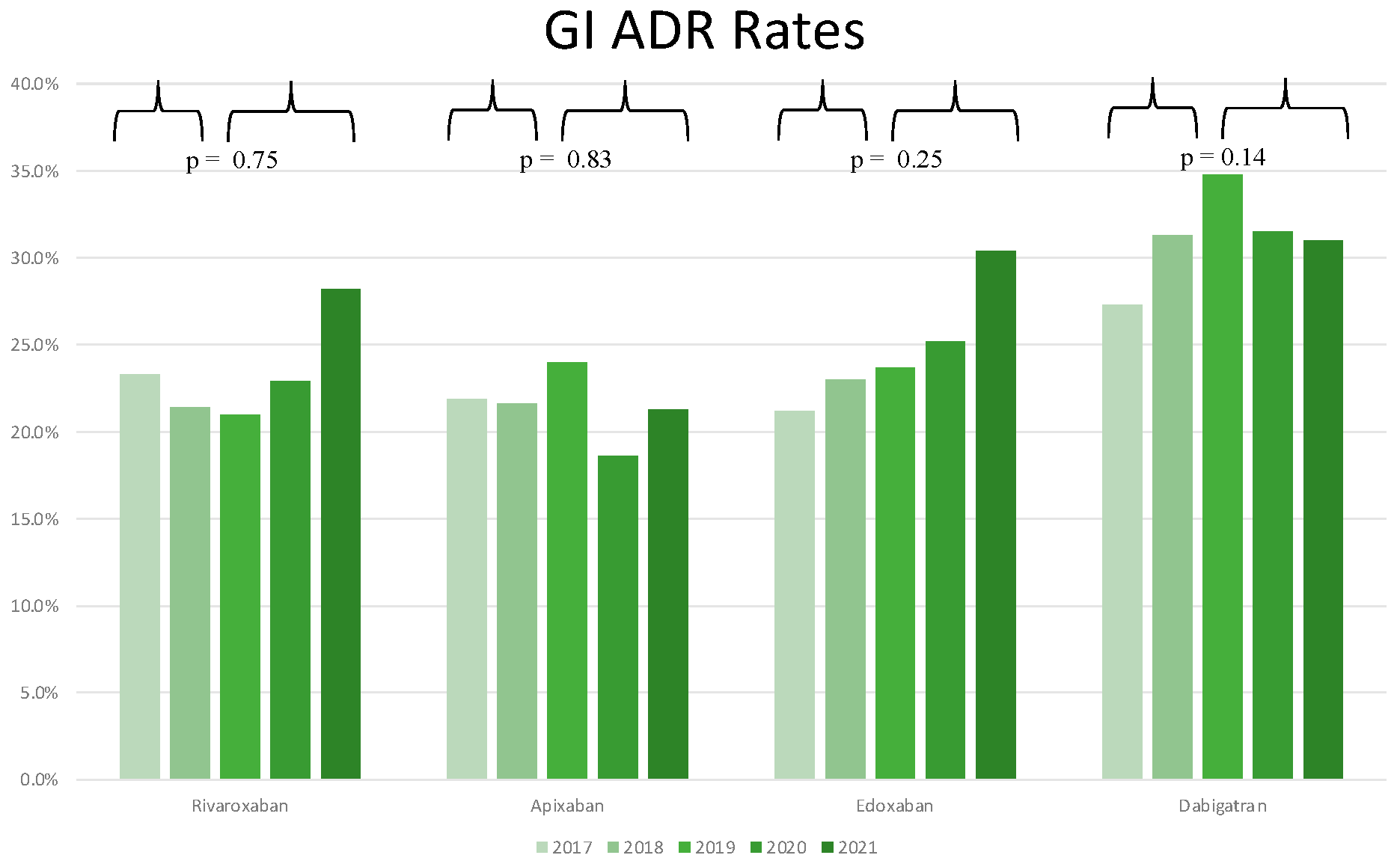
- Rate of GI ADR remained stable during all the study periods for all DOACs, with apixaban and rivaroxaban showing the lowest RIs.
- Apixaban and rivaroxaban use was related to significantly lower rates of serious ADR and GI ADR as compared to dabigatran, while apixaban use resulted in a significantly higher rate of ICH ADR as compared to rivaroxaban.
- In the last five years, nosebleed was the most common ADR reported for rivaroxaban and apixaban, and anemia was the most common for edoxaban, while rectal bleeding was the most frequent ADR reported for dabigatran.
- Although the monthly number of DOACs remained stable during the study period, the total number of ADR reports progressively decreased from 2017 to 2021, pointing out the effect of the under-reporting phenomenon.
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lip, G.Y.; Tse, H.F.; Lane, D.A. Atrial fibrillation. Lancet 2012, 379, 648–661. [Google Scholar] [CrossRef]
- Andersson, T.; Söderberg, S. Incidence of acute pulmonary embolism, related comorbidities and survival; analysis of a Swedish national cohort. BMC Cardiovasc. Disord. 2017, 17, 155. [Google Scholar] [CrossRef] [PubMed]
- Zoni-Berisso, M.; Lercari, F.; Carazza, T.; Domenicucci, S. Epidemiology of atrial fibrillation: European perspective. Clin. Epidemiol. 2014, 6, 213–220. [Google Scholar] [CrossRef] [Green Version]
- Bisson, A.; Clementy, N.; Bodin, A.; Angoulvant, D.; Babuty, D.; Lip, G.Y.; Fauchier, L. Relationship of Preexisting Cardiovascular Comorbidities to Newly Diagnosed Atrial Fibrillation After Ischemic Stroke. Stroke 2017, 48, 2878–2880. [Google Scholar] [CrossRef] [PubMed]
- Bell, D.S.; Goncalves, E. Atrial fibrillation and type 2 diabetes: Prevalence, etiology, pathophysiology and effect of antidiabetic therapies. Diabetes Obes. Metab. 2019, 21, 210–217. [Google Scholar] [CrossRef] [PubMed]
- Alonso, A.; Lopez, F.L.; Matsushita, K.; Loehr, L.R.; Agarwal, S.K.; Chen, L.Y.; Soliman, E.Z.; Astor, B.C.; Coresh, J. Chronic kidney disease is associated with the incidence of atrial fibrillation: The Atherosclerosis Risk in Communities (ARIC) study. Circulation 2011, 123, 2946–2953. [Google Scholar] [CrossRef] [Green Version]
- Magnocavallo, M.; Vetta, G.; Trivigno, S.; Mariani, M.V.; Di Lullo, L.; Bellasi, A.; Della Rocca, D.G.; Severino, P.; Piro, A.; Giunta, G.; et al. The connubium among diabetes, chronic kidney disease and atrial fibrillation. Minerva Cardiol Angiol. 2022, 70, 393–402. [Google Scholar] [CrossRef]
- Konstantinides, S.V.; Meyer, G.; Becattini, C. ESC Scientific Document Group. 2019 ESC Guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European Respiratory Society (ERS). Eur. Heart J. 2020, 41, 543–603. [Google Scholar] [CrossRef] [PubMed]
- Shameem, R.; Ansell, J. Disadvantages of VKA and requirements for novel anticoagulants. Best Pract. Res. Clin. Haematol. 2013, 26, 103–114. [Google Scholar] [CrossRef]
- Connolly, S.J.; Ezekowitz, M.D.; Yusuf, S.; Eikelboom, J.; Oldgren, J.; Parekh, A.; Pogue, J.; Reilly, P.A.; Themeles, E.; RE-LY Steering Committee and Investigators; et al. Dabigatran versus warfarin in patients with atrial fibrillation. N. Engl. J. Med. 2009, 361, 1139–1151. [Google Scholar] [CrossRef] [Green Version]
- Patel, M.R.; Mahaffey, K.W.; Garg, J.; Pan, G.; Singer, D.E.; Hacke, W.; Breithardt, G.; Halperin, J.L.; Hankey, G.J.; ROCKET AF Investigators; et al. Rivaroxaban versus warfarin in nonvalvular atrial fibrillation. N. Engl. J. Med. 2011, 365, 883–891. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Granger, C.B.; Alexander, J.H.; McMurray, J.J.; Lopes, R.D.; Hylek, E.M.; Hanna, M.; Al-Khalidi, H.R.; Ansell, J.; Atar, D.; Avezum, A.; et al. ARISTOTLE Committees and Investigators. Apixaban versus warfarin in patients with atrial fibrillation. N. Engl. J. Med. 2011, 365, 981–992. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giugliano, R.P.; Ruff, C.T.; Braunwald, E.; Murphy, S.A.; Wiviott, S.D.; Halperin, J.L.; Waldo, A.L.; Ezekowitz, M.D.; Weitz, J.I.; Špinar, J.; et al. ENGAGE AFTIMI 48 Investigators. Edoxaban versus warfarin in patients with atrial fibrillation. N. Engl. J. Med. 2013, 369, 2093–2104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruff, C.T.; Giugliano, R.P.; Braunwald, E.; Hoffman, E.B.; Deenadayalu, N.; Ezekowitz, M.D.; Camm, A.J.; Weitz, J.I.; Lewis, B.S.; Parkhomenko, A.; et al. Comparison of the efficacy and safety of new oral anticoagulants with warfarin in patients with atrial fibrillation: A meta–analysis of randomised trials. Lancet 2014, 383, 955–962. [Google Scholar] [CrossRef]
- Schulman, S.; Kearon, C.; Kakkar, A.K.; Mismetti, P.; Schellong, S.; Eriksson, H.; Baanstra, D.; Schnee, J.; Goldhaber, S.Z.; RE-COVER Study Group. Dabigatran versus warfarin in the treatment of acute venous thromboembolism. N. Engl. J. Med. 2009, 10, 2342–2352. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Büller, H.R.; Prins, M.H.; Lensin, A.W.; Decousus, H.; Jacobson, B.F.; Minar, E.; Chlumsky, J.; Verhamme, P.; Wells, P.; EINSTEIN–PE Investigators; et al. Oral rivaroxaban for the treatment of symptomatic pulmonary embolism. N. Engl. J. Med. 2012, 366, 1287–1297. [Google Scholar] [PubMed] [Green Version]
- Agnelli, G.; Buller, H.R.; Cohen, A.; Curto, M.; Gallus, A.S.; Johnson, M.; Masiukiewicz, U.; Pak, R.; Thompson, J.; Raskob, G.E.; et al. Oral apixaban for the treatment of acute venous thromboembolism. N. Engl. J. Med. 2013, 369, 799–808. [Google Scholar] [CrossRef] [Green Version]
- Büller, H.R.; Décousus, H.; Grosso, M.A.; Mercuri, M.; Middeldorp, S.; Prins, M.H.; Raskob, G.E.; Schellong, S.M.; Schwocho, L.; Hokusai-VTE Investigators; et al. Edoxaban versus warfarin for the treatment of symptomatic venous thromboembolism. N. Engl. J. Med. 2013, 369, 1406–1415. [Google Scholar]
- Hindricks, G.; Potpara, T.; Dagres, N.; Arbelo, E.; Bax, J.J.; Blomström-Lundqvist, C.; Boriani, G.; Castella, M.; Dan, G.A.; ESC Scientific Document Group; et al. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS): The Task Force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology (ESC) Developed with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC. Eur. Heart J. 2021, 42, 373–498. [Google Scholar]
- Steffel, J.; Collins, R.; Antz, M.; Cornu, P.; Desteghe, L.; Haeusler, K.G.; Oldgren, J.; Reinecke, H.; Roldan-Schilling, V.; Rowell, N.; et al. 2021 European Heart Rhythm Association Practical Guide on the Use of Non-Vitamin K Antagonist Oral Anticoagulants in Patients with Atrial Fibrillation. Europace 2021, 23, 1612–1676. [Google Scholar] [CrossRef]
- Garrison, L.P.; Neumann, P.J.; Erickson, P.; Marshall, D.; Mullins, C.D. Using real-world data for coverage and payment decisions: The ISPOR Real World Data Task Force report. Value Health 2007, 10, 326–335. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mahajan, R. Real world data: Additional source for making clinical decisions. Int. J. Appl. Basic Med. Res. 2015, 82, 5247. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coppens, M. What can we learn from real world studies on direct oral anticoagulants? Neth. Heart J. 2017, 25, 545–550. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Camm, A.J.; Amarenco, P.; Haas, S.; Hess, S.; Kirchhof, P.; Kuhls, S.; van Eickels, M.; Turpie, A.G. XANTUS: A. real world, prospective, observational study of patients treated with rivaroxaban for stroke prevention in atrial fibrillation. Eur. Heart J. 2016, 11, 1145–1153. [Google Scholar] [CrossRef] [Green Version]
- Kirchhof, P.; Radaideh, G.; Kim, Y.H.; Lanas, F.; Haas, S.; Amarenco, P.; Turpie, A.G.G.; Bach, M.; Lambelet, M.; Hess, S.; et al. Global Prospective Safety Analysis of Rivaroxaban. J. Am. Coll. Cardiol. 2018, 72, 141–153. [Google Scholar] [CrossRef] [PubMed]
- De Caterina, R.; Agnelli, G.; Laeis, P.; Unverdorben, M.; Rauer, H.; Wang, C.C.; Nakamura, M.; Chiu, K.M.; Reimitz, P.E.; Koretsune, Y.; et al. The global Edoxaban Treatment in routine cliNical prActice (ETNA) noninterventional study program: Rationale and design. Clin. Cardiol. 2019, 42, 1147–1154. [Google Scholar]
- De Caterina, R.; Kim, Y.H.; Koretsune, Y.; Wang, C.C.; Yamashita, T.; Chen, C.; Reimitz, P.E.; Unverdorben, M.; Kirchhof, P. Safety and Effectiveness of Edoxaban in Atrial Fibrillation Patients in Routine Clinical Practice: One-Year Follow-Up from the Global Noninterventional ETNA-AF Program. J. Clin. Med. 2021, 10, 573. [Google Scholar] [CrossRef]
- Uguccioni, M.; Terranova, A.; Di Lullo, L. Valutazione delle reazioni avverse agli anticoagulanti orali diretti registrate nella Rete Nazionale di Farmacovigilanza mediante uno specifico indice di rischio. G. Ital. Cardiol. 2018, 19, 3–11. [Google Scholar]
- Lavalle, C.; Di Lullo, L.; Bellasi, A.; Ronco, C.; Radicchia, S.; Barbera, V.; Galardo, G.; Piro, A.; Magnocavallo, M.; Straito, M.; et al. Adverse Drug Reactions during Real-Life Use of Direct Oral Anticoagulants in Italy: An Update Based on Data from the Italian National Pharmacovigilance Network. Cardiorenal. Med. 2020, 10, 266–276. [Google Scholar] [CrossRef]
- Baldo, P.; Francescon, S.; Fornasier, G. Pharmacovigilance workflow in Europe and Italy and pharmacovigilance terminology. Int. J. Clin. Pharmacol. 2018, 40, 748–753. [Google Scholar] [CrossRef] [Green Version]
- Sistema, R.A. Agenzia Italiana del Farmaco. Available online: https://www.aifa.gov.it/web/guest/sistemaram (accessed on 31 January 2022).
- The IQVIA Institute for Human Data Science. Available online: https://www.iqvia.com/insights/theiqviainstitute (accessed on 8 January 2022).
- Mariani, M.V.; Di Lullo, L.; Lavalle, C. Direct oral anticoagulants and chronic kidney disease: It is time to be brave. J. Nephrol. 2021, 34, 1419–1420. [Google Scholar] [CrossRef] [PubMed]
- Magnocavallo, M.; Bellasi, A.; Mariani, M.V.; Fusaro, M.; Ravera, M.; Paoletti, E.; Di Iorio, B.; Barbera, V.; Della Rocca, D.G.; Palumbo, R.; et al. Thromboembolic and Bleeding Risk in Atrial Fibrillation Patients with Chronic Kidney Disease: Role of Anticoagulation Therapy. J. Clin. Med. 2020, 10, 83. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.T.; Hellkamp, A.S.; Becker, R.C.; Berkowitz, S.D.; Breithardt, G.; Fox, K.A.A.; Hacke, W.; Halperin, J.L.; Hankey, G.J.; Mahaffey, K.W.; et al. Efficacy and safety of rivaroxaban versus warfarin in patients with nonval-vular atrial fibrillation and a history of cancer: Observations from ROCKET AF. Eur. Heart J. Qual. Care Clin. Outcomes 2019, 5, 145–152. [Google Scholar] [CrossRef] [PubMed]
- Mariani, M.V.; Magnocavallo, M.; Straito, M.; Piro, A.; Severino, P.; Iannucci, G.; Chimenti, C.; Mancone, M.; Rocca, D.G.D.; Forleo, G.B.; et al. Direct oral anticoagulants versus vitamin K antagonists in patients with atrial fibrillation and cancer a meta-analysis. J. Thromb. Thrombol. 2021, 51, 419–429. [Google Scholar] [CrossRef]
- Raskob, G.E.; van Es, N.; Verhamme, P.; Carrier, M.; Di Nisio, M.; Garcia, D.; Grosso, M.A.; Kakkar, A.K.; Kovacs, M.J.; Mercuri, M.F.; et al. Edoxaban for the treatment of cancer-associated venous thromboembolism. N. Engl. J. Med. 2018, 378, 615–624. [Google Scholar] [CrossRef]
- Agnelli, G.; Becattini, C.; Meyer, G.; Muñoz, A.; Huisman, M.V.; Connors, J.M.; Cohen, A.; Bauersachs, R.; Brenner, B.; Torbicki, A.; et al. Apixaban for the treatment of venous thromboembolism associated with cancer. N. Engl. J. Med. 2020, 382, 1599–1607. [Google Scholar] [CrossRef]
- Lavalle, C.; Mariani, M.; Fedele, F. Factor Xa inhibitors in the prevention of cancer-related venous thromboembolism: Lessons learned by clinical trials. Future Oncol. 2020, 16, 2591–2594. [Google Scholar] [CrossRef]
- Giustozzi, M.; Agnelli, G.; Del Toro-Cervera, J.; Klok, F.A.; Rosovsky, R.P.; Martin, A.C.; Herold, J.; Tzoran, I.; Szmit, S.; Bertoletti, L.; et al. Direct Oral Anticoagulants for the Treatment of Acute Venous Thromboembolism Associated with Cancer: A Systematic Review and Meta-Analysis. Thromb. Haemost. 2020, 120, 1128–1136. [Google Scholar] [CrossRef]
- Zou, R.; Tao, J.; Shi, W.; Yang, M.; Li, H.; Lin, X.; Yang, S.; Hua, P. Meta-analysis of safety and efficacy for direct oral anticoagulation treatment of non-valvular atrial fibrillation in relation to renal function. Thromb. Res. 2017, 160, 41–50. [Google Scholar] [CrossRef]
- Di Lullo, L.; Tripepi, G.; Ronco, C.; D’Arrigo, G.; Barbera, V.; Russo, D.; Di Iorio, B.R.; Uguccioni, M.; Paoletti, E.; Ravera, M.; et al. Cardiac valve calcification and use of anticoagulants: Preliminary observation of a potentially modifiable risk factor. Int. J. Cardiol. 2019, 278, 243–249. [Google Scholar]
- Di Lullo, L.; Lavalle, C.; Magnocavallo, M.; Mariani, M.V.; Della Rocca, D.G.; Severino, P.; Di Iorio, B.R.; Russo, D.; Summaria, F.; Forleo, G.B.; et al. New evidence of direct oral anticoagulation therapy on cardiac valve calcifications, renal preservation and inflammatory modulation. Int. J. Cardiol. 2021, 345, 90–97. [Google Scholar] [CrossRef] [PubMed]
- Stanifer, J.W.; Pokorney, S.D.; Chertow, G.M.; Hohnloser, S.H.; Wojdyla, D.M.; Garonzik, S.; Byon, W.; Hijazi, Z.; Lopes, R.D.; Alexander, J.H.; et al. Apixaban versus warfarin in patients with atrial fibrillation and advanced chronic kidney disease. Circulation 2020, 141, 1384–1392. [Google Scholar] [CrossRef] [PubMed]
- Siontis, K.C.; Zhang, X.; Eckard, A.; Bhave, N.; Schaubel, D.E.; He, K.; Tilea, A.; Stack, A.G.; Balkrishnan, R.; Yao, X.; et al. Outcomes Associated with Apixaban Use in Patients with End-Stage Kidney Disease and Atrial Fibrillation in the United States. Circulation 2018, 138, 1519–1529. [Google Scholar] [CrossRef] [PubMed]
- De Vriese, A.S.; Caluwé, R.; Van Der Meersch, H.; De Boeck, K.; De Bacquer, D. Safety and Efficacy of Vitamin K Antagonists versus Rivaroxaban in Hemodialysis Patients with Atrial Fibrillation: A Multicenter Randomized Controlled Trial. J. Am. Soc. Nephrol. 2021, 32, 1474–1483. [Google Scholar] [CrossRef]
- Chimenti, C.; Lavalle, C.; Magnocavallo, M.; Alfarano, M.; Mariani, M.V.; Bernardini, F.; Della Rocca, D.G.; Galardo, G.; Severino, P.; Di Lullo, L.; et al. A proposed strategy for anticoagulation therapy in noncompaction cardiomyopathy. ESC Heart Fail. 2022, 9, 241–250. [Google Scholar] [CrossRef]
- Camm, A.J.; Amarenco, P.; Haas, S.; Hess, S.; Kirchhof, P.; Lambelet, M.; Bach, M.; Turpie, A.G.G. Real-world vs. randomized trial outcomes in similar populations of rivaroxaban-treated patients with non-valvular atrial fibrillation in ROCKET AF and XANTUS. Europace 2019, 21, 421–427. [Google Scholar] [CrossRef]
- Tamayo, S.; Frank Peacock, W.; Patel, M.; Sicignano, N.; Hopf, K.P.; Fields, L.E.; Sarich, T.; Wu, S.; Yannicelli, D.; Yuan, Z. Characterizing major bleeding in patients with nonvalvular atrial fibrillation: A pharmacovigilance study of 27 467 patients taking rivaroxaban. Clin. Cardiol. 2015, 38, 63–68. [Google Scholar] [CrossRef]
- Monaco, L.; Biagi, C.; Conti, V.; Melis, M.; Donati, M.; Venegoni, M.; Vaccheri, A.; Motola, D. Safety profile of the direct oral anticoagulants: An analysis of the WHO database of adverse drug reactions. Br. J. Clin. Pharmacol. 2017, 83, 1532–1543. [Google Scholar] [CrossRef] [Green Version]
- Gaio, M.; Ferrajolo, C.; Zinzi, A.; Riccardi, C.; Di Filippo, P.; Carangelo, L.; Pieretti, G.; Rossi, F.; Nicoletti, G.F.; Capuano, A. Association of Direct Oral Anticoagulants (DOACs) and Warfarin with Haemorrhagic Risk by Applying Correspondence Analysis to Data from the Italian Pharmacovigilance Database–A Case Study. Front. Pharmacol. 2021, 12, 790740. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Serious ADR/Total ADR | 2017 | 2018 | 2019 | 2020 | 2021 | Serious/Total ADR 2017–2021 |
|---|---|---|---|---|---|---|
| Rivaroxaban | 53.2% (301/566) | 51.7% (304/588) | 63% (582/924) | 63.9% (354/554) | 61% (221/362) | 58.8% (1762/2994) |
| Apixaban | 64.4% (308/478) | 61% (336/551) | 63.8% (444/696) | 53.7% (344/641) | 58.6% (259/442) | 60% (1691/2808) |
| Edoxaban | 43.2% (63/146) | 45.2% (149/330) | 55.9% (257/460) | 69.7% (230/385) | 67.1% (194/289) | 55.5% (893/1610) |
| Dabigatran | 50.5% (360/713) | 61.9% (445/735) | 64.8% (441/680) | 61.5% (297/483) | 82.8% (356/430) | 62.4% (1899/3041) |
| Total serious ADR all DOACs/year | 1032 | 1234 | 1724 | 1225 | 1030 | 6245 |
| ICH ADR/Total ADR | ||||||
| Rivaroxaban | 8.8% (50/566) | 6.9% (41/588) | 8% (74/924) | 7.9% (44/554) | 8% (29/362) | 7.9% (238/2994) |
| Apixaban | 13.2% (63/478) | 13.6% (75/551) | 12.8% (89/696) | 7.1% (46/641) | 11.3% (50/442) | 11.5% (323/2808) |
| Edoxaban | 2% (3/146) | 4.2% (14/330) | 8.4% (39/460) | 6.7% (26/385) | 5.5% (16/289) | 6.1% (98/1610) |
| Dabigatran | 8.5% (61/713) | 10.3% (76/735) | 9% (61/680) | 7.9% (38/483) | 13.5% (58/430) | 9.7% (294/3041) |
| Total ICH ADR all DOACs/year | 177 | 206 | 263 | 154 | 153 | 953 |
| GI ADR/Total ADR | ||||||
| Rivaroxaban | 23.3% (132/566) | 21.4% (126/588) | 21% (194/924) | 22.9% (127/554) | 28.2% (102/362) | 22.7% (681/2994) |
| Apixaban | 21.9% (105/478) | 21.6% (119/551) | 24% (167/696) | 18.6% (119/641) | 21.3% (94/442) | 21.5% (604/2808) |
| Edoxaban | 21.2% (31/146) | 23% (76/330) | 23.7% (109/460) | 25.2% (97/385) | 30.4% (88/289) | 24.9% (401/1610) |
| Dabigatran | 27.3% (195/713) | 31.3% (230/735) | 34.8% (237/680) | 31.5% (152/483) | 31% (133/430) | 31.1% (947/3041) |
| Total GI ADR all DOACs/year | 463 | 551 | 707 | 495 | 417 | 2633 |
| Study Year | 2017 | 2018 | 2019 | 2020 | 2021 |
|---|---|---|---|---|---|
| Rivaroxaban | 37.5 | 35.6 | 34.4 | 33.4 | 32.4 |
| Apixaban | 32.6 | 31.7 | 31.6 | 32.2 | 32.7 |
| Edoxaban | 5.8 | 10.9 | 14 | 16.2 | 16.3 |
| Dabigatran | 24.1 | 21.8 | 20 | 18.2 | 18.7 |
| Most Frequent ADR | Rivaroxaban | Apixaban | Edoxaban | Dabigatran |
|---|---|---|---|---|
| 2017 | Nosebleed (9.7%) | Anemia (6%) | Nosebleed (8.3%) | Abdominal pain (10.5%) |
| 2018 | Nosebleed (11%) | Nosebleed (8%) | Nosebleed (9.5%) | Maelena (5.9%) |
| 2019 | Nosebleed (8.6%) | Nosebleed (8.6%) | Anemia (9.8%) | Rectal bleeding (9.8%) |
| 2020 | Nosebleed (12.8%) | Anemia (7.9%) | Anemia (9.7%) | Anemia (7.4%) |
| 2021 | Nosebleed (13.9%) | Nosebleed (10.4%) | Anemia (12.2%) | Rectal Bleeding (7.8%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lavalle, C.; Mariani, M.V.; Piro, A.; Magnocavallo, M.; Vetta, G.; Trivigno, S.; Forleo, G.B.; Della Rocca, D.G.; Uguccioni, M.; Russo, V.; et al. Five Years of Direct Oral Anticoagulants Use in Italy: Adverse Drug Reactions from the Italian National Pharmacovigilance Network. J. Clin. Med. 2022, 11, 3207. https://doi.org/10.3390/jcm11113207
Lavalle C, Mariani MV, Piro A, Magnocavallo M, Vetta G, Trivigno S, Forleo GB, Della Rocca DG, Uguccioni M, Russo V, et al. Five Years of Direct Oral Anticoagulants Use in Italy: Adverse Drug Reactions from the Italian National Pharmacovigilance Network. Journal of Clinical Medicine. 2022; 11(11):3207. https://doi.org/10.3390/jcm11113207
Chicago/Turabian StyleLavalle, Carlo, Marco Valerio Mariani, Agostino Piro, Michele Magnocavallo, Giampaolo Vetta, Sara Trivigno, Giovanni Battista Forleo, Domenico Giovanni Della Rocca, Massimo Uguccioni, Vincenzo Russo, and et al. 2022. "Five Years of Direct Oral Anticoagulants Use in Italy: Adverse Drug Reactions from the Italian National Pharmacovigilance Network" Journal of Clinical Medicine 11, no. 11: 3207. https://doi.org/10.3390/jcm11113207