
Patient-Derived Training Simulator for Image-Guided Adaptive Brachytherapy of Locally Advanced Cervical Cancers: Development and Initial Use

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Foundation of the Simulator
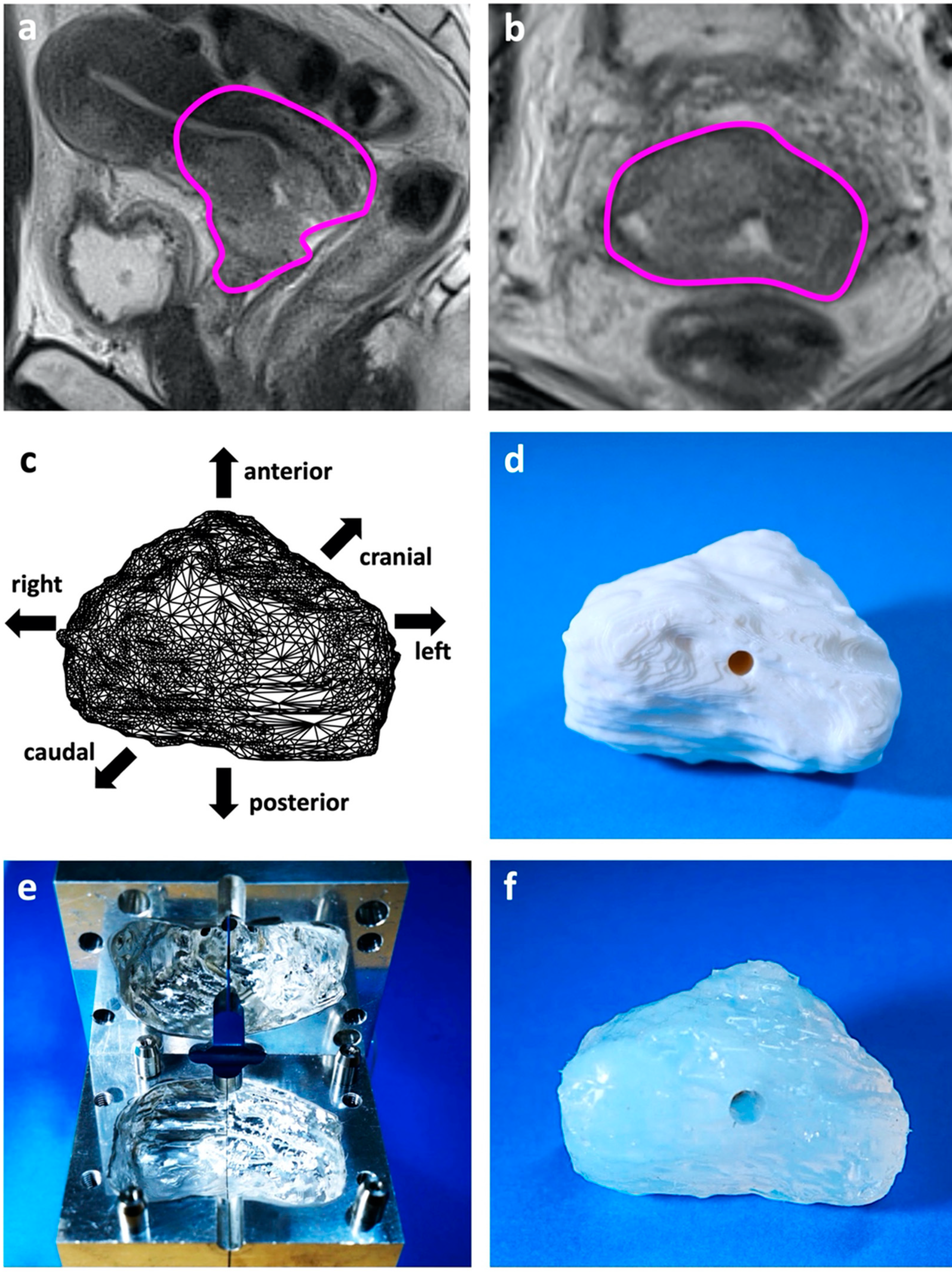
2.2. Patient-Derived Tumor Phantom
2.3. Trial Use of the IC/IS Training Simulator
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Marth, C.; Landoni, F.; Mahner, S.; McCormack, M.; Gonzalez-Martin, A.; Colombo, N.; Committee, E.G. Cervical cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2017, 28, iv72–iv83. [Google Scholar] [CrossRef]
- Monk, B.J.; Tewari, K.S.; Koh, W.J. Multimodality therapy for locally advanced cervical carcinoma: State of the art and future directions. J. Clin. Oncol. 2007, 25, 2952–2965. [Google Scholar] [CrossRef]
- Grover, S.; Longo, J.; Einck, J.; Puri, P.; Brown, D.; Chino, J.; Mahantshetty, U.; Yashar, C.; Erickson, B. The Unique Issues With Brachytherapy in Low- and Middle-Income Countries. Semin. Radiat. Oncol. 2017, 27, 136–142. [Google Scholar] [CrossRef] [PubMed]
- Viswanathan, A.N.; Thomadsen, B.; American Brachytherapy Society Cervical Cancer Recommendations Committee; American Brachytherapy Society. American Brachytherapy Society consensus guidelines for locally advanced carcinoma of the cervix. Part I: General principles. Brachytherapy 2012, 11, 33–46. [Google Scholar] [CrossRef]
- Pötter, R.; Tanderup, K.; Schmid, M.P.; Jürgenliemk-Schulz, I.; Haie-Meder, C.; Fokdal, L.U.; Sturdza, A.E.; Hoskin, P.; Mahantshetty, U.; Segedin, B.; et al. MRI-guided adaptive brachytherapy in locally advanced cervical cancer (EMBRACE-I): A multicentre prospective cohort study. Lancet Oncol. 2021, 22, 538–547. [Google Scholar] [CrossRef]
- Ohno, T.; Noda, S.E.; Okonogi, N.; Murata, K.; Shibuya, K.; Kiyohara, H.; Tamaki, T.; Ando, K.; Oike, T.; Ohkubo, Y.; et al. In-room computed tomography-based brachytherapy for uterine cervical cancer: Results of a 5-year retrospective study. J. Radiat. Res. 2017, 58, 543–551. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pötter, R.; Dimopoulos, J.; Georg, P.; Lang, S.; Waldhäusl, C.; Wachter-Gerstner, N.; Weitmann, H.; Reinthaller, A.; Knocke, T.H.; Wachter, S.; et al. Clinical impact of MRI assisted dose volume adaptation and dose escalation in brachytherapy of locally advanced cervix cancer. Radiother. Oncol. 2007, 83, 148–155. [Google Scholar] [CrossRef]
- Toita, T.; Kitagawa, R.; Hamano, T.; Umayahara, K.; Hirashima, Y.; Aoki, Y.; Oguchi, M.; Mikami, M.; Takizawa, K.; Cervical Cancer (Vulva Cancer); et al. Phase II study of concurrent chemoradiotherapy with high-dose-rate intracavitary brachytherapy in patients with locally advanced uterine cervical cancer: Efficacy and toxicity of a low cumulative radiation dose schedule. Gynecol. Oncol. 2012, 126, 211–216. [Google Scholar] [CrossRef]
- Wakatsuki, M.; Ohno, T.; Yoshida, D.; Noda, S.E.; Saitoh, J.; Shibuya, K.; Katoh, H.; Suzuki, Y.; Takahashi, T.; Nakano, T. Intracavitary combined with CT-guided interstitial brachytherapy for locally advanced uterine cervical cancer: Introduction of the technique and a case presentation. J. Radiat. Res. 2011, 52, 54–58. [Google Scholar] [CrossRef] [Green Version]
- Okazaki, S.; Murata, K.; Noda, S.E.; Kumazaki, Y.; Hirai, R.; Igari, M.; Abe, T.; Komatsu, S.; Nakano, T.; Kato, S. Dose-volume parameters and local tumor control in cervical cancer treated with central-shielding external-beam radiotherapy and CT-based image-guided brachytherapy. J. Radiat. Res. 2019, 60, 490–500. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dimopoulos, J.C.; Kirisits, C.; Petric, P.; Georg, P.; Lang, S.; Berger, D.; Pötter, R. The Vienna applicator for combined intracavitary and interstitial brachytherapy of cervical cancer: Clinical feasibility and preliminary results. Int. J. Radiat. Oncol. Biol. Phys. 2006, 66, 83–90. [Google Scholar] [CrossRef]
- Jürgenliemk-Schulz, I.M.; Tersteeg, R.J.; Roesink, J.M.; Bijmolt, S.; Nomden, C.N.; Moerland, M.A.; de Leeuw, A.A. MRI-guided treatment-planning optimisation in intracavitary or combined intracavitary/interstitial PDR brachytherapy using tandem ovoid applicators in locally advanced cervical cancer. Radiother. Oncol. 2009, 93, 322–330. [Google Scholar] [CrossRef]
- Walter, F.; Maihöfer, C.; Schüttrumpf, L.; Well, J.; Burges, A.; Ertl-Wagner, B.; Mahner, S.; Belka, C.; Gallwas, J.; Corradini, S. Combined intracavitary and interstitial brachytherapy of cervical cancer using the novel hybrid applicator Venezia: Clinical feasibility and initial results. Brachytherapy 2018, 17, 775–781. [Google Scholar] [CrossRef]
- Haie-Meder, C.; Pötter, R.; Van Limbergen, E.; Briot, E.; De Brabandere, M.; Dimopoulos, J.; Dumas, I.; Hellebust, T.P.; Kirisits, C.; Lang, S.; et al. Recommendations from Gynaecological (GYN) GEC-ESTRO Working Group (I): Concepts and terms in 3D image based 3D treatment planning in cervix cancer brachytherapy with emphasis on MRI assessment of GTV and CTV. Radiother. Oncol. 2005, 74, 235–245. [Google Scholar] [CrossRef] [PubMed]
- Pötter, R.; Haie-Meder, C.; Van Limbergen, E.; Barillot, I.; De Brabandere, M.; Dimopoulos, J.; Dumas, I.; Erickson, B.; Lang, S.; Nulens, A.; et al. Recommendations from gynaecological (GYN) GEC ESTRO working group (II): Concepts and terms in 3D image-based treatment planning in cervix cancer brachytherapy-3D dose volume parameters and aspects of 3D image-based anatomy, radiation physics, radiobiology. Radiother. Oncol. 2006, 78, 67–77. [Google Scholar] [CrossRef]
- Ebina, Y.; Mikami, M.; Nagase, S.; Tabata, T.; Kaneuchi, M.; Tashiro, H.; Mandai, M.; Enomoto, T.; Kobayashi, Y.; Katabuchi, H.; et al. Japan Society of Gynecologic Oncology guidelines 2017 for the treatment of uterine cervical cancer. Int J. Clin. Oncol. 2019, 24, 1–19. [Google Scholar] [CrossRef] [PubMed]
- Otani, Y.; Ohno, T.; Ando, K.; Murata, K.; Kato, S.; Noda, S.E.; Murofushi, K.; Ushijima, H.; Yoshida, D.; Okonogi, N.; et al. Dosimetric feasibility of computed tomography-based image-guided brachytherapy in locally advanced cervical cancer: A Japanese prospective multi-institutional study. J. Radiat. Res. 2021, 62, 502–510. [Google Scholar] [CrossRef]
- EMBRACE II Study Protocol v.1.0. Image Guided Intensity Modulated External Beam Radiochemotherapy and MRI Based Adaptive Brachytherapy in Locally Advanced Cervical Cancer. Available online: https://www.embracestudy.dk/UserUpload/PublicDocuments/EMBRACE%20II%20Protocol.pdf (accessed on 20 March 2022).
- Han, K.; Milosevic, M.; Fyles, A.; Pintilie, M.; Viswanathan, A.N. Trends in the utilization of brachytherapy in cervical cancer in the United States. Int. J. Radiat. Oncol. Biol. Phys. 2013, 87, 111–119. [Google Scholar] [CrossRef] [PubMed]
- Robin, T.P.; Amini, A.; Schefter, T.E.; Behbakht, K.; Fisher, C.M. Disparities in standard of care treatment and associated survival decrement in patients with locally advanced cervical cancer. Gynecol. Oncol. 2016, 143, 319–325. [Google Scholar] [CrossRef]
- Compton, J.J.; Gaspar, L.E.; Shrieve, D.C.; Wilson, L.D.; Griem, K.L.; Amdur, R.J.; Lee, W.R. Resident-reported brachytherapy experience in ACGME-accredited radiation oncology training programs. Brachytherapy 2013, 12, 622–627. [Google Scholar] [CrossRef] [PubMed]
- Fokdal, L.; Sturdza, A.; Mazeron, R.; Haie-Meder, C.; Tan, L.T.; Gillham, C.; Šegedin, B.; Jürgenliemk-Schultz, I.; Kirisits, C.; Hoskin, P.; et al. Image guided adaptive brachytherapy with combined intracavitary and interstitial technique improves the therapeutic ratio in locally advanced cervical cancer: Analysis from the retroEMBRACE study. Radiother. Oncol. 2016, 120, 434–440. [Google Scholar] [CrossRef]
- Spampinato, S.; Fokdal, L.U.; Pötter, R.; Haie-Meder, C.; Lindegaard, J.C.; Schmid, M.P.; Sturdza, A.; Jürgenliemk-Schulz, I.M.; Mahantshetty, U.; Segedin, B.; et al. Risk factors and dose-effects for bladder fistula, bleeding and cystitis after radiotherapy with imaged-guided adaptive brachytherapy for cervical cancer: An EMBRACE analysis. Radiother. Oncol. 2021, 158, 312–320. [Google Scholar] [CrossRef] [PubMed]
- Pötter, R.; Tanderup, K.; Kirisits, C.; de Leeuw, A.; Kirchheiner, K.; Nout, R.; Tan, L.T.; Haie-Meder, C.; Mahantshetty, U.; Segedin, B.; et al. The EMBRACE II study: The outcome and prospect of two decades of evolution within the GEC-ESTRO GYN working group and the EMBRACE studies. Clin. Transl. Radiat. Oncol. 2018, 9, 48–60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oike, T.; Ohno, T.; Noda, S.E.; Kiyohara, H.; Ando, K.; Shibuya, K.; Tamaki, T.; Takakusagi, Y.; Sato, H.; Nakano, T. Can combined intracavitary/interstitial approach be an alternative to interstitial brachytherapy with the Martinez Universal Perineal Interstitial Template (MUPIT) in computed tomography-guided adaptive brachytherapy for bulky and/or irregularly shaped gynecological tumors? Radiat. Oncol. 2014, 9, 222. [Google Scholar]
- Fionda, B.; Boldrini, L.; D’Aviero, A.; Lancellotta, V.; Gambacorta, M.A.; Kovács, G.; Patarnello, S.; Valentini, V.; Tagliaferri, L. Artificial intelligence (AI) and interventional radiotherapy (brachytherapy): State of art and future perspectives. J. Contemp. Brachyther. 2020, 12, 497–500. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Applicator | Needles | Practitioner | HR-CTV D90 | Rectum D2cc | Bladder D2cc |
|---|---|---|---|---|---|
| Fletcher-Suit | No | Expert | 4.23 Gy | 5.99 Gy | 3.73 Gy |
| Fletcher-Suit | Yes | Resident | 5.69 Gy | 5.99 Gy | 4.11 Gy |
| Fletcher-Suit | Yes | Expert | 6.70 Gy | 5.98 Gy | 4.05 Gy |
| Venezia | No | Expert | 4.16 Gy | 5.99 Gy | 3.55 Gy |
| Venezia | Yes | Resident | 6.20 Gy | 5.99 Gy | 3.61 Gy |
| Venezia | Yes | Expert | 6.45 Gy | 5.99 Gy | 3.83 Gy |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tomizawa, K.; Oike, T.; Ando, K.; Irie, D.; Sakai, M.; Shimada, H.; Ohno, T. Patient-Derived Training Simulator for Image-Guided Adaptive Brachytherapy of Locally Advanced Cervical Cancers: Development and Initial Use. J. Clin. Med. 2022, 11, 3103. https://doi.org/10.3390/jcm11113103
Tomizawa K, Oike T, Ando K, Irie D, Sakai M, Shimada H, Ohno T. Patient-Derived Training Simulator for Image-Guided Adaptive Brachytherapy of Locally Advanced Cervical Cancers: Development and Initial Use. Journal of Clinical Medicine. 2022; 11(11):3103. https://doi.org/10.3390/jcm11113103
Chicago/Turabian StyleTomizawa, Kento, Takahiro Oike, Ken Ando, Daisuke Irie, Makoto Sakai, Hirofumi Shimada, and Tatsuya Ohno. 2022. "Patient-Derived Training Simulator for Image-Guided Adaptive Brachytherapy of Locally Advanced Cervical Cancers: Development and Initial Use" Journal of Clinical Medicine 11, no. 11: 3103. https://doi.org/10.3390/jcm11113103