
Efficacy of Liraglutide in Non-Diabetic Obese Adults: A Systematic Review and Meta-Analysis of Randomized Controlled Trials

 , , and
, , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search of Studies
2.2. Eligibility Criteria
2.3. Selection of Studies
2.4. Outcomes
2.5. Data Extraction and Management
2.6. Risk of Bias Assessment
2.7. Statistical Analyses
3. Results
3.1. Selection of Studies
3.2. Characteristics of Included Studies
3.3. Risk of Bias
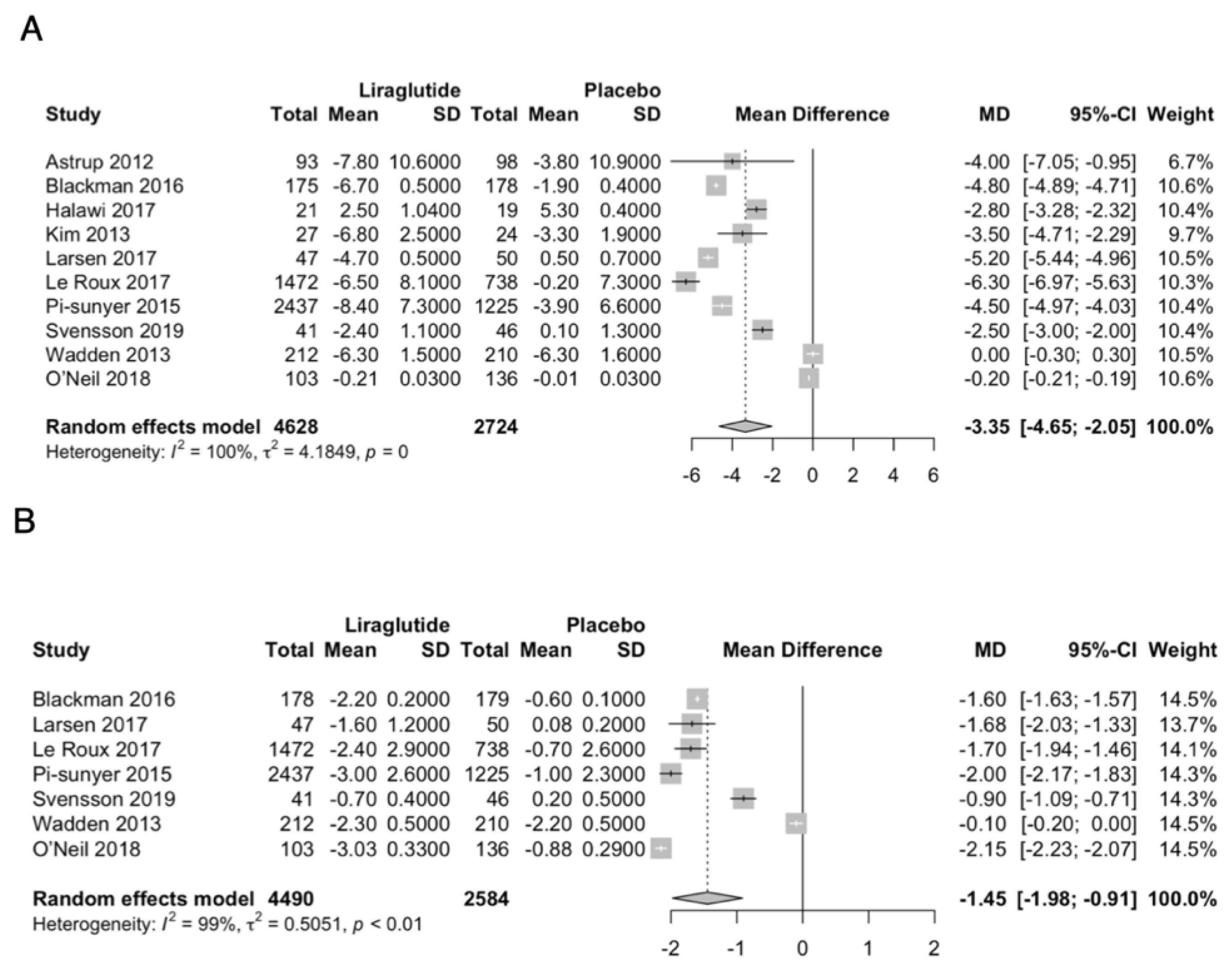
3.4. Effect on Primary Outcomes
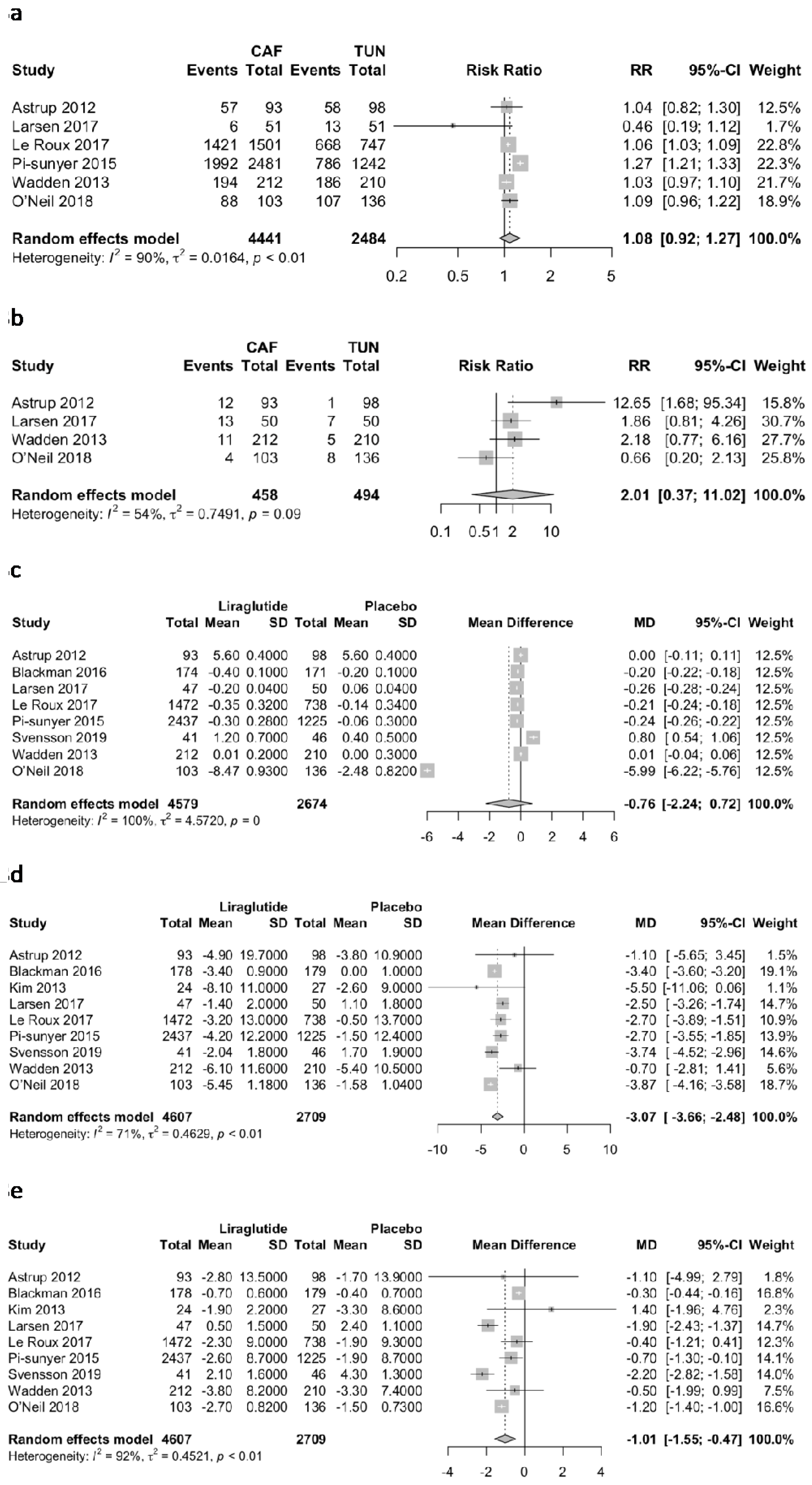
3.5. Effect on Secondary Outcomes
3.6. Subgroup Analyses
3.7. Sensitivity Analyses
3.8. Quality of Evidence
3.9. Publication Bias
4. Discussion
Main Findings
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- GBD 2015 Obesity Collaborators; Afshin, A.; Forouzanfar, M.H.; Reitsma, M.B.; Sur, P.; Estep, K.; Lee, A.; Marczak, L.; Mokdad, A.H.; Moradi-Lakeh, M.; et al. Health Effects of Overweight and Obesity in 195 Countries over 25 Years. N. Engl. J. Med. 2017, 377, 13–27. [Google Scholar] [CrossRef]
- Ahrén, B. Glucagon-like peptide-1 receptor agonists for type 2 diabetes: A rational drug development. J. Diabetes Investig. 2019, 10, 196–201. [Google Scholar] [CrossRef] [PubMed]
- Ladenheim, E. Liraglutide and obesity: A review of the data so far. Drug Des. Dev. Ther. 2015, 9, 1867–1875. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- le Roux, C.W.; Astrup, A.; Fujioka, K.; Greenway, F.; Lau, D.C.W.; Van Gaal, L.; Ortiz, R.V.; Wilding, J.P.H.; Skjøth, T.V.; Manning, L.S.; et al. 3 years of liraglutide versus placebo for type 2 diabetes risk reduction and weight management in individuals with prediabetes: A randomised, double-blind trial. Lancet 2017, 389, 1399–1409. [Google Scholar] [CrossRef] [Green Version]
- Chou, C.; Chuang, S. Evaluation of the efficacy of low-dose liraglutide in weight control among Taiwanese non-diabetes patients. J. Diabetes Investig. 2020, 11, 1524–1531. [Google Scholar] [CrossRef] [PubMed]
- Page, M.; McKenzie, J.; Bossuyt, P.; Boutron, I.; Hoffmann, T.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An up-dated guideline for reporting systematic reviews. Int. J. Surg. 2020, 88, 105906. [Google Scholar] [CrossRef]
- Nilsson, M.E.; Koke, S.C. Defining Treatment-Emergent Adverse Events with the Medical Dictionary for Regulatory Activities (MedDRA). Drug Inf. J. 2001, 35, 1289–1299. [Google Scholar] [CrossRef]
- Santiago, J.V.; Pereira, M.B.; Avioli, L.V. Fasting hypoglycemia in adults. Arch. Intern. Med. 1982, 142, 465–468. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [Green Version]
- Van Aert, R.C.M.; Jackson, D. Multistep estimators of the between-study variance: The relationship with the Paule-Mandel estimator. Stat. Med. 2018, 37, 2616–2629. [Google Scholar] [CrossRef] [Green Version]
- Guyatt, G.H.; Oxman, A.D.; Schuenemann, H.J.; Tugwell, P.; Knottnerus, A. GRADE guidelines: A new series of articles in the Journal of Clinical Epidemiology. J. Clin. Epidemiol. 2011, 64, 380–382. [Google Scholar] [CrossRef] [PubMed]
- Astrup, A.; Carraro, R.; Finer, N.; Harper, A.; Kunesova, M.; Lean, M.E.J.; Niskanen, L.; Rasmussen, M.F.; Rissanen, A.; Rössner, S.; et al. Safety, tolerability and sustained weight loss over 2 years with the once-daily human GLP-1 analog, liraglutide. Int. J. Obes. 2012, 36, 843–854. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, S.H.; Abbasi, F.; Lamendola, C.; Liu, A.; Ariel, D.; Schaaf, P.; Grove, K.; Tomasso, V.; Ochoa, H.; Liu, Y.V.; et al. Benefits of Liraglutide Treatment in Overweight and Obese Older Individuals with Prediabetes. Diabetes Care 2013, 36, 3276–3282. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wadden, T.A.; Hollander, P.; Klein, S.; Niswender, K.; Woo, V.; Hale, P.M.; Aronne, L. Weight maintenance and additional weight loss with liraglutide after low-calorie-diet-induced weight loss: The SCALE Maintenance randomized study. Int. J. Obes. 2013, 37, 1443–1451. [Google Scholar] [CrossRef] [Green Version]
- Lean, M.E.J.; Carraro, R.; Finer, N.; Hartvig, H.; Lindegaard, M.L.; Rössner, S.; van Gaal, L.; Astrup, A.; on behalf of the NN8022-1807 Investigators. Tolerability of nausea and vomiting and associations with weight loss in a randomized trial of liraglutide in obese, non-diabetic adults. Int. J. Obes. 2014, 38, 689–697. [Google Scholar] [CrossRef] [Green Version]
- Pi-Sunyer, X.; Astrup, A.; Fujioka, K.; Greenway, F.; Halpern, A.; Krempf, M.; Lau, D.C.W.; Le Roux, C.W.; Ortiz, R.V.; Jensen, C.B.; et al. A Randomized, Controlled Trial of 3.0 mg of Liraglutide in Weight Management. N. Engl. J. Med. 2015, 373, 11–22. [Google Scholar] [CrossRef]
- Blackman, A.; Foster, G.D.; Zammit, G.; Rosenberg, R.; Aronne, L.; Wadden, T.; Claudius, B.; Jensen, C.B.; Mignot, E.; on behalf of the SCALE study group. Effect of liraglutide 3.0 mg in individuals with obesity and moderate or severe obstructive sleep apnea: The SCALE Sleep Apnea randomized clinical trial. Int. J. Obes. 2016, 40, 1310–1319. [Google Scholar] [CrossRef] [Green Version]
- Halawi, H.; Khemani, D.; Eckert, D.; O’Neill, J.; Kadouh, H.; Grothe, K.; Clark, M.M.; Burton, D.D.; Vella, A.; Acosta, A.; et al. Effects of liraglutide on weight, satiation, and gastric functions in obesity: A randomised, placebo-controlled pilot trial. Lancet Gastroenterol. Hepatol. 2017, 2, 890–899. [Google Scholar] [CrossRef]
- Larsen, J.R.; Vedtofte, L.; Jakobsen, M.S.L.; Jespersen, H.R.; Jakobsen, M.I.; Svensson, C.K.; Koyuncu, K.; Schjerning, O.; Oturai, P.S.; Kjaer, A.; et al. Effect of Liraglutide Treatment on Prediabetes and Overweight or Obesity in Clozapine- or Olanzapine-Treated Patients with Schizophrenia Spectrum Disorder: A Randomized Clinical Trial. JAMA Psychiatry 2017, 74, 719–728. [Google Scholar] [CrossRef]
- O’Neil, P.; Birkenfeld, A.L.; McGowan, B.; Mosenzon, O.; Pedersen, S.D.; Wharton, S.; Carson, C.G.; Jepsen, C.H.; Kabisch, M.; Wilding, J.P.H. Efficacy and safety of semaglutide compared with liraglutide and placebo for weight loss in patients with obesity: A randomised, double-blind, placebo and active controlled, dose-ranging, phase 2 trial. Lancet 2018, 392, 637–649. [Google Scholar] [CrossRef]
- Svensson, C.K.; Larsen, J.R.; Vedtofte, L.; Jakobsen, M.S.L.; Jespersen, H.R.; Jakobsen, M.I.; Koyuncu, K.; Schjerning, O.; Nielsen, J.; Ekstrøm, C.T.; et al. One-year follow-up on liraglutide treatment for prediabetes and overweight/obesity in clozapine- or olanzapine-treated patients. Acta Psychiatr. Scand. 2019, 139, 26–36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saxena, A.R.; Banerjee, A.; Corbin, K.D.; Parsons, S.A.; Smith, S.R. Energy intake as a short-term biomarker for weight loss in adults with obesity receiving liraglutide: A randomized trial. Obes. Sci. Pract. 2021, 7, 281–290. [Google Scholar] [CrossRef] [PubMed]
- Tronieri, J.S.; Fabricatore, A.N.; Wadden, T.A.; Auerbach, P.; Endahl, L.; Sugimoto, D.; Rubino, D. Effects of Dietary Self-Monitoring, Physical Activity, Liraglutide 3.0 mg, and Placebo on Weight Loss in the SCALE IBT Trial. Obes. Facts 2020, 13, 572–583. [Google Scholar] [CrossRef]
- Thakur, U.; Bhansali, A.; Gupta, R.; Rastogi, A. Liraglutide Augments Weight Loss After Laparoscopic Sleeve Gastrectomy: A Randomised, Double-Blind, Placebo-Control Study. Obes. Surg. 2020, 31, 84–92. [Google Scholar] [CrossRef] [PubMed]
- Verma, S.; McGuire, D.K.; Bain, S.C.; Bhatt, D.L.; Leiter, L.A.; Mazer, C.D.; Fries, T.M.; Pratley, R.E.; Rasmussen, S.; Vrazic, H.; et al. Effects of glucagon-like peptide-1 receptor agonists liraglutide and semaglutide on cardiovascular and renal outcomes across body mass index categories in type 2 diabetes: Results of the LEADER and SUSTAIN 6 trials. Diabetes Obes. Metab. 2020, 22, 2487–2492. [Google Scholar] [CrossRef]
- Kaji, N.; Takagi, Y.; Matsuda, S.; Takahashi, A.; Fujio, S.; Asai, F. Effects of liraglutide on metabolic syndrome in WBN/Kob diabetic fatty rats supplemented with a high-fat diet. Anim. Model. Exp. Med. 2020, 3, 62–68. [Google Scholar] [CrossRef]
- Li, Z.; Yang, P.; Liang, Y.; Xia, N.; Li, Y.; Su, H.; Pan, H. Effects of liraglutide on lipolysis and the AC3/PKA/HSL pathway. Diabetes Metab. Syndr. Obes. Targets Ther. 2019, 12, 1697–1703. [Google Scholar] [CrossRef] [Green Version]
- Suhrs, H.E.; Raft, K.F.; Bové, K.; Madsbad, S.; Holst, J.J.; Zander, M.; Prescott, E. Effect of liraglutide on body weight and microvascular function in non-diabetic overweight women with coronary microvascular dysfunction. Int. J. Cardiol. 2019, 283, 28–34. [Google Scholar] [CrossRef]
- Khera, R.; Murad, M.H.; Chandar, A.K.; Dulai, P.S.; Wang, Z.; Prokop, L.J.; Loomba, R.; Camilleri, M.; Singh, S. Association of Pharmacological Treatments for Obesity with Weight Loss and Adverse Events: A Systematic Review and Meta-analysis. JAMA 2016, 315, 2424–2434. [Google Scholar] [CrossRef]
- Zhang, P.; Liu, Y.; Ren, Y.; Bai, J.; Zhang, G.; Cui, Y. The efficacy and safety of liraglutide in the obese, non-diabetic individuals: A systematic review and meta-analysis. Afr. Health Sci. 2019, 19, 2591–2599. [Google Scholar] [CrossRef]
- Diaz-Arocutipa, C.; Benites-Meza, J.K.; Chambergo-Michilot, D.; Barboza, J.J.; Pasupuleti, V.; Bueno, H.; Sambola, A.; Hernandez, A.V. Efficacy and Safety of Colchicine in Post-acute Myocardial Infarction Patients: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Front. Cardiovasc. Med. 2021, 8, 676771. [Google Scholar] [CrossRef] [PubMed]
- Barboza, J.J.; Albitres-Flores, L.; Rivera-Meza, M.; Rodriguez-Huapaya, J.; Caballero-Alvarado, J.; Pasupuleti, V.; Hernandez, A.V. Short-term efficacy of umbilical cord milking in preterm infants: Systematic review and meta-analysis. Pediatr. Res. 2021, 89, 22–30. [Google Scholar] [CrossRef] [PubMed]
- Barboza, J.J.; Chambergo-Michilot, D.; Velasquez-Sotomayor, M.; Silva-Rengifo, C.; Diaz-Arocutipa, C.; Caballero-Alvarado, J.; Garcia-Solorzano, F.O.; Alarcon-Ruiz, C.A.; Albitres-Flores, L.; Rodriguez-Morales, A.J.; et al. Assessment and management of asymptomatic COVID-19 infection: A systematic review. Travel Med. Infect. Dis. 2021, 41, 102058. [Google Scholar] [CrossRef] [PubMed]
- Hernandez, A.V.; Ingemi, J., III; Sherman, M.; Pasupuleti, V.; Barboza, J.J.; Piscoya, A.; Roman, Y.M.; White, C.M. Impact of Prophylactic Hydroxychloroquine on People at High Risk of COVID-19: A Systematic Review and Meta-Analysis. J. Clin. Med. 2021, 10, 2609. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Author | Country | Number of Participants | Age (Mean, SD) | Male (n, %) | HbA1c at Baseline (Mean, SD) | BMI kg/m2 at Baseline (Mean, SD) | Liraglutide Starting and Maximum Doses | Type of Control | Length of Treatment or Following | Primary Outcomes |
|---|---|---|---|---|---|---|---|---|---|---|
| Astrup, 2012 | Denmark | 191 | 45.9 (10.7) | 48 (25%) | LG: 5.6 (0.4); Control: 5.6 (0.4) | NR | Liraglutide 3.0 mg once-daily (increased by 0.6 mg/week) | Placebo | 52 weeks | Body weight loss and glycemic parameters |
| Blackman, 2016 | USA | 359 | 48.6 (9.9) | 258 (73%) | LG: 5.7 (0.4); Control: 5.6 (0.4) | LG: 38.9 (6.4); Control: 39.4 (7.4) | Liraglutide 3.0 mg once-daily (increased by 0.6 mg/week) | Placebo | 32 weeks | Apnea–hypopnea index and Body weight loss |
| Halawi, 2017 | USA | 40 | 37 (29.2) | NR | NR | LG: 37.2 (8.2); Control: 34.6 (6.4) | Liraglutide was administered as recommended by the FDA: initiated at 0.6 mg daily for 1 week, with instructions to increase by 0.6 mg weekly until 3.0 mg was reached (over 4 weeks). | Placebo | 16 weeks | Body weight loss |
| Kim, 2013 | USA | 51 | 58 (7) | 18 (35%) | NR | LG: 31.9 (2.7); Control: 31.9 (3.5) | The starting dose of medication was 0.6 mg; the dose was titrated by 0.6 mg weekly to a maximum dose of 1.8 mg. | Placebo | 14 weeks | Body weight loss and inflammatory markers |
| Larsen, 2017 | Denmark | 103 | 42.1 (10.7) | 60 (58%) | LG: 5.6 (0.4); Control: 5.5 (0.4) | LG: 33.7 (5.1); Control: 33.9 (6.6) | The participants followed a fixed uptitration schedule of 0.6 mg per week to a daily dose of 1.8 mg. | Placebo | 16 weeks | Glucose tolerance, Body weight loss |
| Lean, 2014 | UK | 188 | 45.9 (10.7) | 48 (26%) | NR | LG: 34.8 (2.8); Control: 34.9 (2.8) | Liraglutide doses of 3.0 mg were administered once daily by evening subcutaneous injection, starting with doses of 0.6 mg per day and increasing by weekly increments of 0.6 mg (dose escalation). | Placebo | 20 weeks | Adverse events |
| Le Roux, 2017 | USA | 2254 | NR | 540 (24%) | LG: 5.8 (0.3); Control: 5.7 (0.3) | LG: 38.8 (6.4); Control: 39 (6.3) | Start Liraglutide at 0.6 mg with weekly 0.6 mg incremental increases to 3.0 mg. | Placebo | 56 weeks | Proportion of individuals with type 2 diabetes, Body weight loss |
| O’Neil | USA | 957 | 47 (12) | 338 (35%) | LG: 5.5 (0.4); Control: 5.5 (0.4) | LG: 38.6 (6.6); Control: 40.1 (7.2) | Liraglutide (3·0 mg) as once-daily subcutaneous injections | Placebo | 52 weeks | Body weight loss |
| Pi-sunyer, 2015 | USA | 3731 | 45.2 (12.1) | 803 (22%) | LG: 5.6 (0.4); Control: 5.6 (0.4) | LG: 38.3 (6.4); Control: 39.3 (6.3) | Starting at a dose of 0.6 mg with weekly 0.6 mg increments to 3.0 mg | Placebo | 56 weeks | Body weight loss |
| Saxena | USA | 56 | 46 (10.9) | 18 (32%) | NR | NR | Liraglutide initiated at a dose of 0.6 mg/day and escalated by 0.6 mg/week up to a maximum of 3.0 mg/day) | Placebo | 6 weeks | Change from baseline (CFB) in mean EI (in kcal) during ad libitum lunch meals. |
| Svensson, 2019 | Denmark | 97 | 42.1 (10.7) | 60 (62%) | NR | LG: 38.9 (6.4); Control: 39.4 (7.4) | Starting at a dose of 0.6 mg with weekly 0.6-mg increments to 1.8 mg | Placebo | 16 weeks | Body weight loss |
| Wadden, 2013 | USA | 222 | 45.9 (11.9) | 37 (17%) | LG: 5.6 (0.4); Control: 5.6 (0.4) | LG: 36(5.9); Control: 35.2 (5.9) | Liraglutide 3.0 mg once-daily | Placebo | 56 weeks | Body weight loss |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Barboza, J.J.; Huamán, M.R.; Melgar, B.; Diaz-Arocutipa, C.; Valenzuela-Rodriguez, G.; Hernandez, A.V. Efficacy of Liraglutide in Non-Diabetic Obese Adults: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. J. Clin. Med. 2022, 11, 2998. https://doi.org/10.3390/jcm11112998
Barboza JJ, Huamán MR, Melgar B, Diaz-Arocutipa C, Valenzuela-Rodriguez G, Hernandez AV. Efficacy of Liraglutide in Non-Diabetic Obese Adults: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Journal of Clinical Medicine. 2022; 11(11):2998. https://doi.org/10.3390/jcm11112998
Chicago/Turabian StyleBarboza, Joshuan J., Mariella R. Huamán, Beatriz Melgar, Carlos Diaz-Arocutipa, German Valenzuela-Rodriguez, and Adrian V. Hernandez. 2022. "Efficacy of Liraglutide in Non-Diabetic Obese Adults: A Systematic Review and Meta-Analysis of Randomized Controlled Trials" Journal of Clinical Medicine 11, no. 11: 2998. https://doi.org/10.3390/jcm11112998