
One and Five-Year Mortality Risk Prediction in Patients with Moderate and Severe Aortic Stenosis

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source and Patient Population
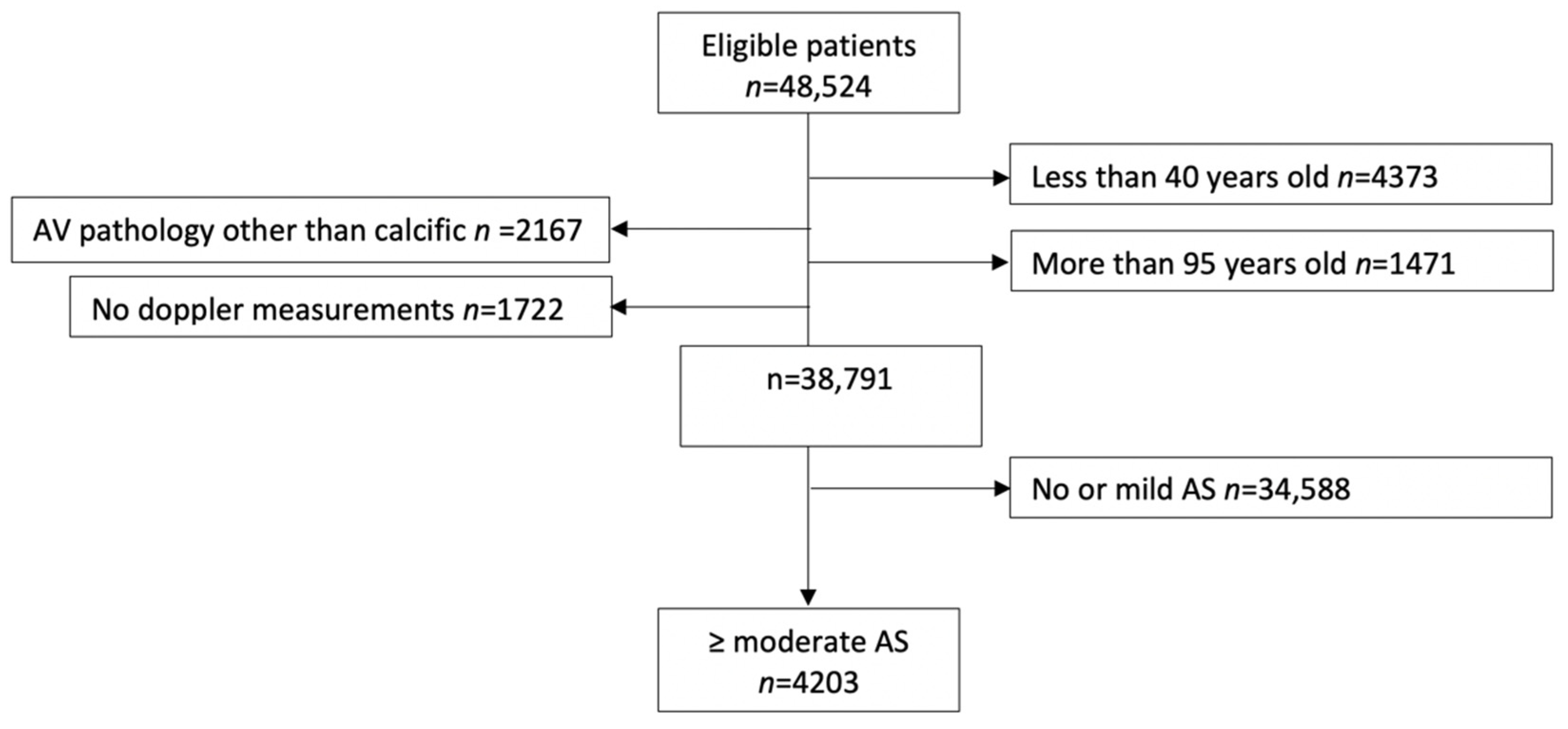
2.2. Analytic Cohort Building
2.3. Aortic Stenosis Severity
2.4. Patient Characteristics
2.5. Aortic Valve Replacement
2.6. Mortality Data
2.7. Statistical Analysis
3. Results
3.1. Patient Characteristics and Comorbidities
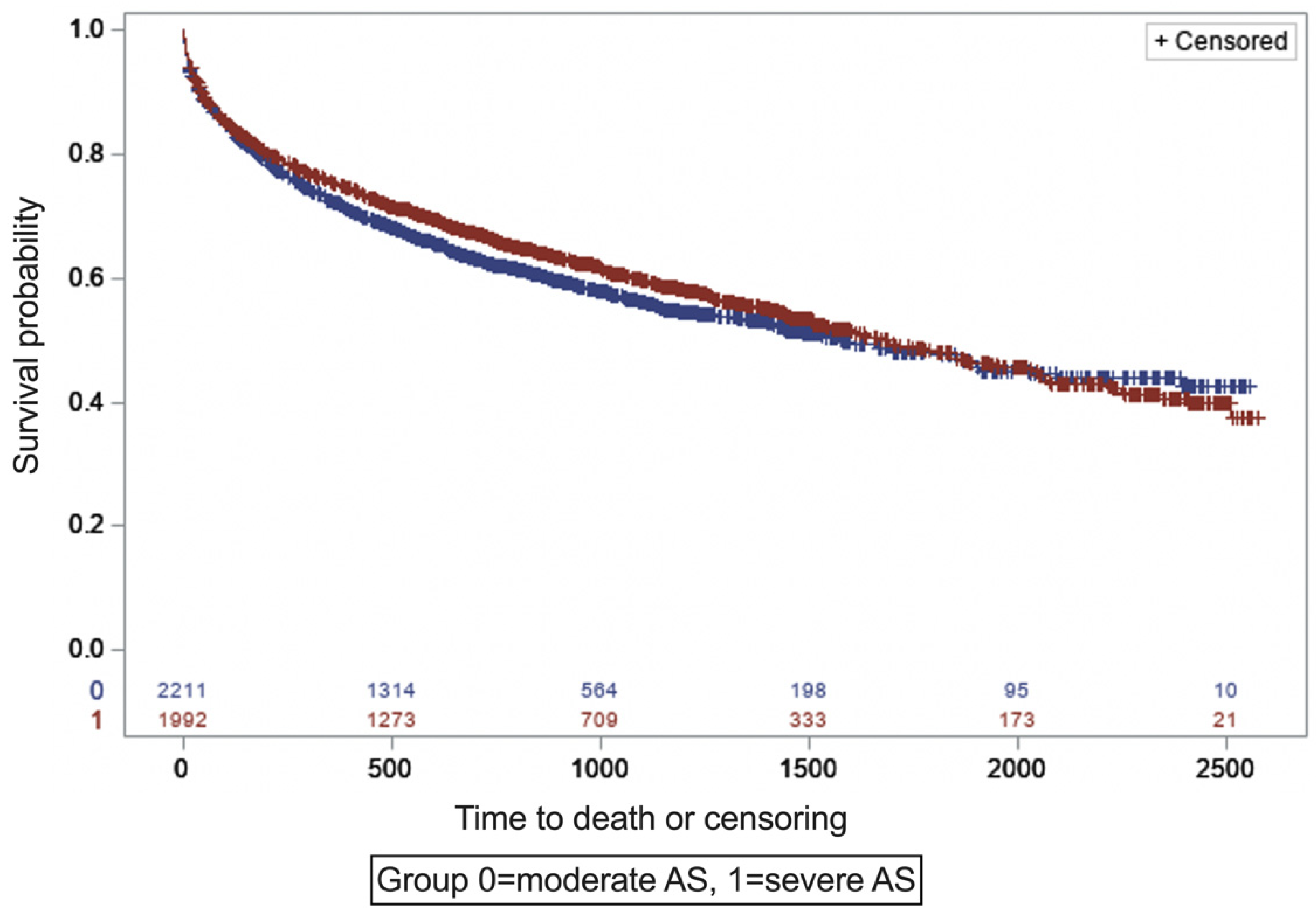
3.2. Comparative Mortality of Patients with Moderate and Severe AS
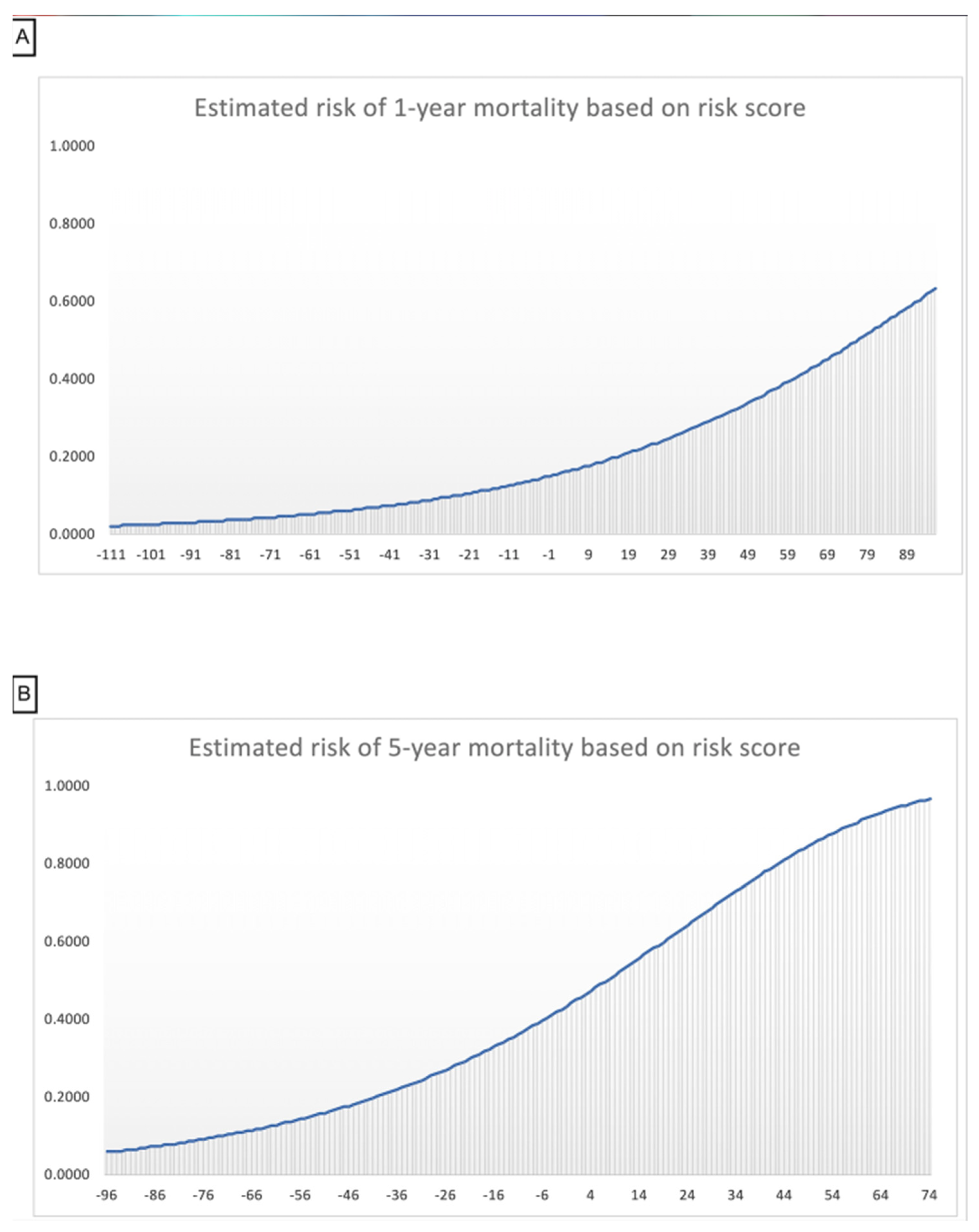
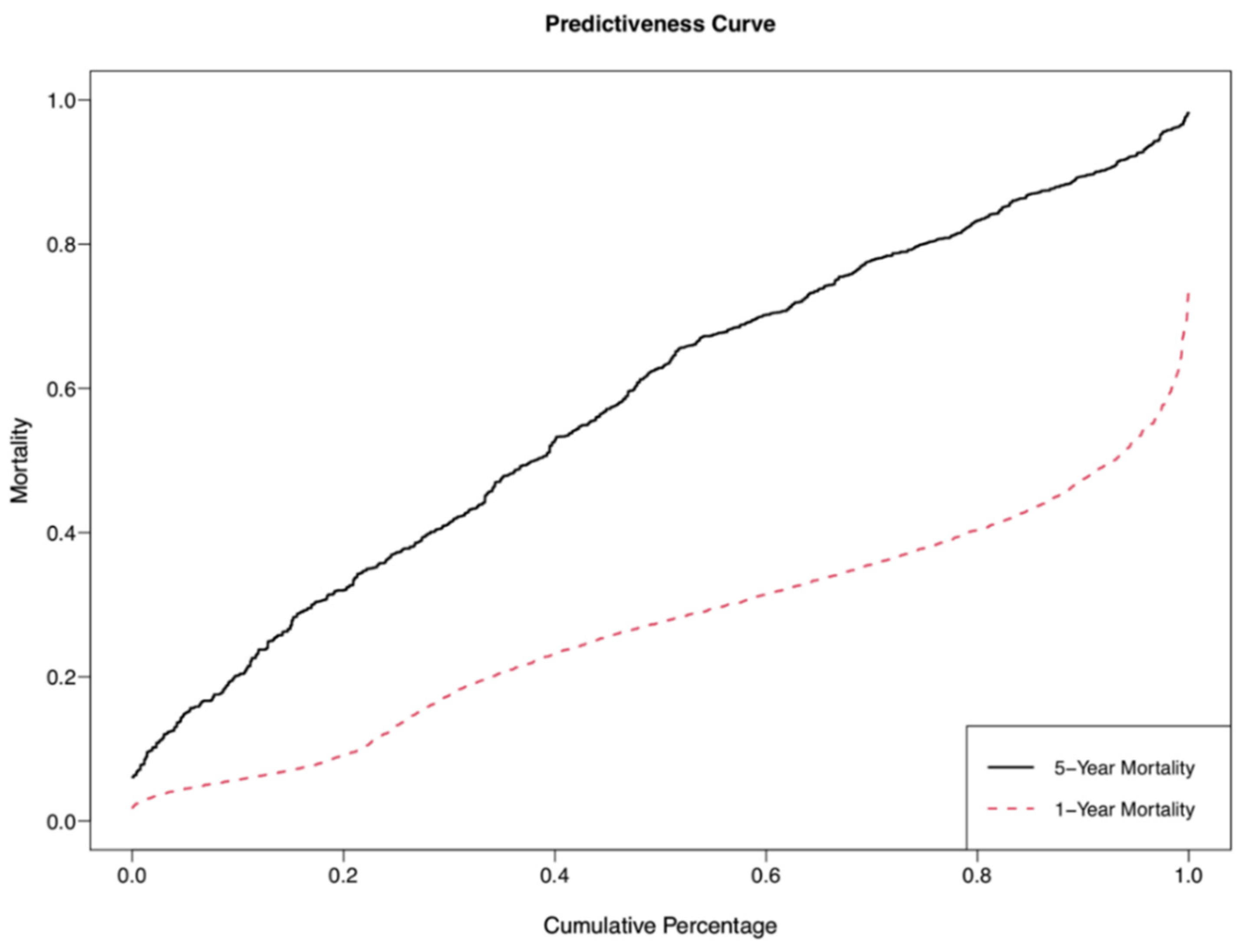
3.3. Predicted Survival among Patients with Moderate and Severe AS
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Disease | ICD10 Code |
|---|---|
| Aortic insufficiency | I35.1 |
| Atrial fibrillation | I48.91, I48.0 |
| Coronary artery disease | I25.10, I21.9, I25.5, I25.2 |
| Stroke | I61.9, I63.9 |
| Chronic kidney disease | N18.6, N18.9, N18.3, N18.6, Z99.2 |
| Chronic obstructive pulmonary disease | J44.9 |
| Endocarditis | I38 |
| Heart failure | I50.9 |
| Heart transplant status | Z94.1 |
| Ventricular assisted device | Z95.811, Z95.812 |
| Hyperlipidemia | E78.5, E78.00 |
| Hypertrophic obstructive cardiomyopathy | I42.1, I42.2 |
| Hypertension | I10 |
| Obesity | E66.9, E66.01 |
| Prosthetic heart valve | Z95.2, Z95.1 |
| Peripheral vascular disease | I73.9 |
| Diabetes mellitus | E10.9, E11.9, E11.65 |
Appendix B

References
- Nkomo, V.T.; Gardin, J.M.; Skelton, T.N.; Gottdiener, J.S.; Scott, C.G.; Enriquez-Sarano, M. Burden of valvular heart diseases: A population-based study. Lancet 2006, 368, 1005–1011. [Google Scholar] [CrossRef]
- Benjamin, E.J.; Virani, S.S.; Callaway, C.W.; Chamberlain, A.M.; Chang, A.R.; Cheng, S.; Chiuve, S.E.; Cushman, M.; Delling, F.N.; Deo, R.; et al. Heart Disease and Stroke Statistics-2018 Update: A Report From the American Heart Association. Circulation 2018, 137, e67–e492. [Google Scholar] [CrossRef] [PubMed]
- Faggiano, P.; Frattini, S.; Zilioli, V.; Rossi, A.; Nistri, S.; Dini, F.L.; Lorusso, R.; Tomasi, C.; Cas, L.D. Prevalence of comorbidities and associated cardiac diseases in patients with valve aortic stenosis. Potential implications for the decision-making process. Int. J. Cardiol. 2012, 159, 94–99. [Google Scholar] [CrossRef] [PubMed]
- Tang, L.; Gössl, M.; Ahmed, A.; Garberich, R.; Bradley, S.M.; Niikura, H.; Witt, D.; Pedersen, W.R.; Bae, R.; Lesser, J.R.; et al. Contemporary Reasons and Clinical Outcomes for Patients With Severe, Symptomatic Aortic Stenosis Not Undergoing Aortic Valve Replacement. Circ. Cardiovasc. Interv. 2018, 11, e007220. [Google Scholar] [CrossRef] [PubMed]
- Lancellotti, P.; Magne, J.; Dulgheru, R.; Clavel, M.-A.; Donal, E.; Vannan, M.A.; Chambers, J.; Rosenhek, R.; Habib, G.; Lloyd, G.; et al. Outcomes of Patients With Asymptomatic Aortic Stenosis Followed Up in Heart Valve Clinics. JAMA Cardiol. 2018, 3, 1060–1068. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Strange, G.; Stewart, S.; Celermajer, D.; Prior, D.; Scalia, G.M.; Marwick, T.; Ilton, M.; Joseph, M.; Codde, J.; Playford, D. Poor Long-Term Survival in Patients With Moderate Aortic Stenosis. J. Am. Coll. Cardiol. 2019, 74, 1851–1863. [Google Scholar] [CrossRef] [PubMed]
- Rosenhek, R.; Klaar, U.; Schemper, M.; Scholten, C.; Heger, M.; Gabriel, H.; Binder, T.; Maurer, G.; Baumgartner, H. Mild and moderate aortic stenosis Natural history and risk stratification by echocardiography. Eur. Heart J. 2004, 25, 199–205. [Google Scholar] [CrossRef] [Green Version]
- Otto, C.M. Aortic stenosis: Even mild disease is significant. Eur. Heart J. 2004, 25, 185–187. [Google Scholar] [CrossRef]
- Rudolph, T.K.; Messika-Zeitoun, D.; Frey, N.; Thambyrajah, J.; Serra, A.; Schulz, E.; Maly, J.; Aiello, M.; Lloyd, G.; Bortone, A.S.; et al. Impact of selected comorbidities on the presentation and management of aortic stenosis. Open Heart 2020, 7, e001271. [Google Scholar] [CrossRef]
- Otto, C.M.; Kuusisto, J.; Reichenbach, D.D.; Gown, A.M.; O’Brien, K.D. Characterization of the early lesion of ’degenerative’ valvular aortic stenosis. Histological and immunohistochemical studies. Circulation 1994, 90, 844–853. [Google Scholar] [CrossRef] [Green Version]
- Lindroos, M.; Kupari, M.; Valvanne, J.; Strandberg, T.; Heikkilä, J.; Tilvis, R. Factors associated with calcific aortic valve degeneration in the elderly. Eur. Heart J. 1994, 15, 865–870. [Google Scholar] [CrossRef] [PubMed]
- Arnold, S.V.; Afilalo, J.; Spertus, J.A.; Tang, Y.; Baron, S.J.; Jones, P.G.; Reardon, M.J.; Yakubov, S.J.; Adams, D.H.; Cohen, D.J. Prediction of Poor Outcome After Transcatheter Aortic Valve Replacement. J. Am. Coll. Cardiol. 2016, 68, 1868–1877. [Google Scholar] [CrossRef]
- Edwards, F.H.; Cohen, D.J.; O’Brien, S.M.; Peterson, E.D.; Mack, M.J.; Shahian, D.M.; Grover, F.L.; Tuzcu, E.M.; Thourani, V.H.; Carroll, J.; et al. Development and Validation of a Risk Pre-diction Model for In-Hospital Mortality After Transcatheter Aortic Valve Replacement. JAMA Cardiol. 2016, 1, 46–52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Minamino-Muta, E.; Kato, T.; Morimoto, T.; Taniguchi, T.; Ando, K.; Kanamori, N.; Murata, K.; Kitai, T.; Kawase, Y.; Miyake, M.; et al. A risk prediction model in asymptomatic patients with severe aortic stenosis: CURRENT-AS risk score. Eur. Hear. J.—Qual. Care Clin. Outcomes 2020, 6, 166–174. [Google Scholar] [CrossRef] [PubMed]
- Braunwald, E. Aortic Stenosis: Then and Now. Circulation 2018, 137, 2099–2100. [Google Scholar] [CrossRef] [PubMed]
- Sundt, T.M.; Bailey, M.S.; Moon, M.R.; Mendeloff, E.N.; Huddleston, C.B.; Pasque, M.K.; Barner, H.B.; Gay, W.A., Jr. Quality of life after aortic valve replacement at the age of >80 years. Circulation 2000, 102 (Suppl. 3), Iii-70–Iii–74. [Google Scholar] [CrossRef]
- Deutsch, M.-A.; Bleiziffer, S.; Elhmidi, Y.; Piazza, N.; Voss, B.; Lange, R.; Krane, M. Beyond Adding Years to Life: Health-related Quality-of-life and Functional Outcomes in Patients with Severe Aortic Valve Stenosis at High Surgical Risk Undergoing Transcatheter Aortic Valve Replacement. Curr. Cardiol. Rev. 2013, 9, 281–294. [Google Scholar] [CrossRef] [Green Version]
- Bevan, G.H.; Zidar, D.A.; Josephson, R.A.; Al-Kindi, S.G. Mortality Due to Aortic Stenosis in the United States, 2008-2017. JAMA 2019, 321, 2236–2238. [Google Scholar] [CrossRef]
- Bach, D.S.; Siao, D.; Girard, S.E.; Duvernoy, C.; McCallister, B.D., Jr.; Gualano, S.K. Evaluation of patients with severe symptomatic aortic stenosis who do not undergo aortic valve replacement: The potential role of subjectively overestimated operative risk. Circ. Cardiovasc. Qual. Outcomes 2009, 2, 533–539. [Google Scholar] [CrossRef] [Green Version]
- Beydoun, H.A.; Beydoun, M.A.; Liang, H.; Dore, G.A.; Shaked, D.; Zonderman, A.B.; Eid, S.M. Sex, Race, and Socioeconomic Disparities in Patients With Aortic Stenosis (from a Nationwide Inpatient Sample). Am. J. Cardiol. 2016, 118, 860–865. [Google Scholar] [CrossRef] [Green Version]
- Baumgartner, H.; Falk, V.; Bax, J.J.; De Bonis, M.; Hamm, C.; Holm, P.J.; Iung, B.; Lancellotti, P.; Lansac, E.; Rodriguez Muñoz, D.; et al. 2017 ESC/EACTS Guidelines for the management of valvular heart disease. Eur. Heart J. 2017, 38, 2739–2791. [Google Scholar] [CrossRef] [PubMed]
- Shtatland, E.S.; Kleinman, K.; Cain, E.M. Model Building in PROC PHREG with Automatic Variable Selection and Information Criteria; SUGI ‘30 Proceeding, Paper 206-30; SAS Institute, Inc.: Cary, NC, USA, 2004. [Google Scholar]
- Sullivan, L.M.; Massaro, J.M.; D’Agostino, R.B., Sr. Presentation of multivariate data for clinical use: The Framingham Study risk score functions. Stat. Med. 2004, 23, 1631–1660. [Google Scholar] [CrossRef] [PubMed]
- Nishimura, R.A.; Otto, C.M.; Bonow, R.O.; Carabello, B.A.; Erwin, J.P., 3rd; Fleisher, L.A.; Jneid, H.; Mack, M.J.; McLeod, C.J.; O’Gara, P.T.; et al. 2017 AHA/ACC Focused Update of the 2014 AHA/ACC Guideline for the Management of Patients With Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation 2017, 135, e1159–e1195. [Google Scholar] [CrossRef]
- Freed, B.H.; Sugeng, L.; Furlong, K.; Mor-Avi, V.; Raman, J.; Jeevanandam, V.; Lang, R.M. Reasons for Nonadherence to Guidelines for Aortic Valve Replacement in Patients with Severe Aortic Stenosis and Potential Solutions. Am. J. Cardiol. 2010, 105, 1339–1342. [Google Scholar] [CrossRef] [PubMed]
- Charlson, E.; Legedza, A.T.; Hamel, M.B. Decision-making and outcomes in severe symptomatic aortic stenosis. J. Hear. Valve Dis. 2006, 15, 312. [Google Scholar]
- Ng, A.C.; Delgado, V.; Bertini, M.; Antoni, M.L.; van Bommel, R.J.; Van Rijnsoever, E.P.; Van Der Kley, F.; Ewe, S.H.; Witkowski, T.; Auger, D.; et al. Alterations in multidirectional myocardial functions in patients with aortic stenosis and preserved ejection fraction: A two-dimensional speckle tracking analysis. Eur. Heart J. 2011, 32, 1542–1550. [Google Scholar] [CrossRef] [PubMed]
- Li, S.X.; Patel, N.K.; Flannery, L.D.; Selberg, A.; Kandanelly, R.R.; Morrison, F.J.; Kim, J.; Tanguturi, V.K.; Crousillat, D.R.; Shaqdan, A.W.; et al. Trends in Utilization of Aortic Valve Replacement for Severe Aortic Stenosis. J. Am. Coll. Cardiol. 2022, 79, 864–877. [Google Scholar] [CrossRef]



| Moderate AS n = 2212 | Severe AS n = 1991 | p | |
|---|---|---|---|
| Age/year | 76.09 ± 11.5 | 80.26 ± 10.6 | <0.0001 |
| Sex (male) | 1178 (53.3%) | 1043 (52.4%) | 0.5730 |
| Race—Caucasian | 1843 (83.3%) | 1764 (88.6%) | <0.0001 |
| Race—African American | 206 (9.3%) | 119 (6%) | |
| Race—Other | 156 (7.1%) | 108 (5.4%) | |
| BSA (m2) | 1.89 ± 0.28 | 1.86 ± 0.28 | <0.0001 |
| Smoking | 694 (31.4%) | 560 (28.1%) | 0.0216 |
| Ejection fraction (%) | 57.01 ± 14 | 56.68 ± 14.62 | <0.0001 |
| Diabetes mellitus | 726 (32.8%) | 615 (30.9%) | 0.1797 |
| Dyslipidemia | 1285 (58.1%) | 1194 (60%) | 0.2166 |
| Obesity | 181 (8.2%) | 121 (6.1%) | 0.0083 |
| CKD | 345 (15.6%) | 328 (16.5%) | 0.4387 |
| Stroke | 303 (13.7%) | 226 (11.4%) | 0.0220 |
| Atrial fibrillation | 555 (25.1%) | 602 (30.2%) | 0.0002 |
| CHD | 751 (34%) | 834 (41.9%) | <0.0001 |
| COPD | 359(16.2%) | 323 (16.2%) | 0.9953 |
| PVD | 222 (10%) | 230 (11.6%) | 0.1132 |
| Heart failure | 409 (18.5%) | 453 (22.8%) | 0.0006 |
| Hypertension | 1708 (77.2%) | 1560 (78.4%) | 0.3760 |
| AV intervention | 61 (2.8%) | 931 (46.8%) | <0.0001 |
| Peak Velocity (m/sec) | 2.82 ± 0.65 | 4.1 ± 0.34 | <0.0001 |
| Mean Gradient (mm Hg) | 18.7 ± 8.2 | 41 ± 5.6 | <0.0001 |
| AVA (cm2) | 1.4 ± 0.28 | 0.78 ± 0.22 | <0.0001 |
| DVI | 0.46 ± 0.13 | 0.25 ± 0.08 | <0.0001 |
| LVIDD (cm) | 4.72 ± 0.81 | 4.63 ± 0.79 | <0.0001 |
| LVISD (cm) | 3.4 ± 0.58 | 3.2 ± 0.88 | 0.0004 |
| Overall mortality | 907 (41%) | 830 (41.7%) | 0.6530 |
| Risk Factor | Patients with 1-Year Follow-up | Patients with 5-Year Follow-up | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Number | β Coefficient | p-Value | Hazard Ratio | 95% CI | Number | β Coefficient | p-Value | Hazard Ratio | 95% CI | |
| Age * | 3966 | 0.0188 | <0.0001 | 1.02 | 1.016–1.022 | 816 | 0.0237 | <0.0001 | 1.02 | 1.018–1.030 |
| Gender | ||||||||||
| Female | 1866 | ref. | 1.00 | |||||||
| Male | 2100 | 0.0792 | 0.11 | 1.08 | 0.98–1.19 | |||||
| Race/ethnicity | ||||||||||
| Caucasian | 3418 | ref. | 1.00 | 713 | ref. | 1.00 | ||||
| African American | 296 | −0.0788 | 0.41 | 0.92 | 0.77–1.11 | 51 | −0.0053 | 0.98 | 1.00 | 0.69–1.43 |
| Another race | 252 | −0.3039 | 0.0071 | 0.74 | 0.59–0.92 | 52 | −0.4021 | 0.040 | 0.67 | 0.46–0.98 |
| Comorbidity | ||||||||||
| Diabetes mellitus | ||||||||||
| No | 2711 | ref. | 1.00 | 555 | ref. | 1.00 | ||||
| Yes | 1255 | 0.1690 | 0.0018 | 1.18 | 1.07–1.32 | 261 | 0.3677 | 0.0002 | 1.44 | 1.19–1.75 |
| Dyslipidemia | ||||||||||
| No | 1642 | ref. | 1.00 | 335 | ref. | 1.00 | ||||
| Yes | 2324 | −0.1965 | 0.0001 | 0.82 | 0.74–0.91 | 481 | −0.2542 | 0.0092 | 0.78 | 0.64–0.94 |
| Obesity | ||||||||||
| No | 3692 | ref. | 1.00 | |||||||
| Yes | 274 | −0.1599 | 0.14 | 0.85 | 0.69–1.05 | |||||
| CKD | ||||||||||
| No | 3340 | ref. | 1.00 | 693 | ref. | 1.00 | ||||
| Yes | 626 | 0.3828 | <0.0001 | 1.47 | 1.30–1.66 | 123 | 0.4721 | <0.0001 | 1.60 | 1.28–2.01 |
| Stroke | ||||||||||
| No | 3462 | ref. | 1.00 | 696 | ref. | 1.00 | ||||
| Yes | 504 | 0.1899 | 0.0055 | 1.21 | 1.06–1.38 | 120 | 0.2202 | 0.061 | 1.25 | 0.99–1.57 |
| COPD | ||||||||||
| No | 3317 | ref. | 1.00 | 654 | ref. | 1.00 | ||||
| Yes | 649 | 0.3161 | <0.0001 | 1.37 | 1.22–1.55 | 162 | 0.1632 | 0.13 | 1.18 | 0.95–1.46 |
| Heart failure | ||||||||||
| No | 3144 | ref. | 1.00 | 570 | ref. | 1.00 | ||||
| Yes | 822 | 0.2129 | 0.0002 | 1.24 | 1.11–1.38 | 246 | 0.2031 | 0.036 | 1.23 | 1.01–1.48 |
| Hypertension | ||||||||||
| No | 892 | ref. | 1.00 | 183 | ref. | 1.00 | ||||
| Yes | 3074 | −0.1066 | 0.087 | 0.90 | 0.80–1.02 | 633 | −0.3824 | 0.0007 | 0.68 | 0.55–0.85 |
| AS Severity | ||||||||||
| Moderate | 2101 | ref. | 1.00 | 368 | ref. | 1.00 | ||||
| Severe | 1865 | 0.3721 | <0.0001 | 1.45 | 1.30–1.61 | 448 | 0.1889 | 0.076 | 1.21 | 0.98–1.49 |
| Intervention | ||||||||||
| No | 2985 | ref. | 1.00 | 476 | ref. | 1.00 | ||||
| Yes | 981 | −1.3131 | <0.0001 | 0.27 | 0.23–0.31 | 340 | −1.2336 | <0.0001 | 0.29 | 0.23–0.37 |
| Risk Factor | Patients with 1-Year Follow-up | Patients with 5-Year Follow-up | ||
|---|---|---|---|---|
| β Coefficient | Score | β Coefficient | Score | |
| Age | 0.0188 | 0.0237 | ||
| 40–49 | 0 | 0 | ||
| 50–59 | 1 | 1 | ||
| 60–69 | 2 | 2 | ||
| 70–79 | 3 | 3 | ||
| 80–89 | 4 | 4 | ||
| 90–99 | 5 | 5 | ||
| Gender | ||||
| Female | ref. | 0 | ||
| Male | 0.0792 | 4 | ||
| Race/ethnicity | ||||
| Caucasian | ref. | 0 | ref. | 0 |
| African American | −0.0788 | −4 | −0.0053 | 0 |
| Another race | −0.3039 | −16 | −0.4021 | −17 |
| Comorbidity | ||||
| Diabetes mellitus | ||||
| No | ref. | 0 | ref. | 0 |
| Yes | 0.1690 | 9 | 0.3677 | 16 |
| Dyslipidemia | ||||
| No | ref. | 0 | ref. | 0 |
| Yes | −0.1965 | −10 | −0.2542 | −11 |
| Obesity | ||||
| No | ref. | 0 | ||
| Yes | −0.1599 | −9 | ||
| CKD | ||||
| No | ref. | 0 | ref. | 0 |
| Yes | 0.3828 | 20 | 0.4721 | 20 |
| Stroke | ||||
| No | ref. | 0 | ref. | 0 |
| Yes | 0.1899 | 10 | 0.2202 | 9 |
| COPD | ||||
| No | ref. | 0 | ref. | 0 |
| Yes | 0.3161 | 17 | 0.1632 | 7 |
| Heart failure | ||||
| No | ref. | 0 | ref. | 0 |
| Yes | 0.2129 | 11 | 0.2031 | 9 |
| Hypertension | ||||
| No | ref. | 0 | ref. | 0 |
| Yes | −0.1066 | −6 | −0.3824 | −16 |
| AS Severity | ||||
| Moderate | ref. | 0 | ref. | 0 |
| Severe | 0.3721 | 20 | 0.1889 | 8 |
| Intervention | ||||
| No | ref. | 0 | ref. | 0 |
| Yes | −1.3131 | −70 | −1.2336 | −52 |
| Patients with 1-Year Follow-up | Patients with 5-Year Follow-up | ||
|---|---|---|---|
| Total Score | Estimate Risk of 1-Year Mortality | Total Score | Estimate Risk of 5-Year Mortality |
| −111 to −90 | 0.0201–0.0296 | −96 to −90 | 0.0582–0.0668 |
| −89 to −70 | 0.0302–0.0429 | −89 to −70 | 0.0683–0.1050 |
| −69 to −50 | 0.0437–0.0618 | −69 to −50 | 0.1074–0.1633 |
| −49 to −30 | 0.0630–0.0888 | −49 to −30 | 0.1669–0.2490 |
| −29 to −10 | 0.0904–0.1266 | −29 to −10 | 0.2542–0.3688 |
| −9 to 10 | 0.1289–0.1790 | −9 to 10 | 0.3757–0.5224 |
| 11 to 30 | 0.1820–0.2496 | 11 to 30 | 0.5308–0.6949 |
| 31 to 50 | 0.2537–0.3418 | 31 to 50 | 0.7035–0.8515 |
| 51 to 70 | 0.3470–0.4562 | 51 to 70 | 0.8581–0.9533 |
| 71 to 96 | 0.4625–0.6296 | 71 to 74 | 0.9566–0.9656 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yousef, S.; Amabile, A.; Huang, H.; Agarwal, R.; Singh, S.; Ram, C.; Milewski, R.K.; Assi, R.; Zhang, Y.; Krane, M.; et al. One and Five-Year Mortality Risk Prediction in Patients with Moderate and Severe Aortic Stenosis. J. Clin. Med. 2022, 11, 2949. https://doi.org/10.3390/jcm11102949
Yousef S, Amabile A, Huang H, Agarwal R, Singh S, Ram C, Milewski RK, Assi R, Zhang Y, Krane M, et al. One and Five-Year Mortality Risk Prediction in Patients with Moderate and Severe Aortic Stenosis. Journal of Clinical Medicine. 2022; 11(10):2949. https://doi.org/10.3390/jcm11102949
Chicago/Turabian StyleYousef, Sameh, Andrea Amabile, Huang Huang, Ritu Agarwal, Saket Singh, Chirag Ram, Rita K. Milewski, Roland Assi, Yawie Zhang, Markus Krane, and et al. 2022. "One and Five-Year Mortality Risk Prediction in Patients with Moderate and Severe Aortic Stenosis" Journal of Clinical Medicine 11, no. 10: 2949. https://doi.org/10.3390/jcm11102949