
Reliability and Time Efficiency of Digital vs. Analog Bite Registration Technique for the Manufacture of Full-Arch Fixed Implant Prostheses



Abstract
:1. Introduction
2. Materials and Methods
2.1. Design of the Study
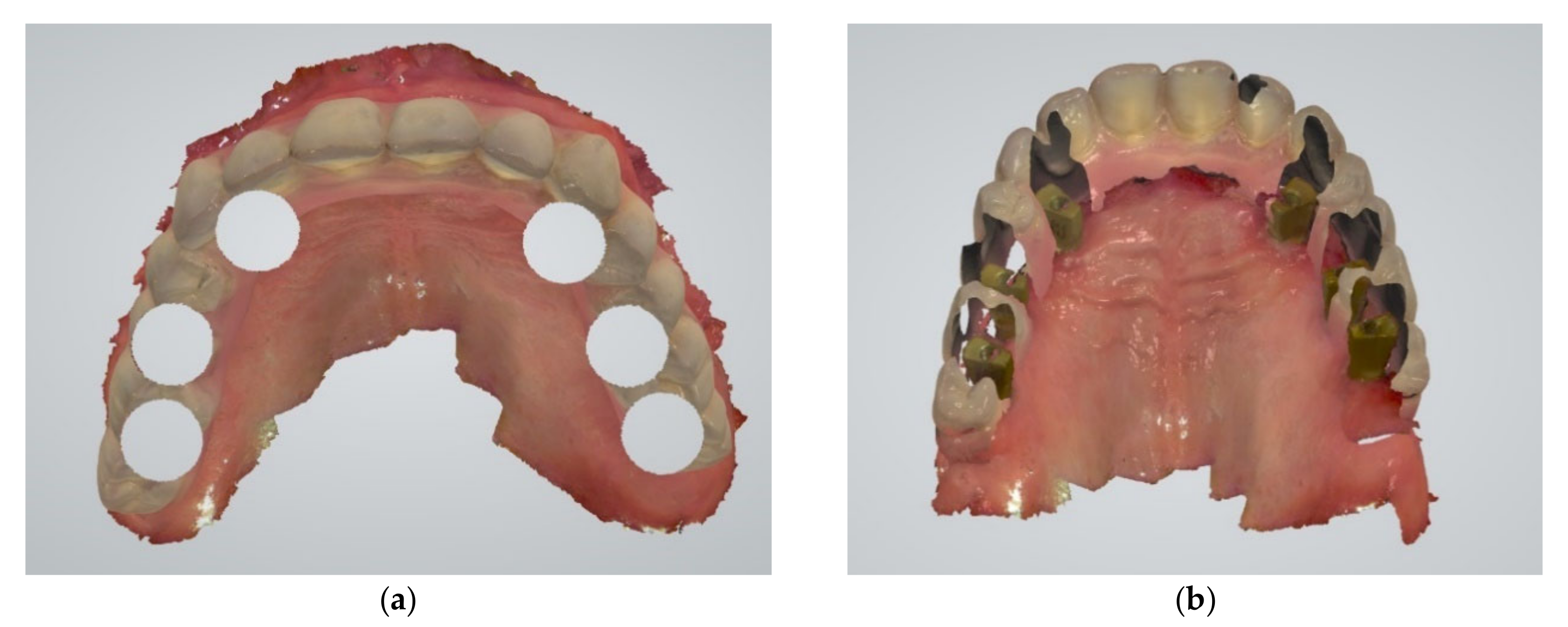
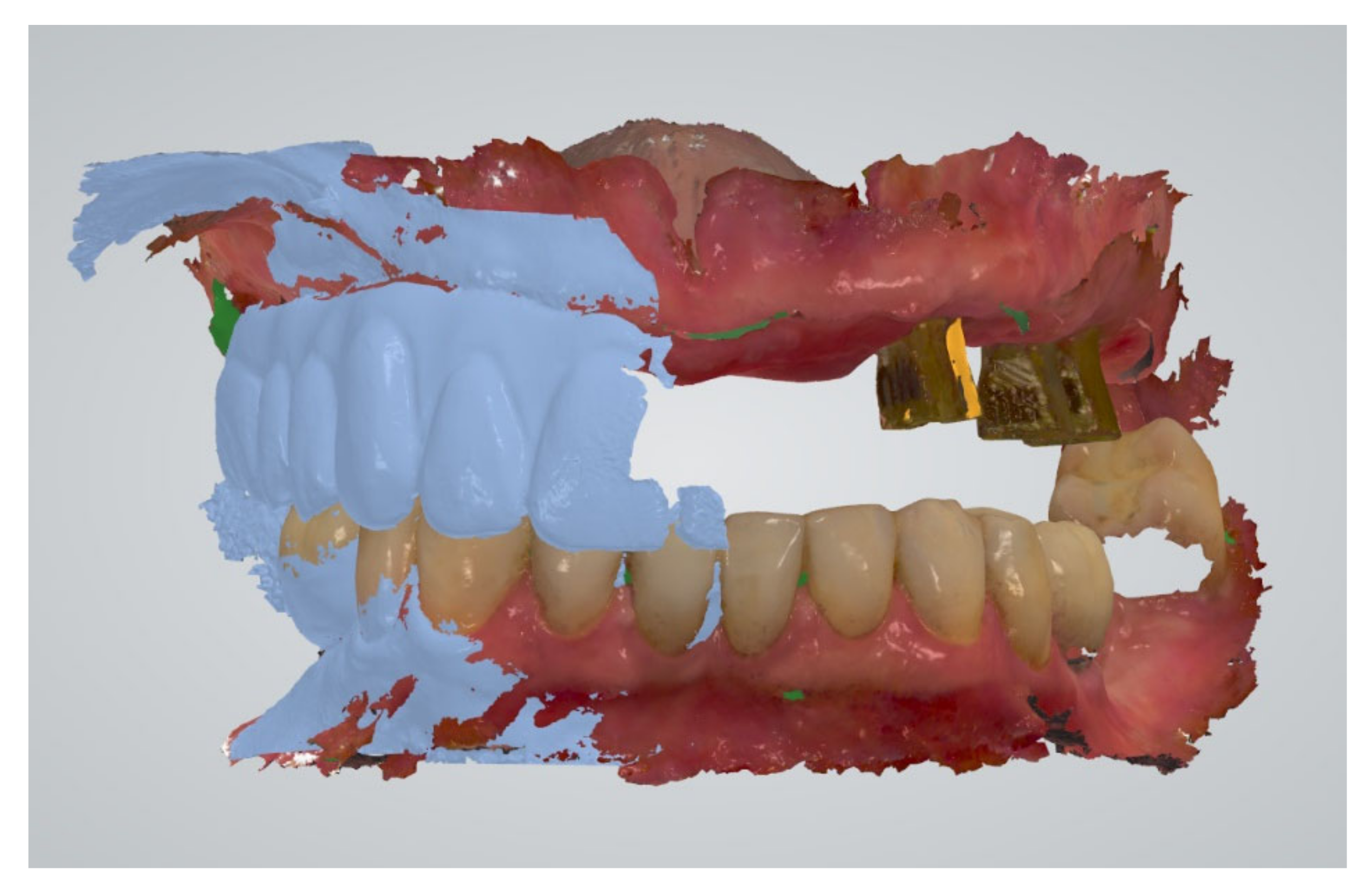
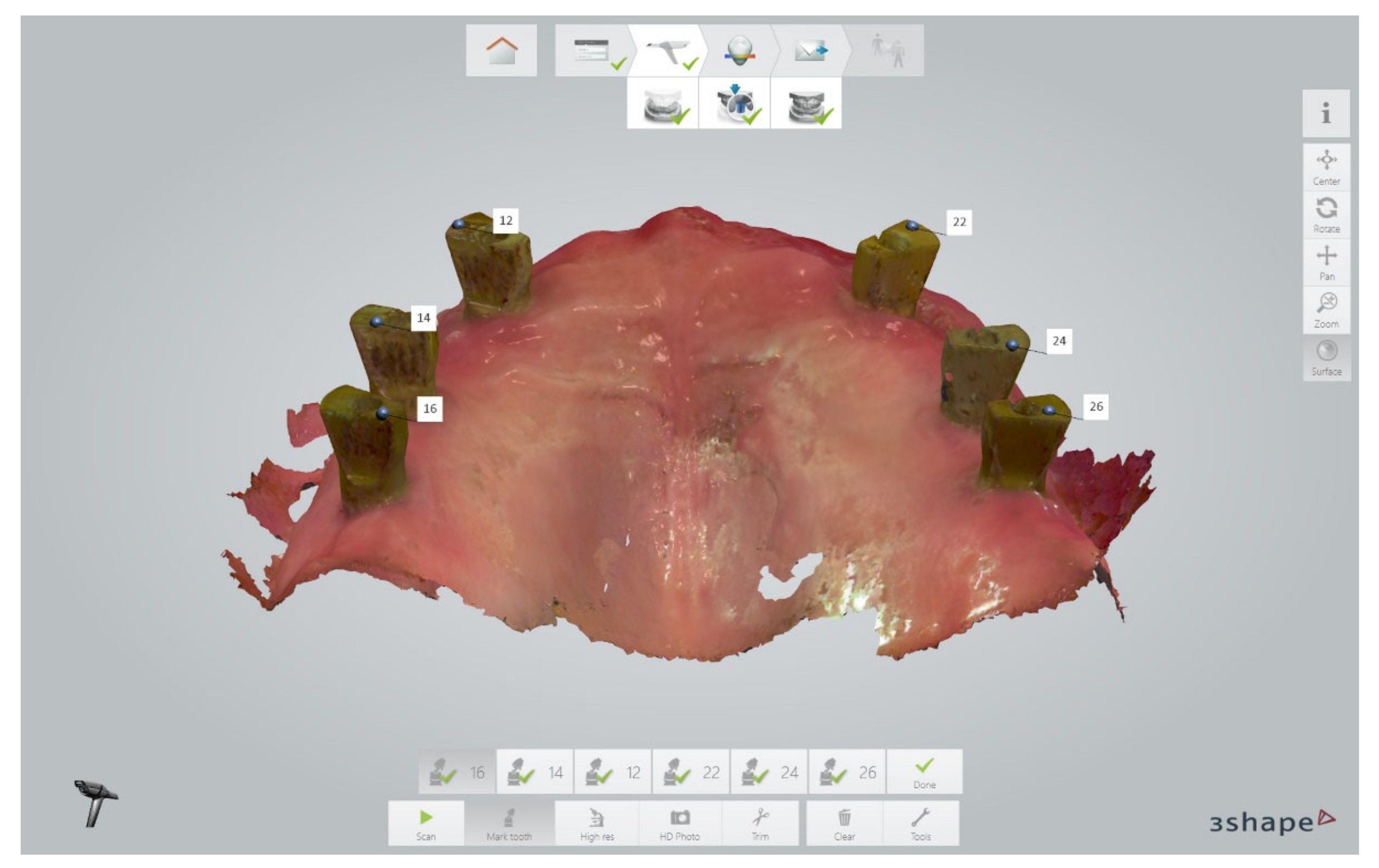
2.2. Data Definition
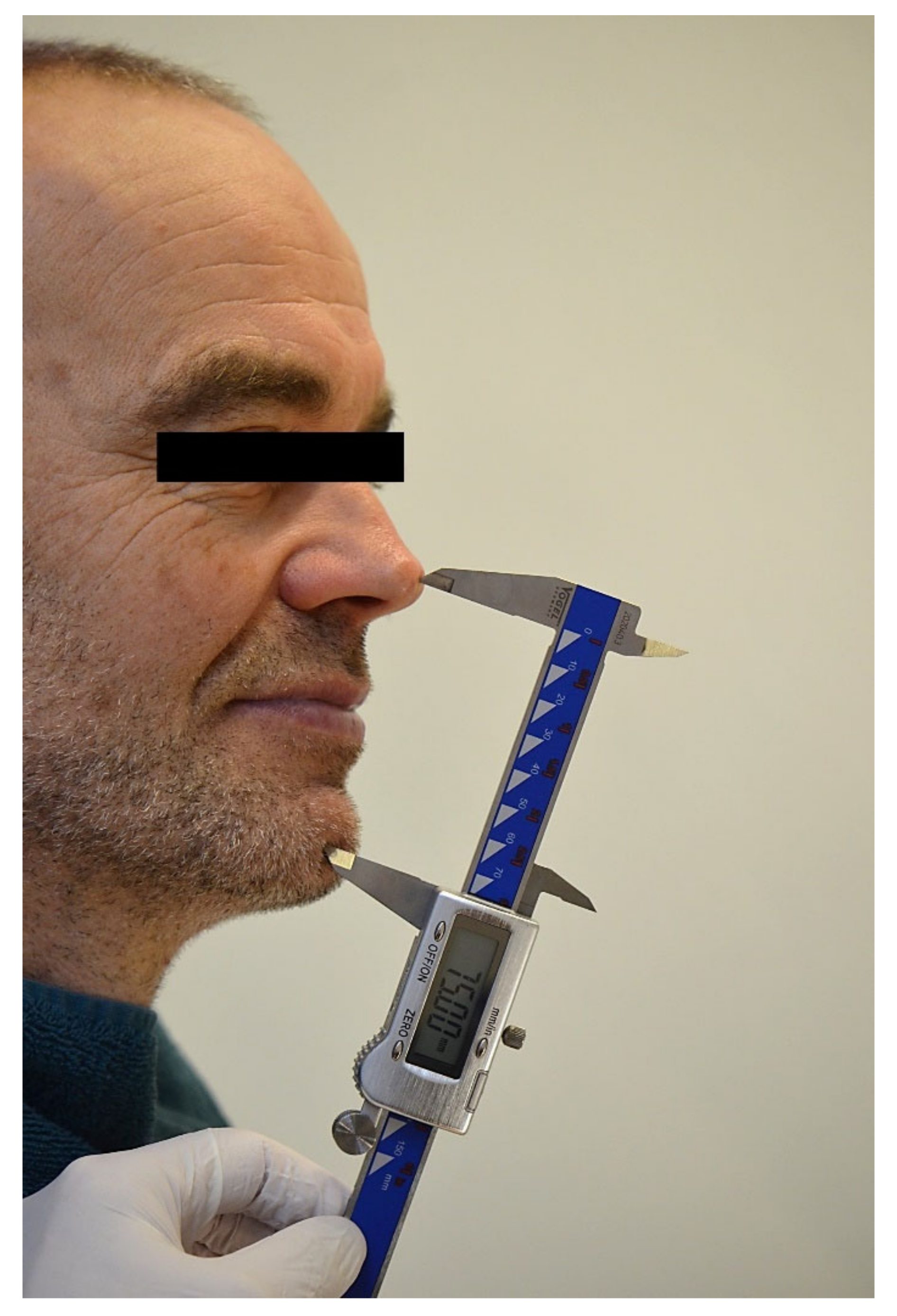
2.3. Linear Measurements
2.4. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
6. Patents
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Needles, J.W. Mandibular Movements and Articulator Design. J. Am. Dent. Assoc. 1923, 10, 927–935. [Google Scholar] [CrossRef]
- Niswonger, M.E. Obtaining the Vertical Relation in Edentulous Cases That Existed Prior to Extraction. J. Am. Dent. Assoc. 1938, 25, 1842–1847. [Google Scholar] [CrossRef]
- Zitzmann, N.U.; Marinello, C.P. Treatment plan for restoring the edentulous maxilla with implant-supported restorations: Removable overdenture versus fixed partial denture design. J. Prosthet. Dent. 1999, 82, 188–196. [Google Scholar] [CrossRef]
- Atwood, D.A. A critique of research of the rest position of the mandible. J. Prosthet. Dent. 1966, 16, 848–854. [Google Scholar] [CrossRef]
- Rugh, J.D.; Drago, C.J. Vertical dimension: A study of clinical rest position and jaw muscle activity. J. Prosthet. Dent. 1981, 45, 670–675. [Google Scholar] [CrossRef]
- Tryde, G.; Stoltze, K.; Fujii, H.; Brill, N. Short-term changes in the perception of comfortable mandibular occlusal positions. J. Oral Rehabil. 1977, 4, 17–21. [Google Scholar] [CrossRef] [PubMed]
- Niswonger, M.E. The Rest Position of the Mandible and the Centric Relation. J. Am. Dent. Assoc. 1934, 21, 1572–1582. [Google Scholar] [CrossRef]
- Wilson, P.H.R.; Banerjee, A. Recording the retruded contact position: A review of clinical techniques. Br. Dent. J. 2004, 196, 395–402. [Google Scholar] [CrossRef] [Green Version]
- Posselt, U. Studies in the mobility of the human mandible. Acta Odontol. Scand. 1952, 10, 19–160. [Google Scholar]
- Ingervall, B. Retruded contact position of the mandible. A comparison between children and adults. Odont. Revy 1964, 15, 130–134. [Google Scholar]
- Kabcenell, J.L. Effect of clinical procedures on mandibular position. J. Prosthet. Dent. 1964, 14, 266–278. [Google Scholar] [CrossRef]
- Hellsing, G.; McWilliam, J.S. Repeatability of the mandibular retruded position. J. Oral Rehabil. 1985, 12, 1–8. [Google Scholar] [CrossRef]
- Schuyler, C.H. Freedom in centric. Dent. Clin. North Am. 1969, 13, 5255322. [Google Scholar] [CrossRef]
- Abbo, B.; Razzoog, M.E. Transferring the existing occlusal vertical dimension using a duplicate denture. J. Prosthet. Dent. 2007, 98, 68–69. [Google Scholar] [CrossRef]
- Clark, W.A.; Duqum, I.; Kowalski, B.J. The digitally replicated denture technique: A case report. J. Esthet. Restor. Dent. 2019, 31, 20–25. [Google Scholar] [CrossRef] [Green Version]
- Michalakis, K.X.; Touloumi, F.; Calvani, L.; Bedi, A.; Hirayama, H. Simplifying Prosthetic Procedures while Converting an Interim Maxillary Removable Complete Denture to an Interim Implant-Supported Fixed Complete Denture. J. Prosthodont. 2011, 20, 408–413. [Google Scholar] [CrossRef]
- Parnia, F.; Moslehifard, E.; Motayagheni, N.; Pournasrollah, A. A time-saving method for transferring occlusal vertical dimension and centric relation of complete denture to a full-arch implant prosthesis. J. Contemp. Dent. Pract. 2014, 15, 672–675. [Google Scholar] [CrossRef]
- Park, D.H.; Park, J.M.; Choi, J.W.; Kang, E.S. Accuracy of several implant bite registration techniques: An in-vitro pilot study. J. Adv. Prosthodont. 2017, 9, 341–349. [Google Scholar] [CrossRef] [Green Version]
- Aprile, H.; Saizar, P. Gothic Arch Tracing and Temporomandibular Anatomy. J. Am. Dent. Assoc. 1947, 35, 256–261. [Google Scholar] [CrossRef]
- Thakur, M.; Jain, V.; Parkash, H.; Kumar, P. A Comparative Evaluation of Static and Functional Methods for Recording Centric Relation and Condylar Guidance: A Clinical Study. J. Indian Prosthodont. Soc. 2012, 12, 175–181. [Google Scholar] [CrossRef]
- Raigrodski, A.J.; Sadan, A.; Carruth, P.L. A Technique to Stabilize Record Bases for Gothic Arch Tracings in Patients with Implant-Retained Complete Dentures. J. Prosthodont. 1998, 7, 273–276. [Google Scholar] [CrossRef] [PubMed]
- Joda, T.; Ferrari, M.; Gallucci, G.O.; Wittneben, J.G.; Bragger, U. Digital technology in fixed implant prosthodontics. Periodontology 2000, 73, 178–192. [Google Scholar] [CrossRef] [PubMed]
- Joda, T.; Brägger, U. Complete digital workflow for the production of implant-supported single-unit monolithic crowns. Clin. Oral Implants Res. 2014, 25, 1304–1306. [Google Scholar] [CrossRef] [PubMed]
- Lepidi, L.; Galli, M.; Mastrangelo, F.; Venezia, P.; Joda, T.; Wang, H.; Li, J. Virtual Articulators and Virtual Mounting Procedures: Where Do We Stand? J. Prosthodont. Dent. 2021, 30, 24–35. [Google Scholar] [CrossRef]
- Lepidi, L.; Chen, Z.; Ravida, A.; Lan, T.; Wang, H.L.; Li, J. A Full-Digital Technique to Mount a Maxillary Arch Scan on a Virtual Articulator. J. Prosthodont. 2019, 28, 335–338. [Google Scholar] [CrossRef]
- Lepidi, L.; Suriano, C.; Wang, H.L.; Granata, S.; Joda, T.; Li, J. Digital fixed complete-arch rehabilitation: From virtual articulator mounting to clinical delivery. J. Prosthet. Dent. 2022, 127, 398–403. [Google Scholar] [CrossRef]
- Hong, S.J.; Choi, Y.; Park, M.; Paek, J.; Pae, A.; Kim, H.S.; Kwon, K.R.; Noh, K. Setting the Sagittal Condylar Inclination on a Virtual Articulator Using Intraoral Scan of Protrusive Interocclusal Position and Cone Beam Computed Tomography. J. Prosthodont. 2020, 29, 185–189. [Google Scholar] [CrossRef]
- Griseto, N.T.; Gallucci, G.O. Digital maxillomandibular relationship registration for an edentulous maxilla: A dental technique. J. Prosthet. Dent. 2021, 125, 858–861. [Google Scholar] [CrossRef]
- Monaco, C.; Ragazzini, N.; Scheda, L.; Evangelisti, E. A fully digital approach to replicate functional and aesthetic parameters in implant-supported full-arch rehabilitation. J. Prosthodont. Res. 2018, 62, 383–385. [Google Scholar] [CrossRef]
- An, X.; Fang, J.H.; Jeong, S.M.; Choi, B.H. A CAD-CAM technique for conversion of interim-to-definitive restoration in patients with complete edentulism. J. Prosthet. Dent. 2018, 120, 190–193. [Google Scholar] [CrossRef]
- Michelinakis, G.; Nikolidakis, D. Using the surgical guide for impression-free digital bite registration in the edentulous maxilla—a technical note. Int. J. Implant. Dent. 2019, 5, 19. [Google Scholar] [CrossRef]
- Ahmed, W.M.; Verhaeghe, T.V.; Mccullagh, A. Maxillary complete-arch implant-supported restoration: A digital scanning and hence- mandibular relationship workflow. J. Prosthet. Dent. 2021, 125, 216–220. [Google Scholar] [CrossRef]
- Shao, J.; Qing, H.; Zhu, Z.; Li, L. CAD-CAM–fabricated interim fixed complete-arch implant-supported restorations based on the existing dentition. J. Prosthet. Dent. 2019, 121, 717–723. [Google Scholar] [CrossRef]
- Papaspyridakos, P.; Chen, Y.W.; Gonzalez-Gusmao, I.; Att, W. Complete digital workflow in prosthesis prototype manufacture for complete-arch implant rehabilitation: A technique. J. Prosthet. Dent. 2019, 122, 189–192. [Google Scholar] [CrossRef]
- Espona, J.; Roig, E.; Ali, A.; Roig, M. Immediately loaded interim complete-arch implant-supported fixed dental prostheses fabricated with a completely digital workflow: A clinical technique. J. Prosthet. Dent. 2020, 124, 423–427. [Google Scholar] [CrossRef]
- Kim, J.E.; Amelya, A.; Shin, Y.; Shim, J.S. Accuracy of intraoral digital impressions using an artificial landmark. J. Prosthet. Dent. 2017, 117, 755–761. [Google Scholar] [CrossRef]
- Cappare, P.; Sannino, G.; Minoli, M.; Montemezzi, P.; Ferrini, F. Conventional versus Digital Impressions for Full Arch Screw-Retained Maxillary Rehabilitations: A Randomized Clinical Trial. Int. J. Environ. Res. Public Health. 2019, 16, 829. [Google Scholar] [CrossRef] [Green Version]
- Rutkunas, V.; Gedrimiene, A.; Akulauskas, M.; Fehmer, V.; Sailer, I.; Jegelevicius, D. In vitro and in vivo accuracy of full-arch digital implant impressions. Clin. Oral Implants Res. 2021, 32, 1444–1454. [Google Scholar] [CrossRef]
- Schimmel, M.; Akino, N.; Srinivasan, M.; Wittneben, J.G.; Yilmaz, B.; Abou-Ayash, S. Accuracy of intraoral scanning in completely and partially edentulous maxillary and mandibular jaws: An in vitro analysis. Clin. Oral Investig. 2021, 25, 1839–1847. [Google Scholar] [CrossRef]
- Albayrak, B.; Sukotjo, C.; Wee, A.G.; Korkmaz, İ.H.; Bayındır, F. Three-Dimensional Accuracy of Conventional Versus Digital Complete Arch Implant Impressions. J. Prosthodont. 2021, 30, 163–170. [Google Scholar] [CrossRef]
- Knechtle, N.; Wiedemeier, D.; Mehl, A.; Ender, A. Accuracy of digital complete-arch, multi-implant scans made in the edentulous jaw with gingival movement simulation: An in vitro study. J. Prosthet. Dent. 2021. [Google Scholar] [CrossRef]
- Baghani, M.T.; Shayegh, S.S.; Johnston, W.M.; Shidfar, S.; Hakimaneh, S.M.R. In vitro evaluation of the accuracy and precision of intraoral and extraoral complete-arch scans. J. Prosthet. Dent. 2021, 126, 665–670. [Google Scholar] [CrossRef]
- Pesce, P.; Pera, F.; Setti, P.; Menini, M. Precision and Accuracy of a Digital Impression Scanner in Full-Arch Implant Rehabilitation. Int. J. Prosthodont. 2018, 31, 171–175. [Google Scholar] [CrossRef]
- Wong, K.Y.; Esguerra, R.J.; Chia, V.A.P.; Tan, Y.H.; Tan, K.B.C. Three-Dimensional Accuracy of Digital Static Interocclusal Registration by Three Intraoral Scanner Systems. J. Prosthodont. 2018, 27, 120–128. [Google Scholar] [CrossRef]
- D’haese, R.; Vrombaut, T.; Roeykens, H.; Vandeweghe, S. In Vitro Accuracy of Digital and Conventional Impressions for Full-Arch Implant-Supported Prostheses. J. Clin. Med. 2021, 11, 594. [Google Scholar] [CrossRef]
- Abdulateef, S.; Edher, F.; Hannam, A.G.; Tobias, D.L.; Wyatt, C.C.L. Clinical accuracy and reproducibility of virtual interocclusal records. J. Prosthet. Dent. 2020, 124, 667–673. [Google Scholar] [CrossRef]
- Zimmermann, M.; Ender, A.; Attin, T.; Mehl, A. Accuracy of Buccal Scan Procedures for the Registration of Habitual Intercuspation. Oper Dent. 2018, 43, 573–580. [Google Scholar] [CrossRef]
- Solaberrieta, E.; Otegi, J.R.; Goicoechea, N.; Brizuela, A.; Pradies, G. Comparison of a conventional and virtual occlusal record. J. Prosthet. Dent. 2015, 114, 92–97. [Google Scholar] [CrossRef]
- Camcı, H.; Salmanpour, F. A new technique for testing accuracy and sensitivity of digital bite registration: A prospective comparative study. Int. Orthod. 2021, 19, 425–432. [Google Scholar] [CrossRef]
- Kattadiyil, M.T.; Alzaid, A.A.; Campbell, S.D. What Materials and Reproducible Techniques May Be Used in Recording Centric Relation? Best Evidence Consensus Statement. J. Prosthodont. 2021, 30 (Suppl. 1), 34–42. [Google Scholar] [CrossRef]
- Ren, S.; Morton, D.; Lin, W.S. Accuracy of virtual interocclusal records for partially edentulous patients. J. Prosthet. Dent. 2020, 123, 860–865. [Google Scholar] [CrossRef] [PubMed]
- Eriksson, A.; Ockert-Eriksson, G.; Lockowandt, P.; Eriksson, O. Clinical factors and clinical variation influencing the reproducibility of interocclusal recording methods. Br. Dent. J. 2002, 192, 395–400. [Google Scholar] [CrossRef] [PubMed]
- Edher, F.; Hannam, A.G.; Tobias, D.L.; Wyatt, C.C.L. The accuracy of virtual interocclusal registration during intraoral scanning. J. Prosthet. Dent. 2018, 120, 904–912. [Google Scholar] [CrossRef] [PubMed]
- Gintaute, A.; Keeling, A.J.; Osnes, C.A.; Zitzmann, N.U.; Ferrari, M.; Joda, T. Precision of maxillo-mandibular registration with intraoral scanners in vitro. J. Prosthodont. Res. 2020, 64, 114–119. [Google Scholar] [CrossRef]
- Resende, C.; Barbosa, T.; Moura, G.F.; Tavares, L.; Rizzante, F.; George, F.M.; Neves, F.; Mendonça, G. Influence of operator experience, scanner type, and scan size on 3D scans. J. Prosthet. Dent. 2021, 125, 294–299. [Google Scholar] [CrossRef]
- Róth, I.; Czigola, A.; Joós-Kovács, G.L.; Dalos, M.; Hermann, P.; Borbély, J. Learning curve of digital intraoral scanning—An in vivo study. BMC Oral Health 2020, 20, 287. [Google Scholar] [CrossRef]
- Al Hamad, K.Q. Learning curve of intraoral scanning by prosthodontic residents. J. Prosthet. Dent. 2020, 123, 277–283. [Google Scholar] [CrossRef]
- Michelinakis, G.; Apostolakis, D.; Kamposiora, P.; Papavasiliou, G.; Özcan, M. The direct digital workflow in fixed implant prosthodontics: A narrative review. BMC Oral Health 2021, 21, 37. [Google Scholar] [CrossRef]
- Gimenez-Gonzalez, B.; Hassan, B.; Özcan, M.; Pradíes, G. An In Vitro Study of Factors Influencing the Performance of Digital Intraoral Impressions Operating on Active Wavefront Sampling Technology with Multiple Implants in the Edentulous Maxilla. J. Prosthodont. 2017, 26, 650–655. [Google Scholar] [CrossRef]
- Rutkūnas, V.; Gečiauskaitė, A.; Jegelevičius, D.; Vaitiekūnas, M. Accuracy of digital implant impressions with intraoral scanners. A systematic review. Eur. J. Oral Implantol. 2017, 10 (Suppl. 1), 101–121. [Google Scholar]
- Nuytens, P. Scan Post, Bite Pillar, Reference Pillar and Related Methods for Recording Dental Implant Position. US Patent 20190223990, 3 October 2017. [Google Scholar]

















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Mean (µm) | Standard Deviation (µm) | Minimum (µm) | Maximum (µm) | 95.0% Lower CL for Mean (µm) | 95.0% Upper CL for Mean (µm) | p Value | |
|---|---|---|---|---|---|---|---|
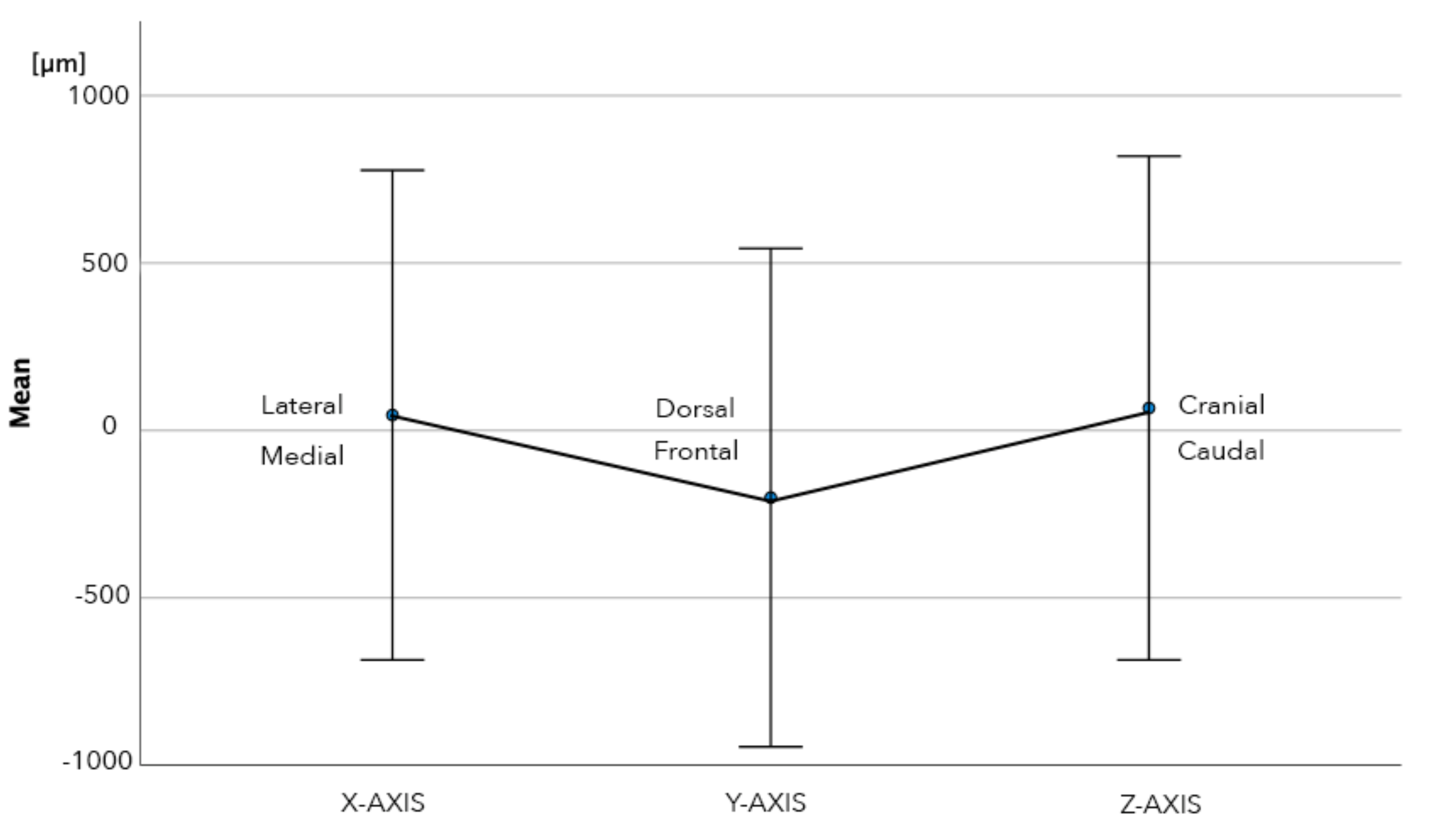
| Y-axis | 200 | 744 | −2.361 | 1.376 | −348 | −53 | 0.008 |
| Z-Axis | 67 | 752 | −1.660 | 1.269 | −82 | 216 | 0.374 |
| X-axis | 46 | 731 | −2.271 | 2.135 | −99 | 191 | 0.529 |
| Absolute Y-axis | 611 | 470 | 10 | 2360 | 518 | 700 | 0.001 |
| Absolute Z-Axis | 630 | 410 | 10 | 1660 | 552 | 710 | 0.001 |
| Absolute X-axis | 470 | 560 | 10 | 2270 | 364 | 580 | 0.001 |
| Distance3D | 1115 | 668 | 150 | 3160 | 980 | 1246 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nuytens, P.; D’haese, R.; Vandeweghe, S. Reliability and Time Efficiency of Digital vs. Analog Bite Registration Technique for the Manufacture of Full-Arch Fixed Implant Prostheses. J. Clin. Med. 2022, 11, 2882. https://doi.org/10.3390/jcm11102882
Nuytens P, D’haese R, Vandeweghe S. Reliability and Time Efficiency of Digital vs. Analog Bite Registration Technique for the Manufacture of Full-Arch Fixed Implant Prostheses. Journal of Clinical Medicine. 2022; 11(10):2882. https://doi.org/10.3390/jcm11102882
Chicago/Turabian StyleNuytens, Philippe, Rani D’haese, and Stefan Vandeweghe. 2022. "Reliability and Time Efficiency of Digital vs. Analog Bite Registration Technique for the Manufacture of Full-Arch Fixed Implant Prostheses" Journal of Clinical Medicine 11, no. 10: 2882. https://doi.org/10.3390/jcm11102882