
Sex-Specific Difference in the Effect of Altitude on Sleep and Nocturnal Breathing in Young Healthy Volunteers
Abstract
:1. Introduction
2. Material and Methods
2.1. Participants
2.2. Study Design and Setting
2.3. Measurements
2.3.1. Clinical Examination and Questionnaires
2.3.2. Sleep Studies
2.3.3. Daytime Evaluation
2.3.4. Blood Tests
2.4. Outcomes
2.5. Statistical Analysis
3. Results
3.1. Participants
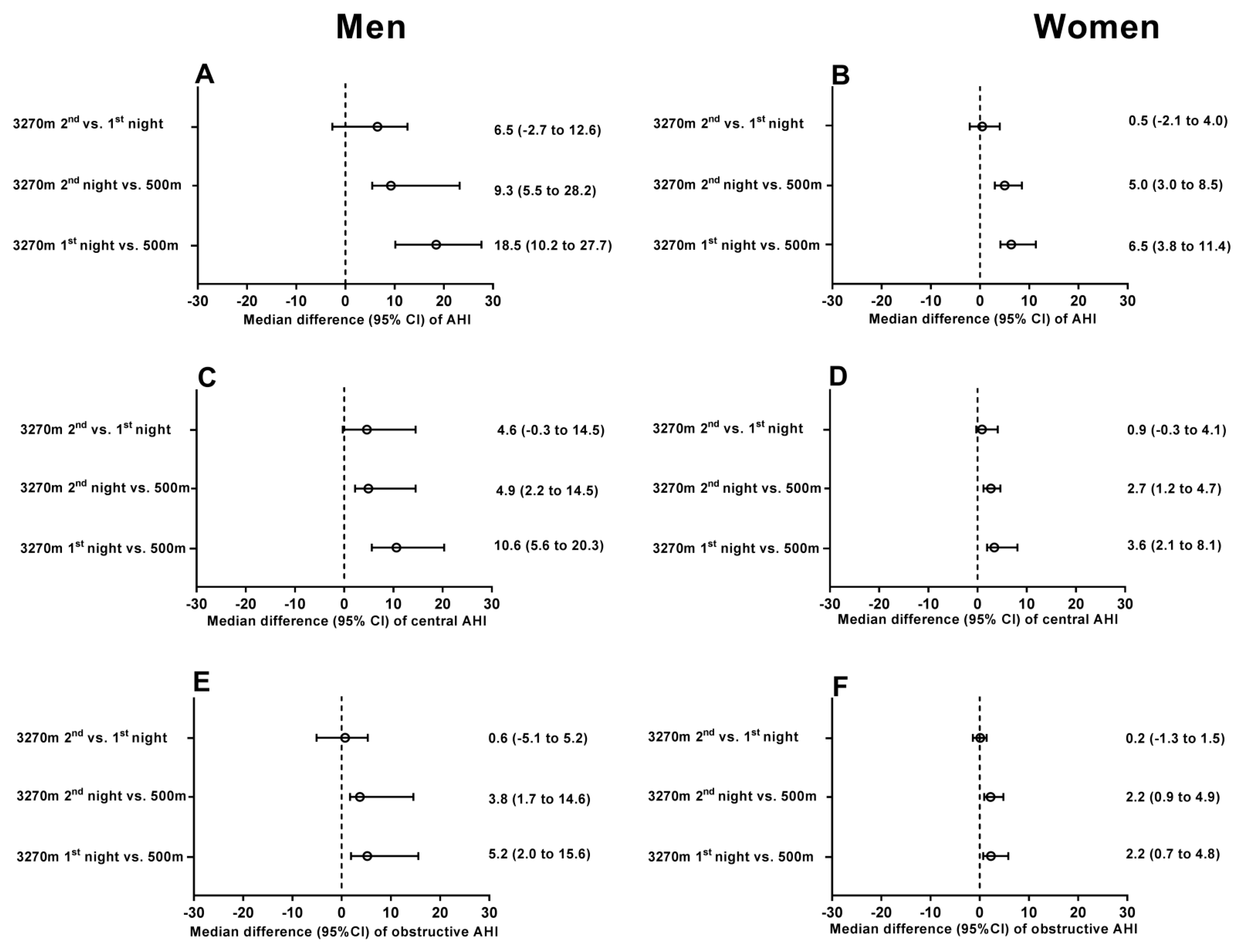
3.2. Respiratory Events, Oxygen Saturations, Heart Rate and Blood Pressure
3.3. Clinical and Daytime Evaluations
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| AHI | Apnea–hypopnea index |
| AMS | Acute mountain sickness |
| BMI | Body mass index |
| CSA | Central sleep apnea |
| ESS | Epworth sleepiness scale |
| FEV1 | Forced expiratory volume in the first second of expiration |
| FVC | Forced vital capacity |
| GAD-7 | 7-item generalized anxiety disorder scale |
| OSA | Obstructive sleep apnea |
| PHQ-9 | 9-item patient health questionnaire |
| PSG | Polysomnography |
| PSQI | Pittsburgh sleep quality index |
| PVT | Psychomotor vigilance test |
| SDB | Sleep-disordered breathing |
References
- Rio-Rama, M.; Maldonado-Erazo, C.; Durán-Sánchez, A.; Alvarez-Garcia, J. Mountain tourism research: A review. Eur. J. Tour. Res. 2019, 22, 130–150. [Google Scholar] [CrossRef]
- Mohd Taher, S.H.; Jamal, S.A.; Sumarjan, N.; Aminudin, N. Examining the structural relations among hikers assessment of pull-factors, satisfaction and revisit intentions: The case of mountain tourism in Malaysia. J. Outdoor Recreat. Tour. 2015, 12, 82–88. [Google Scholar] [CrossRef]
- Villca, N.; Asturizaga, A.; Heath-Freudenthal, A. High-altitude Illnesses and Air Travel: Pediatric Considerations. Pediatr. Clin. N. Am. 2021, 68, 305–319. [Google Scholar] [CrossRef]
- Bloch, K.E.; Buenzli, J.C.; Latshang, T.D.; Ulrich, S. Sleep at high altitude: Guesses and facts. J. Appl. Physiol. 2015, 119, 1466–1480. [Google Scholar] [CrossRef]
- Latshang, T.D.; Cascio, C.M.L.; Stöwhas, A.-C.; Grimm, M.; Stadelmann, K.; Tesler, N.; Achermann, P.; Huber, R.; Kohler, M.; Bloch, K.E. Are Nocturnal Breathing, Sleep, and Cognitive Performance Impaired at Moderate Altitude (1630–2590 m)? Sleep 2013, 36, 1969–1976. [Google Scholar] [CrossRef]
- Luks, A.M.; Swenson, E.R.; Bärtsch, P. Acute high-altitude sickness. Eur. Respir. Rev. 2017, 26, 160096. [Google Scholar] [CrossRef]
- Meier, D.; Collet, T.H.; Locatelli, I.; Cornuz, J.; Kayser, B.; Simel, D.L.; Sartori, C. Does this patient have acute mountain sickness? The rational clinical examination systematic review. JAMA 2017, 318, 1810–1819. [Google Scholar] [CrossRef] [Green Version]
- Tesler, N.; Latshang, T.D.; Cascio, C.M.L.; Stadelmann, K.; Stoewhas, A.-C.; Kohler, M.; Bloch, K.E.; Achermann, P.; Huber, R. Ascent to moderate altitude impairs overnight memory improvements. Physiol. Behav. 2015, 139, 121–126. [Google Scholar] [CrossRef]
- Bloch, K.E.; Latshang, T.D.; Turk, A.J.; Hess, T.; Hefti, U.; Merz, T.; Bosch, M.M.; Barthelmes, D.; Hefti, J.P.; Maggiorini, M.; et al. Nocturnal Periodic Breathing during Acclimatization at Very High Altitude at Mount Muztagh Ata (7546 m). Am. J. Respir. Crit. Care Med. 2010, 182, 562–568. [Google Scholar] [CrossRef]
- Torlasco, C.; Bilo, G.; Giuliano, A.; Soranna, D.; Ravaro, S.; Oliverio, G.; Faini, A.; Zambon, A.; Lombardi, C.; Parati, G. Effects of acute exposure to moderate altitude on blood pressure and sleep breathing patterns. Int. J. Cardiol. 2020, 301, 173–179. [Google Scholar] [CrossRef]
- Nussbaumer-Ochsner, Y.; Ursprung, J.; Siebenmann, C.; Maggiorini, M.; Bloch, K.E. Effect of Short-Term Acclimatization to High Altitude on Sleep and Nocturnal Breathing. Sleep 2012, 35, 419–423. [Google Scholar] [CrossRef] [Green Version]
- Senaratna, C.V.; Perret, J.L.; Lodge, C.J.; Lowe, A.J.; Campbell, B.E.; Matheson, M.C.; Hamilton, G.S.; Dharmage, S.C. Prevalence of obstructive sleep apnea in the general population: A systematic review. Sleep Med. Rev. 2017, 34, 70–81. [Google Scholar] [CrossRef]
- Bonsignore, M.R.; Saaresranta, T.; Riha, R.L. Sex differences in obstructive sleep apnoea. Eur Respir Rev. 2019, 28, 190030. [Google Scholar]
- Latshang, T.D.; Nussbaumer-Ochsner, Y.; Henn, R.M.; Ulrich, S.; Cascio, C.M.L.; Ledergerber, B.; Kohler, M.; Bloch, K.E. Effect of acetazolamide and autoCPAP therapy on breathing disturbances among patients with obstructive sleep apnea syndrome who travel to altitude: A randomized controlled trial. JAMA 2012, 308, 2390–2398. [Google Scholar] [CrossRef] [Green Version]
- Nussbaumer-Ochsner, Y.; Schuepfer, N.; Ulrich, S.; Bloch, K.E. Exacerbation of sleep apnoea by frequent central events in patients with the obstructive sleep apnoea syndrome at altitude: A randomised trial. Thorax 2010, 65, 429–435. [Google Scholar] [CrossRef] [Green Version]
- Patiño, M.C.; Florez, S.J.B.; Gallo, L.; Ortiz, P.A.; Payán-Gómez, C.; Molano-Gonzalez, N.; Rodríguez, J.H. Gender and Polysomnographic Profiles Findings in Obstructive Sleep Apnea Syndrome Patients Living in High Altitude. Nat. Sci. Sleep 2021, 13, 547–556. [Google Scholar] [CrossRef]
- Erba, P.; Anastasi, S.; Senn, O.; Maggiorini, M.; Bloch, K. Acute mountain sickness is related to nocturnal hypoxemia but not to hypoventilation. Eur. Respir. J. 2004, 24, 303–308. [Google Scholar] [CrossRef] [Green Version]
- Nussbaumer-Ochsner, Y.; Schuepfer, N.; Ursprung, J.; Siebenmann, C.; Maggiorini, M.; Bloch, K.E. Sleep and Breathing in High Altitude Pulmonary Edema Susceptible Subjects at 4559 Meters. Sleep 2012, 35, 1413–1421. [Google Scholar] [CrossRef] [Green Version]
- Caravita, S.; Faini, A.; Lombardi, C.; Valentini, M.; Gregorini, F.; Rossi, J.; Meriggi, P.; Di Rienzo, M.; Bilo, G.; Agostoni, P.; et al. Sex and Acetazolamide Effects on Chemoreflex and Periodic Breathing During Sleep at Altitude. Chest 2015, 147, 120–131. [Google Scholar] [CrossRef]
- Bartsch, P.; Swenson, E.R. Clinical practice: Acute high-altitude illnesses. N. Engl. J. Med. 2013, 368, 2294–2302. [Google Scholar] [CrossRef]
- Santantonio, M.; Chapplain, J.-M.; Tattevin, P.; Leroy, H.; Mener, E.; Gangneux, J.-P.; Michelet, C.; Revest, M. Prevalence of and risk factors for acute mountain sickness among a cohort of high-altitude travellers who received pre-travel counselling. Travel Med. Infect. Dis. 2014, 12, 534–540. [Google Scholar] [CrossRef] [PubMed]
- McDevitt, M.; McIntosh, S.E.; Rodway, G.; Peelay, J.; Adams, D.L.; Kayser, B. Risk Determinants of Acute Mountain Sickness in Trekkers in the Nepali Himalaya: A 24-Year Follow-Up. Wilderness Environ. Med. 2014, 25, 152–159. [Google Scholar] [CrossRef] [PubMed]
- Vardy, J.; Vardy, J.; Judge, K. Acute mountain sickness and ascent rates in trekkers above 2500 m in the Nepali Himalaya. Aviat. Space Environ. Med. 2006, 77, 742–744. [Google Scholar] [PubMed]
- Hou, Y.-P.; Wu, J.-L.; Tan, C.; Chen, Y.; Guo, R.; Luo, Y.-J. Sex-based differences in the prevalence of acute mountain sickness: A meta-analysis. Mil. Med. Res. 2019, 6, 38. [Google Scholar] [CrossRef] [PubMed]
- Roach, R.; Hackett, P.H.; Oelz, O.; Bärtsch, P.; Luks, A.M.; MacInnis, M.; Baillie, J.K.; Achatz, E.; Albert, E.; Andrews, J.; et al. The 2018 Lake Louise Acute Mountain Sickness Score. High Alt. Med. Biol. 2018, 19, 4–6. [Google Scholar] [CrossRef]
- Chen, N.; Johns, M.W.; Li, H.; Chu, C.; Liang, S.; Shu, Y.; Chuang, M.; Wang, P. Validation of a Chinese version of the Epworth sleepiness scale. Qual. Life Res. 2002, 11, 817–821. [Google Scholar] [CrossRef]
- Buysse, D.J.; Reynolds, C.F., 3rd; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh Sleep Quality Index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Gong, Y.; Zhou, H.; Zhang, Y.; Zhu, X.; Wang, X.; Shen, B.; Xian, J.; Ding, Y. Validation of the 7-item Generalized Anxiety Disorder scale (GAD-7) as a screening tool for anxiety among pregnant Chinese women. J. Affect. Disord. 2020, 282, 98–103. [Google Scholar] [CrossRef]
- Wang, W.; Bian, Q.; Zhao, Y.; Li, X.; Wang, W.; Du, J.; Zhang, G.; Zhou, Q.; Zhao, M. Reliability and validity of the Chinese version of the Patient Health Questionnaire (PHQ-9) in the general population. Gen. Hosp. Psychiatry 2014, 36, 539–544. [Google Scholar] [CrossRef]
- Yu, J.L.; Rosen, I. Utility of the modified Mallampati grade and Friedman tongue position in the assessment of obstructive sleep apnea. J. Clin. Sleep Med. 2020, 16, 303–308. [Google Scholar] [CrossRef]
- Miller, M.R.; Hankinson, J.; Brusasco, V.; Burgos, F.; Casaburi, R.; Coates, A.; Crapo, R.; Enright, P.; Van Der Grinten, C.P.M.; Gustafsson, P.; et al. Standardisation of spirometry. Eur. Respir. J. 2005, 26, 319–338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berry, R.B.; Budhiraja, R.; Gottlieb, D.J.; Gozal, D.; Iber, C.; Kapur, V.K.; Marcus, C.L.; Mehra, R.; Parthasarathy, S.; Quan, S.F.; et al. Rules for Scoring Respiratory Events in Sleep: Update of the 2007 AASM Manual for the Scoring of Sleep and Associated Events. Deliberations of the Sleep Apnea Definitions Task Force of the American Academy of Sleep Medicine. J. Clin. Sleep Med. 2012, 8, 597–619. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tan, L.; Li, T.; Zhang, Y.; He, D.; Luo, L.; Lei, F.; Ren, R.; He, J.; Bloch, K.E.; Tang, X. Effect of one night of nocturnal oxygen supplementation on highland patients with OSA: A randomized, crossover trial. Chest 2021, 160, 690–700. [Google Scholar] [CrossRef] [PubMed]
- Tang, X.-G.; Wen, J.; Zhang, X.-S.; Jiang, D.-C. Association between decreased osteopontin and acute mountain sickness upon rapid ascent to 3500 m among young Chinese men. J. Travel Med. 2018, 25, tay075. [Google Scholar] [CrossRef] [Green Version]
- Basner, M.; Dinges, D.F. Maximizing Sensitivity of the Psychomotor Vigilance Test (PVT) to Sleep Loss. Sleep 2011, 34, 581–591. [Google Scholar] [CrossRef] [PubMed]
- Tseng, C.-H.; Lin, F.-C.; Chao, H.-S.; Tsai, H.-C.; Shiao, G.-M.; Chang, S.-C. Impact of rapid ascent to high altitude on sleep. Sleep Breath. 2015, 19, 819–826. [Google Scholar] [CrossRef] [PubMed]
- Lombardi, C.; Meriggi, P.; Agostoni, P.; Faini, A.; Bilo, G.; Revera, M.; Caldara, G.; Di Rienzo, M.; Castiglioni, P.; Maurizio, B.; et al. High-altitude hypoxia and periodic breathing during sleep: Gender-related differences. J. Sleep Res. 2013, 22, 322–330. [Google Scholar] [CrossRef]
- Morelli, C.; Badr, M.S.; Mateika, J.H. Ventilatory responses to carbon dioxide at low and high levels of oxygen are elevated after episodic hypoxia in men compared with women. J. Appl. Physiol. 2004, 97, 1673–1680. [Google Scholar] [CrossRef] [Green Version]
- Whittle, A.T.; Marshall, I.; Mortimore, I.L.; Wraith, P.K.; Sellar, R.J.; Douglas, N.J. Neck soft tissue and fat distribution: Comparison between normal men and women by magnetic resonance imaging. Thorax 1999, 54, 323–328. [Google Scholar] [CrossRef] [Green Version]
- Ma, M.A.; Kumar, R.; Macey, P.M.; Yan-Go, F.L.; Harper, R.M. Epiglottis cross-sectional area and oropharyngeal airway length in male and female obstructive sleep apnea patients. Nat. Sci. Sleep 2016, 8, 297–304. [Google Scholar] [CrossRef] [Green Version]
- Zhou, X.S.; Shahabuddin, S.; Zahn, B.R.; Babcock, M.A.; Badr, M.S. Effect of gender on the development of hypocapnic apnea/hypopnea during NREM sleep. J. Appl. Physiol. 2000, 89, 192–199. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Men (n = 10) | Women (n = 18) | p Value | |
|---|---|---|---|
| Numbers | 10 | 18 | |
| Age, y | 27.5 (24.8, 29.5) | 26.0 (24.3, 27.0) | 0.245 |
| BMI, kg/m2 | 23.3 (20.6, 26.7) | 21.3 (20.0, 24.5) | 0.356 |
| Neck circumference, cm | 36.5 (35.5, 38.3) | 31.5 (30.8, 32.9) | <0.001 |
| Waist circumference, cm | 84.0 (78.5, 93.5) | 71.8 (69.0, 82.8) | 0.020 |
| Hip circumference, cm | 101.0 (93.8, 106.5) | 92.0 (90.0, 93.3) | 0.010 |
| Tonsil hypertrophy, n (%) | 1 (10.0) | 2 (11.1) | 0.716 |
| Tongue hypertrophy, n (%) | 2 (20.0) | 2 (11.1) | 0.452 |
| Mallampati score | 0.826 | ||
| Class IV, n (%) | 0 | 0 | |
| Class III, n (%) | 1 (10.0) | 1 (5.6) | |
| Class II, n (%) | 1 (10.0) | 3 (16.7) | |
| Class I, n (%) | 8 (80.0) | 14 (77.8) | |
| FEV1, L | 3.8 (3.4, 4.2) | 3.0 (2.9, 3.3) | 0.002 |
| FEV1, % predicted | 98 (92, 101) | 105 (95, 108) | 0.106 |
| FVC, L | 4.8 (3.7, 5.0) | 3.5 (3.1, 3.7) | 0.011 |
| FVC, % predicted | 98 (90, 113) | 101 (97, 109) | 0.787 |
| FEV1/FVC | 82.1 (76.2, 86.2) | 86.0 (82.8, 94.2) | 0.106 |
| ESS | 5.5 (3.8, 9.3) | 5.5 (2.0, 8.8) | 0.494 |
| PSQI | 2.5 (0.5, 4.0) | 2.5 (1.8, 4.0) | 0.834 |
| GAD-7 | 0.5 (0, 4.8) | 1.0 (0.8, 2.5) | 0.697 |
| PHQ-9 | 2.0 (1.0, 6.8) | 4.0 (0.8, 6.0) | 0.976 |
| Men | Women | |||||||
|---|---|---|---|---|---|---|---|---|
| 500 m | 3270 m 1st Night | 3270 m 2nd Night | ANOVA, p Value | 500 m | 3270 m 1st Night | 3270 m 2nd Night | ANOVA, p Value | |
| Sleep Breathing Parameters | ||||||||
| Total AHI/h | 6.5 (3.6, 9.1) * | 23.7 (16.2, 42.5) a,* | 15.2 (11.8, 20.9) a,* | 0.002 | 2.2 (1.0, 5.5) | 8.0 (5.3, 17.0) a | 7.1 (4.9, 11.5) a | <0.001 |
| Central AHI/h | 0.6 (0.3, 2.6) | 11.7 (7.3, 19.1) a,* | 7.0 (2.8, 9.6) a | <0.001 | 0.4 (0.1, 0.9) | 4.0 (1.9, 7.1) a | 2.7 (1.2, 5.3) a | <0.001 |
| Central apnea index/h | 0.6 (0.3, 2.6) | 5.1 (3.0, 11.3) a,* | 3.5 (2.0, 6.7) a,* | 0.014 | 0.4 (0.1, 0.9) | 1.5 (0.7, 2.6) a | 1.2 (0.5, 2.0) a | 0.029 |
| Central hypopnea index/h | 0 (0, 0) | 4.9 (3.3, 10.3) a | 1.6 (1.0, 5.4) a,b | <0.001 | 0 (0, 0) | 2.0 (0.6, 5.8) a | 1.3 (0.5, 3.3) a | <0.001 |
| Mean CAH duration, s | 13.5 (12.0, 15.2) | 14.1 (13.7, 15.0) | 13.4 (12.9, 14.4) | 0.690 | 13.8 (12.0, 14.7) | 14.3 (13.0, 16.4) | 14.2 (12.8, 15.0) | 0.256 |
| Obstructive AHI/h | 4.3 (2.5, 7.4) * | 9.0 (6.0, 22.8) a,* | 8.8 (4.7, 16.0) a,* | 0.008 | 1.8 (0.9, 3.8) | 3.8 (2.2, 7.6)a | 3.6 (2.1, 7.8) a | 0.022 |
| Obstructive apnea index/h | 0.2 (0, 0.5) | 0 (0, 1.2) | 0.1 (0, 0.3) | 0.508 | 0 (0.1, 0.4) | 0 (0, 0.2) | 0 (0.1, 0.3) | 0.695 |
| Obstructive hypopnea index/h | 3.6 (2.2, 7.2) * | 8.1 (6.0, 21.5) a,* | 8.7 (4.7, 15.7) a,* | 0.002 | 1.8 (0.8, 3.2) | 3.6 (1.9, 7.2)a | 3.6 (1.8, 6.6) a | 0.009 |
| Mean OAH duration, s | 26.9 (23.6, 30.4) * | 18.0 (16.5, 19.6) a | 17.8 (16.0, 19.2) a | 0.001 | 20.4 (17.9, 24.0) | 16.5 (15.2, 17.6) a | 16.3 (15.3, 17.1) a | 0.003 |
| PB duration, %TST | 0 (0, 0) | 0.9 (0.2, 2.8) a,* | 0 (0, 1.1) | 0.002 | 0 (0, 0) | 0 (0, 0.2) | 0 (0, 0) | 0.350 |
| Oxygen desaturation index/h | 4.6 (2.1, 10.4) | 35.5 (31.2, 50.8) a,* | 24.9 (16.8, 36.7) a,* | <0.001 | 2.7 (0.9, 4.7) | 17.7 (11.9, 26.5) a | 12.5 (9.5, 18.4) a | <0.001 |
| Mean oxygen saturation, % | 96.0 (95.0, 97.0) | 79.0 (75.5, 84.5) a | 83.0 (73.2, 85.3) a | <0.001 | 96.0 (95.0, 97.0) | 82.0 (81.0, 85.0) a | 83.5 (79.5, 85.8) a | <0.001 |
| SpO2 < 85%, %TST | 0 (0, 0) | 95.6 (45.5, 98.6) a | 74.5 (41.8, 97.5) a | <0.001 | 0 (0, 0) | 85.3 (41.1, 95.7) a | 74.1 (42.1, 96.7) a | <0.001 |
| Blood Pressure | ||||||||
| Evening systolic blood pressure, mmHg | 119 (110, 122) * | 126 (123, 133) a,* | 121.5 (121.0, 126.8) a,b,* | 0.003 | 106 (98, 111) | 98 (96, 113) | 107 (100, 109) | 0.089 |
| Evening diastolic blood pressure, mmHg | 77 (66, 82) | 79 (75, 85) a,* | 79.5 (71.3, 86.3) a,* | 0.018 | 69 (59, 75) | 65 (56, 77) | 71 (64, 78) | 0.111 |
| Morning systolic blood pressure, mmHg | 118 (112, 119) * | 114 (110, 125) * | 117.0 (112.0, 129.0) * | 0.625 | 100 (971, 109) | 103 (98, 111) | 103 (99, 107) | 0.943 |
| Morning diastolic blood pressure, mmHg | 77 (69, 79) * | 76 (72, 83) * | 76.0 (64.5, 83.0) | 0.889 | 64 (58, 71) | 66 (64, 75) | 69 (61, 79) | 0.576 |
| Median Difference (95% CI) between First Night at 3270 m vs. 500 m in Men | Median Difference (95% CI) between First Night at 3270 m vs. 500 m in Women | Median Difference (95% CI) of Altitude-Induced Changes in Men vs. Women | p | |
|---|---|---|---|---|
| AHI/h | 18.5 (10.2 to 27.7) | 6.5 (3.8 to 11.4) | 11.2 (1.9 to 19.6) | 0.020 |
| Central AHI/h | 10.6 (5.6 to 20.3) | 3.6 (2.1 to 8.1) | 6.6 (0.1 to 10.3) | 0.049 |
| Central apnea index/h | 4.4 (1.9 to 11.3) | 1.1 (0.4 to 2.3) | 3.1 (0.1 to 5.6) | 0.049 |
| Central hypopnea index/h | 5.9 (3.4 to 9.0) | 2.7 (1.3 to 5.6) | 2.8 (0 to 5.1) | 0.055 |
| Mean CAH duration, s | 0.7 (−1.0 to 2.4) | 0.2 (−1.2 to 1.7) | 0.7 (−1.6 to 3.0) | 0.336 |
| Obstructive AHI/h | 5.2 (2.0 to 15.6) | 2.2 (0.7 to 4.8) | 2.6 (−0.3 to 6.7) | 0.055 |
| Obstructive apnea index/h | 0 (−0.5 to 1.0) | 0 (−0.2 to 0.2) | 0 (−0.3 to 0.7) | 0.661 |
| Obstructive hypopnea index/h | 5.3 (1.6 to 16.4) | 2.3 (0.6 to 5.0) | 2.2 (−1.0 to 7.0) | 0.231 |
| Mean OAH duration, s | −9.0 (−11.3 to −7.0) | −4.4 (−7.1 to −1.6) | −4.6 (−8.0 to −1.2) | 0.010 |
| PB duration, %TST | 1.1 (0.3 to 4.8) | 0 (0 to 0.3) | 0.6 (0.1 to 1.5) | 0.006 |
| Oxygen desaturation index/h | 32.6 (24.6 to 44.2) | 16.8 (12.4 to 22.3) | 15.6 (7.1 to 25.1) | 0.003 |
| Mean oxygen saturation, % | −16.0 (−20.5 to −11.0) | −13.5 (−15.0 to −12.0) | −3.0 (−7.0 to 2) | 0.238 |
| SpO2 < 85%, %TST | 77.8 (52.2 to 98.0) | 70.9 (49.5 to 91.3) | 3.7 (−21.9 to 23.2) | 0.415 |
| Total AHI | Central AHI | |||||||
|---|---|---|---|---|---|---|---|---|
| Univariate Analysis | Multivariate Analysis | Univariate Analysis | Multivariate Analysis | |||||
| Independent Variables | Coefficient (95% CI) | p | Coefficient (95% CI) | p | Coefficient (95% CI) | p | Coefficient (95% CI) | p |
| Age, years | 0.01 (−0.03, 0.04) | 0.794 | −0.03 (−0.09, 0.03) | 0.329 | ||||
| BMI, kg/m2 | 0.02 (−0.01, 0.05) | 0.118 | −0.02 (−0.03, 0.001) | 0.063 | −0.02 (−0.06, 0.03) | 0.497 | ||
| Sex (men vs. women) | 0.38 (0.20, 0.56) | <0.001 | 0.18 (0.06, 0.30) | 0.004 | 0.38 (0.08, 0.68) | 0.013 | 0.16 (0.56, 0.04) | 0.026 |
| Mallampati score | ||||||||
| III vs. I | 0.25 (−0.26, 0.75) | 0.340 | −0.17 (−0.94, 0.61) | 0.668 | ||||
| II vs. I | 0.27 (0.03, 0.52) | 0.027 | 0.28 (0.14, 0.42) | <0.001 | 0.09 (−0.29, 0.47) | 0.624 | ||
| pH | 5.95 (3.23, 8.68) | <0.001 | 2.62 (0.70, 4.54) | 0.008 | 9.47 (5.40, 13.53) | <0.001 | 3.98 (−0.96, 7.41) | 0.128 |
| PaCO2, mmHg | 0.00 (−0.03, 0.02) | 0.859 | −0.01 (−0.05, 0.03) | 0.579 | ||||
| AMS, LLS score | 0.03 (−0.03, 0.09) | 0.323 | 0.09 (0.01, 0.18) | 0.035 | −0.01 (−0.09, 0.07) | 0.784 | ||
| Baseline AHI/h | 0.06 (0.04, 0.08) | <0.001 | 0.06 (0.04, 0.07) | <0.001 | 0.05 (0.02, 0.09) | 0.007 | 0.03 (0.00, 0.06) | 0.050 |
| Altitude (3270 m vs. 500 m) | 0.52 (0.35, 0.69) | <0.001 | 0.49 (0.34, 0.64) | 0.004 | 0.95 (0.71, 1.20) | <0.001 | 0.94 (0.56, 1.31) | <0.001 |
| Days at altitude (2nd vs. 1st) | −0.24 (−0.13, −0.35) | <0.001 | −0.15 (−0.27, −0.02) | 0.022 | 0.30 (−0.01, 0.61) | 0.059 | −0.21 (−0.48, 0.07) | 0.150 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, T.; Tan, L.; Furian, M.; Zhang, Y.; Luo, L.; Lei, F.; Xue, X.; He, J.; Tang, X. Sex-Specific Difference in the Effect of Altitude on Sleep and Nocturnal Breathing in Young Healthy Volunteers. J. Clin. Med. 2022, 11, 2869. https://doi.org/10.3390/jcm11102869
Li T, Tan L, Furian M, Zhang Y, Luo L, Lei F, Xue X, He J, Tang X. Sex-Specific Difference in the Effect of Altitude on Sleep and Nocturnal Breathing in Young Healthy Volunteers. Journal of Clinical Medicine. 2022; 11(10):2869. https://doi.org/10.3390/jcm11102869
Chicago/Turabian StyleLi, Taomei, Lu Tan, Michael Furian, Yanyan Zhang, Lian Luo, Fei Lei, Xiaofang Xue, Jiaming He, and Xiangdong Tang. 2022. "Sex-Specific Difference in the Effect of Altitude on Sleep and Nocturnal Breathing in Young Healthy Volunteers" Journal of Clinical Medicine 11, no. 10: 2869. https://doi.org/10.3390/jcm11102869