
Growth Pattern of Hepatic Metastasis as a Prognostic Index Reflecting Liver Metastasis-Associated Survival in Breast Cancer Liver Metastasis

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Classification of Liver Metastasis by Radiologic Images
2.3. Classification of Molecular Subtype, Immunohistochemical Staining and Specimen Analysis
2.4. Statistical Analysis
3. Results
3.1. Baseline Patient Characteristics
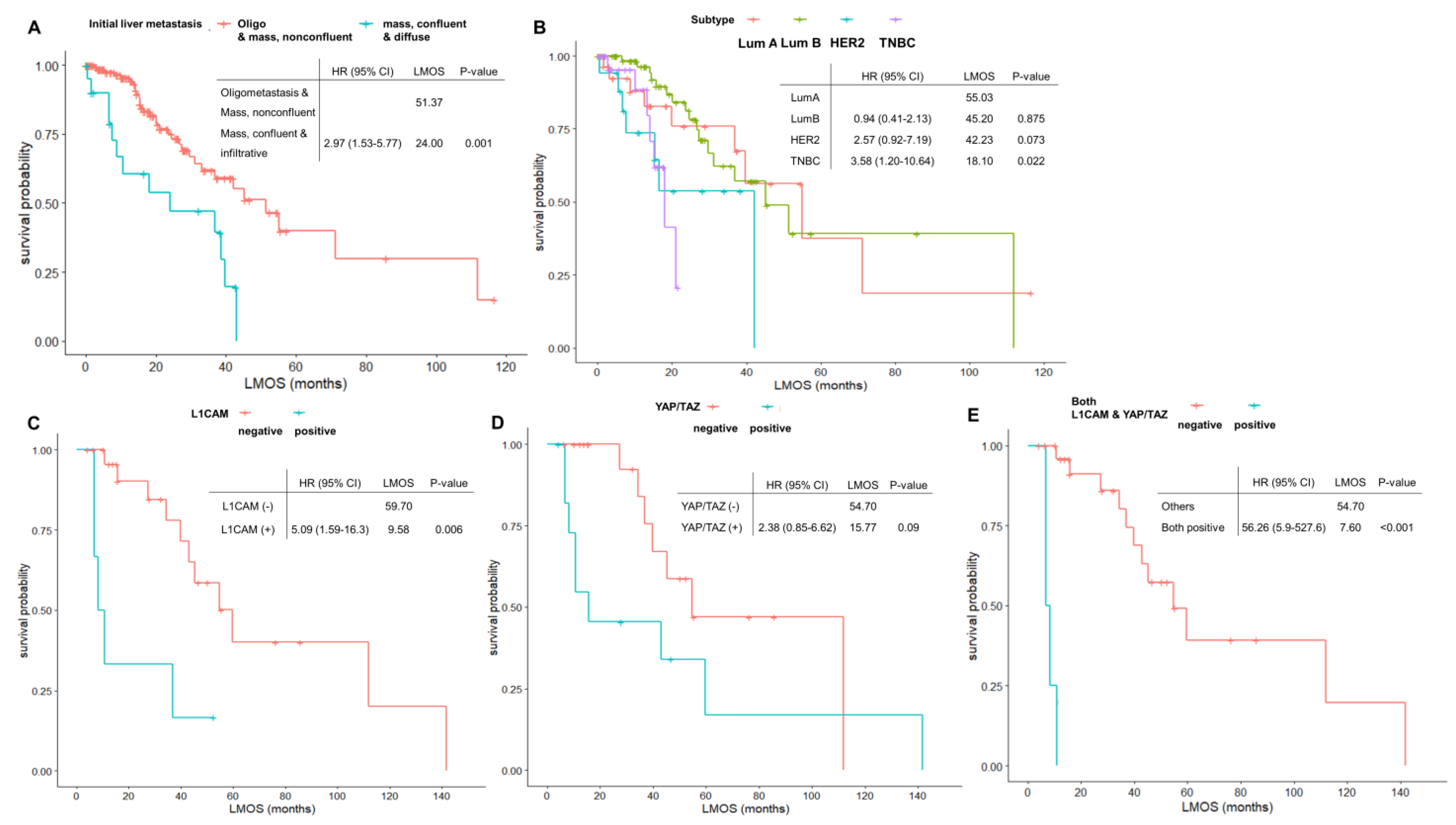
3.2. Liver Metastasis-Associated Overall Survival and Associated Factors
3.3. Expression Pattern of L1CAM, YAP/TAZ, and β1-integrin and Associations with Survival and Liver Metastasis Pattern
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ferlay, J.; Colombet, M.; Soerjomataram, I.; Parkin, D.M.; Piñeros, M.; Znaor, A.; Bray, F. Cancer statistics for the year 2020: An overview. Int. J. Cancer 2021, 149, 778–789. [Google Scholar] [CrossRef] [PubMed]
- Hong, S.; Won, Y.-J.; Park, Y.R.; Jung, K.-W.; Kong, H.-J.; Lee, E.S. Cancer statistics in Korea: Incidence, mortality, survival, and prevalence in 2017. Cancer Res. Treat. 2020, 52, 335. [Google Scholar] [CrossRef] [PubMed]
- Cardoso, F.; Paluch-Shimon, S.; Senkus, E.; Curigliano, G.; Aapro, M.; André, F.; Barrios, C.; Bergh, J.; Bhattacharyya, G.; Biganzoli, L. 5th ESO-ESMO international consensus guidelines for advanced breast cancer (ABC 5). Ann. Oncol. 2020, 31, 1623–1649. [Google Scholar] [CrossRef] [PubMed]
- Harbeck, N.; Penault-Llorca, F.; Cortes, J.; Gnant, M.; Houssami, N.; Poortmans, P.; Ruddy, K.; Tsang, J.; Cardoso, F. Breast cancer. Nat. Rev. Dis. Primers 2019, 5, 66. [Google Scholar] [CrossRef]
- Tsilimigras, D.I.; Brodt, P.; Clavien, P.-A.; Muschel, R.J.; D’Angelica, M.I.; Endo, I.; Parks, R.W.; Doyle, M.; de Santibañes, E.; Pawlik, T.M. Liver metastases. Nat. Rev. Dis. Primers 2021, 7, 27. [Google Scholar] [CrossRef]
- Clark, A.M.; Ma, B.; Taylor, D.L.; Griffith, L.; Wells, A. Liver metastases: Microenvironments and ex-vivo models. Exp. Biol. Med. (Maywood) 2016, 241, 1639–1652. [Google Scholar] [CrossRef]
- Diamond, J.R.; Finlayson, C.A.; Borges, V.F. Hepatic complications of breast cancer. Lancet Oncol. 2009, 10, 615–621. [Google Scholar] [CrossRef]
- Frentzas, S.; Simoneau, E.; Bridgeman, V.L.; Vermeulen, P.B.; Foo, S.; Kostaras, E.; Nathan, M.R.; Wotherspoon, A.; Gao, Z.-H.; Shi, Y. Vessel co-option mediates resistance to anti-angiogenic therapy in liver metastases. Nat. Med. 2016, 22, 1294–1302. [Google Scholar] [CrossRef] [Green Version]
- Van Dam, P.-J.; Van Der Stok, E.P.; Teuwen, L.-A.; Van den Eynden, G.G.; Illemann, M.; Frentzas, S.; Majeed, A.W.; Eefsen, R.L.; Van Den Braak, R.R.C.; Lazaris, A. International consensus guidelines for scoring the histopathological growth patterns of liver metastasis. Br. J. Cancer 2017, 117, 1427–1441. [Google Scholar] [CrossRef] [Green Version]
- Stessels, F.; Van den Eynden, G.; Van der Auwera, I.; Salgado, R.; Van den Heuvel, E.; Harris, A.; Jackson, D.; Colpaert, C.; Van Marck, E.; Dirix, L. Breast adenocarcinoma liver metastases, in contrast to colorectal cancer liver metastases, display a non-angiogenic growth pattern that preserves the stroma and lacks hypoxia. Br. J. Cancer 2004, 90, 1429–1436. [Google Scholar] [CrossRef]
- Latacz, E.; van Dam, P.-J.; Vanhove, C.; Llado, L.; Descamps, B.; Ruiz, N.; Joye, I.; Grünhagen, D.; Van Laere, S.; Dirix, P. Can medical imaging identify the histopathological growth patterns of liver metastases? Semin. Cancer Biol. 2021, 71, 33–41. [Google Scholar] [CrossRef] [PubMed]
- Van Dam, P.-J.; Daelemans, S.; Ross, E.; Waumans, Y.; Van Laere, S.; Latacz, E.; Van Steen, R.; De Pooter, C.; Kockx, M.; Dirix, L.; et al. Histopathological growth patterns as a candidate biomarker for immunomodulatory therapy. Semin. Cancer Biol. 2018, 52, 86–93. [Google Scholar] [CrossRef] [PubMed]
- Chen, D.S.; Mellman, I. Elements of cancer immunity and the cancer–immune set point. Nature 2017, 541, 321–330. [Google Scholar] [CrossRef] [PubMed]
- Vermeulen, P.B.; Bohlok, A.; Leduc, S.; Richard, F.; Botzenhart, L.; Ignatiadis, M.; Aftimos, P.; Sotiriou, C.; Piccart, M.; Hendlisz, A.; et al. Abstract P3-01-13: Association between the histopathological growth patterns (HGP) of liver metastases (LM) and survival after hepatic surgery in patients with oligometastatic breast cancer (BC). Cancer Res. 2020, 80, P3-01-13. [Google Scholar] [CrossRef]
- Galjart, B.; Nierop, P.M.H.; van der Stok, E.P.; van den Braak, R.R.J.C.; Höppener, D.J.; Daelemans, S.; Dirix, L.Y.; Verhoef, C.; Vermeulen, P.B.; Grünhagen, D.J. Angiogenic desmoplastic histopathological growth pattern as a prognostic marker of good outcome in patients with colorectal liver metastases. Angiogenesis 2019, 22, 355–368. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tian, C.; Liu, S.; Wang, Y.; Song, X. Prognosis and Genomic Landscape of Liver Metastasis in Patients with Breast Cancer. Front. Oncol. 2021, 11, 588136. [Google Scholar] [CrossRef]
- Kimbung, S.; Johansson, I.; Danielsson, A.; Veerla, S.; Brage, S.E.; Stolt, M.F.; Skoog, L.; Carlsson, L.; Einbeigi, Z.; Lidbrink, E. Transcriptional Profiling of Breast Cancer Metastases Identifies Liver Metastasis–Selective Genes Associated with Adverse Outcome in Luminal A Primary Breast Cancer. Clin. Cancer Res. 2016, 22, 146–157. [Google Scholar] [CrossRef] [Green Version]
- Donnem, T.; Reynolds, A.R.; Kuczynski, E.A.; Gatter, K.; Vermeulen, P.B.; Kerbel, R.S.; Harris, A.L.; Pezzella, F. Non-angiogenic tumours and their influence on cancer biology. Nat. Rev. Cancer 2018, 18, 323–336. [Google Scholar] [CrossRef]
- Er, E.E.; Valiente, M.; Ganesh, K.; Zou, Y.; Agrawal, S.; Hu, J.; Griscom, B.; Rosenblum, M.; Boire, A.; Brogi, E.; et al. Pericyte-like spreading by disseminated cancer cells activates YAP and MRTF for metastatic colonization. Nat. Cell Biol. 2018, 20, 966–978. [Google Scholar] [CrossRef]
- Liao, A.; Mittal, P.; Lawson, D.H.; Yang, J.J.; Szalai, E.; Grossniklaus, H.E. Radiologic and histopathologic correlation of different growth patterns of metastatic uveal melanoma to the liver. Ophthalmology 2018, 125, 597–605. [Google Scholar] [CrossRef]
- Jeong, W.K.; Choi, S.-Y.; Kim, J. Pseudocirrhosis as a complication after chemotherapy for hepatic metastasis from breast cancer. Clin. Mol. Hepatol. 2013, 19, 190. [Google Scholar] [CrossRef] [PubMed]
- Millard, T.; Gupta, A.; Brenin, C.; Marshall, P.; Dillon, P. Radiographically occult carcinomatous spread of breast cancer to the liver: A challenging case. Case Rep. Oncol. Med. 2019, 2019, 4935615. [Google Scholar] [CrossRef] [PubMed]
- Wyld, L.; Gutteridge, E.; Pinder, S.; James, J.; Chan, S.; Cheung, K.; Robertson, J.; Evans, A. Prognostic factors for patients with hepatic metastases from breast cancer. Br. J. Cancer 2003, 89, 284–290. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hammond, M.E.H.; Hayes, D.F.; Dowsett, M.; Allred, D.C.; Hagerty, K.L.; Badve, S.; Fitzgibbons, P.L.; Francis, G.; Goldstein, N.S.; Hayes, M. American Society of Clinical Oncology/College of American Pathologists guideline recommendations for immunohistochemical testing of estrogen and progesterone receptors in breast cancer (unabridged version). Arch. Pathol. Lab. Med. 2010, 134, e48–e72. [Google Scholar] [CrossRef] [PubMed]
- Gnant, M.; Thomssen, C.; Harbeck, N. St. Gallen/Vienna 2015: A brief summary of the consensus discussion. Breast Care 2015, 10, 124–130. [Google Scholar] [CrossRef] [Green Version]
- Wolff, A.C.; Hammond, M.E.H.; Allison, K.H.; Harvey, B.E.; Mangu, P.B.; Bartlett, J.M.; Bilous, M.; Ellis, I.O.; Fitzgibbons, P.; Hanna, W. Human epidermal growth factor receptor 2 testing in breast cancer: American Society of Clinical Oncology/College of American Pathologists clinical practice guideline focused update. Arch. Pathol. Lab. Med. 2018, 142, 1364–1382. [Google Scholar] [CrossRef] [Green Version]
- Tampakis, A.; Tampaki, E.C.; Nonni, A.; Tsourouflis, G.; Posabella, A.; Patsouris, E.; Kontzoglou, K.; von Flüe, M.; Nikiteas, N.; Kouraklis, G. L1CAM expression in colorectal cancer identifies a high-risk group of patients with dismal prognosis already in early-stage disease. Acta Oncol. 2020, 59, 55–59. [Google Scholar] [CrossRef]
- Han, S.-X.; Bai, E.; Jin, G.-H.; He, C.-C.; Guo, X.-J.; Wang, L.-J.; Li, M.; Ying, X.; Zhu, Q. Expression and clinical significance of YAP, TAZ, and AREG in hepatocellular carcinoma. J. Immunol. Res. 2014, 2014, 261365. [Google Scholar] [CrossRef]
- Johnston, S.; O’Shaughnessy, J.; Martin, M.; Huober, J.; Toi, M.; Sohn, J.; André, V.A.; Martin, H.R.; Hardebeck, M.C.; Goetz, M.P. Abemaciclib as initial therapy for advanced breast cancer: MONARCH 3 updated results in prognostic subgroups. NPJ Breast Cancer 2021, 7, 80. [Google Scholar] [CrossRef]
- Chen, W.; Hoffmann, A.D.; Liu, H.; Liu, X. Organotropism: New insights into molecular mechanisms of breast cancer metastasis. NPJ Precis Oncol. 2018, 2, 4. [Google Scholar] [CrossRef]
- Rashid, N.S.; Grible, J.M.; Clevenger, C.V.; Harrell, J.C. Breast cancer liver metastasis: Current and future treatment approaches. Clin. Exp. Metastasis 2021, 38, 263–277. [Google Scholar] [CrossRef]
- Sadot, E.; Lee, S.Y.; Sofocleous, C.T.; Solomon, S.B.; Gönen, M.; Kingham, T.P.; Allen, P.J.; DeMatteo, R.P.; Jarnagin, W.R.; Hudis, C.A. Hepatic resection or ablation for isolated breast cancer liver metastasis: A case-control study with comparison to medically treated patients. Ann. Surg. 2016, 264, 147. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thompson, B.J. YAP/TAZ: Drivers of tumor growth, metastasis, and resistance to therapy. BioEssays 2020, 42, 1900162. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karreman, M.A.; Winkler, F. The mechanics of metastatic seeding. Nat. Cell Biol. 2018, 20, 860–862. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Total | Oligometastasis | Mass, Nonconfluent | Mass, Confluent | Infiltrative | p Value | |
|---|---|---|---|---|---|---|
| No. of patients | 156 | 77 (49.4%) | 58 (37.2%) | 14 (8.9%) | 7 (4.4%) | |
| Age (median, interquartile range) | 48.0 [42.0;55.0] | 51.0 [44.0;58.0] | 46.0 [42.0;53.0] | 45.5 [39.0;50.0] | 47.0 [43.5;51.5] | 0.174 |
| Pathology | 0.886 | |||||
| Invasive ductal | 147 (94.2%) | 75 (97.4%) | 52 (89.7%) | 13 (92.9%) | 7 (100.0%) | |
| Invasive lobular | 6 (3.8%) | 2 (2.6%) | 3 (5.2%) | 1 (7.1%) | 0 (0.0%) | |
| Invasive ductal with lobular | 1 (0.6%) | 0 (0.0%) | 1 (1.7%) | 0 (0.0%) | 0 (0.0%) | |
| Metaplastic | 1 (0.6%) | 0 (0.0%) | 1 (1.7%) | 0 (0.0%) | 0 (0.0%) | |
| Not assessed | 0 (0.0%) | 0 (0.0%) | 1 (1.7%) | 0 (0.0%) | 0 (0.0%) | |
| Molecular subtype | 0.306 | |||||
| Luminal A | 28 (17.9%) | 15 (19.5%) | 9 (15.5%) | 1 (7.1%) | 3 (42.9%) | |
| Luminal B | 69 (44.2%) | 35 (45.5%) | 26 (44.8%) | 5 (35.7%) | 3 (42.9%) | |
| HER2 positive | 17 (10.9%) | 8 (10.4%) | 5 (8.6%) | 3 (21.4%) | 1 (14.3%) | |
| TNBC | 26 (16.7%) | 13 (16.9%) | 12 (20.7%) | 1 (7.1%) | 0 (0.0%) | |
| Not assessed | 16 (10.3%) | 6 (7.8%) | 6 (10.3%) | 4 (28.6%) | 0 (0.0%) | |
| Diagnosis of liver metastasis | 0.068 | |||||
| initial recurrence or metastasis | 72 (46.2%) | 32 (41.6%) | 25 (43.1%) | 9 (64.3%) | 6 (85.7%) | |
| subsequent recurrence or metastasis | 84 (53.8%) | 45 (58.4%) | 33 (56.9%) | 5 (35.7%) | 1 (14.3%) | |
| Metastasis site | 0.814 | |||||
| liver and others | 142 (91.0%) | 69 (89.6%) | 53 (91.4%) | 13 (92.9%) | 7 (100.0%) | |
| liver only | 14 (9.0%) | 8 (10.4%) | 5 (8.6%) | 1 (7.1%) | 0 (0.0%) | |
| Final liver metastasis pattern | <0.001 | |||||
| Oligometastasis (≤3) | 11 (7.1%) | 11 (14.9%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | |
| mass, nonconfluent | 35 (22.4%) | 15 (20.3%) | 20 (36.4%) | 0 (0.0%) | 0 (0.0%) | |
| mass, confluent | 48 (30.8%) | 28 (37.8%) | 16 (29.1%) | 4 (33.3%) | 0 (0.0%) | |
| infiltrative | 40 (25.6%) | 17 (23.0%) | 13 (23.6%) | 4 (33.3%) | 6 (85.7%) | |
| pseudocirrhosis | 14 (8.9%) | 3 (4.1%) | 6 (10.9%) | 4 (33.3%) | 1 (14.3%) | |
| Not assessed | 8 (5.1%) | |||||
| Initial CPS | <0.001 | |||||
| A | 154 (99.4%) | 77 (100.0%) | 57 (100.0%) | 14 (100.0%) | 6 (85.7%) | |
| B | 1 (0.6%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 1 (14.3%) | |
| Last CPS | 0.032 | |||||
| A | 34 (21.8%) | 23 (34.3%) | 10 (21.7%) | 1 (7.7%) | 0 (0.0%) | |
| B | 24 (15.4%) | 13 (19.4%) | 9 (19.6%) | 2 (15.4%) | 0 (0.0%) | |
| C | 50 (32.1%) | 20 (29.9%) | 16 (34.8%) | 10 (76.9%) | 4 (80.0%) | |
| Not assessed | 23 (14.7%) | 11 (16.4%) | 11 (23.9%) | 0 (0.0%) | 1 (20.0%) | |
| Cause of death | 0.08 | |||||
| Cancer | 77 (58.8%) | 44 (65.7%) | 28 (60.9%) | 4 (30.8%) | 1 (20.0%) | |
| Hepatic failure due to liver metastasis | 46 (35.1%) | 18 (26.9%) | 15 (32.6%) | 9 (69.2%) | 4 (80.0%) | |
| Others | 5 (3.8%) | 4 (6.0%) | 1 (2.2%) | 0 (0.0%) | 0 (0.0%) | |
| Not assessed | 3 (2.3%) | 1 (1.5%) | 2 (4.3%) | 0 (0.0%) | 0 (0.0%) |
| Luminal A | Luminal B | HER2 Positive | TNBC | p Value | |
|---|---|---|---|---|---|
| No. of patients | 28 (20%) | 69 (49.3%) | 17 (12.1%) | 26 (18.6%) | |
| Initial metastasis | 0.505 | ||||
| No | 15 (53.6%) | 37 (53.6%) | 6 (35.3%) | 15 (57.7%) | |
| Yes | 13 (46.4%) | 32 (46.4%) | 11 (64.7%) | 11 (42.3%) | |
| Metastasis site | 0.433 | ||||
| liver and others | 25 (89.3%) | 62 (89.9%) | 17 (100.0%) | 22 (84.6%) | |
| liver only | 3 (10.7%) | 7 (10.1%) | 0 (0.0%) | 4 (15.4%) | |
| Initial liver metastasis pattern | 0.548 | ||||
| Oligometastasis (≤3) | 15 (53.6%) | 35 (50.7%) | 8 (47.1%) | 13 (50.0%) | |
| mass, nonconfluent | 9 (32.1%) | 26 (37.7%) | 5 (29.4%) | 12 (46.2%) | |
| mass, confluent | 1 (3.6%) | 5 (7.2%) | 3 (17.6%) | 1 (3.8%) | |
| infiltrative | 3 (10.7%) | 3 (4.3%) | 1 (5.9%) | 0 (0.0%) | |
| Final liver metastasis pattern | 0.77 | ||||
| Oligometastasis (≤3) | 0 (0.0%) | 6 (9.0%) | 2 (11.8%) | 2 (8.7%) | |
| mass, nonconfluent | 7 (26.9%) | 16 (23.9%) | 5 (29.4%) | 5 (21.7%) | |
| mass, confluent | 6 (23.1%) | 24 (35.8%) | 5 (29.4%) | 10 (43.5%) | |
| infiltrative | 9 (34.6%) | 17 (25.4%) | 4 (23.5%) | 4 (17.4%) | |
| pseudocirrhosis | 4 (15.4%) | 4 (6.0%) | 1 (5.9%) | 2 (8.7%) |
| Characteristics | Liver Metastasis-Associated Overall Survival (LMOS) | |||
|---|---|---|---|---|
| Univariate Analysis | Multivariate Analysis | |||
| Hazard Ratio (95% CI) | p Value | Hazard Ratio (95% CI) | p Value | |
| Molecular subtype | ||||
| Luminal B vs. A | 0.94 (0.41–2.13) | 0.875 | 0.93 (0.41–2.12) | 0.866 |
| HER2 positive vs. A | 2.57 (0.92–7.19) | 0.073 | 2.09 (0.73–5.93) | 0.165 |
| TNBC vs. A | 3.58 (1.20–10.64) | 0.022 | 3.47 (1.17–10.3) | 0.025 |
| Initial liver metastasis | ||||
| Yes vs. No | 1.24 (0.69–2.25) | 0.470 | ||
| Metastasis site | ||||
| liver only vs. multiple metastasis | 0.62 (0.24–1.60) | 0.325 | ||
| Initial liver metastasis pattern | ||||
| mass, confluent or infiltrative vs. oligometastasis or mass, non-confluent | 2.97 (1.53–5.77) | 0.001 | 3.38 (1.59–7.18) | 0.002 |
| Local treatment | ||||
| Yes vs. No | 0.78 (0.36–1.73) | 0.545 | ||
| Final Liver Metastasis Pattern | Oligometastasis and Mass, Non-Confluent | Mass, Confluent and Infiltrative and Pseudocirrhosis | p Value |
|---|---|---|---|
| YAP/TAZ | 0.020 | ||
| negative | 10 (32.3%) | 9 (29.0%) | |
| positive | 1 (3.2%) | 11 (35.5%) | |
| L1CAM | 0.382 | ||
| negative | 10 (32.3%) | 15 (48.4%) | |
| positive | 1 (3.2%) | 5 (16.1%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, J.; Choi, M.; Joe, S.; Shin, K.; Lee, S.-H.; Lee, A. Growth Pattern of Hepatic Metastasis as a Prognostic Index Reflecting Liver Metastasis-Associated Survival in Breast Cancer Liver Metastasis. J. Clin. Med. 2022, 11, 2852. https://doi.org/10.3390/jcm11102852
Lee J, Choi M, Joe S, Shin K, Lee S-H, Lee A. Growth Pattern of Hepatic Metastasis as a Prognostic Index Reflecting Liver Metastasis-Associated Survival in Breast Cancer Liver Metastasis. Journal of Clinical Medicine. 2022; 11(10):2852. https://doi.org/10.3390/jcm11102852
Chicago/Turabian StyleLee, Jieun, Moonhyung Choi, Seungyeon Joe, Kabsoo Shin, Sung-Hak Lee, and Ahwon Lee. 2022. "Growth Pattern of Hepatic Metastasis as a Prognostic Index Reflecting Liver Metastasis-Associated Survival in Breast Cancer Liver Metastasis" Journal of Clinical Medicine 11, no. 10: 2852. https://doi.org/10.3390/jcm11102852