
Independent and Joint Associations of Pessimism, Total Calorie Intake and Acid-Producing Diets with Insomnia Symptoms among Breast Cancer Survivors

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Assessment of Insomnia Symptoms
2.3. Assessment of Pessimism
2.4. Assessment of Dietary Intake
2.5. Assessment of Demographic Information
2.6. Statistical Analysis
3. Results
3.1. Baseline Characteristics by WHI-IRS
3.2. Baseline Characteristics by Pessimism
3.3. Baseline Characteristics by Calorie Consumption
3.4. Baseline Characteristics by PRAL Quartile
3.5. Longitudinal Impact of Pessimism, Calorie Intake, and Dietary Acid Load
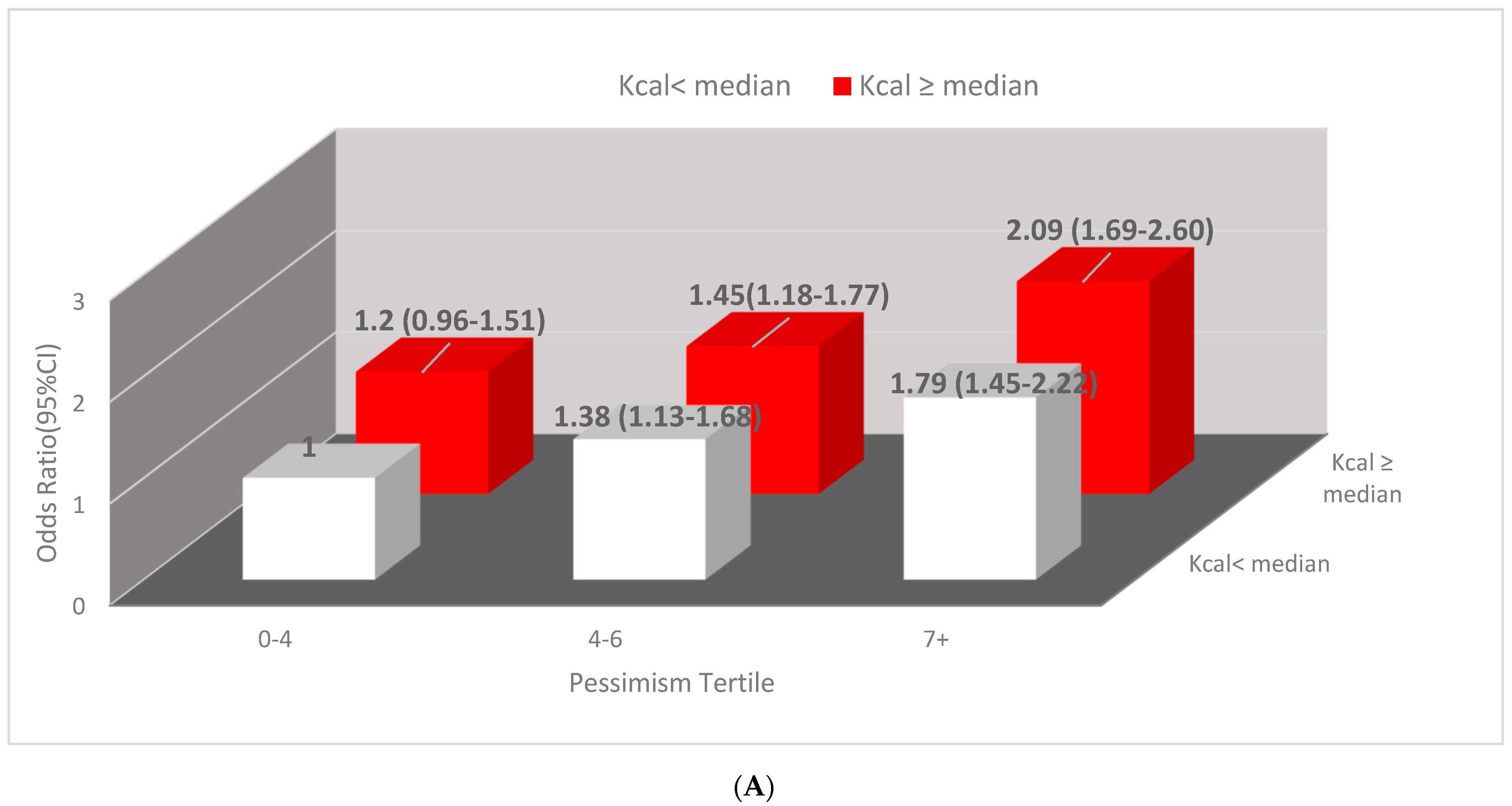
3.6. Joint Impact of Pessimism and Calorie Intake and Joint Impact of Pessimism and Dietary Acid Load on Presentation of Clinical Insomnia
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- World Health Organization Cancer Fact Sheet. Available online: https://www.who.int/news-room/fact-sheets/detail/cancer (accessed on 23 January 2021).
- Key Statistics for Breast Cancer. Available online: https://www.cancer.org/cancer/breast-cancer/about/how-common-is-breast-cancer.html (accessed on 23 January 2022).
- Palesh, O.; Scheiber, C.; Kesler, S.; Janelsins, M.C.; Guido, J.J.; Heckler, C.; Cases, M.G.; Miller, J.; Chrysson, N.G.; Mustian, K.M. Feasibility and acceptability of brief behavioral therapy for cancer-related insomnia: Effects on insomnia and circadian rhythm during chemotherapy: A phase II randomised multicentre controlled trial. Br. J. Cancer 2018, 119, 274–281. [Google Scholar] [CrossRef]
- Mao, J.J.; Armstrong, K.; Bowman, M.; Xie, S.X.; Kadakia, R.; Farrar, J.T. Symptom burden among cancer survivors: Impact of age and comorbidity. J. Am. Board Fam. Med. 2007, 20, 434–443. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leysen, L.; Lahousse, A.; Nijs, J.; Adriaenssens, N.; Mairesse, O.; Ivakhnov, S.; Bilterys, T.; Van Looveren, E.; Pas, R.; Beckwée, D. Prevalence and risk factors of sleep disturbances in breast cancersurvivors: Systematic review and meta-analyses. Support. Care Cancer 2019, 27, 4401–4433. [Google Scholar] [CrossRef] [PubMed]
- Baker, F.C.; de Zambotti, M.; Colrain, I.M.; Bei, B. Sleep problems during the menopausal transition: Prevalence, impact, and management challenges. Nat. Sci. Sleep 2018, 10, 73–95. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, J.; Han, Y.; Cho, H.H.; Kim, M.-R. Sleep Disorders and Menopause. J. Menopausal Med. 2019, 25, 83–87. [Google Scholar] [CrossRef]
- Savard, J.; Simard, S.; Blanchet, J.; Ivers, H.; Morin, C.M. Prevalence, clinical characteristics, and risk factors for insomnia in the context of breast cancer. Sleep 2001, 24, 583–590. [Google Scholar] [CrossRef] [Green Version]
- Nutt, D.; Wilson, S.; Paterson, L. Sleep disorders as core symptoms of depression. Dialogues Clin. Neurosci. 2008, 10, 329–336. [Google Scholar] [CrossRef]
- Zaslavsky, O.; LaCroix, A.Z.; Hale, L.; Tindle, H.; Shochat, T. Longitudinal changes in insomnia status and incidence of physical, emotional, or mixed impairment in postmenopausal women participating in the Women’s Health Initiative (WHI) study. Sleep Med. 2015, 16, 364–371. [Google Scholar] [CrossRef]
- Granö, N.; Vahtera, J.; Virtanen, M.; Keltikangas-Järvinen, L.; Kivimaki, M. Association of hostility with sleep duration and sleep disturbances in an employee population. Int J. Behav. Med. 2008, 15, 73–80. [Google Scholar] [CrossRef]
- Uchino, B.N.; Cribbet, M.; de Grey, R.K.; Cronan, S.; Trettevik, R.; Smith, T.W. Dispositional optimism and sleep quality: A test of mediating pathways. J. Behav. Med. 2017, 40, 360–365. [Google Scholar] [CrossRef]
- Ren, Y.; Li, S.; Zhou, S.; Wang, Y.; Li, L.; Zhang, J.; Yang, Y.; He, J.; Zhu, X. Optimism outweighs neuroticism and anxiety sensitivity to predict insomnia symptoms in women after surgery for breast cancer. Support. Care Cancer 2019, 27, 2903–2909. [Google Scholar] [CrossRef] [PubMed]
- American Psychological Association Dictionary of Psychology. Available online: https://dictionary.apa.org/pessimism (accessed on 23 January 2022).
- Hecht, D. The neural basis of optimism and pessimism. Exp. Neurobiol. 2013, 22, 173–199. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alvaro, P.K.; Roberts, R.M.; Harris, J.K. A Systematic Review Assessing Bidirectionality between Sleep Disturbances, Anxiety, and Depression. Sleep 2013, 36, 1059–1068. [Google Scholar] [CrossRef]
- Gangwisch, J.E.; Hale, L.; St-Onge, M.P.; Choi, L.; LeBlanc, E.S.; Malaspina, D.; Opler, M.G.; Shadyab, A.H.; Shikany, J.M.; Snetselaar, L.; et al. High glycemic index and glycemic load diets as risk factors for insomnia: Analyses from the Women’s Health Initiative. Am. J. Clin. Nutr. 2020, 111, 429–439. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, E.; Yatsuya, H.; Uemura, M.; Murata, C.; Otsuka, R.; Toyoshima, H.; Tamakoshi, K.; Sasaki, S.; Kawaguchi, L.; Aoyama, A. Associations of protein, fat, and carbohydrate intakes with insomnia symptoms among middle-aged Japanese workers. J. Epidemiol 2013, 23, 132–138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheng, F.W.; Li, Y.; Winkelman, J.W.; Hu, F.B.; Rimm, E.B.; Gao, X. Probable insomnia is associated with future total energy intake and diet quality in men. Am. J. Clin. Nutr. 2016, 104, 462–469. [Google Scholar] [CrossRef] [PubMed]
- Wu, T.; Hsu, F.-C.; Pierce, J.P. Increased Acid-Producing Diet and Past Smoking Intensity Are Associated with Worse Prognoses Among Breast Cancer Survivors: A Prospective Cohort Study. J. Clin. Med. 2020, 9, 1817. [Google Scholar] [CrossRef]
- Wu, T.; Hsu, F.-C.; Pierce, J.P. Acid-Producing Diet and Depressive Symptoms among Breast Cancer Survivors: A Longitudinal Study. Cancers 2020, 12, 3183. [Google Scholar] [CrossRef]
- Tessou, K.; Lemus, H.; Hsu, F.-C.; Pierce, J.; Hong, S.; Brown, L.; Wu, T. Independent and Joint Impacts of Acid-Producing Diets and Depression on Physical Health among Breast Cancer Survivors. Nutrients 2021, 13, 2422. [Google Scholar] [CrossRef]
- Chronister, B.N.C.; Wu, T.; Santella, R.M.; Neugut, A.I.; Wolff, M.S.; Chen, J.; Teitelbaum, S.L.; Parada, H. Dietary Acid Load, Serum Polychlorinated Biphenyl Levels, and Mortality Following Breast Cancer in the Long Island Breast Cancer Study Project. Int. J. Env. Res. Public Health 2021, 19, 374. [Google Scholar] [CrossRef]
- Shirali, A. Electrolyte and Acid–Base Disorders in Malignancy, in Onco-Nephrology Curriculum; American Society of Nephrology: Washington, DC, USA, 2016. [Google Scholar]
- Abdullah, S.Y.; Ali, M.K.; Sabha, M.M. Type-B lactic acidosis associated with progressive multiple myeloma. Saudi. Med. J. 2015, 36, 239–242. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pierce, J.P.; Faerber, S.; Wright, F.A.; Rock, C.L.; Newman, V.; Flatt, S.W.; Kealey, S.; Jones, V.E.; Caan, B.J.; Gold, E.B.; et al. A randomized trial of the effect of a plant-based dietary pattern on additional breast cancer events and survival: The Women’s Healthy Eating and Living (WHEL) Study. Control. Clin. Trials 2002, 23, 728–756. [Google Scholar] [CrossRef]
- Levine, D.W.; Kripke, D.F.; Kaplan, R.M.; Lewis, M.A.; Naughton, M.J.; Bowen, D.J.; Shumaker, S.A. Reliability and validity of the Women’s Health Initiative Insomnia Rating Scale. Psychol Assess. 2003, 15, 137–148. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Levine, D.W.; Kaplan, R.M.; Kripke, D.F.; Bowen, D.J.; Naughton, M.J.; Shumaker, S.A. Factor structure and measurement invariance of the Women’s Health Initiative Insomnia Rating Scale. Psychol Assess. 2003, 15, 123–136. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tindle, H.A.; Duncan, M.S.; Liu, S.; Kuller, L.H.; Woods, N.F.; Rapp, S.R.; Kroenke, C.H.; Coday, M.; Loucks, E.B.; Lamonte, M.J.; et al. Optimism, pessimism, cynical hostility, and biomarkers of metabolic function in the Women’s Health Initiative. J. Diabetes 2018, 10, 512–523. [Google Scholar] [CrossRef] [PubMed]
- Kubzansky, L.D.; Kubzansky, P.E.; Maselko, J. Optimism and pessimism in the context of health: Bipolar opposites or separate constructs? Pers. Soc. Psychol. Bull. 2004, 30, 943–956. [Google Scholar] [CrossRef]
- Frassetto, L.A.; Todd, K.M.; Morris, R.C.J.; Sebastian, A. Estimation of net endogenous noncarbonic acid production in humans from diet potassium and protein contents. Am. J. Clin. Nutr. 1998, 68, 576–583. [Google Scholar] [CrossRef] [Green Version]
- Remer, T.; Manz, F. Potential renal acid load of foods and its influence on urine pH. J. Am. Diet. Assoc. 1995, 95, 791–797. [Google Scholar] [CrossRef]
- Schou, I.; Ekeberg, Ø.; Sandvik, L.; Hjermstad, M.J.; Ruland, C.M. Multiple predictors of health-related quality of life in early stage breast cancer. Data from a year follow-up study compared with the general population. Qual. Life Res. 2005, 14, 1813–1823. [Google Scholar] [CrossRef]
- Petersen, L.R.; Clark, M.M.; Novotny, P.; Kung, S.; Sloan, J.A.; Patten, C.A.; Vickers, K.S.; Rummans, T.A.; Rn, M.H.F.; Colligan, R.C. Relationship of optimism-pessimism and health-related quality of life in breast cancer survivors. J. Psychosoc. Oncol. 2008, 26, 15–32. [Google Scholar] [CrossRef]
- Calderon, C.; Carmona-Bayonas, A.; Hernández, R.; Ghanem, I.; Castelo, B.; de Castro, E.M.; Ferreira, E.; Ciria, L.; Muñiz, M.; Jimenez-Fonseca, P. Effects of pessimism, depression, fatigue, and pain on functional health-related quality of life in patients with resected non-advanced breast cancer. Breast 2019, 44, 108–112. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Wu, C.; Gan, Y.; Qu, X.; Lu, Z. Insomnia and the risk of depression: A meta-analysis of prospective cohort studies. BMC Psychiatry 2016, 16, 375. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pänkäläinen, M.; Kerola, T.; Kampman, O.; Kauppi, M.; Hintikka, J. Pessimism and risk of death from coronary heart disease among middle-aged and older Finns: An eleven-year follow-up study. BMC Public Health 2016, 16, 1124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nabi, H.; Koskenvuo, M.; Singh-Manoux, A.; Korkeila, J.; Suominen, S.; Korkeila, K.; Vahtera, J.; Kivimaki, M. Low pessimism protects against stroke: The Health and Social Support (HeSSup) prospective cohort study. Stroke 2010, 41, 187–190. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Daneshzad, E.; Keshavarz, S.-A.; Qorbani, M.; Larijani, B.; Bellissimo, N.; Azadbakht, L. Association of dietary acid load and plant-based diet index with sleep, stress, anxiety and depression in diabetic women. Br. J. Nutr. 2020, 123, 901–912. [Google Scholar] [CrossRef]
- Afsar, B.; Elsurer, R. Association between serum bicarbonate and pH with depression, cognition and sleep quality in hemodialysis patients. Ren. Fail. 2015, 37, 957–960. [Google Scholar] [CrossRef] [Green Version]
- Gong, X.-H.; Wang, J.-W.; Li, J.; Chen, X.-F.; Sun, L.; Yuan, Z.-P.; Yu, J.-M. Physical exercise, vegetable and fruit intake and health-related quality of life in Chinese breast cancer survivors: A cross-sectional study. Qual. Life Res. 2017, 26, 1541–1550. [Google Scholar] [CrossRef]
- Kim, N.-H.; Song, S.; Jung, S.-Y.; Lee, E.; Kim, Z.; Moon, H.-G.; Noh, D.-Y.; Lee, J.E. Dietary pattern and health-related quality of life among breast cancer survivors. BMC Womens Health 2018, 18, 65. [Google Scholar] [CrossRef] [Green Version]
- Sharp, J.T.; Druz, W.S.; D’Souza, V.; Diamond, E. Effect of metabolic acidosis upon sleep apnea. Chest 1985, 87, 619–624. [Google Scholar] [CrossRef]
- Levitzky, M.G. Using the pathophysiology of obstructive sleep apnea to teach cardiopulmonary integration. Adv. Physiol Educ. 2008, 32, 196–202. [Google Scholar] [CrossRef] [Green Version]
- Allebrandt, K.V.; Teder-Laving, M.; Kantermann, T.; Peters, A.; Campbell, H.; Rudan, I.; Wilson, J.F.; Metspalu, A.; Roenneberg, T. Chronotype and sleep duration: The influence of season of assessment. Chronobiol. Int. 2014, 31, 731–740. [Google Scholar] [CrossRef] [PubMed]
- Kant, A.K.; I Graubard, B. Association of self-reported sleep duration with eating behaviors of American adults: NHANES 2005-2010. Am. J. Clin. Nutr. 2014, 100, 938–947. [Google Scholar] [CrossRef] [Green Version]
- Marinac, C.R.; Nelson, S.H.; Breen, C.I.; Hartman, S.J.; Natarajan, L.; Pierce, J.P.; Flatt, S.W.; Sears, D.D.; Patterson, R.E. Prolonged Nightly Fasting and Breast Cancer Prognosis. JAMA Oncol. 2016, 2, 1049–1055. [Google Scholar] [CrossRef] [PubMed]
- Gagliardi, G.S.; Shah, A.P.; Goldstein, M.; Denua–Rivera, S.; Doghramji, K.; Cohen, S.; Dimarino, A.J. Effect of zolpidem on the sleep arousal response to nocturnal esophageal acid exposure. Clin. Gastroenterol Hepatol. 2009, 7, 948–952. [Google Scholar] [CrossRef] [PubMed]
- Jung, R.S.C.H.-K.; Choung, R.S.; Talley, N.J. Gastroesophageal reflux disease and sleep disorders: Evidence for a causal link and therapeutic implications. J. Neurogastroenterol. Motil. 2010, 16, 22–29. [Google Scholar] [CrossRef] [PubMed]
- Futagami, S.; Shimpuku, M.; Yamawaki, H.; Izumi, N.; Kodaka, Y.; Nagoya, H.; Wakabayashi, T.; Shindo, T.; Kawagoe, T.; Sakamoto, C. Sleep disorders in functional dyspepsia and future therapy. J. Nippon. Med. Sch. 2013, 80, 104–109. [Google Scholar] [CrossRef] [Green Version]
- Yamawaki, H.; Futagami, S.; Shimpuku, M.; Sato, H.; Wakabayashi, T.; Maruki, Y.; Kodaka, Y.; Nagoya, H.; Shindo, T.; Kawagoe, T.; et al. Impact of sleep disorders, quality of life and gastric emptying in distinct subtypes of functional dyspepsia in Japan. J. Neurogastroenterol. Motil. 2014, 20, 104–112. [Google Scholar] [CrossRef] [Green Version]
- Greer, S.M.; Goldstein, A.N.; Walker, M.P. The impact of sleep deprivation on food desire in the human brain. Nat. Commun. 2013, 4, 2259. [Google Scholar] [CrossRef] [Green Version]
- Chaput, J.P. Sleep patterns, diet quality and energy balance. Physiol. Behav. 2014, 134, 86–91. [Google Scholar] [CrossRef]
- Spaeth, A.M.; Dinges, D.F.; Goel, N. Sex and race differences in caloric intake during sleep restriction in healthy adults. Am. J. Clin. Nutr. 2014, 100, 559–566. [Google Scholar] [CrossRef] [Green Version]
- Pänkäläinen, M.; Fogelholm, M.; Valve, R.; Kampman, O.; Kauppi, M.; Lappalainen, E.; Hintikka, J. Pessimism, diet, and the ability to improve dietary habits: A three-year follow-up study among middle-aged and older Finnish men and women. Nutr. J. 2018, 17, 92. [Google Scholar] [CrossRef] [PubMed]
- Ait-Hadad, W.; Bénard, M.; Shankland, R.; Kesse-Guyot, E.; Robert, M.; Touvier, M.; Hercberg, S.; Buscail, C.; Péneau, S. Optimism is associated with diet quality, food group consumption and snacking behavior in a general population. Nutr. J. 2020, 19, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Insomnia Score < 9 | Insomnia Score ≥ 9 | ||
|---|---|---|---|
| n = 1812 | n = 1148 | p-Value | |
| Pessimism a | 6.0 (4.0, 7.0) | 6.0 (5.0, 8.0) | <0.0001 |
| KCAL a | 1685.0 (1431.0, 1979.5) | 1703.5 (1450.0, 1988.5) | 0.30 |
| PRAL a | −4.2(−13.9, 4.4) | −3.0 (−13.4, 5.5) | 0.02 |
| NEAP a | 39.6 (32.3, 48.3) | 40.6 (32.8, 48.8) | 0.06 |
| Age at Diagnosis (years) a | 50 (45, 57) | 50 (45, 57) | 0.48 |
| Normal Weight, N (%) | 801 (62.9) | 472 (37.1) | 0.07 |
| White, N (%) | 1545 (61.1) | 983 (38.9) | 0.79 |
| Stage at Diagnosis | |||
| I, N (%) | 698 (69.0) | 447 (39.0) | 0.80 |
| II, N (%) | 1019 (61.2) | 647 (38.8) | |
| III, N (%) | 95 (63.8) | 54 (36.2) | |
| Intervention Group, N (%) | 929 (63.0) | 546 (37.0) | 0.05 |
| Hormone Receptor Status | |||
| ER+/PR+, N (%) | 1109 (60.3) | 729 (39.7) | 0.35 |
| Post-Menopause, N (%) | 1398 (59.4) | 954 (40.6) | <0.0001 |
| Chemotherapy, N (%) | 1266 (61.4) | 797 (38.6) | 0.92 |
| Radiation, N (%) | 1112 (61.2) | 704(38.8) | 0.85 |
| Smoking Status | |||
| Never N, (%) | 988 (62.0) | 606 (38.0) | 0.48 |
| Past N, (%) | 739 (60.0) | 493 (40.0) | |
| Current N, (%) | 85 (63.4) | 49 (36.6) | |
| Education | |||
| Some College or above N, (%) | 1015 (63.5) | 584 (36.5) | 0.006 |
| Alcohol Abstainer N, (%) | 571 (61.4) | 359 (38.6) | 0.97 |
| Pessimism Score | ||||
|---|---|---|---|---|
| Tertile 1 | Tertile 2 | Tertile 3 | p-Value | |
| 0–4 | 5–6 | 7+ | ||
| n = 813 | n = 1105 | n = 1042 | ||
| Insomnia a | 6.0 (3, 10) | 7 (4, 10) | 8.0 (5, 12) | <0.0001 |
| Overweight and obese, N (%) | 429 (25.4) | 624 (37.0) | 634 (37.6) | 0.002 |
| Stage at Diagnosis | ||||
| I, N (%) | 295 (25.8) | 448 (39.1) | 402 (35.1) | 0.31 |
| II, N (%) | 474 (28.5) | 609 (36.6) | 583 (35.0) | |
| III, N (%) | 44 (29.5) | 48 (32.2) | 57 (38.2) | |
| ER+/PR+, N (%) | 523 (28.5) | 684 (37.2) | 631 (34.3) | 0.01 |
| Post-Menopause, N (%) | 654 (27.8) | 881 (37.5) | 817 (34.7) | 0.82 |
| Chemotherapy, N (%) | 546 (26.5) | 768 (37.2) | 749 (36.3) | 0.23 |
| Radiation, N (%) | 503 (27.7) | 665 (36.6) | 648 (35.6) | 0.83 |
| Smoking Status | ||||
| Never, N (%) | 404 (25.4) | 605 (38.0) | 585 (36.7) | 0.003 |
| Past, N (%) | 379 (30.8) | 455 (36.9) | 398 (32.3) | |
| Current, N (%) | 30 (22.4) | 45 (33.6) | 59 (44.0) | |
| Alcohol Abstainer, N (%) | 239 (25.7) | 330 (35.5) | 361 (38.8) | 0.003 |
| Education College or Greater, N (%) | 484 (30.2) | 624 (39.0) | 491 (30.7) | <0.001 |
| Calorie Intake | |||||
|---|---|---|---|---|---|
| Quartile 1 | Quartile 2 | Quartile 3 | Quartile 4 | p-Value | |
| <1363 | 1363< to <1603 | 1603< to <1876 | ≥1876 | ||
| n = 550 | n = 668 | n = 777 | n = 965 | ||
| Insomnia a | 7.0 (4.0, 11.0) | 7.0 (4.0, 11.0) | 7.0 (4.0, 11.0) | 7.0 (4.0, 11.0) | 0.94 |
| Normal Weight, N (%) | 231 (18.2) | 315 (24.7) | 355 (27.9) | 372 (29.2) | 0.002 |
| Stage at Diagnosis | |||||
| I, N (%) | 227 (19.8) | 251 (21.9) | 296 (25.9) | 371 (32.4) | 0.18 |
| II, N (%) | 301 (18.1) | 390 (23.4) | 429 (25.8) | 546 (32.8) | |
| III, N (%) | 22 (14.8) | 27 (18.1) | 52 (34.9) | 48 (32.2) | |
| ER+/PR+, N (%) | 354 (19.3) | 408 (22.2) | 479 (26.1) | 597 (32.5) | 0.48 |
| Post-Menopause, N (%) | 464 (19.7) | 546 (23.2) | 609 (25.9) | 733 (31.2) | 0.005 |
| Chemotherapy, N (%) | 369 (17.9) | 455 (22.1) | 555 (26.9) | 684 (33.2) | 0.43 |
| Radiation, N (%) | 333 (18.3) | 395 (21.8) | 498 (27.4) | 590 (32.5) | 0.10 |
| Smoking Status | |||||
| Never, N (%) | 303 (19.0) | 359 (22.5) | 432 (27.1) | 500 (31.4) | 0.37 |
| Past, N (%) | 217 (17.6) | 286 (23.2) | 309 (25.1) | 420 (34.1) | |
| Current, N (%) | 30 (22.4) | 23 (17.2) | 36 (26.9) | 45 (33.6) | |
| Alcohol Abstainer, N (%) | 259 (27.9) | 228 (24.5) | 216 (23.2) | 227 (24.4) | <0.0001 |
| Education College or Greater, N (%) | 272 (17.0) | 369 (23.1) | 439 (27.5) | 519 (32.5) | 0.07 |
| PRAL Score | |||||
|---|---|---|---|---|---|
| Quartile 1 | Quartile 2 | Quartile 3 | Quartile 4 | p-Value | |
| <−19.49 | −19.49< to <−6.94 | −6.94< to <3.22 | ≥3.22 | ||
| n = 434 | n = 782 | n = 881 | n = 863 | ||
| Insomnia a | 6 (3, 10) | 7 (4, 11) | 7 (4, 11) | 7 (4, 11) | 0.002 |
| Normal Weight, N (%) | 259 (20.4) | 393 (30.9) | 338 (26.6) | 283 (22.2) | <0.0001 |
| Stage at Diagnosis | |||||
| I, N (%) | 171 (14.9) | 298 (26.0) | 335 (29.3) | 341 (29.8) | 0.58 |
| II, N (%) | 241 (14.5) | 450 (27.0) | 506 (30.4) | 469 (28.2) | |
| III, N (%) | 22 (14.8) | 34 (22.8) | 40 (26.9) | 53 (35.6) | |
| ER+/PR+, N (%) | 271 (14.7) | 492 (26.8) | 566 (30.8) | 509 (27.7) | 0.0001 |
| Post-Menopause, N (%) | 369 (15.7) | 644 (27.4) | 700 (29.8) | 639 (27.2) | 0.0001 |
| Chemotherapy, N (%) | 287 (13.9) | 515 (25.0) | 631 (30.6) | 630 (30.5) | 0.02 |
| Radiation, N (%) | 267 (14.7) | 494 (27.2) | 521 (28.7) | 534 (29.4) | 0.46 |
| Smoking Status | |||||
| Never, N (%) | 230 (14.4) | 419 (26.3) | 476 (29.9) | 469 (29.4) | 0.27 |
| Past, N (%) | 194 (15.8) | 326 (26.5) | 364 (29.6) | 348 (28.3) | |
| Current, N (%) | 10 (7.5) | 37 (27.6) | 41 (30.6) | 46 (34.3) | |
| Alcohol Abstainer, N (%) | 143 (15.4) | 234 (25.2) | 282 (30.3) | 271 (29.1) | 0.70 |
| Education College or Greater, N (%) | 283 (17.7) | 452 (28.3) | 470 (29.4) | 394 (24.6) | <0.0001 |
| Insomnia Score (≥9 vs. <9) | ||||
|---|---|---|---|---|
| OR (95% CI) | OR (95% CI) | |||
| Range | Age-Adjusted Model | Multivariable Model | ||
| Pessimism | ||||
| Tertile 1 | <5 | Ref | Ref | |
| Tertile 2 | 5 to <6 | 1.17 (1.04–1.32) | 1.14 (1.01–1.28) | |
| Tertile 3 | ≥6 | 1.64 (1.43–1.86) | 1.57 (1.37–1.79) | |
| p for trend | <0.001 | <0.001 | ||
| Calorie Intake | Range | |||
| Quartile 1 | <1363 | Ref | Ref | |
| Quartile 2 | 1363 to <1603 | 1.11 (0.99–1.26) | 1.12 (0.98–1.27) | |
| Quartile 3 | 1603 to <1876 | 1.17 (1.03–1.34) | 1.19 (1.04–1.36) | |
| Quartile 4 | ≥1876 | 1.14 (1.00–1.30) | 1.17 (1.02–1.35) | |
| p for trend | 0.01 | 0.02 | ||
| PRAL (mEq/day) | Range | |||
| Quartile 1 | <−19.50 | Ref | Ref | |
| Quartile 2 | −19.50 to <−6.94 | 1.19 (1.05–1.34) | 1.16 (1.02–1.32) | |
| Quartile 3 | −6.94 to <3.22 | 1.29 (1.13–1.46) | 1.24 (1.09–1.42) | |
| Quartile 4 | ≥3.22 | 1.31 (1.15–1.50) | 1.21 (1.05–1.39) | |
| p for trend | <0.001 | 0.02 | ||
| NEAP (mEq/day) | Range | |||
| Quartile 1 | <28.44 | Ref | Ref | |
| Quartile 2 | 28.44 to <37.25 | 1.15 (1.02–1.30) | 1.13(1.00–1.29) | |
| Quartile 3 | 37.25 to <46.90 | 1.27 (1.11–1.44) | 1.22 (1.07–1.39) | |
| Quartile 4 | ≥46.90 | 1.24 (1.08–1.42) | 1.14 (1.00–1.32) | |
| p for trend | 0.004 | 0.16 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wu, T.; Arevalo, C.; Hsu, F.-C.; Hong, S.; Parada, H., Jr.; Yang, M.; Pierce, J.P. Independent and Joint Associations of Pessimism, Total Calorie Intake and Acid-Producing Diets with Insomnia Symptoms among Breast Cancer Survivors. J. Clin. Med. 2022, 11, 2828. https://doi.org/10.3390/jcm11102828
Wu T, Arevalo C, Hsu F-C, Hong S, Parada H Jr., Yang M, Pierce JP. Independent and Joint Associations of Pessimism, Total Calorie Intake and Acid-Producing Diets with Insomnia Symptoms among Breast Cancer Survivors. Journal of Clinical Medicine. 2022; 11(10):2828. https://doi.org/10.3390/jcm11102828
Chicago/Turabian StyleWu, Tianying, Cesar Arevalo, Fang-Chi Hsu, Suzi Hong, Humberto Parada, Jr., Mingan Yang, and John P. Pierce. 2022. "Independent and Joint Associations of Pessimism, Total Calorie Intake and Acid-Producing Diets with Insomnia Symptoms among Breast Cancer Survivors" Journal of Clinical Medicine 11, no. 10: 2828. https://doi.org/10.3390/jcm11102828