
Efficacy of 3 Tesla Functional Magnetic Stimulation for the Treatment of Female Urinary Incontinence

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
3. Statistical Analysis
4. Results
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Thomas, T.M.; Plymat, K.R.; Blannin, J.; Meade, T.W. Prevalence of urinary incontinence. BMJ 1980, 281, 1243–1245. [Google Scholar] [CrossRef] [Green Version]
- Norton, P.A. Prevalence and social impact of urinary incontinence in women. Clin. Obs. Gynecol. 1990, 33, 295–297. [Google Scholar] [CrossRef] [PubMed]
- Norton, P.A.; MacDonald, L.D.; Sedgwick, P.M.; Stanton, S.L. Distress and delay associated with urinary incontinence, frequency and urgency in women. BMJ 1998, 297, 1187–1189. [Google Scholar] [CrossRef] [Green Version]
- Nambiar, A.K.; Bosch, R.; Cruz, F.; Lemack, G.E.; Thiruchelvam, N.; Tubaro, A.; Bedretdinova, D.A.; Ambühl, D.; Farag, F.; Lombardo, R.; et al. EAU Guidelines on Assessment and Nonsurgical Management of Urinary Incontinence. Eur. Urol. 2018, 73, 596–609. [Google Scholar] [CrossRef]
- Galloway, N.T.M.; El-Galley, R.E.; Sand, P.K.; Appell, R.A.; Russell, H.W.; Carlan, S.J. Extracorporeal magnetic innervation therapy for stress urinary incontinence. Urology 1999, 53, 1108–1111. [Google Scholar] [CrossRef]
- Barker, A.T.; Freeston, I.L.; Jalinous, R.; Jarratt, J.A. Magnetic stimulation of the human brain and peripheral nervous system: An introduction and the results of an initial clinical evaluation. Neurosurgery 1987, 20, 100–109. [Google Scholar] [CrossRef] [PubMed]
- Lo, T.S.; Tseng, L.H.; Lin, Y.H.; Liang, C.C.; Lu, C.Y.; Pue, L.B. Effect of extracorporeal magnetic energy stimulation on bothersome lower urinary tract symptoms and quality of life in female patients with stress urinary incontinence and overactive bladder. J. Obstet. Gynaecol. Res. 2013, 39, 1526–1532. [Google Scholar] [CrossRef] [PubMed]
- Lukanović, D.; Kunič, T.; Batkoska, M.; Matjašič, M.; Barbič, M. Effectiveness of Magnetic Stimulation in the Treatment of Urinary Incontinence: A Systematic Review and Results of Our Study. J. Clin. Med. 2021, 10, 5210. [Google Scholar] [CrossRef] [PubMed]
- Haylen, B.T.; De Ridder, D.; Freeman, R.M.; Swift, S.E.; Berghmans, B.; Lee, J.; Monga, A.; Petri, E.; Rizk, D.E.; Sand, P.K.; et al. An International Urogynecological Association (IUGA)/International Continence Society (ICS) Joint Report on the Terminology for Female Pelvic Floor Dysfunction. Neurourol. Urodyn. 2010, 29, 4–20. [Google Scholar] [CrossRef] [PubMed]
- Fall, M.; Lindström, S. Functional electrical stimulation: Physiological basis and clinical principles. Review article. Int. Urogynecol. J. 1994, 5, 296–304. [Google Scholar] [CrossRef]
- Yalcin, I.; Bump, R.C. Validation of two global impression questionnaires for incontinence. Am. J. Obstet. Gynecol. 2003, 189, 98–101. [Google Scholar] [CrossRef] [PubMed]
- Campeau, L.; Tu, L.M.; Lemieux, M.C.; Naud, A.; Karsenty, G.; Schick, E.; Corcos, J. A multicenter, prospective, randomized clinical trial comparing tension-free vaginal tape surgery and no treatment for the management of stress urinary incontinence in elderly women. Neurourol. Urodyn. 2007, 26, 990–994. [Google Scholar] [CrossRef] [PubMed]
- Rosmini, F.; Ferrigno, L. Ethical aspects of epidemiological research. Istisan reports 15/44. In Epidemiology and Public Health; National Institute of Health: Rome, Italy, 2015; pp. 2384–8936. [Google Scholar]
- Samuels, J.B.; Pezzella, A.; Berenholz, J.; Alinsod, R. Safety and Efficacy of a Non-Invasive High-Intensity Focused Electromagnetic Field (HIFEM) Device for Treatment of Urinary Incontinence and Enhancement of Quality of Life. Lasers Surg. Med. 2019, 51, 760–766. [Google Scholar] [CrossRef] [PubMed]
- Weber-Rajek, M.; Strączyńska, A.; Strojek, K.; Piekorz, Z.; Pilarska, B.; Podhorecka, M.; Sobieralska-Michalak, K.; Goch, A.; Radzimińska, A. Assessment of the Effectiveness of Pelvic Floor Muscle Training (PFMT) and Extracorporeal Magnetic Innervation (ExMI) in Treatment of Stress Urinary Incontinence in Women: A Randomized Controlled Trial. BioMed Res. Int. 2020, 2020, 1019872. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Özengin, N.; Bakar, Y.; Özdemir, Ö.C.; Duran, B. The comparison of EMG-biofeedback and extracorporeal magnetic innervation treatments in women with urinary incontinence. Clin. Exp. Obstet. Gynecol. 2016, 43, 550–554. [Google Scholar] [CrossRef] [PubMed]
- Doğanay, M.; Kılıç, S.; Yılmaz, N. Long-term effects of extracorporeal magnetic innervations in the treatment of women withurinary incontinence: Results of 3-year follow-up. Arch. Gynecol. Obstet. 2010, 282, 49–53. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Programs | Frequency (Hz) | Time (s) | Pulsed Time (μs) | Active Time (s) | Passive Time (s) | Therapy Time (min) |
|---|---|---|---|---|---|---|
| SUI | 35 | 12 | 300 | 6 | 6 | 30 |
| OAB | 10 | 12 | 250 | 6 | 6 | 30 |
| Patients Characteristics | SUI (60) | OAB (40) | p Value |
|---|---|---|---|
| Age, yr, median, (IQR) | 52 (52–63) | 63 (63–72) | 0.06 |
| BMI, kg/m2, median, (IQR) | 26 (26–29) | 29 (29–30) | 0.23 |
| Menopausal, no. (%) | 24 (48) | 25 (83.3) | 0.05 |
| HRT, no. (%) | 4 (8) | 4 (13.3) | 0.71 |
| Previous vaginal deliveries, median, (IQR) | 1 (1–3) | 2 (1–3) | 0.88 |
| Macrosome, ≥4000 g, no. (%) | 2 (4) | 5 (16.7) | 0.11 |
| Operative delivery, vacuum/forceps, no. (%) | 3 (6) | 5 (16.7) | 0.22 |
| Cesarean delivery, no. (%) | 4 (8) | 2 (6.7) | 1.00 |
| Recurrent Urinary Tract Infection, no. (%) | 4 (8) | 2 (6.7) | 1.00 |
| Patients Symptoms | Cure Rate % (n/n) | Cure and Improvement Rate % (n/n) |
|---|---|---|
| SUI | 47 (28/60) | 68.3 (41/60) |
| OAB | 50 (20/40) | 70 (28/40) |
| p value 0.84 | p value 1.00 |
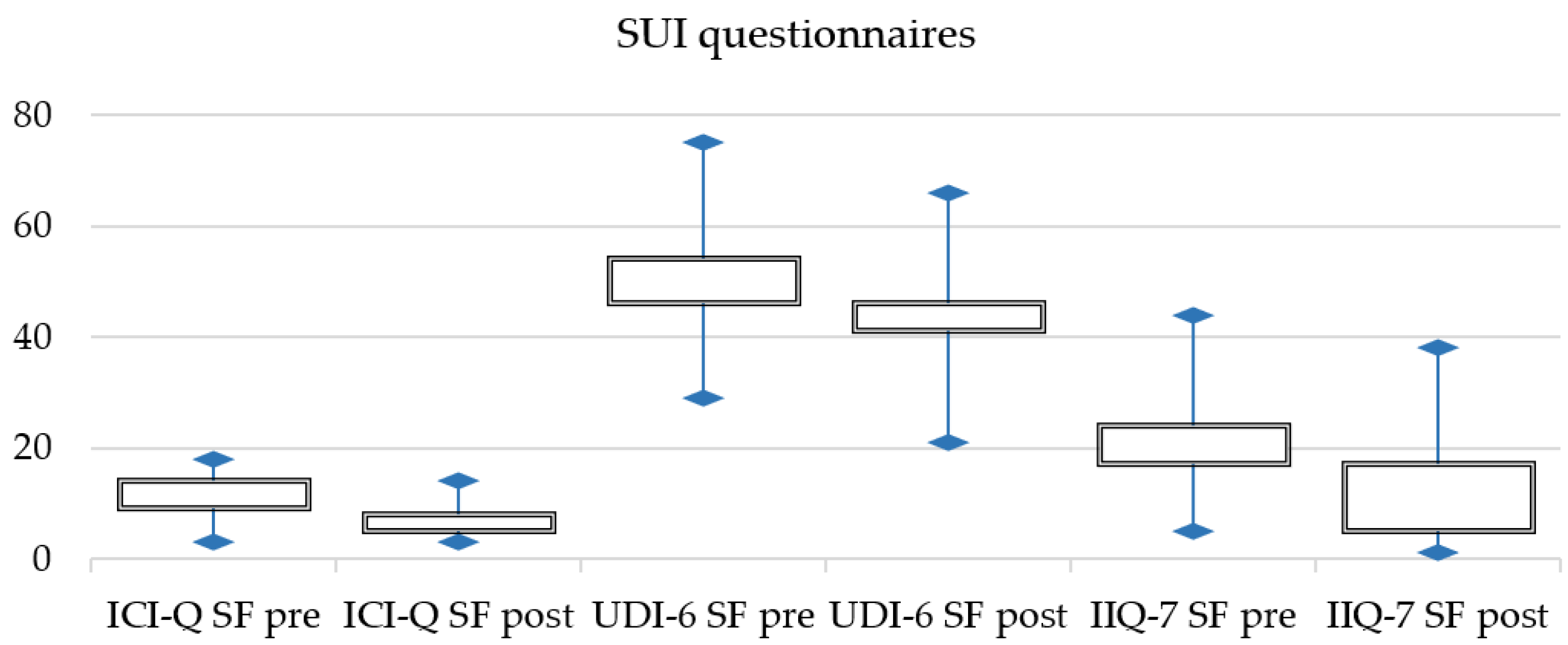
| Questionnaire | SUI Pre (m/IQR) | SUI Post (m/IQR) | p Value ** | OAB Pre (m/IQR) | OAB Post (m/IQR) | p Value ** |
|---|---|---|---|---|---|---|
| ICI-Q SF | 9 (9–14) | 5 (5–8) | 0.001 | 11 (10–13) | 6 (6–9) | 0.001 |
| UDI-6 SF | 46 (46–54) | 41 (41–46) | 0.001 | 50 (50–54) | 38 (38–42) | 0.001 |
| IIQ-7 SF | 17 (17–24) | 6 (5–17) | 0.001 | 17 (17–33) | 11 (11–17) | 0.001 |
| OAB-q SF | - | - | 48 (28–55) | 38 (38–53) | 0.001 |
| Characteristics | Cured (n = 28) | Not Cured (n = 32) | p Value ** |
|---|---|---|---|
| Age, year, median (IQR) | 49 (33–63) | 55 (45.5–67) | 0.21 |
| Menopause, n (%) | 15 (53.5) | 14 (43.7) | 0.60 |
| BMI, kg/m2, median (IQR) | 24.7 (21.8–30.1) | 24.6 (24.28–27.5) | 0.72 |
| UDI-6 SF pre, median (IQR) | 45.8 (41–56) | 47.9 (43.7–54) | 0.89 |
| ICIQ-SF pre, median (IQR) | 10 (7–14) | 12.5 (7–14.5) | 0.71 |
| IIQ-7 SF pre, median (IQR) | 16.5 (0–30) | 22 (11–38.2) | 0.25 |
| Characteristics | Cured (n = 20) | Not Cured (n = 20) | p Value ** |
|---|---|---|---|
| Age, year, median (IQR) | 56 (53–73) | 67.5 (51.5–73) | 0.66 |
| Menopause, n (%) | 5 (25) | 3 (15) | 0.69 |
| BMI, kg/m2, median (IQR) | 24.8 (24–29) | 29.3 (23.8–31.35) | 0.86 |
| UDI-6 SF pre, median (IQR) | 50 (44–62) | 45.8 (41.6–60) | 0.45 |
| ICIQ-SF pre, median (IQR) | 10 (8–15.5) | 10 (3.5–15) | 0.36 |
| IIQ-7 SF pre, median (IQR) | 16.5 (5.5–49.5) | 16.5 (14–58) | 0.79 |
| OAB-q SF pre, median (IQR) | 52 (48–67) | 46 (37.5–74) | 0.78 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Braga, A.; Castronovo, F.; Caccia, G.; Papadia, A.; Regusci, L.; Torella, M.; Salvatore, S.; Scancarello, C.; Ghezzi, F.; Serati, M. Efficacy of 3 Tesla Functional Magnetic Stimulation for the Treatment of Female Urinary Incontinence. J. Clin. Med. 2022, 11, 2805. https://doi.org/10.3390/jcm11102805
Braga A, Castronovo F, Caccia G, Papadia A, Regusci L, Torella M, Salvatore S, Scancarello C, Ghezzi F, Serati M. Efficacy of 3 Tesla Functional Magnetic Stimulation for the Treatment of Female Urinary Incontinence. Journal of Clinical Medicine. 2022; 11(10):2805. https://doi.org/10.3390/jcm11102805
Chicago/Turabian StyleBraga, Andrea, Fabiana Castronovo, Giorgio Caccia, Andrea Papadia, Luca Regusci, Marco Torella, Stefano Salvatore, Chiara Scancarello, Fabio Ghezzi, and Maurizio Serati. 2022. "Efficacy of 3 Tesla Functional Magnetic Stimulation for the Treatment of Female Urinary Incontinence" Journal of Clinical Medicine 11, no. 10: 2805. https://doi.org/10.3390/jcm11102805