
Design and Rationale of the Sevoflurane for Sedation in Acute Respiratory Distress Syndrome (SESAR) Randomized Controlled Trial

 , , , , , , and add
Show full author list
, , , , , , and add
Show full author list
Abstract
:1. Introduction
2. Materials and Methods
2.1. Objectives
- To examine the efficacy of inhaled sevoflurane versus intravenous propofol in improving a composite outcome of mortality and time off the ventilator at 28 days in ARDS.
- To evaluate the safety of inhaled sevoflurane in ARDS (clinical adverse events), to describe its effects on the duration of mechanical ventilation, organ dysfunction, the use of rescue procedures, ICU-acquired delirium, major clinical and long-term outcomes, and healthcare-related costs during ICU and hospital stay.
- To investigate the physiological and biological mechanisms of protection by inhaled sevoflurane in ARDS, if any, and their potential roles in heterogeneity of treatment effects.
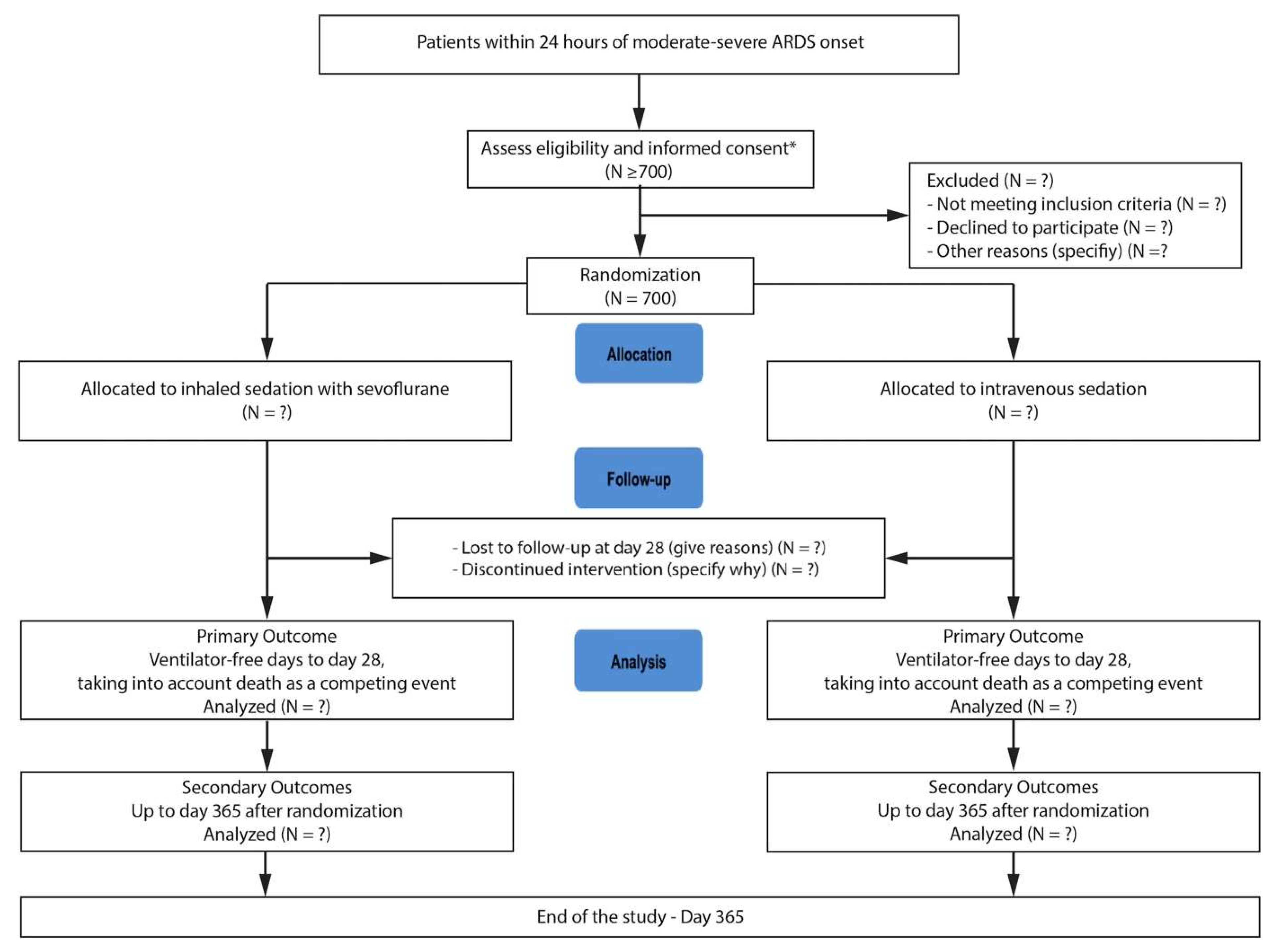
2.2. Trial Design
2.3. Eligibility Criteria and Exclusions
2.4. Randomization
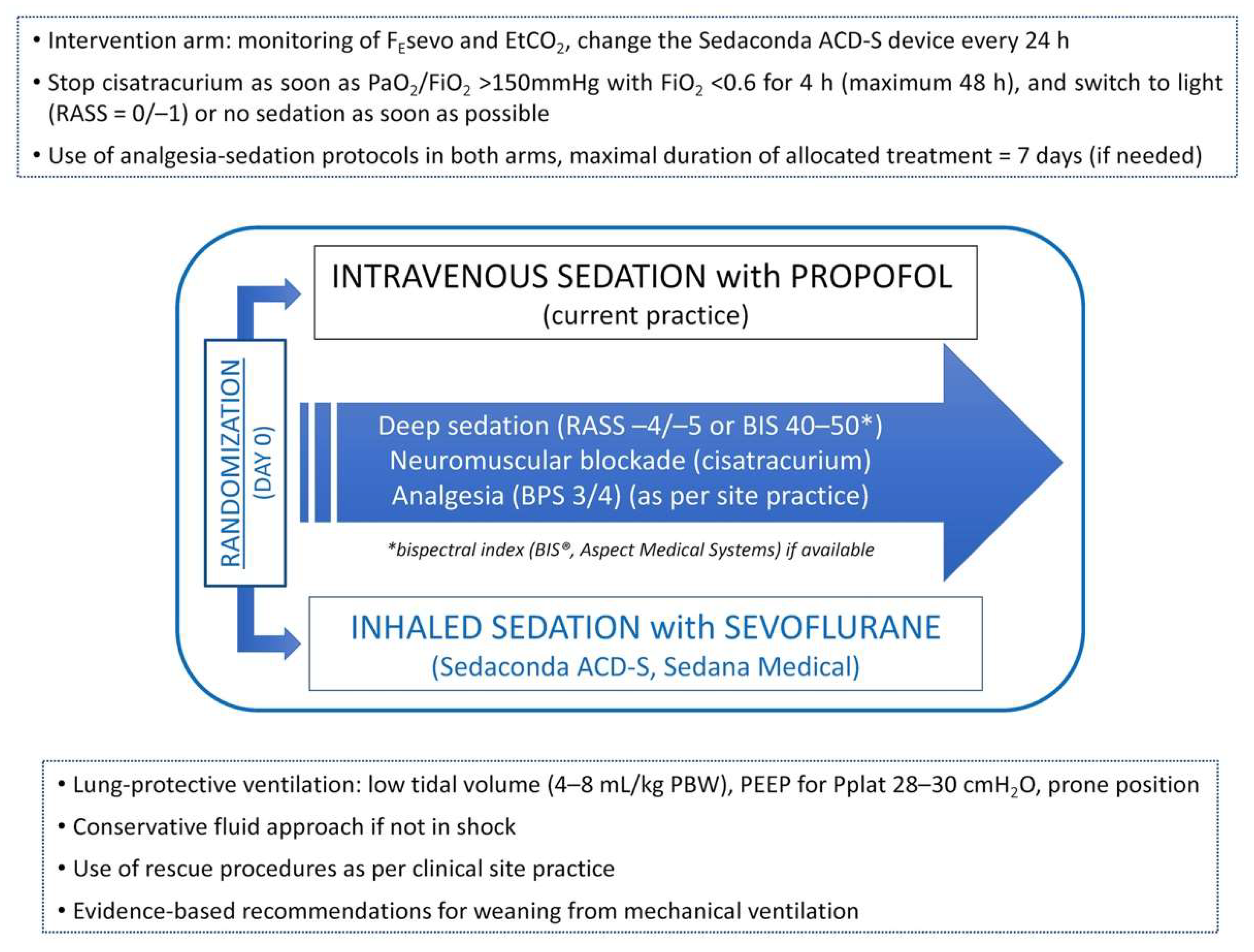
2.5. Treatment Arms, Administration, and Standardization of Care
2.5.1. Interventions
2.5.2. Study Arms: Intervention—Inhaled Sedation with Sevoflurane
2.5.3. Study Arms: Control—Intravenous Sedation with Propofol
2.5.4. Common Strategies for Both Groups
2.5.5. Standardization and Adherence
2.6. Patient Timeline, Assessments, and Measures
2.7. Trial Outcome Measures
2.7.1. Primary Outcome
2.7.2. Key Secondary Outcomes
2.7.3. Secondary Outcomes
2.7.4. Exploratory Outcomes
2.7.5. Exploratory Biological Outcomes
2.7.6. Safety Outcomes
2.8. Laboratory Evaluations
2.8.1. Safety Data
2.8.2. Data and Safety Monitoring
2.8.3. Statistical Considerations
2.8.4. Sample-Size Justification
3. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Soukup, J.; Schärff, K.; Kubosch, K.; Pohl, C.; Bomplitz, M.; Kompardt, J. State of the Art: Sedation Concepts with Volatile Anesthetics in Critically Ill Patients. J. Crit. Care 2009, 24, 535–544. [Google Scholar] [CrossRef] [PubMed]
- DAS-Taskforce 2015; Baron, R.; Binder, A.; Biniek, R.; Braune, S.; Buerkle, H.; Dall, P.; Demirakca, S.; Eckardt, R.; Eggers, V.; et al. Evidence and consensus based guideline for the management of delirium, analgesia, and sedation in intensive care medicine. Revision 2015 (DAS-Guideline 2015)-short version. Ger. Med. Sci. 2015, 13, 19. [Google Scholar]
- Jerath, A.; Parotto, M.; Wasowicz, M.; Ferguson, N.D. Volatile Anesthetics. Is a New Player Emerging in Critical Care Sedation? Am. J. Respir. Crit. Care Med. 2016, 193, 1202–1212. [Google Scholar] [CrossRef] [PubMed]
- Blondonnet, R.; Quinson, A.; Lambert, C.; Audard, J.; Godet, T.; Zhai, R.; Pereira, B.; Futier, E.; Bazin, J.-E.; Constantin, J.-M.; et al. Use of Volatile Agents for Sedation in the Intensive Care Unit: A National Survey in France. PLoS ONE 2021, 16, e0249889. [Google Scholar] [CrossRef] [PubMed]
- Meiser, A.; Volk, T.; Wallenborn, J.; Guenther, U.; Becher, T.; Bracht, H.; Schwarzkopf, K.; Knafelj, R.; Faltlhauser, A.; Thal, S.C.; et al. Inhaled Isoflurane via the Anaesthetic Conserving Device versus Propofol for Sedation of Invasively Ventilated Patients in Intensive Care Units in Germany and Slovenia: An Open-Label, Phase 3, Randomised Controlled, Non-Inferiority Trial. Lancet Respir. Med. 2021, 9, 1231–1240. [Google Scholar] [CrossRef]
- Ferrando, C.; Aguilar, G.; Piqueras, L.; Soro, M.; Moreno, J.; Belda, F.J. Sevoflurane, but Not Propofol, Reduces the Lung Inflammatory Response and Improves Oxygenation in an Acute Respiratory Distress Syndrome Model: A Randomised Laboratory Study. Eur. J. Anaesthesiol. 2013, 30, 455–463. [Google Scholar] [CrossRef]
- Voigtsberger, S.; Lachmann, R.A.; Leutert, A.C.; Schläpfer, M.; Booy, C.; Reyes, L.; Urner, M.; Schild, J.; Schimmer, R.C.; Beck-Schimmer, B. Sevoflurane Ameliorates Gas Exchange and Attenuates Lung Damage in Experimental Lipopolysaccharide-Induced Lung Injury. Anesthesiology 2009, 111, 1238–1248. [Google Scholar] [CrossRef] [Green Version]
- Schläpfer, M.; Leutert, A.C.; Voigtsberger, S.; Lachmann, R.A.; Booy, C.; Beck-Schimmer, B. Sevoflurane Reduces Severity of Acute Lung Injury Possibly by Impairing Formation of Alveolar Oedema. Clin. Exp. Immunol. 2012, 168, 125–134. [Google Scholar] [CrossRef] [Green Version]
- Suter, D.; Spahn, D.R.; Blumenthal, S.; Reyes, L.; Booy, C.; Z’graggen, B.R.; Beck-Schimmer, B. The Immunomodulatory Effect of Sevoflurane in Endotoxin-Injured Alveolar Epithelial Cells. Anesth. Analg. 2007, 104, 638–645. [Google Scholar] [CrossRef] [Green Version]
- Steurer, M.; Schläpfer, M.; Steurer, M.; Z’graggen, B.R.; Booy, C.; Reyes, L.; Spahn, D.R.; Beck-Schimmer, B. The Volatile Anaesthetic Sevoflurane Attenuates Lipopolysaccharide-Induced Injury in Alveolar Macrophages. Clin. Exp. Immunol. 2009, 155, 224–230. [Google Scholar] [CrossRef]
- O’Gara, B.; Talmor, D. Lung Protective Properties of the Volatile Anesthetics. Intensive Care Med. 2016, 42, 1487–1489. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mesnil, M.; Capdevila, X.; Bringuier, S.; Trine, P.-O.; Falquet, Y.; Charbit, J.; Roustan, J.-P.; Chanques, G.; Jaber, S. Long-Term Sedation in Intensive Care Unit: A Randomized Comparison between Inhaled Sevoflurane and Intravenous Propofol or Midazolam. Intensive Care Med. 2011, 37, 933–941. [Google Scholar] [CrossRef] [PubMed]
- Jerath, A.; Panckhurst, J.; Parotto, M.; Lightfoot, N.; Wasowicz, M.; Ferguson, N.D.; Steel, A.; Beattie, W.S. Safety and efficacy of volatile anesthetic agents compared with standard intravenous midazolam/propofol sedation in ventilated critical care patients: A meta-analysis and systematic review of prospective trials. Anesth. Analg. 2017, 124, 1190–1199. [Google Scholar] [CrossRef] [PubMed]
- Jabaudon, M.; Boucher, P.; Imhoff, E.; Chabanne, R.; Faure, J.-S.; Roszyk, L.; Thibault, S.; Blondonnet, R.; Clairefond, G.; Guérin, R.; et al. Sevoflurane for Sedation in Acute Respiratory Distress Syndrome. A Randomized Controlled Pilot Study. Am. J. Respir. Crit. Care Med. 2017, 195, 792–800. [Google Scholar] [CrossRef]
- Bourdeaux, D.; Sautou-Miranda, V.; Montagner, A.; Perbet, S.; Constantin, J.M.; Bazin, J.-E.; Chopineau, J. Simple Assay of Plasma Sevoflurane and Its Metabolite Hexafluoroisopropanol by Headspace GC–MS. J. Chromatogr. B 2010, 878, 45–50. [Google Scholar] [CrossRef]
- Chabanne, R.; Perbet, S.; Futier, E.; Ben Said, N.A.; Jaber, S.; Bazin, J.-E.; Pereira, B.; Constantin, J.-M. Impact of the Anesthetic Conserving Device on Respiratory Parameters and Work of Breathing in Critically Ill Patients under Light Sedation with Sevoflurane. Anesthesiology 2014, 121, 808–816. [Google Scholar] [CrossRef] [Green Version]
- Perbet, S.; Bourdeaux, D.; Sautou, V.; Pereira, B.; Chabanne, R.; Constantin, J.M.; Chopineau, J.; Bazin, J.E. A Pharmacokinetic Study of 48-Hour Sevoflurane Inhalation Using a Disposable Delivery System (AnaConDa®) in ICU Patients. Minerva Anestesiol. 2014, 80, 655–665. [Google Scholar]
- Chanques, G.; Constantin, J.-M.; Devlin, J.W.; Ely, E.W.; Fraser, G.L.; Gélinas, C.; Girard, T.D.; Guérin, C.; Jabaudon, M.; Jaber, S.; et al. Analgesia and Sedation in Patients with ARDS. Intensive Care Med. 2020, 46, 2342–2356. [Google Scholar] [CrossRef]
- ARDS Definition Task Force; Ranieri, V.M.; Rubenfeld, G.D.; Thompson, B.T.; Ferguson, N.D.; Caldwell, E.; Fan, E.; Camporota, L.; Slutsky, A.S. Acute Respiratory Distress Syndrome: The Berlin Definition. JAMA 2012, 307, 2526–2533. [Google Scholar]
- Papazian, L.; Forel, J.-M.; Gacouin, A.; Penot-Ragon, C.; Perrin, G.; Loundou, A.; Jaber, S.; Arnal, J.-M.; Perez, D.; Seghboyan, J.-M.; et al. Neuromuscular Blockers in Early Acute Respiratory Distress Syndrome. N. Engl. J. Med. 2010, 363, 1107–1116. [Google Scholar] [CrossRef] [Green Version]
- National Heart, Lung, and Blood Institute PETAL Clinical Trials Network; Moss, M.; Huang, D.T.; Brower, R.G.; Ferguson, N.D.; Ginde, A.A.; Gong, M.N.; Grissom, C.K.; Gundel, S.; Hayden, D.; et al. Early Neuromuscular Blockade in the Acute Respiratory Distress Syndrome. N. Engl. J. Med. 2019, 380, 1997–2008. [Google Scholar] [PubMed]
- Rice, T.W.; Wheeler, A.P.; Bernard, G.R.; Hayden, D.L.; Schoenfeld, D.A.; Ware, L.B. National Institutes of Health, National Heart, Lung, and Blood Institute ARDS Network. Comparison of the SpO2/FIO2 Ratio and the PaO2/FIO2 ratio in patients with acute lung injury or ARDS. Chest 2007, 132, 410–417. [Google Scholar] [CrossRef] [PubMed]
- Guérin, C.; Reignier, J.; Richard, J.-C.; Beuret, P.; Gacouin, A.; Boulain, T.; Mercier, E.; Badet, M.; Mercat, A.; Baudin, O.; et al. Prone Positioning in Severe Acute Respiratory Distress Syndrome. N. Engl. J. Med. 2013, 368, 2159–2168. [Google Scholar] [CrossRef] [PubMed]
- Constantin, J.-M.; Jabaudon, M.; Lefrant, J.-Y.; Jaber, S.; Quenot, J.-P.; Langeron, O.; Ferrandière, M.; Grelon, F.; Seguin, P.; Ichai, C.; et al. Personalised Mechanical Ventilation Tailored to Lung Morphology versus Low Positive End-Expiratory Pressure for Patients with Acute Respiratory Distress Syndrome in France (the LIVE Study): A Multicentre, Single-Blind, Randomised Controlled Trial. Lancet Respir. Med. 2019, 7, 870–880. [Google Scholar] [CrossRef]
- Acute Respiratory Distress Syndrome Network; Brower, R.G.; Matthay, M.A.; Morris, A.; Schoenfeld, D.; Thompson, B.T.; Wheeler, A. Ventilation with Lower Tidal Volumes as Compared with Traditional Tidal Volumes for Acute Lung Injury and the Acute Respiratory Distress Syndrome. N. Engl. J. Med. 2000, 342, 1301–1308. [Google Scholar]
- Fan, E.; Del Sorbo, L.; Goligher, E.C.; Hodgson, C.L.; Munshi, L.; Walkey, A.J.; Adhikari, N.K.J.; Amato, M.B.P.; Branson, R.; Brower, R.G.; et al. An Official American Thoracic Society/European Society of Intensive Care Medicine/Society of Critical Care Medicine Clinical Practice Guideline: Mechanical Ventilation in Adult Patients with Acute Respiratory Distress Syndrome. Am. J. Respir. Crit. Care Med. 2017, 195, 1253–1263. [Google Scholar] [CrossRef]
- Mercat, A.; Richard, J.-C.M.; Vielle, B.; Jaber, S.; Osman, D.; Diehl, J.-L.; Lefrant, J.-Y.; Prat, G.; Richecoeur, J.; Nieszkowska, A.; et al. Positive End-Expiratory Pressure Setting in Adults with Acute Lung Injury and Acute Respiratory Distress Syndrome: A Randomized Controlled Trial. JAMA 2008, 299, 646–655. [Google Scholar] [CrossRef] [Green Version]
- Grissom, C.K.F.; Hirshberg, E.L.M.S.; Dickerson, J.B.M.; Brown, S.M.M.S.; Lanspa, M.J.M.S.; Liu, K.D.; Schoenfeld, D.; Tidswell, M.; Hite, R.D.; Rock, P.; et al. Fluid management with a simplified conservative protocol for the acute respiratory distress syndrome*. Crit. Care Med. 2015, 43, 288–295. [Google Scholar] [CrossRef]
- Vincent, J.L.; Moreno, R.; Takala, J.; Willatts, S.; De Mendonça, A.; Bruining, H.; Reinhart, C.K.; Suter, P.M.; Thijs, L.G. The SOFA (Sepsis-Related Organ Failure Assessment) Score to Describe Organ Dysfunction/failure. On Behalf of the Working Group on Sepsis-Related Problems of the European Society of Intensive Care Medicine. Intensive Care Med. 1996, 22, 707–710. [Google Scholar] [CrossRef]
- Sinha, P.; Calfee, C.S.; Beitler, J.R.; Soni, N.; Ho, K.; Matthay, M.A.; Kallet, R.H. Physiologic Analysis and Clinical Performance of the Ventilatory Ratio in Acute Respiratory Distress Syndrome. Am. J. Respir. Crit. Care Med. 2019, 199, 333–341. [Google Scholar] [CrossRef]
- Famous, K.R.; Delucchi, K.; Ware, L.B.; Kangelaris, K.N.; Liu, K.D.; Thompson, B.T.; Calfee, C.S. ARDS Network Acute Respiratory Distress Syndrome Subphenotypes Respond Differently to Randomized Fluid Management Strategy. Am. J. Respir. Crit. Care Med. 2017, 195, 331–338. [Google Scholar] [CrossRef] [PubMed]
- Huang, D.T.; Angus, D.C.; Moss, M.; Thompson, B.T.; Ferguson, N.D.; Ginde, A.; Gong, M.N.; Gundel, S.; Hayden, D.L.; Hite, R.D.; et al. Design and Rationale of the Reevaluation of Systemic Early Neuromuscular Blockade Trial for Acute Respiratory Distress Syndrome. Ann. Am. Thorac. Soc. 2017, 14, 124–133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Calfee, C.S.; Gallagher, D.; Abbott, J.; Thompson, B.T.; Matthay, M.A. NHLBI ARDS Network Plasma Angiopoietin-2 in Clinical Acute Lung Injury: Prognostic and Pathogenetic Significance. Crit. Care Med. 2012, 40, 1731–1737. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Calfee, C.S.; Janz, D.R.; Bernard, G.R.; May, A.K.; Kangelaris, K.N.; Matthay, M.A.; Ware, L.B. Distinct molecular phenotypes of direct vs indirect ARDS in single-center and multicenter studies. Chest 2015, 147, 1539–1548. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Uchida, T.; Shirasawa, M.; Ware, L.B.; Kojima, K.; Hata, Y.; Makita, K.; Mednick, G.; Matthay, Z.A.; Matthay, M.A. Receptor for Advanced Glycation End-Products Is a Marker of Type I Cell Injury in Acute Lung Injury. Am. J. Respir. Crit. Care Med. 2006, 173, 1008–1015. [Google Scholar] [CrossRef] [Green Version]
- Jabaudon, M.; Blondonnet, R.; Roszyk, L.; Bouvier, D.; Audard, J.; Clairefond, G.; Fournier, M.; Marceau, G.; Déchelotte, P.; Pereira, B.; et al. Soluble Receptor for Advanced Glycation End-Products Predicts Impaired Alveolar Fluid Clearance in Acute Respiratory Distress Syndrome. Am. J. Respir. Crit. Care Med. 2015, 192, 191–199. [Google Scholar] [CrossRef]
- Vijayan, A.; Faubel, S.; Askenazi, D.J.; Cerda, J.; Fissell, W.H.; Heung, M.; Humphreys, B.D.; Koyner, J.L.; Liu, K.D.; Mour, G.; et al. Clinical Use of the Urine Biomarker [TIMP-2] × [IGFBP7] for Acute Kidney Injury Risk Assessment. Am. J. Kidney Dis. 2016, 68, 19–28. [Google Scholar] [CrossRef] [Green Version]
- McNeil, J.B.; Shaver, C.M.; Kerchberger, V.E.; Russell, D.W.; Grove, B.S.; Warren, M.A.; Wickersham, N.E.; Ware, L.B.; McDonald, W.H.; Bastarache, J.A. Novel Method for Noninvasive Sampling of the Distal Airspace in Acute Respiratory Distress Syndrome. Am. J. Respir. Crit. Care Med. 2018, 197, 1027–1035. [Google Scholar] [CrossRef]
- Tronche, P.-A.; Lalande, R.; Blondonnet, R.; Roszyk, L.; Zhai, R.; Morand, D.; Pereira, B.; Sapin, V.; Malinovsky, J.-M.; Mourvillier, B.; et al. Assessment of a Novel Method for Non-Invasive Sampling of the Distal Airspace in Acute Respiratory Distress Syndrome Patients Receiving Inhaled Sedation with Sevoflurane: The ANAISS Study Protocol. medRxiv 2020. [Google Scholar] [CrossRef]
- Khwaja, A. KDIGO Clinical Practice Guidelines for Acute Kidney Injury. Nephron Clin. Pract. 2012, 120, c179–c184. [Google Scholar] [CrossRef]
- Gordon Lan, K.K.; DeMets, D.L. Discrete sequential boundaries for clinical trials. Biometrika 1983, 70, 659–663. [Google Scholar] [CrossRef]
- Checkley, W.; Brower, R.G.; Muñoz, A.; NIH Acute Respiratory Distress Syndrome Network Investigators. Inference for Mutually Exclusive Competing Events through a Mixture of Generalized Gamma Distributions. Epidemiology 2010, 21, 557–565. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wan, X.; Wang, W.; Liu, J.; Tong, T. Estimating the Sample Mean and Standard Deviation from the Sample Size, Median, Range and/or Interquartile Range. BMC Med. Res. Methodol. 2014, 14, 135. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hozo, S.P.; Djulbegovic, B.; Hozo, I. Estimating the Mean and Variance from the Median, Range, and the Size of a Sample. BMC Med. Res. Methodol. 2005, 5, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beitler, J.R.; Sarge, T.; Banner-Goodspeed, V.M.; Gong, M.N.; Cook, D.; Novack, V.; Loring, S.H.; Talmor, D.; EPVent-2 Study Group. Effect of Titrating Positive End-Expiratory Pressure (PEEP) with an esophageal pressure-guided strategy vs an empirical high PEEP-Fio2 strategy on death and days free from mechanical ventilation among patients with acute respiratory distress syndrome: A randomized clinical trial. JAMA 2019, 321, 846–857. [Google Scholar] [PubMed] [Green Version]
- Matthay, M.A.; McAuley, D.F.; Ware, L.B. Clinical trials in acute respiratory distress syndrome: Challenges and opportunities. Lancet Respir. Med. 2017, 5, 524–534. [Google Scholar] [CrossRef]
- Ware, L.B.; Matthay, M.A.; Mebazaa, A. Designing an ARDS Trial for 2020 and beyond: Focus on Enrichment Strategies. Intensive Care Med. 2020, 46, 2153–2156. [Google Scholar] [CrossRef]
- Ely, E.W. The ABCDEF Bundle: Science and Philosophy of How ICU Liberation Serves Patients and Families. Crit. Care Med. 2017, 45, 321–330. [Google Scholar] [CrossRef] [Green Version]
- Devlin, J.W.; Skrobik, Y.; Gélinas, C.; Needham, D.M.; Slooter, A.J.C.; Pandharipande, P.P.; Watson, P.L.; Weinhouse, G.L.; Nunnally, M.E.; Rochwerg, B.; et al. Clinical Practice Guidelines for the Prevention and Management of Pain, Agitation/Sedation, Delirium, Immobility, and Sleep Disruption in Adult Patients in the ICU. Crit. Care Med. 2018, 46, e825–e873. [Google Scholar] [CrossRef] [Green Version]
- National Heart, Lung, and Blood Institute Acute Respiratory Distress Syndrome (ARDS) Clinical Trials Network; Wiedemann, H.P.; Wheeler, A.P.; Bernard, G.R.; Thompson, B.T.; Hayden, D.; de Boisblanc, B.; Connors, A.F.; Hite, R.D.; Harabin, A.L. Comparison of two fluid-management strategies in acute lung injury. N. Engl. J. Med. 2006, 354, 2564–2575. [Google Scholar] [CrossRef] [Green Version]
- Vignon, P.; Evrard, B.; Asfar, P.; Busana, M.; Calfee, C.S.; Coppola, S.; Demiselle, J.; Geri, G.; Jozwiak, M.; Martin, G.S.; et al. Fluid Administration and Monitoring in ARDS: Which Management? Intensive Care Med. 2020, 46, 2252–2264. [Google Scholar] [CrossRef] [PubMed]
- Qadir, N.; Bartz, R.R.; Cooter, M.L.; Hough, C.L.; Lanspa, M.J.; Banner-Goodspeed, V.M.; Chen, J.-T.; Giovanni, S.; Gomaa, D.; Sjoding, M.W.; et al. Variation in Early Management Practices in Moderate-to-Severe ARDS in the United States: The Severe ARDS: Generating Evidence Study. Chest 2021, 160, 1304–1315. [Google Scholar] [CrossRef] [PubMed]
- Hraiech, S.; Yoshida, T.; Annane, D.; Duggal, A.; Fanelli, V.; Gacouin, A.; Heunks, L.; Jaber, S.; Sottile, P.D.; Papazian, L. Myorelaxants in ARDS Patients. Intensive Care Med. 2020, 46, 2357–2372. [Google Scholar] [CrossRef]
- Brower, R.G.; Lanken, P.N.; MacIntyre, N.; Matthay, M.A.; Morris, A.; Ancukiewicz, M.; Schoenfeld, D.; Thompson, B.T.; National Heart, Lung, and Blood Institute ARDS Clinical Trials Network. Higher versus lower positive end-expiratory pressures in patients with the acute respiratory distress syndrome. N. Engl. J. Med. 2004, 351, 327–336. [Google Scholar] [PubMed] [Green Version]
- Herridge, M.S.; Moss, M.; Hough, C.L.; Hopkins, R.O.; Rice, T.W.; Bienvenu, O.J.; Azoulay, E. Recovery and Outcomes after the Acute Respiratory Distress Syndrome (ARDS) in Patients and Their Family Caregivers. Intensive Care Med. 2016, 42, 725–738. [Google Scholar] [CrossRef] [PubMed]
- Matthay, M.A.; Zemans, R.L.; Zimmerman, G.A.; Arabi, Y.M.; Beitler, J.R.; Mercat, A.; Herridge, M.; Randolph, A.G.; Calfee, C.S. Acute Respiratory Distress Syndrome. Nat. Rev. Dis. Primers 2019, 5, 18. [Google Scholar] [CrossRef]
- Englert, J.A.; Macias, A.A.; Amador-Munoz, D.; Pinilla Vera, M.; Isabelle, C.; Guan, J.; Magaoay, B.; Suarez Velandia, M.; Coronata, A.; Lee, A.; et al. Isoflurane Ameliorates Acute Lung Injury by Preserving Epithelial Tight Junction Integrity. Anesthesiology 2015, 123, 377–388. [Google Scholar] [CrossRef] [Green Version]
- Watanabe, K.; Iwahara, C.; Nakayama, H.; Iwabuchi, K.; Matsukawa, T.; Yokoyama, K.; Yamaguchi, K.; Kamiyama, Y.; Inada, E. Sevoflurane Suppresses Tumour Necrosis Factor-α-Induced Inflammatory Responses in Small Airway Epithelial Cells after Anoxia/reoxygenation. Br. J. Anaesth. 2013, 110, 637–645. [Google Scholar] [CrossRef] [Green Version]
- Beitler, J.R.; Goligher, E.C.; Schmidt, M.; Spieth, P.M.; Zanella, A.; Martin-Loeches, I.; Calfee, C.S.; Cavalcanti, A.B.; ARDSne(x)t Investigators. Personalized medicine for ARDS: The 2035 research agenda. Intensive Care Med. 2016, 42, 756–767. [Google Scholar] [CrossRef] [Green Version]
- Jabaudon, M.; Blondonnet, R.; Audard, J.; Fournet, M.; Godet, T.; Sapin, V.; Constantin, J.-M. Recent Directions in Personalised Acute Respiratory Distress Syndrome Medicine. Anaesth. Crit. Care Pain Med. 2018, 37, 251–258. [Google Scholar] [CrossRef]
- Sinha, P.; Calfee, C.S. Phenotypes in Acute Respiratory Distress Syndrome: Moving towards Precision Medicine. Curr. Opin. Crit. Care 2019, 25, 12–20. [Google Scholar] [CrossRef] [PubMed]
- Matthay, M.A.; Arabi, Y.M.; Siegel, E.R.; Ware, L.B.; Bos, L.D.J.; Sinha, P.; Beitler, J.R.; Wick, K.D.; Curley, M.A.Q.; Constantin, J.-M.; et al. Phenotypes and Personalized Medicine in the Acute Respiratory Distress Syndrome. Intensive Care Med. 2020, 46, 2136–2152. [Google Scholar] [CrossRef] [PubMed]
- Jerath, A.; Ferguson, N.D.; Cuthbertson, B. Inhalational Volatile-Based Sedation for COVID-19 Pneumonia and ARDS. Intensive Care Med. 2020, 46, 1563–1566. [Google Scholar] [CrossRef] [PubMed]
- Roberts, R.J.; Barletta, J.F.; Fong, J.J.; Schumaker, G.; Kuper, P.J.; Papadopoulos, S.; Yogaratnam, D.; Kendall, E.; Xamplas, R.; Gerlach, A.T.; et al. Incidence of Propofol-Related Infusion Syndrome in Critically Ill Adults: A Prospective, Multicenter Study. Crit. Care 2009, 13, R169. [Google Scholar] [CrossRef] [Green Version]
- L’her, E.; Dy, L.; Pili, R.; Prat, G.; Tonnelier, J.-M.; Lefevre, M.; Renault, A.; Boles, J.-M. Feasibility and Potential Cost/benefit of Routine Isoflurane Sedation Using an Anesthetic-Conserving Device: A Prospective Observational Study. Respir. Care 2008, 53, 1295–1303. [Google Scholar]
- Röhm, K.D.; Wolf, M.W.; Schöllhorn, T.; Schellhaass, A.; Boldt, J.; Piper, S.N. Short-Term Sevoflurane Sedation Using the Anaesthetic Conserving Device after Cardiothoracic Surgery. Intensive Care Med. 2008, 34, 1683–1689. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Inclusion criteria |
|
| Exclusion criteria |
|
| Primary outcome | Ventilator-free days through day 28 (VFD28), as defined as the number of days alive and off the ventilator at 28 days, thereby considering death as a competing event * |
| Key secondary outcome | 90 day survival (assessed on study day 91) |
| Secondary outcomes |
|
| Exploratory outcomes |
|
| Exploratory biological outcomes |
|
| Safety outcomes |
|
| Intention-to-treat population | All randomized patients except those who withdraw their consent for the use of data. |
| Per-protocol population #1 | All randomized patients except patients having one or more major protocol violations defined as:
|
| Per-protocol population #2 | All randomized patients except patients having one or more major protocol violations defined as:
|
| Subgroup populations |
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Blondonnet, R.; Simand, L.-A.; Vidal, P.; Borao, L.; Bourguignon, N.; Morand, D.; Bernard, L.; Roszyk, L.; Audard, J.; Godet, T.; et al. Design and Rationale of the Sevoflurane for Sedation in Acute Respiratory Distress Syndrome (SESAR) Randomized Controlled Trial. J. Clin. Med. 2022, 11, 2796. https://doi.org/10.3390/jcm11102796
Blondonnet R, Simand L-A, Vidal P, Borao L, Bourguignon N, Morand D, Bernard L, Roszyk L, Audard J, Godet T, et al. Design and Rationale of the Sevoflurane for Sedation in Acute Respiratory Distress Syndrome (SESAR) Randomized Controlled Trial. Journal of Clinical Medicine. 2022; 11(10):2796. https://doi.org/10.3390/jcm11102796
Chicago/Turabian StyleBlondonnet, Raiko, Laure-Anne Simand, Perine Vidal, Lucile Borao, Nathalie Bourguignon, Dominique Morand, Lise Bernard, Laurence Roszyk, Jules Audard, Thomas Godet, and et al. 2022. "Design and Rationale of the Sevoflurane for Sedation in Acute Respiratory Distress Syndrome (SESAR) Randomized Controlled Trial" Journal of Clinical Medicine 11, no. 10: 2796. https://doi.org/10.3390/jcm11102796