
The Feasibility of the Functional Listening Index—Paediatric (FLI-P®) for Young Children with Hearing Loss


Abstract
:1. Introduction
- Can the FLI-P be used successfully with all children with hearing loss attending an early intervention/clinical service?
- Do children’s individual FLI-P trajectories change over time as would be expected?
- Do the data for known groups show the expected differences (typical hearing versus hearing loss, bilateral versus unilateral hearing loss, presence of an additional disability to hearing, ANSD, age at diagnosis, type of device, level of loss, age of implant)?
2. Materials and Methods
2.1. Participants
2.2. Early Intervention (EI) Group
2.3. Typical Hearing (TH) Group
2.4. Procedures: EI Group
2.5. Procedures: TH Group
2.6. Definitions
2.7. Data Collection, Extraction and Validation
2.8. Data Analysis
3. Results
3.1. Use of the FLI-P in a Clinical/Educational Setting
3.2. Changes to Children’s Individual Scores over Time
3.2.1. Age of Implant
3.2.2. Developmental Need in Addition to Hearing Loss
3.2.3. Auditory Neuropathy Spectrum Disorder
3.3. Differences in Group Scores
3.3.1. TH Group/EI Group
3.3.2. Bilateral and Unilateral Hearing Loss
3.3.3. Additional Needs
3.3.4. Auditory Neuropathy Spectrum Disorder
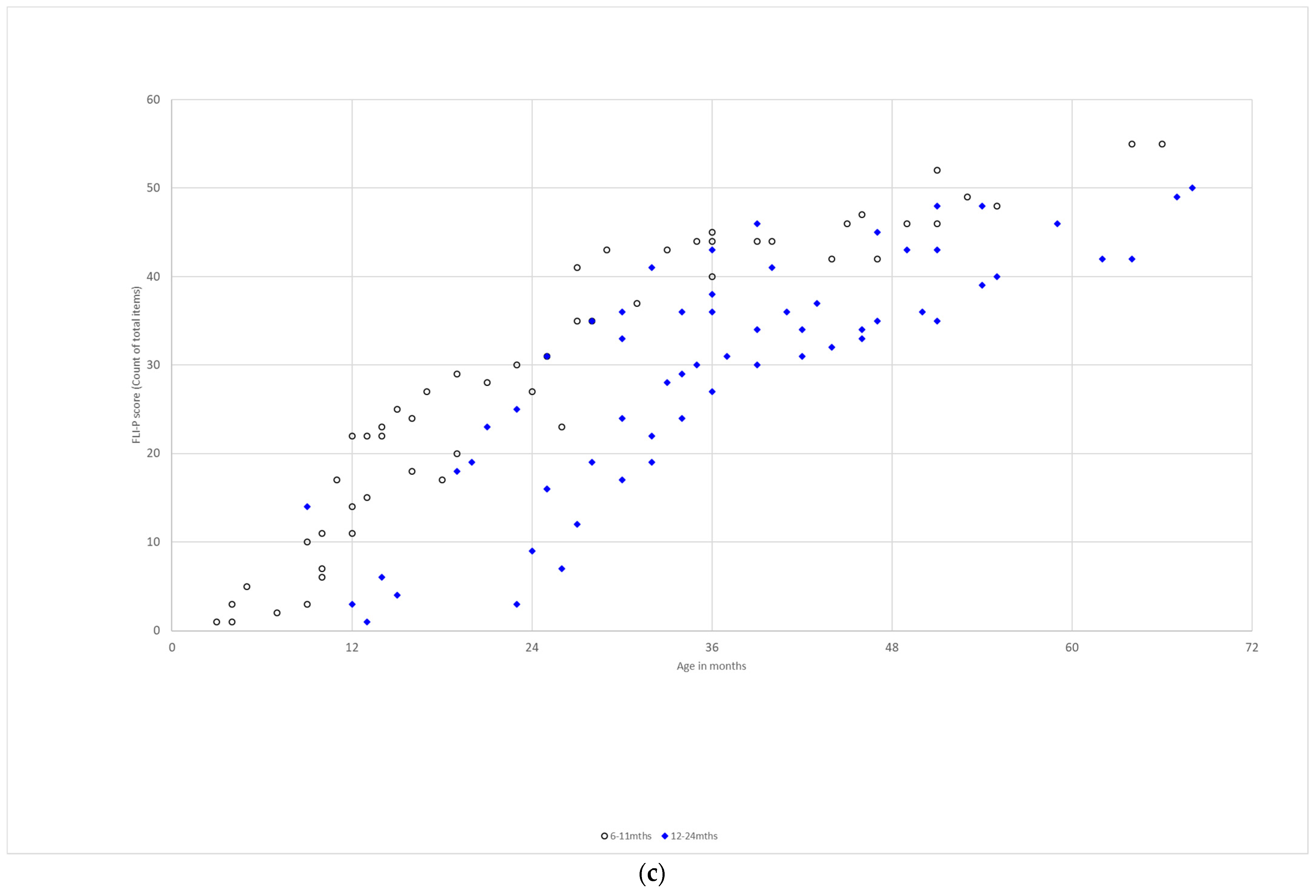
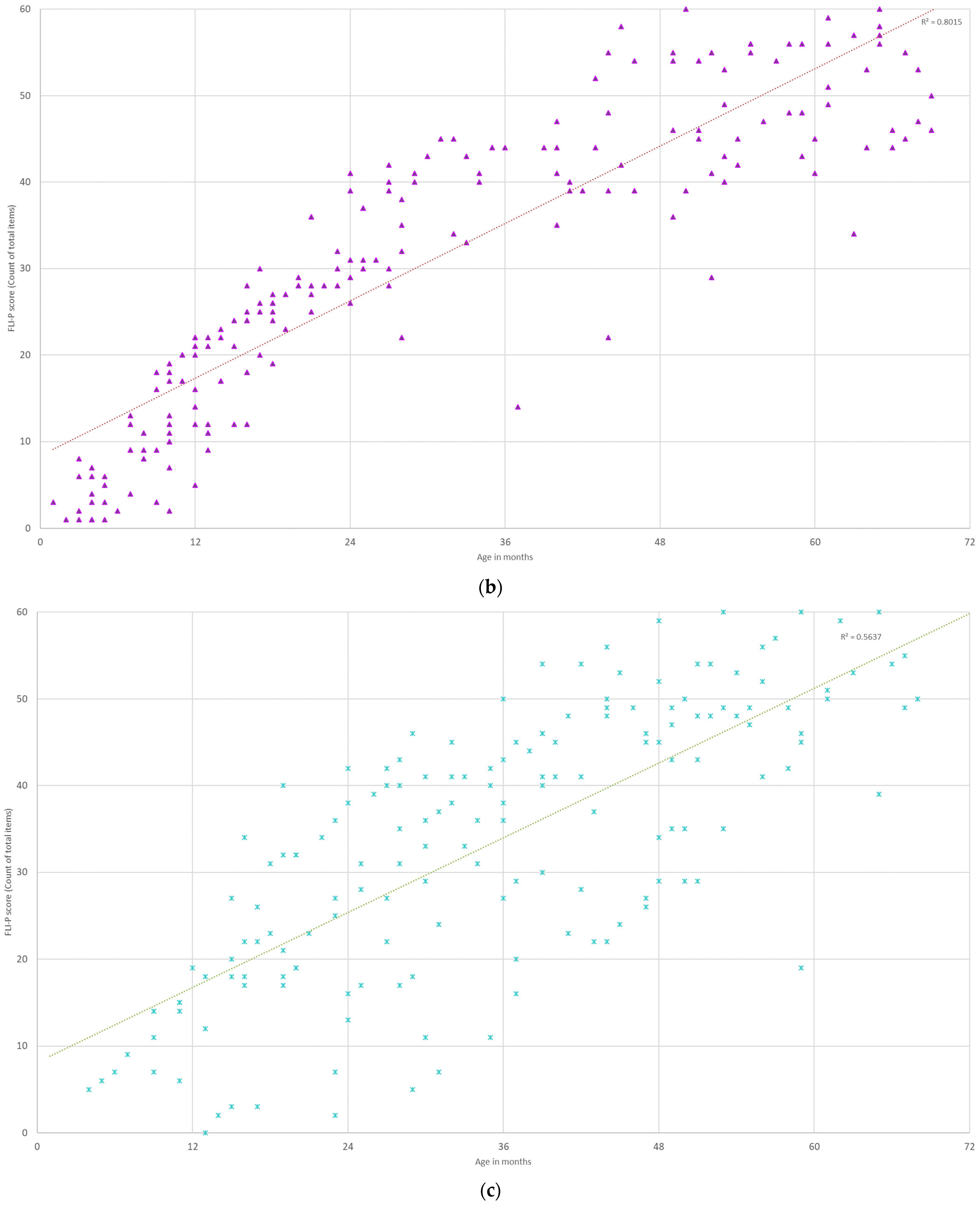
3.3.5. Age at Diagnosis
3.3.6. Type of Device
3.3.7. Level of Hearing Loss
3.3.8. Age at Implant
4. Discussion
- Whether the FLI-P could be used successfully with the entire population of children with hearing loss in a clinical/educational setting;
- If children’s individual FLI-P trajectories change with time as would be expected;
- If the data for known groups demonstrated the expected differences.
4.1. Use of the FLI-P in a Clinical/Education Setting
4.2. Changes to Children’s Individual Scores over Time
4.3. Differences in Group Scores
4.4. Clinical Implications and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Phase 1: Sound Awareness | |||
|---|---|---|---|
| 1.1. Jumps or startles to loud sounds | |||
| 1.2. Looks or smiles at me when I talk to them using a ‘sing-song’ voice | |||
| 1.3. Hears at least 3 or 4 different animal or transport noises when I make them | |||
| 1.4. Pays attention to talking, singing or music for 20–30 s, even when there is nothing to see | |||
| 1.5. Hears ALL of the “Ling 6” sounds when presented with emphasis | |||
| 1.6. Can work out where a sound is coming from | |||
| 1.7. Hears me when I whisper | |||
| Phase 2: Associating sound with meaning | |||
| 2.1. Makes sounds back to me when I talk to them | |||
| 2.2. Can tell the difference between talking and singing | |||
| 2.3. Knows the voices of 2 family members | |||
| 2.4. Recognizes a favorite song or music from the TV, tablet, or phone | |||
| 2.5. Pays attention and stays engaged through 2–3 nursery rhymes or with a favorite book | |||
| 2.6. Knows what some of the sounds around us are | |||
| 2.7. Looks at who is talking in a group | |||
| 2.8. Knows what is going to happen next in familiar songs | |||
| 2.9. Hears ALL the “Ling 6” sounds without looking at me when I am close and I say them in a normal voice close by | |||
| 2.10. Knows if someone is happy or angry from the sound of their voice | |||
| 2.11. Recognizes at least 3 songs or nursery rhymes when I sing them without the actions | |||
| Phase 3: Comprehending simple spoken language | |||
| 3.1. Repeats 3 familiar sounds after me | |||
| 3.2. Understands a word or phrase without any actions or gestures | |||
| 3.3. Matches 3 to 4 animals or objects with the sounds they make | |||
| 3.4. Knows their own name and will look at me when I say it | |||
| 3.5. Can give me one thing when I ask for it without pointing | |||
| 3.6. Repeats some of the words that I say | |||
| 3.7. Repeats ‘ah’, ‘oo’, ‘ee’, and ‘mm’ from the “Ling 6” sounds clearly after me | |||
| 3.8. Is able to tell the difference between ‘ss’ and ‘sh’ from the “Ling 6” sounds | |||
| 3.9. Says some of words in familiar songs | |||
| 3.10. Understands 10 words or phrases | |||
| 3.11. Knows the names of 3 familiar people or pets | |||
| 3.12. Hears me when I call their name in a noisy place | |||
| Phase 4: Comprehending language in different listening conditions | |||
| 4.1. Follows short directions that are unpredictable or silly | |||
| 4.2. Knows the actions for several different verses of a song | |||
| 4.3. Repeats a 2-to-3-word sentence | |||
| 4.4. Sings a line of a familiar song | |||
| 4.5. Can go and get two things that I ask for | |||
| 4.6. Follows 2 instructions when given in the same sentence | |||
| 4.7. Repeats all of the “Ling 6” sounds accurately | |||
| 4.8. Repeats words and phrases they have heard on the TV, tablet, or phone | |||
| 4.9. Repeats most of the sounds I say | |||
| 4.10. When I am more than 3 m away, they can accurately repeat all of “Ling 6” sounds after me | |||
| 4.11. Follows instructions or answers questions they have heard on the TV, tablet, or phone | |||
| Phase 5: Listening through discourse and narratives | |||
| 5.1. Recognizes a familiar person on the phone | |||
| 5.2. Says things that surprise me as I don’t know where they heard it | |||
| 5.3. Guesses which item I am talking about when I describe something that they can see | |||
| 5.4. Can find a page in a familiar book if I describe what is on it | |||
| 5.5. Is able to sing or say most of a familiar nursery rhyme or song | |||
| 5.6. Can answer simple questions about a favorite toy or activity | |||
| 5.7. Hears differences in similar sounding words and understands that this changes their meaning | |||
| 5.8. Will fetch 3 things at once if I ask for them | |||
| 5.9. Has a short conversation with me if I start it by telling them what we are talking about | |||
| 5.10. Follows 3 instructions in the same sentence | |||
| 5.11. Guesses what I’m describing from clues when I describe an object or an animal they know | |||
| 5.12. Accurately repeats sentences of 5 to 6 words after me if they know all the words | |||
| 5.13. Is able to tell me how 3 or 4 things are related when I name them | |||
| 5.14. Brings back 4 things that I ask for in one sentence | |||
| Phase 6: Advanced open set listening | |||
| 6.1. Can have a simple conversation with a familiar person on the phone | |||
| 6.2. Guesses a less familiar item from clues that I give | |||
| 6.3. Remembers 4 things that happened in a story in the right order after reading a book together | |||
| 6.4. Easily repeats a sentence of 8 to 10 words after me, even when one or two of the words are new to them | |||
| 6.5. Understands that the way something is said changes the meaning of the sentence | |||
| 6.6. Is able to follow a long, complicated instruction that has more than 5 components | |||
| 6.7. Easily repeats a sentence of 8 to 10 words they have heard on the TV, tablet, or phone, even when one or two of the words are new to them | |||
| 6.8. Follows instructions, has a conversation or can listen to a story and answers questions about it when we are in a noisy place | |||
| 6.9. When we’re somewhere noisy, they can have a conversation on the phone, or they can listen to a story on a digital device and answer questions or tell you about it | |||
References
- Pinker, S. The Language Instinct: How the Mind Creates Language; Penguin: London, UK, 2003. [Google Scholar]
- Ching, T.Y.; Dillon, H.; Leigh, G.; Cupples, L. Learning from the Longitudinal Outcomes of Children with Hearing Impairment (LOCHI) study: Summary of 5-year findings and implications. Int. J. Audiol. 2018, 57 (Suppl. 2), S105–S111. [Google Scholar] [CrossRef] [PubMed]
- Lederberg, A.R.; Schick, B.; Spencer, P.E. Language and literacy development of deaf and hard-of-hearing children: Successes and challenges. Dev. Psychol. 2013, 49, 15–30. [Google Scholar] [CrossRef] [PubMed]
- Yoshinaga-Itano, C. Early intervention after universal neonatal hearing screening: Impact on outcomes. Ment. Retard. Dev. Disabil. Res. Rev. 2003, 9, 252–266. [Google Scholar] [CrossRef] [PubMed]
- Nott, P.; Cowan, R.; Brown, P.M.; Wigglesworth, G. Early language development in children with profound hearing loss fitted with a device at a young age: Part II—Content of the first lexicon. Ear Hear. 2009, 30, 541–551. [Google Scholar] [CrossRef]
- Carvill, S. Sensory impairments, intellectual disability and psychiatry. J. Intellect. Disabil. Res. 2001, 45, 467–483. [Google Scholar] [CrossRef] [Green Version]
- Mohr, P.E.; Feldman, J.J.; Dunbar, J.L.; McConkey-Robbins, A.; Niparko, J.K.; Rittenhouse, R.K.; Skinner, M.W. The societal costs of severe to profound hearing loss in the United States. Int. J. Technol. Assess. Health Care 2000, 16, 1120–1135. [Google Scholar] [CrossRef]
- Erber, N.P. Auditory Training; Alexander Graham Bell Association for the Deaf: Washington, DC, USA, 1982. [Google Scholar]
- Scollie, S.D.; Ching, T.Y.; Seewald, R.C.; Dillon, H.; Britton, L.; Steinberg, J.; King, K. Children’s speech perception and loudness ratings when fitted with hearing aids using the DSL v. 4.1 and the NAL-NL1 prescriptions. Int. J. Audiol. 2010, 49 (Suppl. 1), S26–S34. [Google Scholar] [CrossRef]
- Vandali, A.E.; van Hoesel, R.J. Development of a temporal fundamental frequency coding strategy for cochlear implants. J. Acoust. Soc. Am. 2011, 129, 4023–4036. [Google Scholar] [CrossRef]
- Joint Committee on Infant Hearing; Muse, C.; Harrison, J.; Yoshinaga-Itano, C.; Grimes, A.; Brookhouser, P.E.; Epstein, S.; Buchman, C.; Mehl, A.; Vohr, B.; et al. Supplement to the JCIH 2007 position statement: Principles and guidelines for early intervention after confirmation that a child is deaf or hard of hearing [Practice Guideline]. Pediatrics 2013, 131, e1324–e1349. [Google Scholar]
- Olusanya, B.O.; Davis, A.C.; Hoffman, H.J. Hearing loss grades and the International classification of functioning, disability and health. B. World Health Organ. 2019, 97, 725–728. [Google Scholar] [CrossRef]
- Semel, E.M.; Wiig, E.H.; Secord, W. Clinical Evaluation of Language Fundamentals, fourth Edition (CELF-4); PsychCorp: Toronto, ON, Canada, 2004. [Google Scholar]
- Clark, J.G. Uses and abuses of hearing loss classification. ASHA 1981, 23, 493–500. [Google Scholar] [PubMed]
- Goodman, A. Reference zero levels for pure-tone audiometer. ASHA 1965, 7, 1. [Google Scholar]
- Krishnan, L.A.; Van Hyfte, S. Management of unilateral hearing loss. Int. J. Pediatr. Otorhinolaryngol. 2016, 88, 63–73. [Google Scholar] [CrossRef] [PubMed]
- Lieu, J.E.C. Speech-Language and Educational Consequences of Unilateral Hearing Loss in Children. Arch. Otolaryngol. Head Neck Surg. 2004, 130, 524–530. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lieu, J.E.C. Unilateral hearing loss in children: Speech-language and school performance. B-ENT 2013, 9 (Suppl. 21), 107–115. [Google Scholar]
- Bess, F.H.; Tharpe, A.M.; Gibler, A.M. Auditory Performance of Children with Unilateral Sensorineural Hearing Loss. Ear Hear. 1986, 7, 20–26. [Google Scholar] [CrossRef]
- Oyler, R.; McKay, S. Unilateral hearing loss in children: Challenges and opportunities. ASHA Lead. 2008, 13, 12–15. [Google Scholar] [CrossRef]
- Birman, C.S.; Elliott, E.J.; Gibson, W.P. Pediatric cochlear implants: Additional disabilities prevalence, risk factors, and effect on language outcomes. Otol. Neurotol. 2012, 33, 1347–1352. [Google Scholar] [CrossRef]
- Cupples, L.; Ching, T.Y.; Button, L.; Leigh, G.; Marnane, V.; Whitfield, J.; Gunnourie, M.; Martin, L. Language and speech outcomes of children with hearing loss and additional disabilities: Identifying the variables that influence performance at five years of age. Int. J. Audiol. 2018, 57 (Suppl. 2), S93–S104. [Google Scholar] [CrossRef]
- Breneman, A.I.; Gifford, R.H.; DeJong, M.D. Cochlear Implantation in Children with Auditory Neuropathy Spectrum Disorder: Long-Term Outcomes. J. Am. Acad. Audiol. 2012, 23, 5–17. [Google Scholar] [CrossRef]
- Harrison, R.V.; Gordon, K.A.; Papsin, B.C.; Negandhi, J.; James, A.L. Auditory neuropathy spectrum disorder (ANSD) and cochlear implantation. Int. J. Pediatr. Otorhinolaryngol. 2015, 79, 1980–1987. [Google Scholar] [CrossRef] [PubMed]
- Teagle, H.F.; Roush, P.A.; Woodard, J.S.; Hatch, D.R.; Zdanski, C.J.; Buss, E.; Buchman, C.A. Cochlear Implantation in Children with Auditory Neuropathy Spectrum Disorder. Ear Hear. 2010, 31, 325–335. [Google Scholar] [CrossRef] [PubMed]
- Ching, T.Y.C.; Day, J.; Dillon, H.; Gardner-Berry, K.; Hou, S.; Seeto, M.; Wong, A.; Zhang, V. Impact of the presence of auditory neuropathy spectrum disorder (ANSD) on outcomes of children at three years of age. Int. J. Audiol. 2013, 52 (Suppl. 2), S55–S64. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blaiser, K. Supporting Communicative Development of Infants and Toddlers with Hearing Loss. Semin. Speech Lang. 2012, 33, 273–279. [Google Scholar] [CrossRef] [PubMed]
- White, K.R. The evolution of EHDI: From concept to standard of care. In A Resource Guide for Early Hearing Detection and Intervention; National Center for Hearing Assessment and Management: Logan, UT, USA, 2014. [Google Scholar]
- Yoshinaga-Itano, C.; Coulter, D.; Thomson, V. The Colorado Newborn Hearing Screening Project: Effects on speech and language development for children with hearing loss. J. Perinatol. 2000, 20, S132–S137. [Google Scholar] [CrossRef]
- Sininger, Y.S.; Grimes, A.; Christensen, E. Auditory development in early amplified children: Factors influencing auditory-based communication outcomes in children with hearing loss. Ear Hear. 2010, 31, 166–185. [Google Scholar] [CrossRef] [Green Version]
- Tomblin, J.B.; Harrison, M.; Ambrose, S.E.; Walker, E.A.; Oleson, J.J.; Moeller, M.P. Language Outcomes in Young Children with Mild to Severe Hearing Loss. Ear Hear. 2015, 36 (Suppl. 1), 76S–91S. [Google Scholar] [CrossRef] [Green Version]
- Fulcher, A.; Purcell, A.A.; Baker, E.; Munro, N. Listen up: Children with early identified hearing loss achieve age-appropriate speech/language outcomes by 3years-of-age. Int. J. Pediatr. Otorhinolaryngol. 2012, 76, 1785–1794. [Google Scholar] [CrossRef]
- Leigh, J.; Dettman, S.; Dowell, R.; Briggs, R. Communication Development in Children Who Receive a Cochlear Implant by 12 Months of Age. Otol. Neurotol. 2013, 34, 443–450. [Google Scholar] [CrossRef]
- Percy-Smith, L.; Busch, G.; Sandahl, M.; Nissen, L.; Josvassen, J.L.; Lange, T.; Rusch, E.; Cayé-Thomasen, P. Language understanding and vocabulary of early cochlear implanted children. Int. J. Pediatr. Otorhinolaryngol. 2013, 77, 184–188. [Google Scholar] [CrossRef]
- Cowan, R.S.C.; Edwards, B.; Ching, T.Y.C. Longitudinal outcomes of children with hearing impairment (LOCHI): 5 year data. Int. J. Audiol. 2018, 57 (Suppl. 2), S1–S2. [Google Scholar] [CrossRef] [PubMed]
- Geers, A.; Brenner, C.; Davidson, L. Factors Associated with Development of Speech Perception Skills in Children Implanted by Age Five. Ear Hear. 2003, 24, 24S–35S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Geers, A.E.; Nicholas, J.; Moog, J.S. Estimating the influence of cochlear implantation on language development in children. Audiol. Med. 2007, 5, 262–273. [Google Scholar] [CrossRef]
- Niparko, J.K.; Tobey, E.A.; Thal, D.J.; Eisenberg, L.S.; Wang, N.-Y.; Quittner, A.L.; Fink, N.E.; Team, C.I. Spoken language development in children following cochlear implantation. J. Am. Med. Assoc. 2010, 303, 1498–1506. [Google Scholar] [CrossRef] [PubMed] [Green Version]






















| EI Group | Characteristic | Number of Children |
|---|---|---|
| Gender | Male | 285 |
| Female | 258 | |
| Symmetry of hearing loss (HL) | Bilateral | 385 |
| Unilateral | 140 | |
| Unknown | 18 | |
| Presence of additional needs that impact on learning | Yes | 92 |
| No | 451 | |
| Newborn Hearing Screening | Pass | 54 |
| Refer | 427 | |
| Not tested | 19 | |
| Unknown | 43 | |
| Age at diagnosis (months) | <3 | 380 |
| 3–6 | 23 | |
| 7–11 | 15 | |
| 12–23 | 37 | |
| 24–36 | 23 | |
| >36 | 33 | |
| Unknown | 32 | |
| Age at first device fitting (months) | <3 | 177 |
| 3–6 | 73 | |
| 7–11 | 34 | |
| 12–23 | 81 | |
| 24–36 | 44 | |
| >36 | 51 | |
| Unknown | 83 | |
| Age at entry to EI (months) | <3 | 168 |
| 3–6 | 96 | |
| 7–11 | 70 | |
| 12–23 | 86 | |
| 24–36 | 53 | |
| >36 | 70 | |
| Unknown | 0 |
| Left | ||||||
|---|---|---|---|---|---|---|
| Conductive | Sensorineural | Mixed | Unknown | * ANSD | ||
| Right | Conductive | 23 (88) | 3 (23) | 1 (2) | n/a | n/a |
| Sensorineural | 1 (3) | 286 (1616) | 2 (6) | 1 (1) | 2 (5) | |
| Mixed | 2 (20) | 3 (6) | 24 (138) | 1 (1) | n/a | |
| Unknown | n/a | n/a | n/a | 15 (45) | n/a | |
| ANSD | n/a | 1 (6) | n/a | n/a | 13 (127) | |
| Normal | n/a | 4 (19) | n/a | n/a | n/a | |
| EI Group | Type | Number of Children |
|---|---|---|
| Left | Conductive | 14 |
| Sensorineural | 37 | |
| Mixed | 5 | |
| Unknown | 1 | |
| Auditory Neuropathy Spectrum Disorder | 11 | |
| Right | Conductive | 26 |
| Sensorineural | 29 | |
| Mixed | 7 | |
| Unknown | 1 | |
| Auditory Neuropathy Spectrum Disorder | 9 |
| EI Group | Type | Number of Children |
|---|---|---|
| Left | Cochlear implant | 138 |
| Hearing aid | 218 | |
| Bone conduction device | 13 | |
| Unknown | 14 | |
| Unaided | 1 | |
| Right | Cochlear implant | 146 |
| Hearing aid | 215 | |
| Bone conduction device | 9 | |
| Unknown | 15 | |
| Unaided | 0 |
| EI Group | Type | Number of Children |
|---|---|---|
| Left | Cochlear implant | 11 |
| Hearing aid | 15 | |
| Bone conduction device | 15 | |
| Unknown | 30 | |
| Right | Cochlear implant | 10 |
| Hearing aid | 18 | |
| Bone conduction device | 21 | |
| Unknown | 31 |
| EI Group | Type | Number of Children |
|---|---|---|
| Left | Normal | 81 |
| High frequency | 8 | |
| Mild | 52 | |
| Mild–moderate to profound | 106 | |
| Mod–moderate/severe to profound | 122 | |
| Severe, severe–profound | 58 | |
| Profound | 80 | |
| Unknown | 36 | |
| Right | Normal | 70 |
| High frequency | 8 | |
| Mild | 50 | |
| Mild–moderate to profound | 115 | |
| Mod–moderate/severe to profound | 128 | |
| Severe, severe–profound | 49 | |
| Profound | 85 | |
| Unknown | 38 |
| EI Group | Type | Number of Children |
|---|---|---|
| Normal | 70 | |
| High frequency | 1 | |
| Mild | 6 | |
| Mild–moderate to profound | 6 | |
| Mod–moderate/severe to profound | 25 | |
| Severe, severe–profound | 19 | |
| Profound | 9 | |
| Unknown | 4 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Davis, A.; Harrison, E.; Cowan, R. The Feasibility of the Functional Listening Index—Paediatric (FLI-P®) for Young Children with Hearing Loss. J. Clin. Med. 2022, 11, 2764. https://doi.org/10.3390/jcm11102764
Davis A, Harrison E, Cowan R. The Feasibility of the Functional Listening Index—Paediatric (FLI-P®) for Young Children with Hearing Loss. Journal of Clinical Medicine. 2022; 11(10):2764. https://doi.org/10.3390/jcm11102764
Chicago/Turabian StyleDavis, Aleisha, Elisabeth Harrison, and Robert Cowan. 2022. "The Feasibility of the Functional Listening Index—Paediatric (FLI-P®) for Young Children with Hearing Loss" Journal of Clinical Medicine 11, no. 10: 2764. https://doi.org/10.3390/jcm11102764