
Sclerobanding (Combined Rubber Band Ligation with 3% Polidocanol Foam Sclerotherapy) for the Treatment of Second- and Third-Degree Hemorrhoidal Disease: Feasibility and Short-Term Outcomes

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
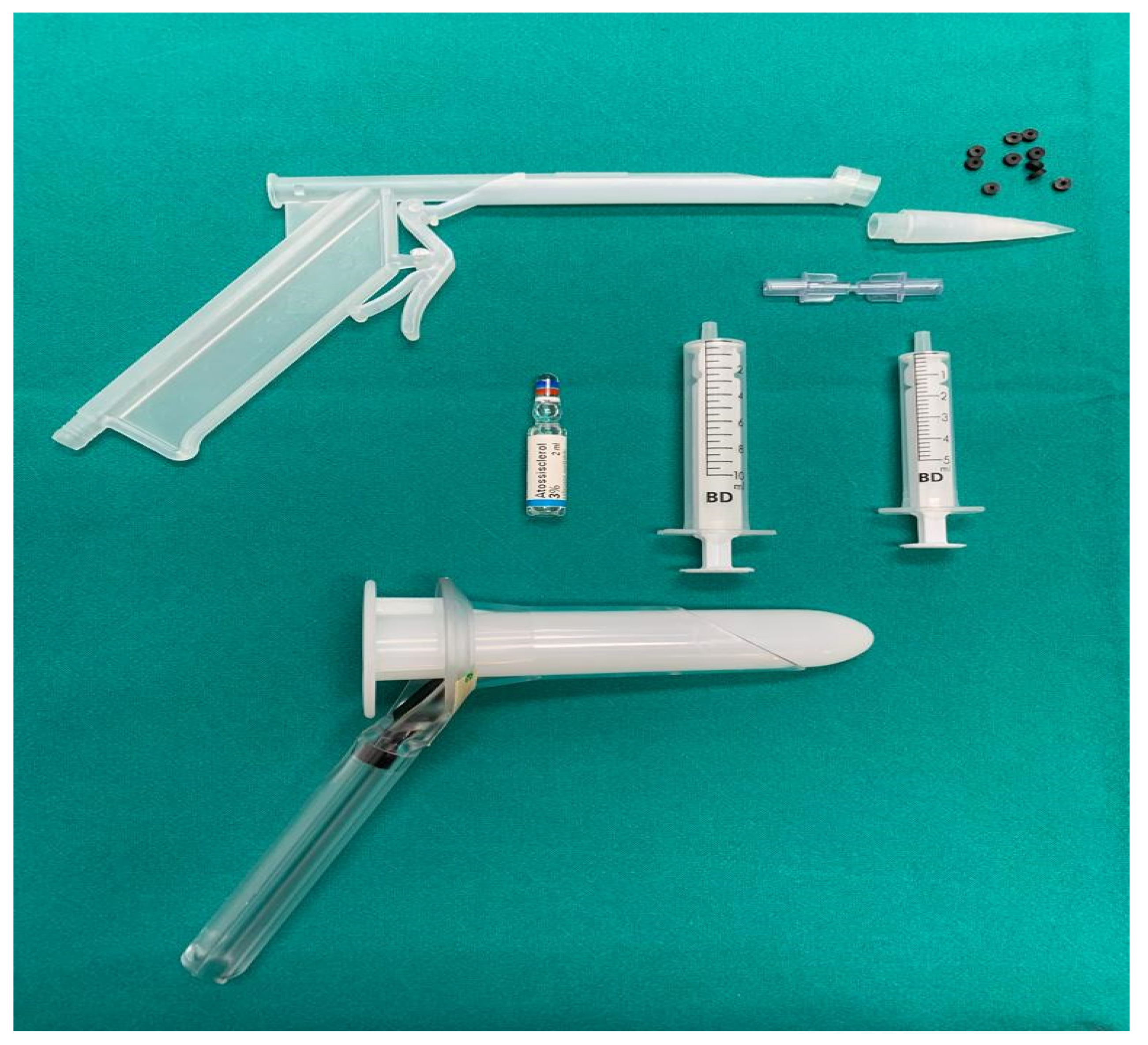
2.1. Surgical Technique
2.2. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Watson, A.J.; Hudson, J.; Wood, J.; Kilonzo, M.; Brown, S.R.; McDonald, A.; Norrie, J.; Bruhn, H.; Cook, J.A.; eTHoS Study Group. Comparison of stapled haemorrhoidopexy with traditional excisional surgery for haemorrhoidal disease (eTHoS): A pragmatic, multicentre, randomised controlled trial. Lancet 2016, 388, 2375–2385, Erratum in Lancet 2016, 388, 2354. [Google Scholar] [CrossRef]
- Aly, E.H. Stapled haemorrhoidopexy: Is it time to move on? Ann. R. Coll. Surg. Engl. 2015, 97, 490–493. [Google Scholar] [CrossRef]
- Gallo, G.; Martellucci, J.; Sturiale, A.; Clerico, G.; Milito, G.; Marino, F.; Cocorullo, G.; Giordano, P.; Mistrangelo, M.; Trompetto, M. Consensus statement of the Italian society of colorectal surgery (SICCR): Management and treatment of hemorrhoidal disease. Tech. Coloproctol. 2020, 24, 145–164. [Google Scholar] [CrossRef]
- Brown, S.R.; Tiernan, J.P.; Watson, A.J.M.; Biggs, K.; Shephard, N.; Wailoo, A.J.; Bradburn, M.; Alshreef, A.; Hind, D.; HubBLe Study Team. Haemorrhoidal artery ligation versus rubber band ligation for the management of symptomatic second-degree and third-degree haemorrhoids (HubBLe): A multicentre, open-label, randomised controlled trial. Lancet 2016, 388, 356–364, Erratum in Lancet 2016, 388, 342. [Google Scholar] [CrossRef]
- Di Saverio, S.; Pata, F.; Gallo, G.; Carrano, F.; Scorza, A.; Sileri, P.; Smart, N.; Spinelli, A.; Pellino, G. Coronavirus pandemic and colorectal surgery: Practical advice based on the Italian experience. Color. Dis. 2020, 22, 625–634. [Google Scholar] [CrossRef]
- COVIDSurg Collaborative; Nepogodiev, D.; Bhangu, A. Elective surgery cancellations due to the COVID-19 pandemic: Global predictive modelling to inform surgical recovery plans. J. Br. Surg. 2020, 22, 625–634. [Google Scholar] [CrossRef]
- Glasbey, J.; Ademuyiwa, A.; Adisa, A.; AlAmeer, E.; Arnaud, A.P.; Ayasra, F.; Azevedo, J.; Minaya-Bravo, A.; Costas-Chavarri, A.; Edwards, J.; et al. Effect of COVID-19 pandemic lockdowns on planned cancer surgery for 15 tumour types in 61 countries: An international, prospective, cohort study. Lancet Oncol. 2021, 22, 1507–1517. [Google Scholar] [CrossRef]
- La Torre, M.; Pata, F.; Gallo, G. Delayed benign surgery during the COVID-19 pandemic: The other side of the coin. J. Br. Surg. 2020, 107, e258. [Google Scholar] [CrossRef] [PubMed]
- Giani, I.; Elbetti, C.; Trompetto, M.; Gallo, G. Proctology in the COVID-19 era: Handle with care. J. Br. Surg. 2020, 107, e243. [Google Scholar] [CrossRef] [PubMed]
- Albuquerque, A. Rubber band ligation of hemorrhoids: A guide for complications. World J. Gastrointest. Surg. 2016, 8, 614–620. [Google Scholar] [CrossRef] [PubMed]
- Gallo, G.; Ronconi, M.; Trompetto, M. Sclerotherapy with 3% polidocanol foam: Revolutionizing outpatient treatment in patients with haemorrhoidal disease. Updat. Surg. 2021, 73, 2029–2030. [Google Scholar] [CrossRef]
- Brown, S.; Tiernan, J.; Biggs, K.; Hind, D.; Shephard, N.; Bradburn, M.; Wailoo, A.; Alshreef, A.; Swaby, L.; Watson, A.; et al. The HubBLe Trial: Haemorrhoidal artery ligation (HAL) versus rubber band ligation (RBL) for symptomatic second- and third-degree haemorrhoids: A multicentre randomised controlled trial and health-economic evaluation. Health Technol. Assess. 2016, 20, 1–150. [Google Scholar] [CrossRef]
- Rosa, B. Polidocanol Foam: A Breath of Fresh Air for the Treatment of Internal Hemorrhoids. GE Port. J. Gastroenterol. 2018, 26, 153–154. [Google Scholar] [CrossRef] [PubMed]
- Bracchitta, S.; Bracchitta, L.M.; Pata, F. Combined rubber band ligation with 3% polidocanol foam sclerotherapy (ScleroBanding) for the treatment of second-degree haemorrhoidal disease: A video vignette. Color. Dis. 2021, 23, 1585–1586. [Google Scholar] [CrossRef] [PubMed]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for Reporting Observational Studies. PLoS Med. 2007, 4, e296. [Google Scholar] [CrossRef] [PubMed]
- Moser, K.-H.; Mosch, C.; Walgenbach, M.; Bussen, D.G.; Kirsch, J.; Joos, A.K.; Gliem, P.; Sauerland, S. Efficacy and safety of sclerotherapy with polidocanol foam in comparison with fluid sclerosant in the treatment of first-grade haemorrhoidal disease: A randomised, controlled, single-blind, multicentre trial. Int. J. Color. Dis. 2013, 28, 1439–1447. [Google Scholar] [CrossRef]
- Mott, T.; Latimer, K.; Edwards, C. Hemorrhoids: Diagnosis and Treatment Options. Am. Fam. Physician 2018, 97, 172–179. [Google Scholar]
- Jacobs, D. Hemorrhoids. N. Engl. J. Med. 2014, 371, 944–951. [Google Scholar] [CrossRef]
- Rivadeneira, D.E.; Steele, S.R.; Ternent, C.; Chalasani, S.; Buie, W.D.; Rafferty, J.L. Practice Parameters for the Management of Hemorrhoids (Revised 2010). Dis. Colon Rectum 2011, 54, 1059–1064. [Google Scholar] [CrossRef]
- Pata, F.; Gallo, G.; Pellino, G.; Vigorita, V.; Podda, M.; Di Saverio, S.; D’Ambrosio, G.; Sammarco, G. Evolution of Surgical Management of Hemorrhoidal Disease: An Historical Overview. Front. Surg. 2021, 8, 319. [Google Scholar] [CrossRef]
- Orangio, G.R. Expert Commentary on the Evaluation and Management of Hemorrhoids. Dis. Colon Rectum 2020, 63, 424–426. [Google Scholar] [CrossRef]
- Iyer, V.S.; Shrier, I.; Gordon, P.H. Long-term outcome of rubber band ligation for symptomatic primary and recurrent internal hemorrhoids. Dis. Colon. Rectum. 2004, 47, 1364–1370. [Google Scholar] [CrossRef]
- Bat, L.; Melzer, E.; Koler, M.; Dreznick, Z.; Shemesh, E. Complications of rubber band ligation of symptomatic internal hemorrhoids. Dis. Colon Rectum 1993, 36, 287–290. [Google Scholar] [CrossRef]
- Marshman, D.; Huber, P.J.; Timmerman, W.; Simonton, C.T.; Odom, F.C.; Kaplan, E.R. Hemorrhoidal ligation. A review of efficacy. Dis. Colon. Rectum. 1989, 32, 369–371. [Google Scholar] [CrossRef]
- Lobascio, P.; Laforgia, R.; Novelli, E.; Perrone, F.; Di Salvo, M.; Pezzolla, A.; Trompetto, M.; Gallo, G. Short-Term Results of Sclerotherapy with 3% Polidocanol Foam for Symptomatic Second- and Third-Degree Hemorrhoidal Disease. J. Investig. Surg. 2020, 34, 1059–1065. [Google Scholar] [CrossRef] [PubMed]
- Odelowo, O.O.; Mekasha, G.; Johnson, M.A. Massive life-threatening lower gastrointestinal hemorrhage following hemorrhoidal rubber band ligation. J. Natl. Med. Assoc. 2002, 94, 1089–1092. [Google Scholar] [PubMed]
- Alatise, O.I.; Akindiose, C.; Arowolo, O.A.; Agbakwuru, A.E. Evaluation of two injection sclerosants in the treatment of symptomatic haemorrhoids in Nigerians. Niger. Postgrad. Med. J. 2016, 23, 110. [Google Scholar] [CrossRef] [PubMed]
- Schulte, T.; Fändrich, F.; Kahlke, V. Life-threatening rectal necrosis after injection sclerotherapy for haemorrhoids. Int. J. Color. Dis. 2007, 23, 725–726. [Google Scholar] [CrossRef] [PubMed]
- Pellino, G.; Spinelli, A. How Coronavirus Disease 2019 Outbreak Is Impacting Colorectal Cancer Patients in Italy: A Long Shadow Beyond Infection. Dis. Colon Rectum 2020, 63, 720–722. [Google Scholar] [CrossRef]
- Pata, F.; Bondurri, A.; Ferrara, F.; Parini, D.; Rizzo, G.; Qiao, Y.; Lui, R.; Granero, A.G.; Segura-Sampedro, J.J.; The Multidisciplinary Italian Study Group for STOmas (MISSTO). Enteral stoma care during the COVID-19 pandemic: Practical advice. Color. Dis. 2020, 22, 985–992. [Google Scholar] [CrossRef]
- Carr, A.; Smith, J.A.; Camaradou, J.; Prieto-Alhambra, D. Growing backlog of planned surgery due to COVID-19. BMJ 2021, 372, n339. [Google Scholar] [CrossRef]
- Macdonald, N.; Clements, C.; Sobti, A.; Rossiter, D.; Unnithan, A.; Bosanquet, N. Tackling the elective case backlog generated by COVID-19: The scale of the problem and solutions. J. Public Health 2020, 42, 712–716. [Google Scholar] [CrossRef]
- Chew, S.S.B.; Marshall, L.; Kalish, L.; Tham, J.; Grieve, D.A.; Douglas, P.R.; Newstead, G.L. Short-Term and Long-Term Results of Combined Sclerotherapy and Rubber Band Ligation of Hemorrhoids and Mucosal Prolapse. Dis. Colon Rectum 2003, 46, 1232–1237. [Google Scholar] [CrossRef] [PubMed]
- Kanellos, I.; Kazantzidou, D.; Christoforidis, E.; Demetriades, C.; Papavasiliou, K.; Dadoukis, I. Simultaneous, combined sclerotherapy and rubber band ligation of haemorrhoids. Tech. Coloproctol. 1999, 3, 59–61. [Google Scholar] [CrossRef]
- Kanellos, I.; Goulimaris, I.; Christoforidis, E.; Kelpis, T.; Betsis, D. A comparison of the simultaneous application of sclerotherapy and rubber band ligation, with sclerotherapy and rubber band ligation applied separately, for the treatment of haemorrhoids: A prospective randomized trial. Color. Dis. 2003, 5, 133–138. [Google Scholar] [CrossRef] [PubMed]
- Rabau, M.Y.; Bat, L. Treatment of bleeding hemorrhoids by injection sclerotherapy and rubber band ligation. Isr. J. Med Sci. 1985, 21, 569–571. [Google Scholar]
- Choi, J.; Freeman, J.B.; Touchette, J. Long-term follow-up of concomitant band ligation and sclerotherapy for internal hemorrhoids. Can. J. Surg. 1985, 28, 523–524. [Google Scholar] [PubMed]


{kind=link}
| VARIABLE | N (%) |
|---|---|
| Patients | 97 |
| Men | 56 (57.7%) |
| Women | 41 (42.3%) |
| Age | 52 years (20–84) |
| Goligher classification | |
| 2nd degree | 20 (20.6%) |
| 3rd degree | 77 (79.4%) |
| Ligations per procedure | 2.7 (1–3) |
| Follow-up (median) | 13 months (1–26) |
| Intraoperative complications | 0 (0%) |
| 30-day complications | 4 (4.1%) |
| 2nd degree | 0 (0%) |
| 3rd degree | 4 (5.2%) |
| Readmission | 0% |
| Mortality | 0% |
| Anesthesia Techniques | No. of Patients (%) |
|---|---|
| No anesthesia | 41 (42.3%) |
| Local anesthesia | 46 (47.4%) |
| Spinal anesthesia | 10 (10.3%) |
| Authors | Year | Design | No. of Patients | Technique | Degrees of HD | Follow-Up | Overall Complications | Recurrence |
|---|---|---|---|---|---|---|---|---|
| Rabau et al. [36] | 1985 | Retrospective | 178 | RBL (first) then SCT of the same nodule | I to III | 1 year | 5.6% | 10–15% |
| Choi et al. [37] | 1985 | Retrospective | 111 | RBL (first) then SCT of the same nodule | I to III | 18 months (range 2–60) | 1.8% (8.1% considering postoperative pain in the first 72 h) | 15% |
| Kanellos et al. [34] | 1999 | Prospective | 83 | RBL for larger and SCT for minor nodules | II | 2 years | 9.2% | NR |
| Chew et al. [33] | 2003 | Retrospective | 1102 | Sclerotherapy (first) then RBL of the same nodule | I to II | 1–11 years (mail/phone interview) | 3.1% | 16% |
| Kanellos et al. [35] | 2003 | Randomized control trial | 255 (85 in RBL + SCT group) | RBL for larger and SCT for minor nodules | II | 4 years | 10.8% | 10% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pata, F.; Bracchitta, L.M.; D’Ambrosio, G.; Bracchitta, S. Sclerobanding (Combined Rubber Band Ligation with 3% Polidocanol Foam Sclerotherapy) for the Treatment of Second- and Third-Degree Hemorrhoidal Disease: Feasibility and Short-Term Outcomes. J. Clin. Med. 2022, 11, 218. https://doi.org/10.3390/jcm11010218
Pata F, Bracchitta LM, D’Ambrosio G, Bracchitta S. Sclerobanding (Combined Rubber Band Ligation with 3% Polidocanol Foam Sclerotherapy) for the Treatment of Second- and Third-Degree Hemorrhoidal Disease: Feasibility and Short-Term Outcomes. Journal of Clinical Medicine. 2022; 11(1):218. https://doi.org/10.3390/jcm11010218
Chicago/Turabian StylePata, Francesco, Luigi Maria Bracchitta, Giancarlo D’Ambrosio, and Salvatore Bracchitta. 2022. "Sclerobanding (Combined Rubber Band Ligation with 3% Polidocanol Foam Sclerotherapy) for the Treatment of Second- and Third-Degree Hemorrhoidal Disease: Feasibility and Short-Term Outcomes" Journal of Clinical Medicine 11, no. 1: 218. https://doi.org/10.3390/jcm11010218