
Gouty Arthropathy: Review of Clinical Manifestations and Treatment, with Emphasis on Imaging

 , ,
, , {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Clinical
3. Imaging
3.1. Radiographs
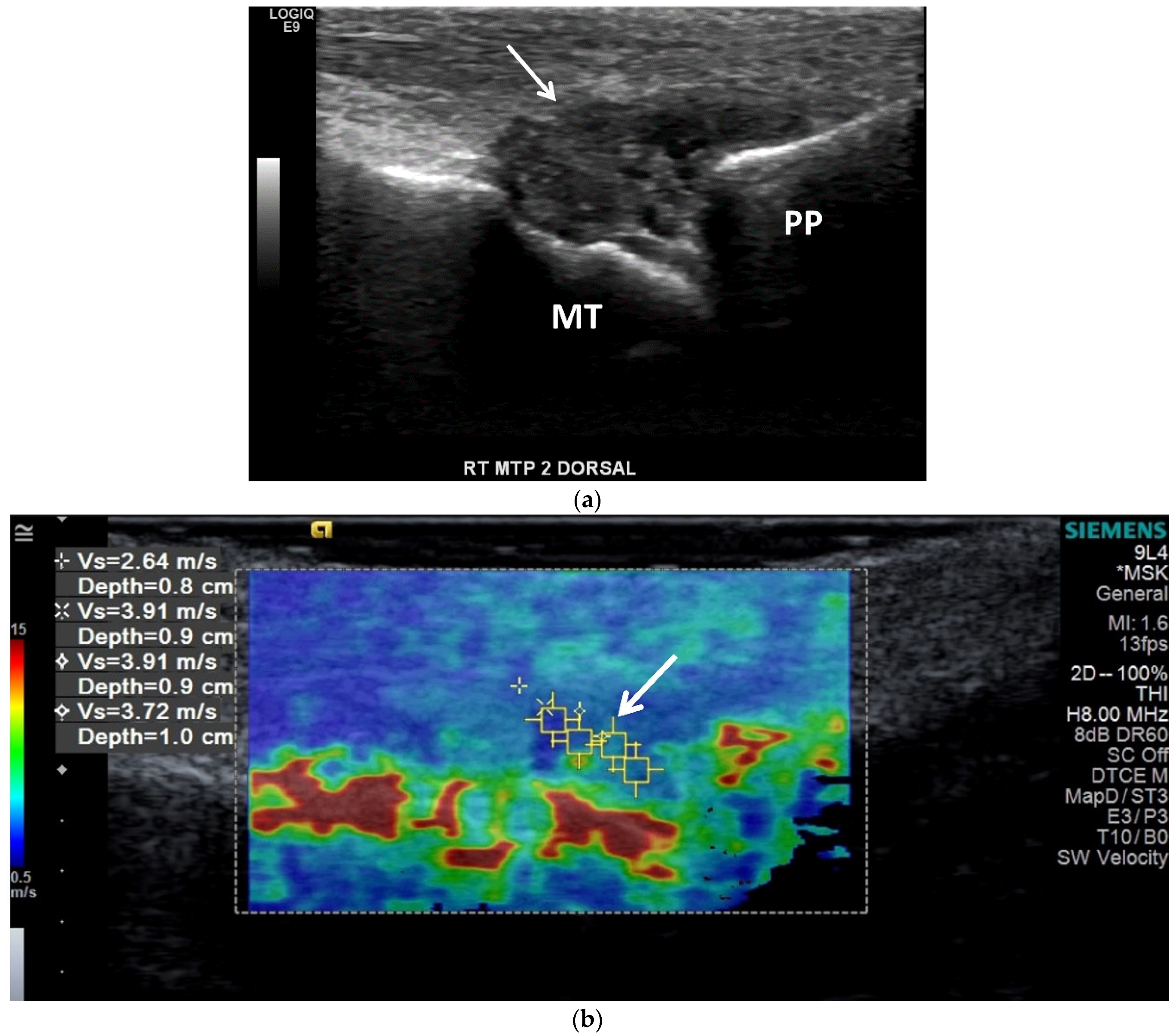
3.2. Ultrasound (US)
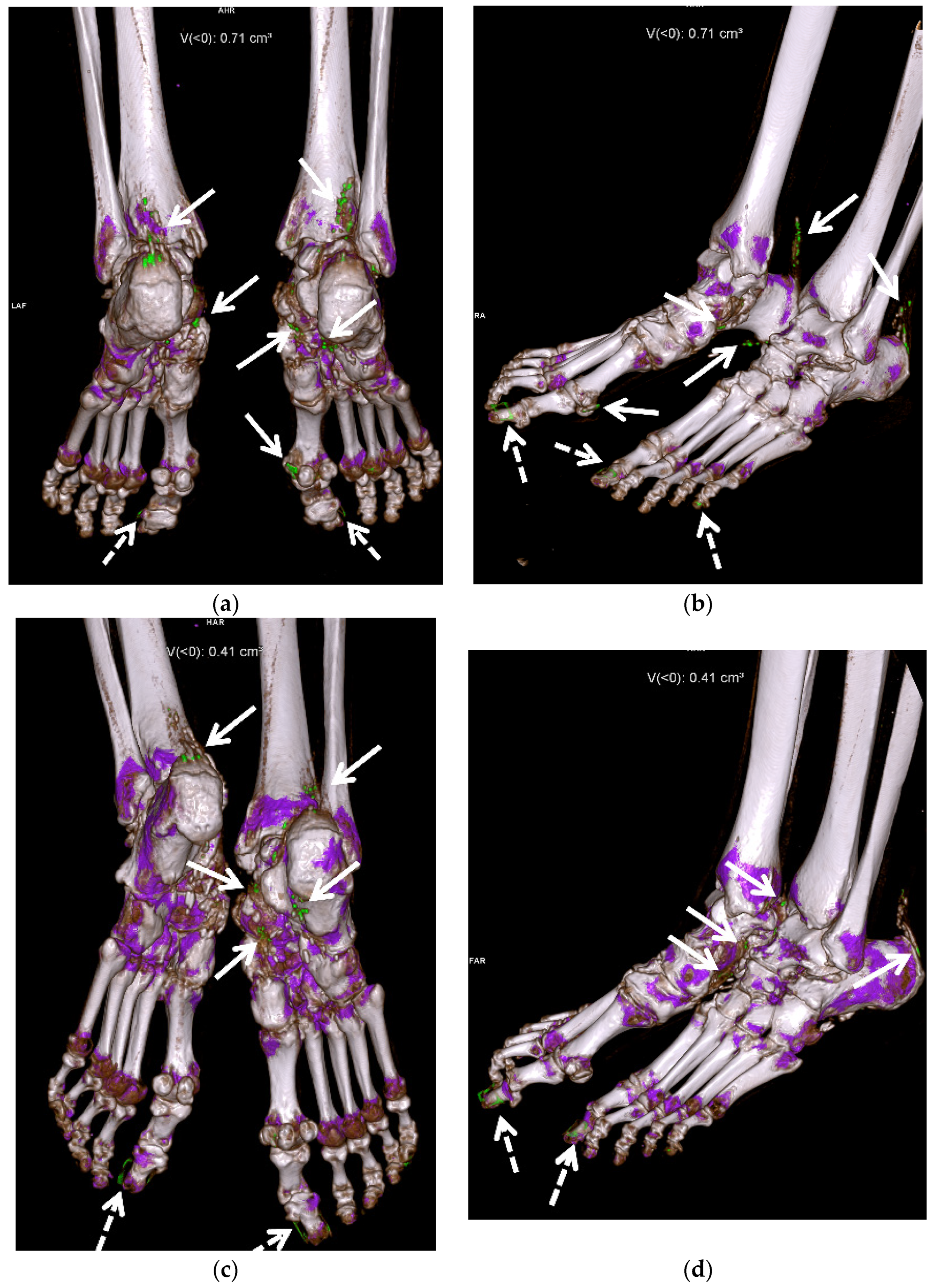
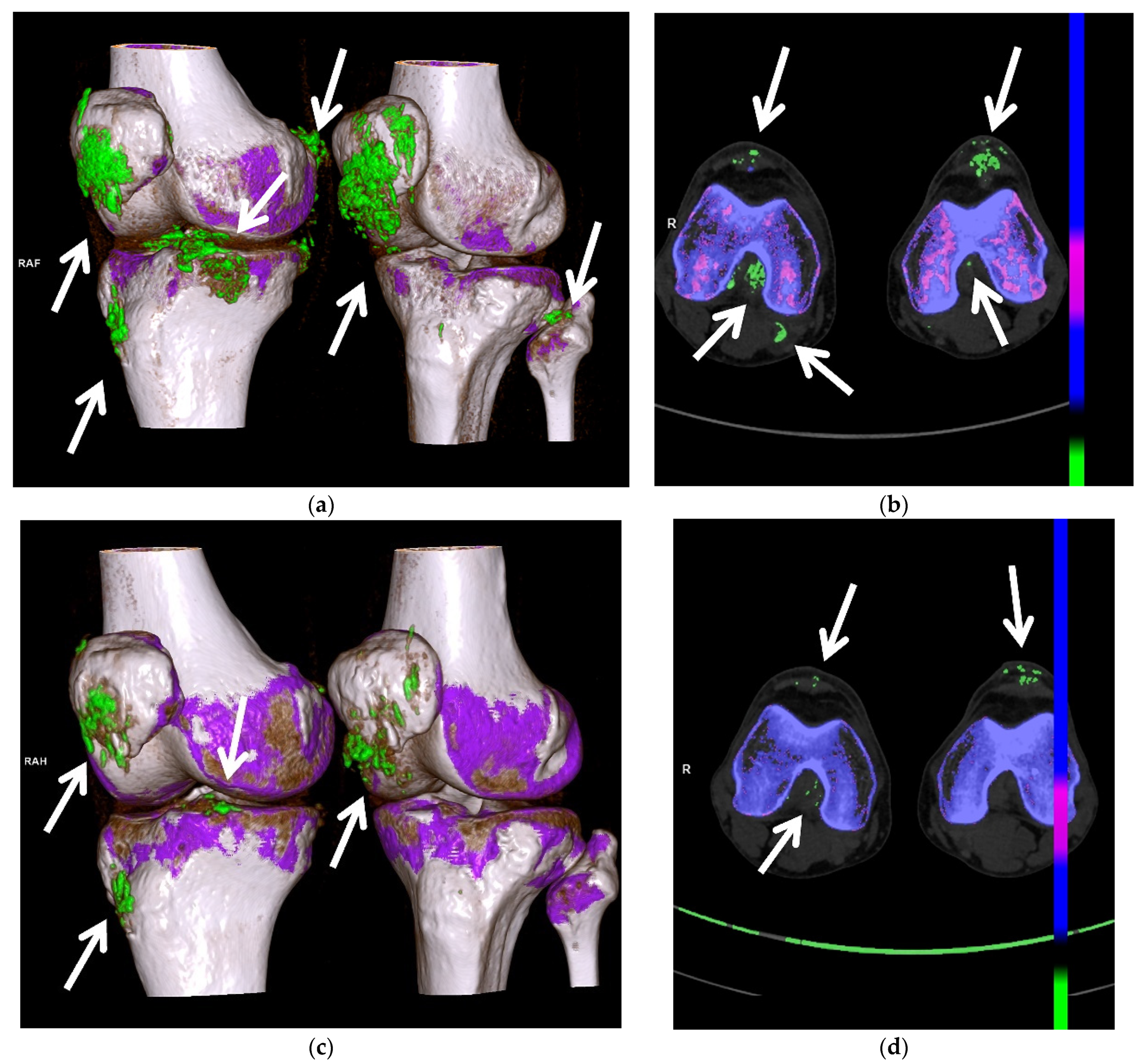
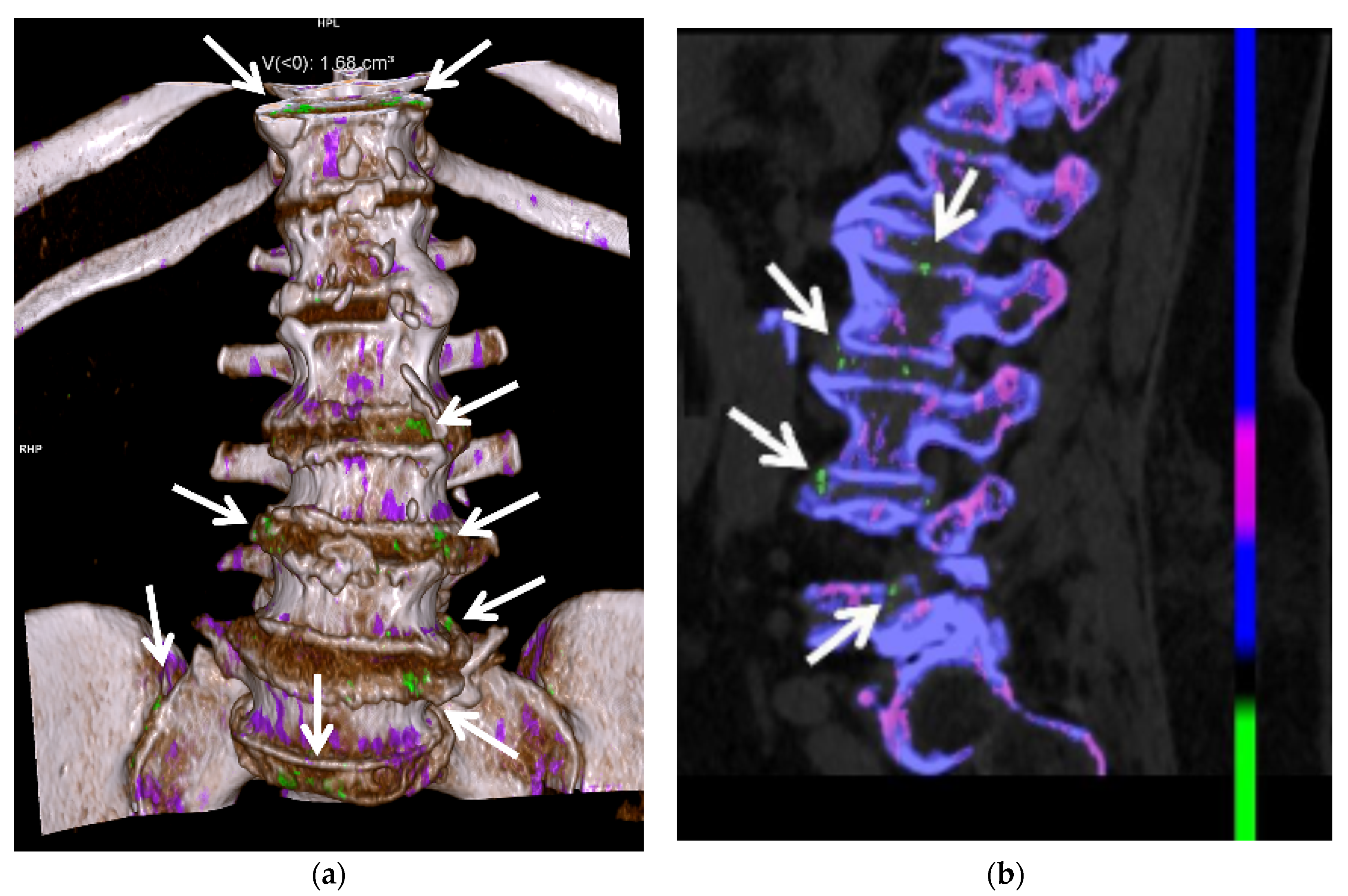
3.3. Computed Tomography (CT): Conventional and Dual Energy (DECT)
3.4. Magnetic Resonance Imaging (MRI)
3.5. Nuclear Medicine
4. Laboratory Evaluation
5. Medical Management of Acute Gouty Arthritis
5.1. Glucocorticoids
5.2. Nonsteroidal Anti-Inflammatory Drugs (NSAIDs)
5.3. Colchicine
5.4. Interleukin-1 (IL-1) Inhibitors
5.5. Urate-Lowering Therapies
5.6. Allopurinol
5.7. Febuxostat
5.8. Probenecid
5.9. Pegloticase
6. Surgical Management of Chronic Gouty Arthritis
7. New Horizons in the Treatment of Gouty Arthritis
8. Imaging of Treatment Response
9. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Kuo, C.F.; Grainge, M.J.; Zhang, W.; Doherty, M. Global epidemiology of gout: Prevalence, incidence and risk factors. Nat. Rev. Rheumatol. 2015, 11, 649–662. [Google Scholar] [CrossRef]
- Neogi, T.; Chen, C.; Niu, J.; Chaisson, C.; Hunter, D.J.; Zhang, Y. Alcohol quantity and type on risk of recurrent gout attacks: An internet-based case-crossover study. Am. J. Med. 2014, 127, 311–318. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neogi, T.; Jansen, T.L.; Dalbeth, N.; Fransen, J.; Schumacher, H.R.; Berendsen, D.; Brown, M.; Choi, H.; Edwards, N.L.; Janssens, H.J.; et al. 2015 Gout Classification Criteria: An American College of Rheumatology/European League Against Rheumatism collaborative initiative. Arthritis Rheumatol. 2015, 67, 2557–2568. [Google Scholar] [CrossRef] [PubMed]
- Taylor, W.J.; Fransen, J.; Jansen, T.L.; Dalbeth, N.; Schumacher, H.R.; Brown, M.; Louthrenoo, W.; Vazquez-Mellado, J.; Eliseev, M.; McCarthy, G.; et al. Study for Updated Gout Classification Criteria: Identification of Features to Classify Gout. Arthritis Care Res. (Hoboken) 2015, 67, 1304–1315. [Google Scholar] [CrossRef] [PubMed]
- Low, E.; Ouellette, H.; Munk, P.L. Tophaceous Gout. Ann. Acad. Med. Singap. 2020, 49, 931–933. [Google Scholar] [CrossRef] [PubMed]
- Monu, J.U.; Pope, T.L., Jr. Gout: A clinical and radiologic review. Radiol. Clin. N. Am. 2004, 42, 169–184. [Google Scholar] [CrossRef]
- Girish, G.; Glazebrook, K.N.; Jacobson, J.A. Advanced imaging in gout. AJR Am. J. Roentgenol. 2013, 201, 515–525. [Google Scholar] [CrossRef] [PubMed]
- Richette, P.; Doherty, M.; Pascual, E.; Barskova, V.; Becce, F.; Castaneda, J.; Coyfish, M.; Guillo, S.; Jansen, T.; Janssens, H.; et al. 2018 updated European League Against Rheumatism evidence-based recommendations for the diagnosis of gout. Ann. Rheum. Dis. 2020, 79, 31–38. [Google Scholar] [CrossRef] [Green Version]
- Christiansen, S.N.; Østergaard, M.; Terslev, L. Ultrasonography in gout: Utility in diagnosis and monitoring. Clin. Exp. Rheumatol. 2018, 36 (Suppl. 114), 61–67. [Google Scholar] [PubMed]
- Glazebrook, K.N.; Guimarães, L.S.; Murthy, N.S.; Black, D.F.; Bongartz, T.; Manek, N.J.; Leng, S.; Fletcher, J.G.; McCollough, C.H. Identification of intraarticular and periarticular uric acid crystals with dual-energy CT: Initial evaluation. Radiology 2011, 261, 516–524. [Google Scholar] [CrossRef] [PubMed]
- Bongartz, T.; Glazebrook, K.N.; Kavros, S.J.; Murthy, N.S.; Merry, S.P.; Franz, W.B., 3rd; Michet, C.J.; Veetil, B.M.; Davis, J.M., 3rd; Mason, T.G., 2nd; et al. Dual-energy CT for the diagnosis of gout: An accuracy and diagnostic yield study. Ann. Rheum. Dis. 2015, 74, 1072–1077. [Google Scholar] [CrossRef] [Green Version]
- Coupal, T.M.; Mallinson, P.I.; Gershony, S.L.; McLaughlin, P.D.; Munk, P.L.; Nicolaou, S.; Ouellette, H.A. Getting the Most From Your Dual-Energy Scanner: Recognizing, Reducing, and Eliminating Artifacts. AJR Am. J. Roentgenol. 2016, 206, 119–128. [Google Scholar] [CrossRef] [PubMed]
- Schwabl, C.; Taljanovic, M.; Widmann, G.; Teh, J.; Klauser, A.S. Ultrasonography and dual-energy computed tomography: Impact for the detection of gouty deposits. Ultrasonography 2021, 40, 197–206. [Google Scholar] [CrossRef] [PubMed]
- Desai, M.A.; Peterson, J.J.; Garner, H.W.; Kransdorf, M.J. Clinical utility of dual-energy CT for evaluation of tophaceous gout. Radiographics 2011, 31, 1365–1375; discussion 1376–1377. [Google Scholar] [CrossRef]
- Girish, G.; Melville, D.M.; Kaeley, G.S.; Brandon, C.J.; Goyal, J.R.; Jacobson, J.A.; Jamadar, D.A. Imaging appearances in gout. Arthritis 2013, 2013, 673401. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Connor, P.J. Crystal deposition disease and psoriatic arthritis. Semin. Musculoskelet. Radiol. 2013, 17, 74–79. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taljanovic, M.S.; Melville, D.M.; Gimber, L.H.; Scalcione, L.R.; Miller, M.D.; Kwoh, C.K.; Klauser, A.S. High-Resolution US of Rheumatologic Diseases. Radiographics 2015, 35, 2026–2048. [Google Scholar] [CrossRef] [PubMed]
- Teh, J.; McQueen, F.; Eshed, I.; Plagou, A.; Klauser, A. Advanced Imaging in the Diagnosis of Gout and Other Crystal Arthropathies. Semin. Musculoskelet. Radiol. 2018, 22, 225–236. [Google Scholar] [CrossRef]
- Suh, Y.S.; Cheon, Y.H.; Kim, J.E.; Kim, J.M.; Kim, S.H.; Lee, W.S.; Yoo, W.H.; Lee, S.I.; Kim, H.O. Usefulness of plain radiography for assessing hypouricemic treatment response in patients with tophaceous gout. Int. J. Rheum. Dis. 2016, 19, 1183–1188. [Google Scholar] [CrossRef]
- Ottaviani, S.; Gill, G.; Aubrun, A.; Palazzo, E.; Meyer, O.; Dieudé, P. Ultrasound in gout: A useful tool for following urate-lowering therapy. Jt. Bone Spine 2015, 82, 42–44. [Google Scholar] [CrossRef]
- de Ávila Fernandes, E.; Kubota, E.S.; Sandim, G.B.; Mitraud, S.A.; Ferrari, A.J.; Fernandes, A.R. Ultrasound features of tophi in chronic tophaceous gout. Skeletal. Radiol. 2011, 40, 309–315. [Google Scholar] [CrossRef] [PubMed]
- Abhishek, A.; Roddy, E.; Doherty, M. Gout—A guide for the general and acute physicians. Clin. Med. 2017, 17, 54–59. [Google Scholar] [CrossRef] [Green Version]
- Dalbeth, N.; Merriman, T.R.; Stamp, L.K. Gout. Lancet 2016, 388, 2039–2052. [Google Scholar] [CrossRef]
- Abdellatif, W.; Ding, J.; Khorshed, D.; Shojania, K.; Nicolaou, S. Unravelling the mysteries of gout by multimodality imaging. Semin. Arthritis Rheum. 2020, 50, S17–S23. [Google Scholar] [CrossRef]
- Wright, S.A.; Filippucci, E.; McVeigh, C.; Grey, A.; McCarron, M.; Grassi, W.; Wright, G.D.; Taggart, A.J. High-resolution ultrasonography of the first metatarsal phalangeal joint in gout: A controlled study. Ann. Rheum. Dis. 2007, 66, 859–864. [Google Scholar] [CrossRef]
- Thiele, R.G.; Schlesinger, N. Ultrasonography shows disappearance of monosodium urate crystal deposition on hyaline cartilage after sustained normouricemia is achieved. Rheumatol. Int. 2010, 30, 495–503. [Google Scholar] [CrossRef]
- Das, S.; Goswami, R.P.; Ghosh, A.; Ghosh, P.; Lahiri, D.; Basu, K. Temporal evolution of urate crystal deposition over articular cartilage after successful urate-lowering therapy in patients with gout: An ultrasonographic perspective. Mod. Rheumatol. 2017, 27, 518–523. [Google Scholar] [CrossRef] [PubMed]
- Rettenbacher, T.; Ennemoser, S.; Weirich, H.; Ulmer, H.; Hartig, F.; Klotz, W.; Herold, M. Diagnostic imaging of gout: Comparison of high-resolution US versus conventional X-ray. Eur. Radiol. 2008, 18, 621–630. [Google Scholar] [CrossRef] [PubMed]
- Pattamapaspong, N.; Vuthiwong, W.; Kanthawang, T.; Louthrenoo, W. Value of ultrasonography in the diagnosis of gout in patients presenting with acute arthritis. Skeletal. Radiol. 2017, 46, 759–767. [Google Scholar] [CrossRef]
- Klauser, A.S.; Halpern, E.J.; Strobl, S.; Abd Ellah, M.M.H.; Gruber, J.; Bellmann-Weiler, R.; Auer, T.; Feuchtner, G.; Jaschke, W. Gout of hand and wrist: The value of US as compared with DECT. Eur. Radiol. 2018, 28, 4174–4181. [Google Scholar] [CrossRef] [Green Version]
- Bayat, S.; Baraf, H.S.B.; Rech, J. Update on imaging in gout: Contrasting and comparing the role of dual-energy computed tomography to traditional diagnostic and monitoring techniques. Clin. Exp. Rheumatol. 2018, 36 (Suppl. 114), 53–60. [Google Scholar] [PubMed]
- Grainger, R.; Dalbeth, N.; Keen, H.; Durcan, L.; Lawrence Edwards, N.; Perez-Ruiz, F.; Diaz-Torne, C.; Singh, J.A.; Khanna, D.; Simon, L.S.; et al. Imaging as an Outcome Measure in Gout Studies: Report from the OMERACT Gout Working Group. J. Rheumatol. 2015, 42, 2460–2464. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, T.; Yang, F.; Li, J.; Pan, Z. Gout of the axial joint-A patient level systemic review. Semin. Arthritis Rheum. 2019, 48, 649–657. [Google Scholar] [CrossRef]
- Pillinger, M.H.; Mandell, B.F. Therapeutic approaches in the treatment of gout. Semin. Arthritis Rheum. 2020, 50, S24–S30. [Google Scholar] [CrossRef] [PubMed]
- Singh, J.A.; Gaffo, A. Gout epidemiology and comorbidities. Semin. Arthritis Rheum. 2020, 50, S11–S16. [Google Scholar] [CrossRef] [PubMed]
- Davies, J.; Riede, P.; van Langevelde, K.; Teh, J. Recent developments in advanced imaging in gout. Ther. Adv. Musculoskelet. Dis. 2019, 11, 1759720x19844429. [Google Scholar] [CrossRef] [PubMed]
- Choi, H.K.; Atkinson, K.; Karlson, E.W.; Willett, W.; Curhan, G. Alcohol intake and risk of incident gout in men: A prospective study. Lancet 2004, 363, 1277–1281. [Google Scholar] [CrossRef]
- Hak, A.E.; Curhan, G.C.; Grodstein, F.; Choi, H.K. Menopause, postmenopausal hormone use and risk of incident gout. Ann. Rheum. Dis. 2010, 69, 1305–1309. [Google Scholar] [CrossRef] [Green Version]
- Bhole, V.; de Vera, M.; Rahman, M.M.; Krishnan, E.; Choi, H. Epidemiology of gout in women: Fifty-two-year followup of a prospective cohort. Arthritis Rheum. 2010, 62, 1069–1076. [Google Scholar] [CrossRef] [PubMed]
- Zhu, L.; Wu, H.; Wu, X.; Sun, W.; Zhang, T.; Ye, L.; Wang, W.; Wang, J. Comparison Between Dual-Energy Computed Tomography and Ultrasound in the Diagnosis of Gout of Various Joints. Acad. Radiol. 2015, 22, 1497–1502. [Google Scholar] [CrossRef]
- Choi, H.K.; Curhan, G. Independent impact of gout on mortality and risk for coronary heart disease. Circulation 2007, 116, 894–900. [Google Scholar] [CrossRef]
- Choi, H.K.; De Vera, M.A.; Krishnan, E. Gout and the risk of type 2 diabetes among men with a high cardiovascular risk profile. Rheumatology (Oxford) 2008, 47, 1567–1570. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choi, H.K.; Ford, E.S.; Li, C.; Curhan, G. Prevalence of the metabolic syndrome in patients with gout: The Third National Health and Nutrition Examination Survey. Arthritis Rheum. 2007, 57, 109–115. [Google Scholar] [CrossRef]
- Bardin, T.; Richette, P. Impact of comorbidities on gout and hyperuricaemia: An update on prevalence and treatment options. BMC Med. 2017, 15, 123. [Google Scholar] [CrossRef] [PubMed]
- Klauser, A.S.; Halpern, E.J.; Strobl, S.; Gruber, J.; Feuchtner, G.; Bellmann-Weiler, R.; Weiss, G.; Stofferin, H.; Jaschke, W. Dual-Energy Computed Tomography Detection of Cardiovascular Monosodium Urate Deposits in Patients With Gout. JAMA Cardiol. 2019, 4, 1019–1028. [Google Scholar] [CrossRef] [PubMed]
- Chou, H.; Chin, T.Y.; Peh, W.C. Dual-energy CT in gout—A review of current concepts and applications. J. Med. Radiat. Sci. 2017, 64, 41–51. [Google Scholar] [CrossRef]
- Liu, F.; Dong, J.; Zhou, D.; Kang, Q.; Xiong, F. Gout is not associated with the risk of fracture: A meta-analysis. J. Orthop. Surg. Res. 2019, 14, 272. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Towiwat, P.; Chhana, A.; Dalbeth, N. The anatomical pathology of gout: A systematic literature review. BMC Musculoskelet. Disord. 2019, 20, 140. [Google Scholar] [CrossRef] [PubMed]
- Nicolaou, S.; Yong-Hing, C.J.; Galea-Soler, S.; Hou, D.J.; Louis, L.; Munk, P. Dual-energy CT as a potential new diagnostic tool in the management of gout in the acute setting. AJR Am. J. Roentgenol. 2010, 194, 1072–1078. [Google Scholar] [CrossRef] [PubMed]
- Mallinson, P.I.; Reagan, A.C.; Coupal, T.; Munk, P.L.; Ouellette, H.; Nicolaou, S. The distribution of urate deposition within the extremities in gout: A review of 148 dual-energy CT cases. Skeletal. Radiol. 2014, 43, 277–281. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.K.; Jung, J.Y.; Jee, W.H.; Lee, J.J.; Park, S.H. Combining non-contrast and dual-energy CT improves diagnosis of early gout. Eur. Radiol. 2019, 29, 1267–1275. [Google Scholar] [CrossRef]
- Dalbeth, N.; Kalluru, R.; Aati, O.; Horne, A.; Doyle, A.J.; McQueen, F.M. Tendon involvement in the feet of patients with gout: A dual-energy CT study. Ann. Rheum. Dis. 2013, 72, 1545–1548. [Google Scholar] [CrossRef] [PubMed]
- Schumacher, H.R., Jr.; Becker, M.A.; Palo, W.A.; Streit, J.; MacDonald, P.A.; Joseph-Ridge, N. Tophaceous gout: Quantitative evaluation by direct physical measurement. J. Rheumatol. 2005, 32, 2368–2372. [Google Scholar]
- Dalbeth, N.; Schauer, C.; Macdonald, P.; Perez-Ruiz, F.; Schumacher, H.R.; Hamburger, S.; Choi, H.K.; McQueen, F.M.; Doyle, A.; Taylor, W.J. Methods of tophus assessment in clinical trials of chronic gout: A systematic literature review and pictorial reference guide. Ann. Rheum. Dis. 2011, 70, 597–604. [Google Scholar] [CrossRef]
- Ko, K.H.; Hsu, Y.C.; Lee, H.S.; Lee, C.H.; Huang, G.S. Tophaceous gout of the knee: Revisiting MRI patterns in 30 patients. J. Clin. Rheumatol. 2010, 16, 209–214. [Google Scholar] [CrossRef] [PubMed]
- Dalbeth, N.; Pool, B.; Gamble, G.D.; Smith, T.; Callon, K.E.; McQueen, F.M.; Cornish, J. Cellular characterization of the gouty tophus: A quantitative analysis. Arthritis Rheum. 2010, 62, 1549–1556. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.H.; Song, G.G. Diagnostic accuracy of ultrasound in patients with gout: A meta-analysis. Semin. Arthritis Rheum. 2018, 47, 703–709. [Google Scholar] [CrossRef] [PubMed]
- Fields, T.R. The Challenges of Approaching and Managing Gout. Rheum. Dis. Clin. N. Am. 2019, 45, 145–157. [Google Scholar] [CrossRef]
- Ogdie, A.; Taylor, W.J.; Neogi, T.; Fransen, J.; Jansen, T.L.; Schumacher, H.R.; Louthrenoo, W.; Vazquez-Mellado, J.; Eliseev, M.; McCarthy, G.; et al. Performance of Ultrasound in the Diagnosis of Gout in a Multicenter Study: Comparison With Monosodium Urate Monohydrate Crystal Analysis as the Gold Standard. Arthritis Rheumatol. 2017, 69, 429–438. [Google Scholar] [CrossRef]
- Kravchenko, D.; Karakostas, P.; Kuetting, D.; Meyer, C.; Brossart, P.; Behning, C.; Schäfer, V.S. The role of dual energy computed tomography in the differentiation of acute gout flares and acute calcium pyrophosphate crystal arthritis. Clin. Rheumatol. 2021. [Google Scholar] [CrossRef]
- Bloch, C.; Hermann, G.; Yu, T.F. A radiologic reevaluation of gout: A study of 2,000 patients. AJR Am. J. Roentgenol. 1980, 134, 781–787. [Google Scholar] [CrossRef] [Green Version]
- Glazebrook, K.N.; Kakar, S.; Ida, C.M.; Laurini, J.A.; Moder, K.G.; Leng, S. False-negative dual-energy computed tomography in a patient with acute gout. J. Clin. Rheumatol. 2012, 18, 138–141. [Google Scholar] [CrossRef]
- Terslev, L.; Gutierrez, M.; Christensen, R.; Balint, P.V.; Bruyn, G.A.; Delle Sedie, A.; Filippucci, E.; Garrido, J.; Hammer, H.B.; Iagnocco, A.; et al. Assessing Elementary Lesions in Gout by Ultrasound: Results of an OMERACT Patient-based Agreement and Reliability Exercise. J. Rheumatol. 2015, 42, 2149–2154. [Google Scholar] [CrossRef] [Green Version]
- Christiansen, S.N.; Filippou, G.; Scirè, C.A.; Balint, P.V.; Bruyn, G.A.; Dalbeth, N.; Dejaco, C.; Sedie, A.D.; Filippucci, E.; Hammer, H.B.; et al. Consensus-based semi-quantitative ultrasound scoring system for gout lesions: Results of an OMERACT Delphi process and web-reliability exercise. Semin. Arthritis Rheum. 2021, 51, 644–649. [Google Scholar] [CrossRef] [PubMed]
- Grassi, W.; Meenagh, G.; Pascual, E.; Filippucci, E. "Crystal clear"-sonographic assessment of gout and calcium pyrophosphate deposition disease. Semin. Arthritis Rheum. 2006, 36, 197–202. [Google Scholar] [CrossRef] [PubMed]
- Howard, R.G.; Pillinger, M.H.; Gyftopoulos, S.; Thiele, R.G.; Swearingen, C.J.; Samuels, J. Reproducibility of musculoskeletal ultrasound for determining monosodium urate deposition: Concordance between readers. Arthritis Care Res. (Hoboken) 2011, 63, 1456–1462. [Google Scholar] [CrossRef] [PubMed]
- Thiele, R.G. Role of ultrasound and other advanced imaging in the diagnosis and management of gout. Curr. Rheumatol. Rep. 2011, 13, 146–153. [Google Scholar] [CrossRef]
- Filippucci, E.; Riveros, M.G.; Georgescu, D.; Salaffi, F.; Grassi, W. Hyaline cartilage involvement in patients with gout and calcium pyrophosphate deposition disease. An ultrasound study. Osteoarthr. Cartil. 2009, 17, 178–181. [Google Scholar] [CrossRef] [Green Version]
- Pineda, C.; Amezcua-Guerra, L.M.; Solano, C.; Rodriguez-Henríquez, P.; Hernández-Díaz, C.; Vargas, A.; Hofmann, F.; Gutiérrez, M. Joint and tendon subclinical involvement suggestive of gouty arthritis in asymptomatic hyperuricemia: An ultrasound controlled study. Arthritis Res. Ther. 2011, 13, R4. [Google Scholar] [CrossRef]
- Wakefield, R.J.; Balint, P.V.; Szkudlarek, M.; Filippucci, E.; Backhaus, M.; D’Agostino, M.A.; Sanchez, E.N.; Iagnocco, A.; Schmidt, W.A.; Bruyn, G.A.; et al. Musculoskeletal ultrasound including definitions for ultrasonographic pathology. J. Rheumatol. 2005, 32, 2485–2487. [Google Scholar]
- Carter, J.D.; Kedar, R.P.; Anderson, S.R.; Osorio, A.H.; Albritton, N.L.; Gnanashanmugam, S.; Valeriano, J.; Vasey, F.B.; Ricca, L.R. An analysis of MRI and ultrasound imaging in patients with gout who have normal plain radiographs. Rheumatology (Oxford) 2009, 48, 1442–1446. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taljanovic, M.S.; Gimber, L.H.; Becker, G.W.; Latt, L.D.; Klauser, A.S.; Melville, D.M.; Gao, L.; Witte, R.S. Shear-Wave Elastography: Basic Physics and Musculoskeletal Applications. Radiographics 2017, 37, 855–870. [Google Scholar] [CrossRef] [Green Version]
- Tang, Y.; Yan, F.; Yang, Y.; Xiang, X.; Wang, L.; Zhang, L.; Qiu, L. Value of Shear Wave Elastography in the Diagnosis of Gouty and Non-Gouty Arthritis. Ultrasound Med. Biol. 2017, 43, 884–892. [Google Scholar] [CrossRef]
- Wang, Q.; Guo, L.H.; Li, X.L.; Zhao, C.K.; Li, M.X.; Wang, L.; Liu, X.Y.; Xu, H.X. Differentiating the acute phase of gout from the intercritical phase with ultrasound and quantitative shear wave elastography. Eur. Radiol. 2018, 28, 5316–5327. [Google Scholar] [CrossRef] [PubMed]
- Mallinson, P.I.; Coupal, T.M.; McLaughlin, P.D.; Nicolaou, S.; Munk, P.L.; Ouellette, H.A. Dual-Energy CT for the Musculoskeletal System. Radiology 2016, 281, 690–707. [Google Scholar] [CrossRef] [PubMed]
- Carotti, M.; Salaffi, F.; Filippucci, E.; Aringhieri, G.; Bruno, F.; Giovine, S.; Gentili, F.; Floridi, C.; Borgheresi, A.; De Filippo, M.; et al. Clinical utility of Dual Energy Computed Tomography in gout: Current concepts and applications. Acta Biomed. 2020, 91, 116–124. [Google Scholar] [CrossRef]
- Gamala, M.; Jacobs, J.W.G.; van Laar, J.M. The diagnostic performance of dual energy CT for diagnosing gout: A systematic literature review and meta-analysis. Rheumatology (Oxford) 2019, 58, 2117–2121. [Google Scholar] [CrossRef]
- De Vulder, N.; Chen, M.; Huysse, W.; Herregods, N.; Verstraete, K.; Jans, L. Case Series: Dual-Energy CT in Extra-Articular Manifestations of Gout: Main Teaching Point: Dual-energy CT is a valuable asset in the detection of extra-articular manifestations of gout. J. Belg. Soc. Radiol. 2020, 104, 27. [Google Scholar] [CrossRef]
- Wang, J.X.; Ng, B.; Bak, H.; Spencer, D.; Manolios, N.; Wong, P.K.K. The utility of dual energy computed tomography in the management of axial gout: Case reports and literature review. BMC Rheumatol. 2020, 4, 22. [Google Scholar] [CrossRef]
- Marty-Ané, A.; Norberciak, L.; Andrès, M.; Houvenagel, E.; Ducoulombier, V.; Legrand, J.; Budzik, J.F.; Pascart, T. Crystal deposition measured with dual-energy computed tomography: Association with mortality and cardiovascular risks in gout. Rheumatology (Oxford) 2021, 60, 4855–4860. [Google Scholar] [CrossRef]
- Popovich, I.; Dalbeth, N.; Doyle, A.; Reeves, Q. McQueen FM: Exploring cartilage damage in gout using 3-T MRI: Distribution and associations with joint inflammation and tophus deposition. Skelet. Radiol. 2014, 43, 917–924. [Google Scholar] [CrossRef] [PubMed]
- McQueen, F.M.; Doyle, A.; Reeves, Q.; Gao, A.; Tsai, A.; Gamble, G.D.; Curteis, B.; Williams, M.; Dalbeth, N. Bone erosions in patients with chronic gouty arthropathy are associated with tophi but not bone oedema or synovitis: New insights from a 3 T MRI study. Rheumatology (Oxford) 2014, 53, 95–103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fernandes, A.; Faria, M.T.; Oliveira, A.; Vieira, T.; Pereira, J. Bone scintigraphy in tophaceous gout. Eur. J. Nucl. Med. Mol. Imaging 2016, 43, 1387–1388. [Google Scholar] [CrossRef] [PubMed]
- Goshen, E.; Schwartz, A.; Zwas, S.T. Chronic tophaceous gout: Scintigraphic findings on bone scan. Clin. Nucl. Med. 2000, 25, 146–147. [Google Scholar] [CrossRef]
- Emsen, B.; Fitoussi, A.; Chalaye, J.; Adam, C.; Itti, E. FDG PET/CT of Cervical Gout with Spinal Cord Compression. Clin. Nucl. Med. 2020, 45, e29–e31. [Google Scholar] [CrossRef]
- Ito, K.; Minamimoto, R.; Morooka, M.; Kubota, K. A case of gouty arthritis to tophi on 18F-FDG PET/CT imaging. Clin. Nucl. Med. 2012, 37, 614–617. [Google Scholar] [CrossRef]
- Qiu, L.; Chen, Y.; Huang, Z.; Cai, L.; Zhang, L. Widespread gouty tophi on 18F-FDG PET/CT imaging. Clin. Nucl. Med. 2014, 39, 579–581. [Google Scholar] [CrossRef]
- Vicente, J.S.; Gómez, A.L.; Moreno, R.L.; Torre, J.R.I.; Bernardo, L.G.; Madrid, J.I.R. Lumbar Gout Tophus Mimicking Epidural Abscess with Magnetic Resonance Imaging, Bone, and Gallium Scans. Indian J. Nucl. Med. 2018, 33, 158–160. [Google Scholar] [CrossRef]
- Schlesinger, N.; Norquist, J.M.; Watson, D.J. Serum urate during acute gout. J. Rheumatol. 2009, 36, 1287–1289. [Google Scholar] [CrossRef]
- Swan, A.; Amer, H.; Dieppe, P. The value of synovial fluid assays in the diagnosis of joint disease: A literature survey. Ann. Rheum. Dis. 2002, 61, 493–498. [Google Scholar] [CrossRef]
- Janssens, H.J.; Janssen, M.; van de Lisdonk, E.H.; van Riel, P.L.; van Weel, C. Use of oral prednisolone or naproxen for the treatment of gout arthritis: A double-blind, randomised equivalence trial. Lancet 2008, 371, 1854–1860. [Google Scholar] [CrossRef]
- Man, C.Y.; Cheung, I.T.; Cameron, P.A.; Rainer, T.H. Comparison of oral prednisolone/paracetamol and oral indomethacin/paracetamol combination therapy in the treatment of acute goutlike arthritis: A double-blind, randomized, controlled trial. Ann. Emerg. Med. 2007, 49, 670–677. [Google Scholar] [CrossRef] [PubMed]
- Rainer, T.H.; Cheng, C.H.; Janssens, H.J.; Man, C.Y.; Tam, L.S.; Choi, Y.F.; Yau, W.H.; Lee, K.H.; Graham, C.A. Oral Prednisolone in the Treatment of Acute Gout: A Pragmatic, Multicenter, Double-Blind, Randomized Trial. Ann. Intern. Med. 2016, 164, 464–471. [Google Scholar] [CrossRef] [PubMed]
- Wechalekar, M.D.; Vinik, O.; Schlesinger, N.; Buchbinder, R. Intra-articular glucocorticoids for acute gout. Cochrane Database Syst. Rev. 2013. [Google Scholar] [CrossRef] [Green Version]
- Zeng, L.; Qasim, A.; Neogi, T.; Fitzgerald, J.D.; Dalbeth, N.; Mikuls, T.R.; Guyatt, G.H.; Brignardello-Petersen, R. Efficacy and Safety of Pharmacologic Interventions in Patients Experiencing a Gout Flare: A Systematic Review and Network Meta-Analysis. Arthritis Care Res. (Hoboken) 2021, 73, 755–764. [Google Scholar] [CrossRef] [PubMed]
- Sutaria, S.; Katbamna, R.; Underwood, M. Effectiveness of interventions for the treatment of acute and prevention of recurrent gout--a systematic review. Rheumatology (Oxford) 2006, 45, 1422–1431. [Google Scholar] [CrossRef] [Green Version]
- Schumacher, H.R., Jr.; Boice, J.A.; Daikh, D.I.; Mukhopadhyay, S.; Malmstrom, K.; Ng, J.; Tate, G.A.; Molina, J. Randomised double blind trial of etoricoxib and indometacin in treatment of acute gouty arthritis. BMJ 2002, 324, 1488–1492. [Google Scholar] [CrossRef] [Green Version]
- Schumacher, H.R.; Berger, M.F.; Li-Yu, J.; Perez-Ruiz, F.; Burgos-Vargas, R.; Li, C. Efficacy and tolerability of celecoxib in the treatment of acute gouty arthritis: A randomized controlled trial. J. Rheumatol. 2012, 39, 1859–1866. [Google Scholar] [CrossRef]
- van Durme, C.M.; Wechalekar, M.D.; Buchbinder, R.; Schlesinger, N.; van der Heijde, D.; Landewe, R.B. Non-steroidal anti-inflammatory drugs for acute gout. Cochrane Database Syst. Rev. 2014, CD010120. [Google Scholar] [CrossRef] [Green Version]
- Terkeltaub, R.A.; Furst, D.E.; Bennett, K.; Kook, K.A.; Crockett, R.S.; Davis, M.W. High versus low dosing of oral colchicine for early acute gout flare: Twenty-four-hour outcome of the first multicenter, randomized, double-blind, placebo-controlled, parallel-group, dose-comparison colchicine study. Arthritis Rheum. 2010, 62, 1060–1068. [Google Scholar] [CrossRef]
- Terkeltaub, R.A. Colchicine update: 2008. Semin. Arthritis Rheum. 2009, 38, 411–419. [Google Scholar] [CrossRef] [PubMed]
- Liew, J.W.; Gardner, G.C. Use of Anakinra in Hospitalized Patients with Crystal-associated Arthritis. J. Rheumatol. 2019, 46, 1345–1349. [Google Scholar] [CrossRef] [PubMed]
- Saag, K.G.; Khanna, P.P.; Keenan, R.T.; Ohlman, S.; Osterling Koskinen, L.; Sparve, E.; Akerblad, A.C.; Wiken, M.; So, A.; Pillinger, M.H.; et al. A Randomized, Phase II Study Evaluating the Efficacy and Safety of Anakinra in the Treatment of Gout Flares. Arthritis Rheumatol. 2021, 73, 1533–1542. [Google Scholar] [CrossRef]
- FitzGerald, J.D.; Dalbeth, N.; Mikuls, T.; Brignardello-Petersen, R.; Guyatt, G.; Abeles, A.M.; Gelber, A.C.; Harrold, L.R.; Khanna, D.; King, C.; et al. 2020 American College of Rheumatology Guideline for the Management of Gout. Arthritis Rheumatol. 2020, 72, 879–895. [Google Scholar] [CrossRef] [PubMed]
- Borstad, G.C.; Bryant, L.R.; Abel, M.P.; Scroggie, D.A.; Harris, M.D.; Alloway, J.A. Colchicine for prophylaxis of acute flares when initiating allopurinol for chronic gouty arthritis. J. Rheumatol. 2004, 31, 2429–2432. [Google Scholar]
- Hershfield, M.S.; Callaghan, J.T.; Tassaneeyakul, W.; Mushiroda, T.; Thorn, C.F.; Klein, T.E.; Lee, M.T. Clinical Pharmacogenetics Implementation Consortium guidelines for human leukocyte antigen-B genotype and allopurinol dosing. Clin. Pharmacol. Ther. 2013, 93, 153–158. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Becker, M.A.; Schumacher, H.R., Jr.; Wortmann, R.L.; MacDonald, P.A.; Eustace, D.; Palo, W.A.; Streit, J.; Joseph-Ridge, N. Febuxostat compared with allopurinol in patients with hyperuricemia and gout. N. Engl. J. Med. 2005, 353, 2450–2461. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Becker, M.A.; Schumacher, H.R.; Espinoza, L.R.; Wells, A.F.; MacDonald, P.; Lloyd, E.; Lademacher, C. The urate-lowering efficacy and safety of febuxostat in the treatment of the hyperuricemia of gout: The CONFIRMS trial. Arthritis Res. Ther. 2010, 12, R63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- White, W.B.; Saag, K.G.; Becker, M.A.; Borer, J.S.; Gorelick, P.B.; Whelton, A.; Hunt, B.; Castillo, M.; Gunawardhana, L.; Investigators, C. Cardiovascular Safety of Febuxostat or Allopurinol in Patients with Gout. N. Engl. J. Med. 2018, 378, 1200–1210. [Google Scholar] [CrossRef] [PubMed]
- Khanna, D.; Fitzgerald, J.D.; Khanna, P.P.; Bae, S.; Singh, M.K.; Neogi, T.; Pillinger, M.H.; Merill, J.; Lee, S.; Prakash, S.; et al. 2012 American College of Rheumatology guidelines for management of gout. Part 1: Systematic nonpharmacologic and pharmacologic therapeutic approaches to hyperuricemia. Arthritis Care Res. (Hoboken) 2012, 64, 1431–1446. [Google Scholar] [CrossRef] [Green Version]
- Sundy, J.S.; Baraf, H.S.; Yood, R.A.; Edwards, N.L.; Gutierrez-Urena, S.R.; Treadwell, E.L.; Vazquez-Mellado, J.; White, W.B.; Lipsky, P.E.; Horowitz, Z.; et al. Efficacy and tolerability of pegloticase for the treatment of chronic gout in patients refractory to conventional treatment: Two randomized controlled trials. JAMA 2011, 306, 711–720. [Google Scholar] [CrossRef] [Green Version]
- Baraf, H.S.; Yood, R.A.; Ottery, F.D.; Sundy, J.S.; Becker, M.A. Infusion-related reactions with pegloticase, a recombinant uricase for the treatment of chronic gout refractory to conventional therapy. J. Clin. Rheumatol. 2014, 20, 427–432. [Google Scholar] [CrossRef]
- Tang, C.Y.; Fung, B. The last defence? Surgical aspects of gouty arthritis of hand and wrist. Hong Kong Med. J. 2011, 17, 480–486. [Google Scholar] [PubMed]
- Capobianco, C.M. Surgical treatment approaches to second metatarsophalangeal joint pathology. Clin. Podiatr. Med. Surg. 2012, 29, 443–449. [Google Scholar] [CrossRef]
- Caliogna, L.; Medetti, M.; Bina, V.; Brancato, A.M.; Castelli, A.; Jannelli, E.; Ivone, A.; Gastaldi, G.; Annunziata, S.; Mosconi, M.; et al. Pulsed Electromagnetic Fields in Bone Healing: Molecular Pathways and Clinical Applications. Int. J. Mol. Sci. 2021, 22, 7403. [Google Scholar] [CrossRef] [PubMed]
- Ouyang, J.; Zhang, B.; Kuang, L.; Yang, P.; Du, X.; Qi, H.; Su, N.; Jin, M.; Yang, J.; Xie, Y.; et al. Pulsed Electromagnetic Field Inhibits Synovitis via Enhancing the Efferocytosis of Macrophages. Biomed. Res. Int. 2020, 2020, 4307385. [Google Scholar] [CrossRef] [PubMed]
- Ross, C.L.; Ang, D.C.; Almeida-Porada, G. Targeting Mesenchymal Stromal Cells/Pericytes (MSCs) With Pulsed Electromagnetic Field (PEMF) Has the Potential to Treat Rheumatoid Arthritis. Front. Immunol. 2019, 10, 266. [Google Scholar] [CrossRef] [PubMed]
- Garner, H.W.; Wessell, D.E. Current status of ultrasound and dual-energy computed tomography in the evaluation of gout. Rheumatol. Int. 2018, 38, 1339–1344. [Google Scholar] [CrossRef] [PubMed]
- Dalbeth, N.; Frampton, C.; Fung, M.; Baumgartner, S.; Nicolaou, S.; Choi, H.K. Concurrent validity of provisional remission criteria for gout: A dual-energy CT study. Arthritis Res. Ther. 2019, 21, 150. [Google Scholar] [CrossRef] [Green Version]
- Schumacher, H.R.; Taylor, W.; Edwards, L.; Grainger, R.; Schlesinger, N.; Dalbeth, N.; Sivera, F.; Singh, J.; Evans, R.; Waltrip, R.W.; et al. Outcome domains for studies of acute and chronic gout. J. Rheumatol. 2009, 36, 2342–2345. [Google Scholar] [CrossRef] [PubMed]
- Perez-Ruiz, F.; Martin, I.; Canteli, B. Ultrasonographic measurement of tophi as an outcome measure for chronic gout. J. Rheumatol. 2007, 34, 1888–1893. [Google Scholar] [PubMed]
- Peiteado, D.; Villalba, A.; Martín-Mola, E.; Balsa, A.; De Miguel, E. Ultrasound sensitivity to changes in gout: A longitudinal study after two years of treatment. Clin. Exp. Rheumatol. 2017, 35, 746–751. [Google Scholar] [PubMed]
- Ebstein, E.; Forien, M.; Norkuviene, E.; Richette, P.; Mouterde, G.; Daien, C.; Ea, H.K.; Brière, C.; Lioté, F.; Petraitis, M.; et al. Ultrasound evaluation in follow-up of urate-lowering therapy in gout: The USEFUL study. Rheumatology (Oxford) 2019, 58, 410–417. [Google Scholar] [CrossRef] [PubMed]
- Cipolletta, E.; Di Battista, J.; Di Carlo, M.; Di Matteo, A.; Salaffi, F.; Grassi, W.; Filippucci, E. Sonographic estimation of monosodium urate burden predicts the fulfillment of the 2016 remission criteria for gout: A 12-month study. Arthritis Res. Ther. 2021, 23, 185. [Google Scholar] [CrossRef]
- Christiansen, S.N.; Østergaard, M.; Slot, O.; Keen, H.; Bruyn, G.A.W.; D’Agostino, M.A.; Terslev, L. Assessing the sensitivity to change of the OMERACT ultrasound structural gout lesions during urate-lowering therapy. RMD Open 2020, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hammer, H.B.; Karoliussen, L.; Terslev, L.; Haavardsholm, E.A.; Kvien, T.K.; Uhlig, T. Ultrasound shows rapid reduction of crystal depositions during a treat-to-target approach in gout patients: 12-month results from the NOR-Gout study. Ann. Rheum. Dis. 2020, 79, 1500–1505. [Google Scholar] [CrossRef]
- Ebstein, E.; Forien, M.; Norkuviene, E.; Richette, P.; Mouterde, G.; Daien, C.; Ea, H.K.; Brière, C.; Lioté, F.; Petraitis, M.; et al. UltraSound evaluation in follow-up of urate-lowering therapy in gout phase 2 (USEFUL-2): Duration of flare prophylaxis. Jt. Bone Spine 2020, 87, 647–651. [Google Scholar] [CrossRef] [PubMed]
- Dalbeth, N.; Nicolaou, S.; Baumgartner, S.; Hu, J.; Fung, M.; Choi, H.K. Presence of monosodium urate crystal deposition by dual-energy CT in patients with gout treated with allopurinol. Ann. Rheum. Dis. 2018, 77, 364–370. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Uhlig, T.; Eskild, T.; Karoliussen, L.F.; Sexton, J.; Kvien, T.K.; Haavardsholm, E.A.; Dalbeth, N.; Hammer, H.B. Two-year reduction of dual-energy CT urate depositions during a treat-to-target strategy in gout in the NOR-Gout longitudinal study. Rheumatology (Oxford) 2021. [Google Scholar] [CrossRef]
- Dalbeth, N.; Billington, K.; Doyle, A.; Frampton, C.; Tan, P.; Aati, O.; Allan, J.; Drake, J.; Horne, A.; Stamp, L.K. Effects of Allopurinol Dose Escalation on Bone Erosion and Urate Volume in Gout: A Dual-Energy Computed Tomography Imaging Study Within a Randomized, Controlled Trial. Arthritis Rheumatol. 2019, 71, 1739–1746. [Google Scholar] [CrossRef]
















Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Weaver, J.S.; Vina, E.R.; Munk, P.L.; Klauser, A.S.; Elifritz, J.M.; Taljanovic, M.S. Gouty Arthropathy: Review of Clinical Manifestations and Treatment, with Emphasis on Imaging. J. Clin. Med. 2022, 11, 166. https://doi.org/10.3390/jcm11010166
Weaver JS, Vina ER, Munk PL, Klauser AS, Elifritz JM, Taljanovic MS. Gouty Arthropathy: Review of Clinical Manifestations and Treatment, with Emphasis on Imaging. Journal of Clinical Medicine. 2022; 11(1):166. https://doi.org/10.3390/jcm11010166
Chicago/Turabian StyleWeaver, Jennifer S., Ernest R. Vina, Peter L. Munk, Andrea S. Klauser, Jamie M. Elifritz, and Mihra S. Taljanovic. 2022. "Gouty Arthropathy: Review of Clinical Manifestations and Treatment, with Emphasis on Imaging" Journal of Clinical Medicine 11, no. 1: 166. https://doi.org/10.3390/jcm11010166