
The Role of Factor Xa-Independent Pathway and Anticoagulant Therapies in Cancer-Related Stroke

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Methods
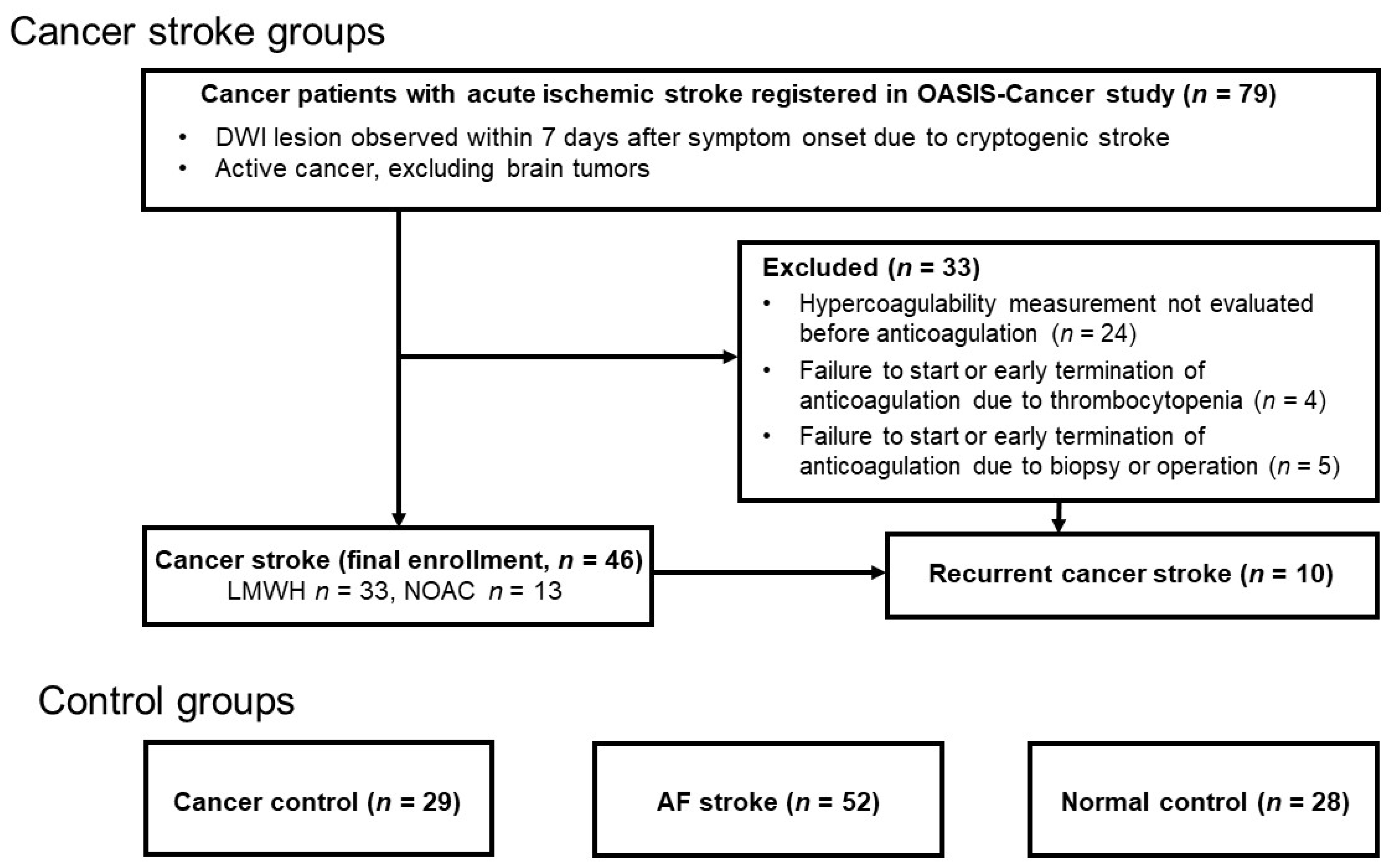
2.1. Patients
2.2. Work-Up for Stroke
2.3. Hypercoagulability Measurements
2.4. Statistical Analysis
3. Results
3.1. Baseline D-Dimer and cfDNA Levels, and Factor Xa Activity among the Groups
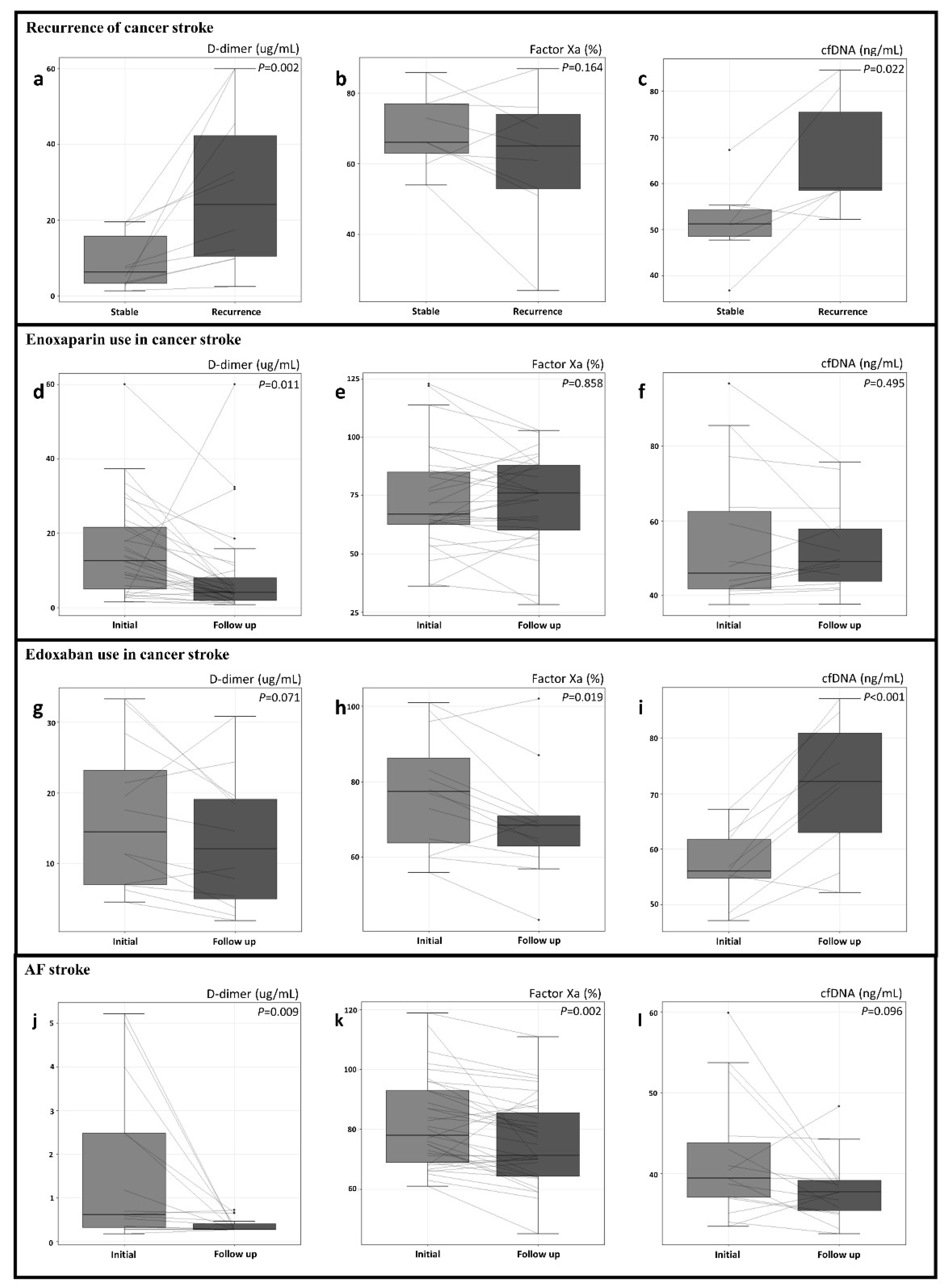
3.2. D-Dimer and cfDNA Levels, and Factor Xa Activity in Recurrent Cancer Stroke
3.3. Changes in D-Dimer and cfDNA Levels, and Factor Xa Activity after Anticoagulation
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bang, O.Y.; Chung, J.W.; Lee, M.J.; Seo, W.K.; Kim, G.M.; Ahn, M.J.; OASIS-Cancer Study Investigators. Cancer-Related Stroke: An Emerging Subtype of Ischemic Stroke with Unique Pathomechanisms. J. Stroke 2020, 22, 1–10. [Google Scholar] [CrossRef]
- Kim, S.J.; Park, J.H.; Lee, M.J.; Park, Y.G.; Ahn, M.J.; Bang, O.Y. Clues to occult cancer in patients with ischemic stroke. PLoS ONE 2012, 7, e44959. [Google Scholar] [CrossRef] [PubMed]
- Almeida, V.H.; Rondon, A.M.R.; Gomes, T.; Monteiro, R.Q. Novel Aspects of Extracellular Vesicles as Mediators of Cancer-Associated Thrombosis. Cells 2019, 8, 716. [Google Scholar] [CrossRef] [Green Version]
- Bang, O.Y.; Chung, J.W.; Cho, Y.H.; Oh, M.J.; Seo, W.K.; Kim, G.M.; Ahn, M.J. Circulating DNAs, a Marker of Neutrophil Extracellular Traposis and Cancer-Related Stroke: The OASIS-Cancer Study. Stroke 2019, 50, 2944–2947. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.J.; Chung, J.W.; Ahn, M.J.; Kim, S.; Seok, J.M.; Jang, H.M.; Kim, G.M.; Chung, C.S.; Lee, K.H.; Bang, O.Y. Hypercoagulability and Mortality of Patients with Stroke and Active Cancer: The OASIS-CANCER Study. J. Stroke 2017, 19, 77–87. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khorana, A.A.; McCrae, K.R.; Milentijevic, D.; Fortier, J.; Nelson, W.W.; Laliberte, F.; Crivera, C.; Lefebvre, P.; Yannicelli, D.; Schein, J. Current practice patterns and patient persistence with anticoagulant treatments for cancer-associated thrombosis. Res. Pract. Thromb. Haemost. 2017, 1, 14–22. [Google Scholar] [CrossRef] [PubMed]
- Navi, B.B.; Marshall, R.S.; Bobrow, D.; Singer, S.; Stone, J.B.; DeSancho, M.T.; DeAngelis, L.M. Enoxaparin vs Aspirin in Patients with Cancer and Ischemic Stroke: The TEACH Pilot Randomized Clinical Trial. JAMA Neurol. 2018, 75, 379–381. [Google Scholar] [CrossRef]
- Hindricks, G.; Potpara, T.; Dagres, N.; Arbelo, E.; Bax, J.J.; Blomström-Lundqvist, C.; Boriani, G.; Castella, M.; Dan, G.A.; Dilaveris, P.E.; et al. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association of Cardio-Thoracic Surgery (EACTS). Eur. Heart J. 2020, 42, 373–498. [Google Scholar] [CrossRef] [PubMed]
- January, C.T.; Wann, L.S.; Calkins, H.; Chen, L.Y.; Cigarroa, J.E.; Cleveland, J.C., Jr.; Ellinor, P.T.; Ezekowitz, M.D.; Field, M.E.; Furie, K.L.; et al. 2019 AHA/ACC/HRS Focused Update of the 2014 AHA/ACC/HRS Guideline for the Management of Patients with Atrial Fibrillation: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society in Collaboration With the Society of Thoracic Surgeons. Circulation 2019, 140, e125–e151. [Google Scholar] [CrossRef] [PubMed]
- Vedovati, M.C.; Germini, F.; Agnelli, G.; Becattini, C. Direct oral anticoagulants in patients with VTE and cancer: A systematic review and meta-analysis. Chest 2015, 147, 475–483. [Google Scholar] [CrossRef] [PubMed]
- Cosmi, B. An update on the efficacy and safety of novel anticoagulants for cancer associated thrombosis. Expert Opin Pharm. 2021, 22, 583–594. [Google Scholar] [CrossRef] [PubMed]
- Raskob, G.E.; van Es, N.; Verhamme, P.; Carrier, M.; Di Nisio, M.; Garcia, D.; Grosso, M.A.; Kakkar, A.K.; Kovacs, M.J.; Mercuri, M.F.; et al. Edoxaban for the Treatment of Cancer-Associated Venous Thromboembolism. N. Engl. J. Med. 2018, 378, 615–624. [Google Scholar] [CrossRef] [PubMed]
- Agnelli, G.; Becattini, C.; Meyer, G.; Munoz, A.; Huisman, M.V.; Connors, J.M.; Cohen, A.; Bauersachs, R.; Brenner, B.; Torbicki, A.; et al. Apixaban for the Treatment of Venous Thromboembolism Associated with Cancer. N. Engl. J. Med. 2020, 382, 1599–1607. [Google Scholar] [CrossRef]
- Lyman, G.H.; Khorana, A.A.; Kuderer, N.M.; Lee, A.Y.; Arcelus, J.I.; Balaban, E.P.; Clarke, J.M.; Flowers, C.R.; Francis, C.W.; Gates, L.E.; et al. Venous thromboembolism prophylaxis and treatment in patients with cancer: American Society of Clinical Oncology clinical practice guideline update. J. Clin. Oncol. 2013, 31, 2189–2204. [Google Scholar] [CrossRef] [PubMed]
- Farge, D.; Bounameaux, H.; Brenner, B.; Cajfinger, F.; Debourdeau, P.; Khorana, A.A.; Pabinger, I.; Solymoss, S.; Douketis, J.; Kakkar, A. International clinical practice guidelines including guidance for direct oral anticoagulants in the treatment and prophylaxis of venous thromboembolism in patients with cancer. Lancet Oncol. 2016, 17, e452–e466. [Google Scholar] [CrossRef] [Green Version]
- Lyman, G.H.; Bohlke, K.; Khorana, A.A.; Kuderer, N.M.; Lee, A.Y.; Arcelus, J.I.; Balaban, E.P.; Clarke, J.M.; Flowers, C.R.; Francis, C.W.; et al. Venous thromboembolism prophylaxis and treatment in patients with cancer: American society of clinical oncology clinical practice guideline update 2014. J. Clin. Oncol. 2015, 33, 654–656. [Google Scholar] [CrossRef] [PubMed]
- Gon, Y.; Sakaguchi, M.; Takasugi, J.; Mochizuki, H. Ischemic stroke in cancer patients treated with direct oral anticoagulants for venous thromboembolism. Thromb. Res. 2017, 154, 16–18. [Google Scholar] [CrossRef] [PubMed]
- Seok, J.M.; Kim, S.G.; Kim, J.W.; Chung, C.S.; Kim, G.M.; Lee, K.H.; Bang, O.Y. Coagulopathy and embolic signal in cancer patients with ischemic stroke. Ann. Neurol. 2010, 68, 213–219. [Google Scholar] [CrossRef]
- Toh, C.H.; Hoots, W.K. The scoring system of the Scientific and Standardisation Committee on Disseminated Intravascular Coagulation of the International Society on Thrombosis and Haemostasis: A 5-year overview. J. Thromb. Haemost. 2007, 5, 604–606. [Google Scholar] [CrossRef] [PubMed]
- Ay, H.; Furie, K.L.; Singhal, A.; Smith, W.S.; Sorensen, A.G.; Koroshetz, W.J. An evidence-based causative classification system for acute ischemic stroke. Ann. Neurol. 2005, 58, 688–697. [Google Scholar] [CrossRef] [PubMed]
- Cabral, K.P.; Ansell, J. Oral direct factor Xa inhibitors for stroke prevention in atrial fibrillation. Nat. Rev. Cardiol. 2012, 9, 385–391. [Google Scholar] [CrossRef] [PubMed]
- Khorana, A.A.; Ahrendt, S.A.; Ryan, C.K.; Francis, C.W.; Hruban, R.H.; Hu, Y.C.; Hostetter, G.; Harvey, J.; Taubman, M.B. Tissue factor expression, angiogenesis, and thrombosis in pancreatic cancer. Clin. Cancer Res. 2007, 13, 2870–2875. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rondon, A.M.R.; Kroone, C.; Kapteijn, M.Y.; Versteeg, H.H.; Buijs, J.T. Role of Tissue Factor in Tumor Progression and Cancer-Associated Thrombosis. Semin. Thromb. Hemost. 2019, 45, 396–412. [Google Scholar] [CrossRef] [PubMed]
- Bang, O.Y.; Chung, J.W.; Lee, M.J.; Kim, S.J.; Cho, Y.H.; Kim, G.M.; Chung, C.S.; Lee, K.H.; Ahn, M.J.; Moon, G.J. Cancer Cell-Derived Extracellular Vesicles Are Associated with Coagulopathy Causing Ischemic Stroke via Tissue Factor-Independent Way: The OASIS-CANCER Study. PLoS ONE 2016, 11, e0159170. [Google Scholar] [CrossRef]
- Saffarzadeh, M. Neutrophil Extracellular Traps as a Drug Target to Counteract Chronic and Acute Inflammation. Curr. Pharm. Biotechnol. 2018, 19, 1196–1202. [Google Scholar] [CrossRef] [PubMed]
- Demers, M.; Wagner, D.D. NETosis: A new factor in tumor progression and cancer-associated thrombosis. Semin. Thromb. Hemost. 2014, 40, 277–283. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Downing, L.J.; Strieter, R.M.; Kadell, A.M.; Wilke, C.A.; Greenfield, L.J.; Wakefield, T.W. Low-dose low-molecular-weight heparin is anti-inflammatory during venous thrombosis. J. Vasc. Surg. 1998, 28, 848–854. [Google Scholar] [CrossRef] [Green Version]
- Loizou, E.; Mayhew, D.J.; Martlew, V.; Murthy, B.V.S. Implications of deranged activated partial thromboplastin time for anaesthesia and surgery. Anaesthesia 2018, 73, 1557–1563. [Google Scholar] [CrossRef] [Green Version]
- Hart, R.G.; Sharma, M.; Mundl, H.; Kasner, S.E.; Bangdiwala, S.I.; Berkowitz, S.D.; Swaminathan, B.; Lavados, P.; Wang, Y.; Wang, Y.; et al. Rivaroxaban for Stroke Prevention after Embolic Stroke of Undetermined Source. N. Engl. J. Med. 2018, 378, 2191–2201. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Groups | P | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Cancer Stroke (CS) | Cancer Control (CC, N = 29) | AF Stroke(AF, N = 52) | Normal Control (NC, N = 28) | LMWH vs. DOAC | CS vs. CC | CS vs. AF | CS vs. NC | |||
| Total (N = 46) | LMWH (N = 33) | DOAC (N = 13) | ||||||||
| Age (years) | 64.4 ± 10.3 | 64.5 ± 10.8 | 64.0 ± 9.1 | 64.1 ± 9.6 | 71.5 ± 8.8 | 61.8 ± 4.4 | 0.593 | 0.910 | <0.001 | 0.144 |
| Male | 32 (69.6%) | 22 (66.7%) | 10 (76.9%) | 15 (51.7%) | 28 (53.9%) | 7 (25.0%) | 0.817 | 0.190 | <0.001 | <0.001 |
| Risk factor | ||||||||||
| Hypertension | 19 (41.3%) | 15 (45.5%) | 4 (30.8%) | 7 (24.1%) | 30 (57.7%) | 5 (17.9%) | 0.641 | 0.203 | <0.001 | 0.067 |
| Diabetes | 10 (21.7%) | 5 (15.2%) | 5 (38.5%) | 1 (3.5%) | 8 (15.4%) | 1 (3.6%) | 0.152 | 0.065 | <0.001 | 0.073 |
| Hyperlipidemia | 9 (19.6%) | 7 (21.2%) | 2 (15.4%) | 1 (3.5%) | 22 (42.3%) | 1 (3.6%) | >0.99 | 0.099 | <0.001 | 0.109 |
| Current smoking | 11 (23.9%) | 9 (27.3%) | 2 (15.4%) | 8 (27.6%) | 4 (7.7%) | 2 (7.1%) | 0.696 | 0.933 | <0.001 | 0.128 |
| Cancer type | ||||||||||
| Adenocarcinoma | 31 (67.4%) | 22 (66.7%) | 9 (69.2%) | 24 (82.8%) | N/A | N/A | >0.99 | 0.231 | N/A | N/A |
| Systemic metastasis | 33 (71.7%) | 23 (69.7%) | 10 (76.9%) | 17 (58.6%) | N/A | N/A | 0.973 | 0.357 | N/A | N/A |
| Primary cancer lesion | 0.638 | N/A | N/A | N/A | ||||||
| Lung | 18 (39.1%) | 11 (33.3%) | 7 (53.9%) | 29 (100.0%) | N/A | N/A | ||||
| Gastrointestinal | 6 (13.0%) | 5 (15.2%) | 1 (7.7%) | 0 (0.0%) | N/A | N/A | ||||
| Hepatobiliary | 13 (28.3%) | 10 (30.3%) | 3 (23.1%) | 0 (0.0%) | N/A | N/A | ||||
| Breast-gynecology | 6 (13.0%) | 4 (12.1%) | 2 (15.4%) | 0 (0.0%) | N/A | N/A | ||||
| Other | 3 (6.5%) | 3 (9.1%) | 0 (0.0%) | 0 (0.0%) | N/A | N/A | ||||
| Treatment within 4 weeks before enrollment | ||||||||||
| Surgery | 5 (10.9%) | 4 (12.1%) | 1 (7.7%) | 3 (10.3%) | N/A | N/A | 0.999 | 0.999 | N/A | N/A |
| Chemotherapy | 24 (52.2%) | 18 (54.6%) | 6 (46.2%) | 13 (44.8%) | N/A | N/A | 0.853 | 0.702 | N/A | N/A |
| Radiotherapy | 10 (21.7%) | 6 (18.2%) | 4 (30.8%) | 5 (17.2%) | N/A | N/A | 0.593 | 0.859 | N/A | N/A |
| Laboratory results | ||||||||||
| D-dimer, μg/mL | 19.0 ± 15.1 (n = 46) | 16.8 ± 16.6 (n = 33) | 17.0 ± 11.0 (n = 13) | 0.8 ± 1.3 (n = 23) | 1.5 ± 1.9 (n = 39) | 0.4 ± 0.3 (n = 28) | 0.863 | <0.001 | <0.001 | <0.001 |
| Factor Xa, % | 70.8 ± 23.4 (n = 44) | 69.4 ± 25.0 (n = 31) | 74.2 ± 19.3 (n = 13) | 95.5 ± 12.6 (n = 29) | 79.2 ± 14.2 (n = 52) | 98.1 ± 13.5 (n = 28) | 0.245 | <0.001 | 0.041 | <0.001 |
| cfDNA, ng/mL | 56.6 ± 16.7 (n = 29) | 55.7 ± 19.4 (n = 19) | 58.3 ± 10.6 (n = 10) | 37.2 ± 5.0 (n = 17) | 43.2 ± 7.9 (n = 43) | 38.6 ± 6.6 (n = 28) | 0.633 | <0.001 | <0.001 | <0.001 |
| Platelet count, 103/μL | 165.2 ± 89.5 | 172.2 ± 92.9 | 147.6 ± 81.1 | 222.0 ± 82.1 | 215.2 ± 70.1 | N/A | 0.301 | <0.001 | <0.001 | N/A |
| (n = 46) | (n = 33) | (n = 13) | (n = 29) | (n = 52) | ||||||
| PT (INR) | 1.4 ± 0.6 | 1.4 ± 0.7 | 1.3 ± 0.4 | 1.0 ± 0.1 | 1.0 ± 0.1 | N/A | 0.301 | <0.001 | <0.001 | N/A |
| (n = 46) | (n = 33) | (n = 13) | (n = 29) | (n = 52) | ||||||
| aPTT (sec) | 43.7 ± 26.5 | 46.1 ± 30.8 | 37.6 ± 6.8 | 34.1 ± 3.4 | 34.4 ± 3.7 | N/A | 0.151 | <0.001 | <0.001 | N/A |
| (n = 46) | (n = 33) | (n = 13) | (n = 29) | (n = 52) | ||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, H.J.; Chung, J.-W.; Bang, O.Y.; Cho, Y.H.; Lim, Y.J.; Hwang, J.; Seo, W.-K.; Kim, G.-M.; Kim, H.-J.; Ahn, M.-J. The Role of Factor Xa-Independent Pathway and Anticoagulant Therapies in Cancer-Related Stroke. J. Clin. Med. 2022, 11, 123. https://doi.org/10.3390/jcm11010123
Kim HJ, Chung J-W, Bang OY, Cho YH, Lim YJ, Hwang J, Seo W-K, Kim G-M, Kim H-J, Ahn M-J. The Role of Factor Xa-Independent Pathway and Anticoagulant Therapies in Cancer-Related Stroke. Journal of Clinical Medicine. 2022; 11(1):123. https://doi.org/10.3390/jcm11010123
Chicago/Turabian StyleKim, Hyung Jun, Jong-Won Chung, Oh Young Bang, Yeon Hee Cho, Yun Jeong Lim, Jaechun Hwang, Woo-Keun Seo, Gyeong-Moon Kim, Hee-Jin Kim, and Myung-Ju Ahn. 2022. "The Role of Factor Xa-Independent Pathway and Anticoagulant Therapies in Cancer-Related Stroke" Journal of Clinical Medicine 11, no. 1: 123. https://doi.org/10.3390/jcm11010123