
Usefulness of the MAGGIC Score in Predicting the Competing Risk of Non-Sudden Death in Heart Failure Patients Receiving an Implantable Cardioverter-Defibrillator: A Sub-Analysis of the OBSERVO-ICD Registry

 , , ,
, , ,
Abstract
:1. Introduction
2. Material and Methods
2.1. Data Collection
2.2. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Levy, W.C.; Mozaffarian, D.; Linker, D.T.; Sutradhar, S.C.; Anker, S.D.; Cropp, A.B.; Anand, I.; Maggioni, A.; Burton, P.; Sullivan, M.D.; et al. The seattle heart failure model: Prediction of survival in heart failure. Circulation 2006, 113, 1424–1433. [Google Scholar] [CrossRef]
- Pocock, S.J.; Ariti, C.A.; McMurray, J.J.; Maggioni, A.; Kober, L.; Squire, I.B.; Swedberg, K.; Dobson, J.; Poppe, K.K.; Whalley, G.A.; et al. Predicting survival in heart failure: A risk score based on 39,372 patients from 30 studies. Eur. Heart J. 2013, 34, 1404–1413. [Google Scholar] [CrossRef] [PubMed]
- Canepa, M.; Fonseca, C.; Chioncel, O.; Laroche, C.; Crespo-Leiro, M.G.; Coats, A.J.S.; Mebazaa, A.; Piepoli, M.F.; Tavazzi, L.; Maggioni, A.P. Performance of prognostic risk scores in chronic heart failure patients enrolled in the european society of cardiology heart failure long-term registry. JACC Heart Fail. 2018, 6, 452–462. [Google Scholar] [CrossRef]
- Mozaffarian, D.; Anker, S.D.; Anand, I.; Linker, D.T.; Sullivan, M.D.; Cleland, J.G.F.; Carson, P.E.; Maggioni, A.P.; Mann, D.L.; Pitt, B.; et al. Prediction of mode of death in heart failure: The Seattle heart failure model. Circulation 2007, 116, 392–398. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Canepa, M.; Ameri, P.; Lucci, D.; Nicolosi, G.L.; Marchioli, R.; Porcu, M.; Tognoni, G.; Franzosi, M.G.; Latini, R.; Maseri, A.; et al. Modes of death and prognostic outliers in chronic heart failure. Am. Heart J. 2019, 208, 100–109. [Google Scholar] [CrossRef] [PubMed]
- Shen, L.; Jhund, P.S.; Petrie, M.C.; Claggett, B.L.; Barlera, S.; Cleland, J.G.F.; Dargie, M.B.; Granger, C.C.; Kjekshus, J.; Køber, L.; et al. Declining risk of sudden death in heart failure. N. Engl. J. Med. 2017, 377, 41–51. [Google Scholar] [CrossRef]
- Nichol, G.; Sayre, M.R.; Guerra, F.; Poole, J. Defibrillation for ventricular fibrillation: A shocking update. J. Am. Coll. Cardiol. 2017, 70, 1496–1509. [Google Scholar] [CrossRef] [PubMed]
- Ruwald, A.C.; Vinther, M.; Gislason, G.H.; Johansen, J.B.; Nielsen, J.C.; Petersen, H.H.; Riahi, S.; Jons, C. The impact of co-morbidity burden on appropriate implantable cardioverter defibrillator therapy and all-cause mortality: Insight from Danish nationwide clinical registers. Eur. J. Heart Fail. 2017, 19, 377–386. [Google Scholar] [CrossRef] [Green Version]
- Beggs, S.A.S.; Gardner, R.S.; McMurray, J.J.V. Who benefits from a defibrillator-balancing the risk of sudden versus non-sudden death. Curr. Heart Fail. Rep. 2018, 15, 376–389. [Google Scholar] [CrossRef] [Green Version]
- Koller, M.T.; Schaer, B.; Wolbers, M.; Sticherling, C.; Bucher, H.C.; Osswald, S. Death without prior appropriate implantable cardioverter-defibrillator therapy: A competing risk study. Circulation 2008, 117, 1918–1926. [Google Scholar] [CrossRef] [Green Version]
- Weber, D.; Koller, M.; Theuns, D.; Yap, S.; Kuhne, M.; Sticherling, C.; Reichlin, T.; Szili-Torok, T.; Osswald, S.; Schaer, B. Predicting defibrillator benefit in patients with cardiac resynchronization therapy: A competing risk study. Heart Rhythm 2019, 16, 1057–1064. [Google Scholar] [CrossRef] [PubMed]
- Guerra, F.; Palmisano, P.; Dell’Era, G.; Ziacchi, M.; Ammendola, E.; Bonelli, P.; Patani, F.; Cupido, C.; Devecchi, C.; Accogli, M.; et al. Implantable cardioverter-defibrillator programming and electrical storm: Results of the OBSERVational registry on long-term outcome of ICD patients (OBSERVO-ICD). Heart Rhythm 2016, 13, 1987–1992. [Google Scholar] [CrossRef] [PubMed]
- Guerra, F.; Palmisano, P.; Dell’Era, G.; Ziacchi, M.; Ammendola, E.; Pongetti, G.; Bonelli, P.; Patani, F.; Devecchi, C.; Accogli, M.; et al. Cardiac resynchronization therapy and electrical storm: Results of the OBSERVational registry on long-term outcome of ICD patients (OBSERVO-ICD). Europace 2018, 20, 979–985. [Google Scholar] [CrossRef]
- Poupin, P.; Bouleti, C.; Degand, B.; Paccalin, M.; Le Gal, F.; Bureau, M.L.; Alos, B.; Roumegou, P.; Christiaens, L.; Ingrand, P.; et al. Prognostic value of Charlson comorbidity index in the elderly with a cardioverter defibrillator implantation. Int. J. Cardiol. 2020, 314, 64–69. [Google Scholar] [CrossRef]
- Van der Heijden, A.C.; van Rees, J.B.; Levy, W.C.; van der Bom, J.G.; Cannegieter, S.C.; de Bie, M.K.; van Erven, L.; Schalij, M.J.; Borleffs, C.J.W. Application and comparison of the FADES, MADIT, and SHFM-D risk models for risk stratification of prophylactic implantable cardioverter-defibrillator treatment. Europace 2017, 19, 72–80. [Google Scholar] [CrossRef]
- Sharma, A.; Al-Khatib, S.M.; Ezekowitz, J.A.; Cooper, L.B.; Fordyce, C.B.; Michael Felker, G.; Bardy, G.H.; Poole, J.E.; Bigger, J.T.; Buxton, A.E.; et al. Implantable cardioverter-defibrillators in heart failure patients with reduced ejection fraction and diabetes. Eur. J. Heart Fail. 2018, 20, 1031–1038. [Google Scholar] [CrossRef] [PubMed]
- Van Rees, J.B.; Borleffs, C.J.F.; van Welsenes, G.H.; van der Velde, E.T.; Bax, J.J.; van Erven, L.; Putter, H.; van der Bom, J.G.; Schalij, M.J. Clinical prediction model for death prior to appropriate therapy in primary prevention implantable cardioverter defibrillator patients with ischaemic heart disease: The FADES risk score. Heart 2012, 98, 872–877. [Google Scholar] [CrossRef] [PubMed]
- Goldenberg, I.; Vyas, A.K.; Hall, J.W.; Moss, A.J.; Wang, H.; He, H.; Zareba, W.; McNitt, S.; Andrews, M.L. Risk stratification for primary implantation of a cardioverter-defibrillator in patients with ischemic left ventricular dysfunction. J. Am. Coll. Cardiol. 2008, 22, 288–296. [Google Scholar] [CrossRef] [Green Version]
- Levy, W.C.; Lee, K.L.; Hellkamp, A.S.; Poole, J.E.; Mozaffarian, D.; Linker, D.T.; Maggioni, A.P.; Anand, I.; Poole-Wilson, P.A.; Fishbein, D.P.; et al. Maximizing survival benefit with primary prevention implantable cardioverter-defibrillator therapy in a heart failure population. Circulation 2009, 120, 835–842. [Google Scholar] [CrossRef] [Green Version]
- Levy, W.C.; Li, Y.; Reed, S.D.; Zile, M.R.; Shadman, R.; Dardas, T.; Whellan, D.J.; Schulman, K.A.; Ellis, S.J.; Neilson, M.; et al. Does the implantable cardioverter-defibrillator benefit vary with the estimated proportional risk of sudden death in heart failure patients? JACC Clin. Electrophysiol. 2017, 3, 291–298. [Google Scholar] [CrossRef]
- Bilchick, K.C.; Wang, Y.; Cheng, A.; Curtis, J.P.; Dharmarajan, K.; Stukenborg, G.J.; Shadman, R.; Anand, I.; Lund, L.H.; Dahlström, U.; et al. Seattle heart failure and proportional risk models predict benefit from implantable cardioverter-defibrillators. J. Am. Coll. Cardiol. 2017, 69, 2606–2618. [Google Scholar] [CrossRef] [PubMed]
- Ameri, P.; Canepa, M.; Anker, M.S.; Belenkov, Y.; Bergler-Klein, J.; Cohen-Solal, A.; Farmakis, D.; López-Fernández, T.; Lainscak, M.; Pudil, R.; et al. Cancer diagnosis in patients with heart failure: Epidemiology, clinical implications and gaps in knowledge. Eur. J. Heart Fail. 2018, 20, 879–887. [Google Scholar] [CrossRef] [PubMed]
- Canepa, M.; Franssen, F.M.E.; Olschewski, H.; Lainscak, M.; Bohm, M.; Tavazzi, L.; Rosenkranz, S. Diagnostic and therapeutic gaps in patients with heart failure and chronic obstructive pulmonary disease. JACC Heart Fail. 2019, 7, 823–833. [Google Scholar] [CrossRef] [PubMed]
- Boriani, G.; Savelieva, I.; Dan, G.A.; Deharo, J.C.; Ferro, C.; Israel, C.W.; Lane, D.A.; La Manna, G.; Morton, J.; Mitjans, A.M.; et al. Chronic kidney disease in patients with cardiac rhythm disturbances or implantable electrical devices: Clinical significance and implications for decision making—A position paper of the European Heart Rhythm Association endorsed by the Heart Rhythm Society and the Asia Pacific Heart Rhythm Society. Europace 2015, 17, 1169–1196. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Overall Sample n = 1089 | Low MAGGIC Risk n = 345 3-Year Death Probability < 23% | Mid MAGGIC Risk n = 398 3-Year Death Probability 23–39% | High MAGGIC Risk n = 346 3-Year Death Probability > 39% | p Value | |
|---|---|---|---|---|---|
| Age, years | 66.1 ± 11.8 | 56.9 ± 11.0 | 66.7 ± 9.6 | 74.4 ± 7.9 | <0.0001 |
| Male sex, % | 77.8 | 79.7 | 74.1 | 79.1 | 0.124 |
| Systolic blood pressure (mmHg) | 121.9 ± 16.9 | 124.5 ± 16.8 | 122.8 ± 17.0 | 118.3 ± 16.3 | <0.0001 |
| BMI (kg/m2) | 26.3 ± 4.6 | 27.7 ± 4.9 | 26.1 ± 4.6 | 25.2 ± 4.0 | <0.0001 |
| Obesity | 25.9 | 30.9 | 26.9 | 18.9 | 0.001 |
| Dyslipidemia, % | 64.7 | 61.0 | 63.6 | 67.9 | 0.154 |
| COPD, % | 26.8 | 11.4 | 27.9 | 40.4 | <0.0001 |
| NYHA | <0.0001 | ||||
| 1 | 6.8 | 15.0 | 4.2 | 1.7 | |
| 2 | 51.9 | 73.0 | 53.4 | 28.9 | |
| 3 | 39.7 | 12.0 | 41.9 | 65.0 | |
| 4 | 1.6 | 0.0 | 0.5 | 4.3 | |
| Current smoking | 9.5 | 11.98 | 8.98 | 7.45 | 0.110 |
| Hypertension | 77.0 | 70.5 | 77.6 | 82.5 | 0.0007 |
| Diabetes, % | 34.4 | 17.8 | 34.2 | 50.1 | <0.0001 |
| Chronic kidney disease, % | 24.8 | 9.8 | 23.4 | 41.3 | <0.0001 |
| Atrial fibrillation (paroxysmal or persistent), % | 14.9 | 11.2 | 14.7 | 19.5 | 0.008 |
| Atrial fibrillation (permanent), % | 13.6 | 9.2 | 14.5 | 17.2 | 0.007 |
| Left ventricular ejection fraction, % | 28.4 ± 5.6 | 30.1 ± 5.5 | 28.1 ± 5.4 | 27.2 ± 5.5 | <0.0001 |
| HF diagnosis within 18 months, % | 45.6 | 41.5 | 46.1 | 47.9 | 0.211 |
| Creatinine (mg/dL) | 1.2 ± 0.6 | 1.0 ± 0.4 | 1.2 ± 0.6 | 1.5 ± 0.8 | <0.0001 |
| Hemoglobin (g/dL) | 12.9 ± 1.8 | 13.5 ± 1.7 | 12.9 ± 1.7 | 12.6 ± 2.0 | <0.0001 |
| Uric Acid (mg/dL) | 6.4 ± 1.9 | 6.2 ± 1.8 | 6.4 ± 1.9 | 6.6 ± 2.2 | 0.004 |
| Ischemic etiology, % | 52.5 | 44.9 | 51.5 | 61.3 | <0.0001 |
| Previous CABG, % | 23.3 | 17.1 | 21.1 | 32.1 | <0.0001 |
| Previous PCI, % | 31.1 | 26.4 | 32.4 | 34.4 | 0.059 |
| ICD type, % | 0.001 | ||||
| Single chamber | 24.2 | 29.6 | 19.6 | 24.3 | |
| Dual chamber | 31.8 | 34.8 | 32.7 | 27.8 | |
| Biventricular | 44.0 | 35.7 | 47.7 | 48.0 | |
| Beta blockers, % | 91.1 | 96.5 | 90.5 | 86.4 | <0.0001 |
| ACEi/ARB, % | 88.7 | 91.9 | 88.7 | 85.6 | 0.031 |
| Aspirin, % | 59.6 | 58.8 | 59.1 | 60.7 | 0.86 |
| Thienopyridines, % | 18.7 | 13.7 | 21.1 | 21.0 | 0.022 |
| Anticoagulant, % | 30.1 | 22.6 | 30.7 | 36.8 | 0.0002 |
| Diuretics, % | 83.2 | 78.0 | 83.9 | 87.6 | 0.003 |
| Antialdosterone drugs, % | 57.6 | 53.9 | 56.8 | 62.1 | 0.084 |
| Statins, % | 64.5 | 61.2 | 66.6 | 65.5 | 0.274 |
| Nitrates, % | 17.6 | 12.2 | 17.1 | 23.7 | 0.0003 |
| Amiodarone, % | 21.6 | 17.4 | 21.9 | 25.4 | 0.036 |
| Other antiarrhythmic drugs, % | 1.7 | 0.6 | 1.3 | 3.5 | 0.01 |
| Digitalis, % | 11.2 | 8.4 | 13.6 | 11.3 | 0.084 |
| Follow-Up Time, Months | 12 | 24 | 36 | 48 | 60 |
|---|---|---|---|---|---|
| ICD therapy vs. non-sudden death | |||||
| Low MAGGIC risk, n = 345 | |||||
| Patients at risk | 315 | 285 | 196 | 120 | 10 |
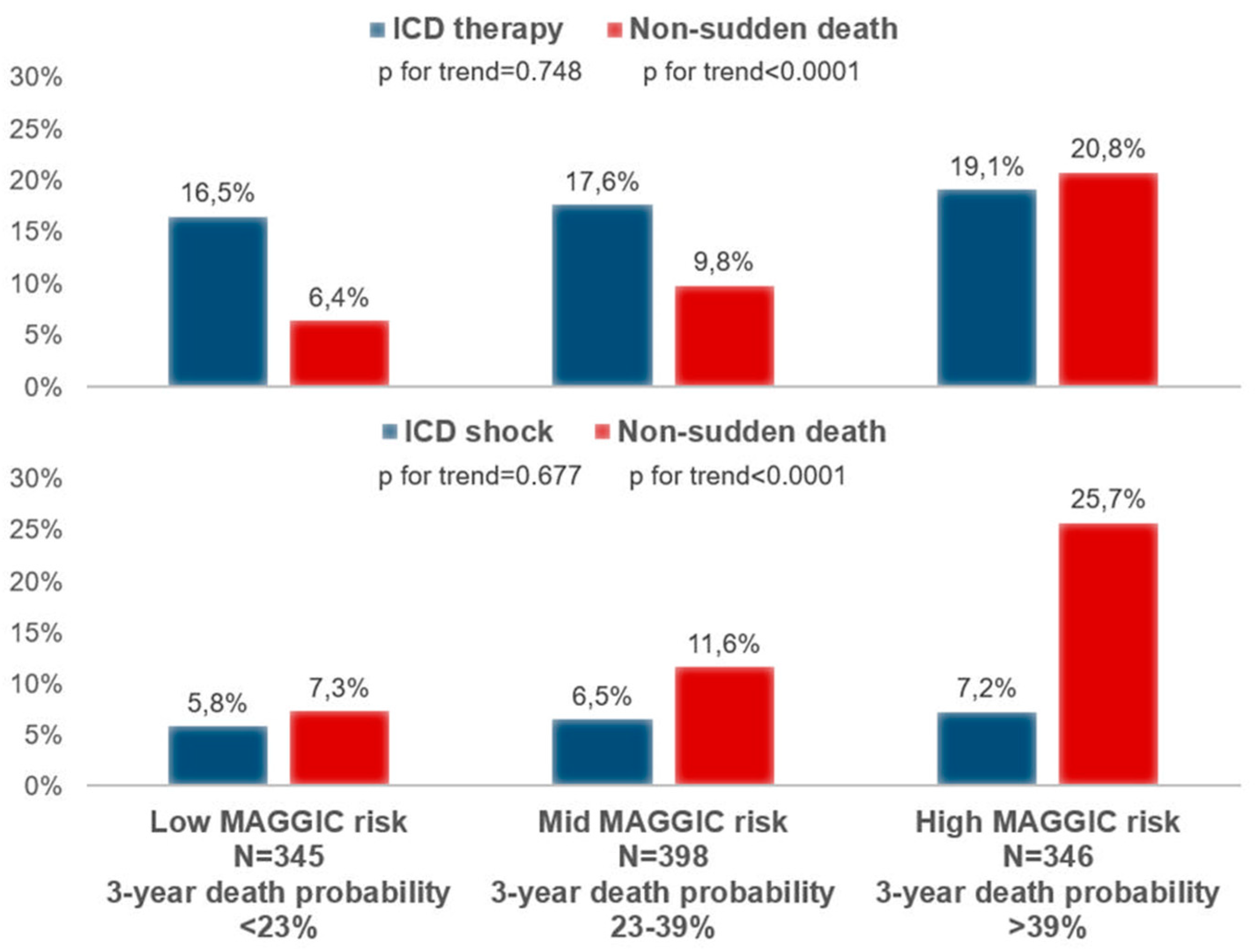
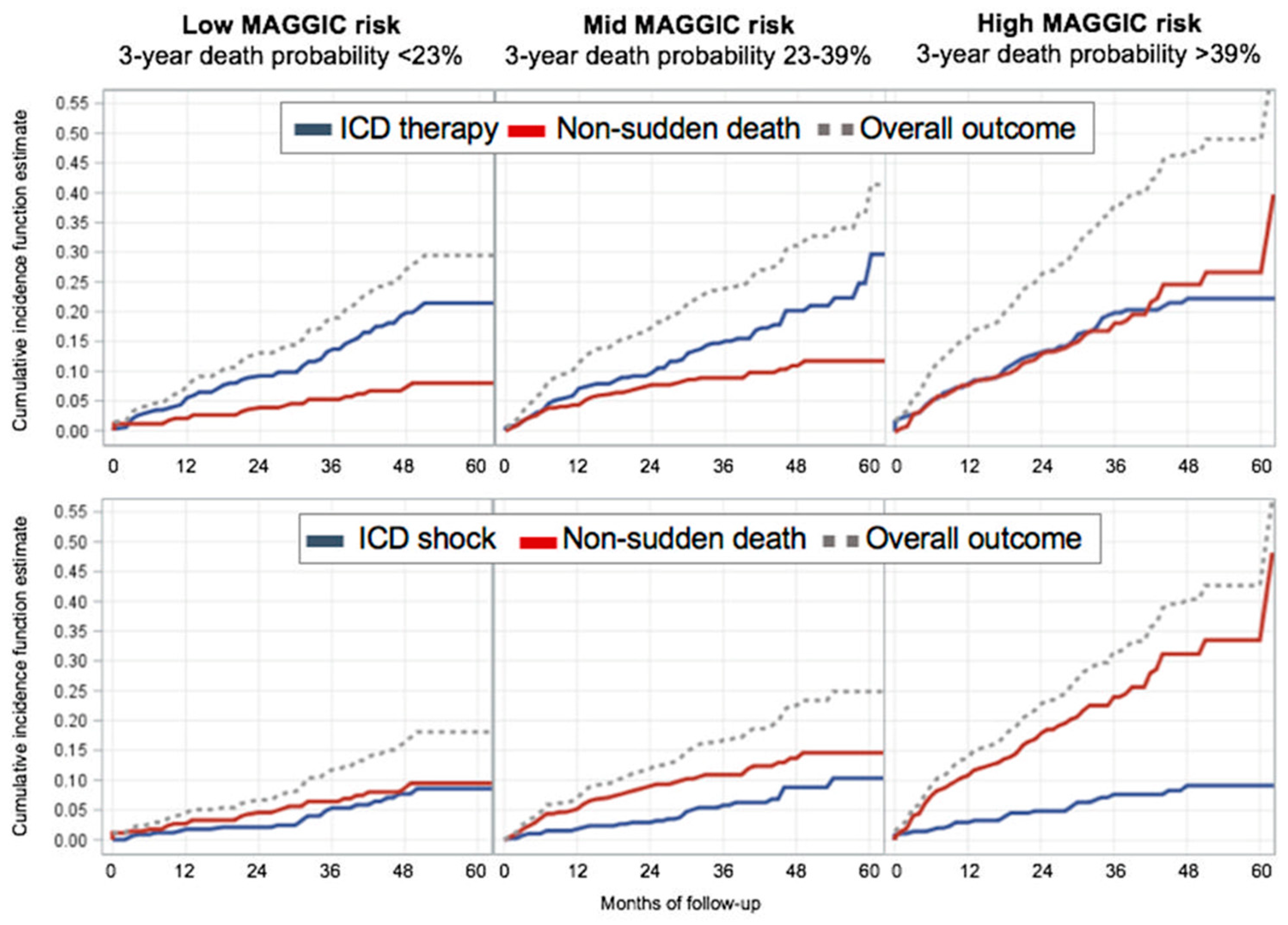
| ICD therapy | 5.6% | 9.2% | 13.7% | 19.9% | 21.5% |
| Non-sudden death | 2.0% | 3.9% | 5.3% | 7.3% | 8.0% |
| Mid MAGGIC risk, n = 398 | |||||
| Patients at risk | 352 | 310 | 207 | 101 | 13 |
| ICD therapy | 7.1% | 9.7% | 15.0% | 20.2% | 29.7% |
| Non-sudden death | 4.3% | 7.7% | 8.9% | 10.9% | 11.7% |
| High MAGGIC risk, n = 346 | |||||
| Patients at risk | 279 | 235 | 145 | 75 | 5 |
| ICD therapy | 8.0% | 13.3% | 19.9% | 22.3% | 22.3% |
| Non-sudden death | 7.8% | 13.1% | 18.2% | 24.6% | 26.7% |
| ICD shock vs. non-sudden death | |||||
| Low MAGGIC risk, n = 345 | |||||
| Patients at risk | 315 | 285 | 196 | 120 | 10 |
| ICD shock | 1.8% | 2.1% | 5.3% | 7.7% | 8.6% |
| Non-sudden death | 2.7% | 4.6% | 6.4% | 8.7% | 9.5% |
| Mid MAGGIC risk, n = 398 | |||||
| Patients at risk | 352 | 310 | 207 | 101 | 13 |
| ICD shock | 1.8% | 2.9% | 5.8% | 8.8% | 10.3% |
| Non-sudden death | 5.2% | 9.0% | 10.9% | 13.7% | 14.6% |
| High MAGGIC risk, n = 346 | |||||
| Patients at risk | 279 | 235 | 145 | 75 | 5 |
| ICD shock | 3.0% | 4.9% | 7.7% | 9.1% | 9.2% |
| Non-sudden death | 10.8% | 17.9% | 24.0% | 31.2% | 33.5% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Canepa, M.; Palmisano, P.; Dell’Era, G.; Ziacchi, M.; Ammendola, E.; Accogli, M.; Occhetta, E.; Biffi, M.; Nigro, G.; Ameri, P.; et al. Usefulness of the MAGGIC Score in Predicting the Competing Risk of Non-Sudden Death in Heart Failure Patients Receiving an Implantable Cardioverter-Defibrillator: A Sub-Analysis of the OBSERVO-ICD Registry. J. Clin. Med. 2022, 11, 121. https://doi.org/10.3390/jcm11010121
Canepa M, Palmisano P, Dell’Era G, Ziacchi M, Ammendola E, Accogli M, Occhetta E, Biffi M, Nigro G, Ameri P, et al. Usefulness of the MAGGIC Score in Predicting the Competing Risk of Non-Sudden Death in Heart Failure Patients Receiving an Implantable Cardioverter-Defibrillator: A Sub-Analysis of the OBSERVO-ICD Registry. Journal of Clinical Medicine. 2022; 11(1):121. https://doi.org/10.3390/jcm11010121
Chicago/Turabian StyleCanepa, Marco, Pietro Palmisano, Gabriele Dell’Era, Matteo Ziacchi, Ernesto Ammendola, Michele Accogli, Eraldo Occhetta, Mauro Biffi, Gerardo Nigro, Pietro Ameri, and et al. 2022. "Usefulness of the MAGGIC Score in Predicting the Competing Risk of Non-Sudden Death in Heart Failure Patients Receiving an Implantable Cardioverter-Defibrillator: A Sub-Analysis of the OBSERVO-ICD Registry" Journal of Clinical Medicine 11, no. 1: 121. https://doi.org/10.3390/jcm11010121