
Methodological Aspects of Randomized Controlled Trials for Tinnitus: A Systematic Review and How a Decision Support System Could Overcome Barriers

 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Inclusion Criteria
2.2. Exclusion Criteria
2.3. Information Sources
2.4. Search
2.5. Study Selection
2.6. Data Collection Process
2.7. Extracted Data Items
- Study identificationAuthor, year of publication.
- Methods and inclusion criteria
- Methods and study procedures
- Methods and outcome measures
- Results
2.8. Risk of Bias in Individual Studies
2.9. Synthesis of Results
3. Results
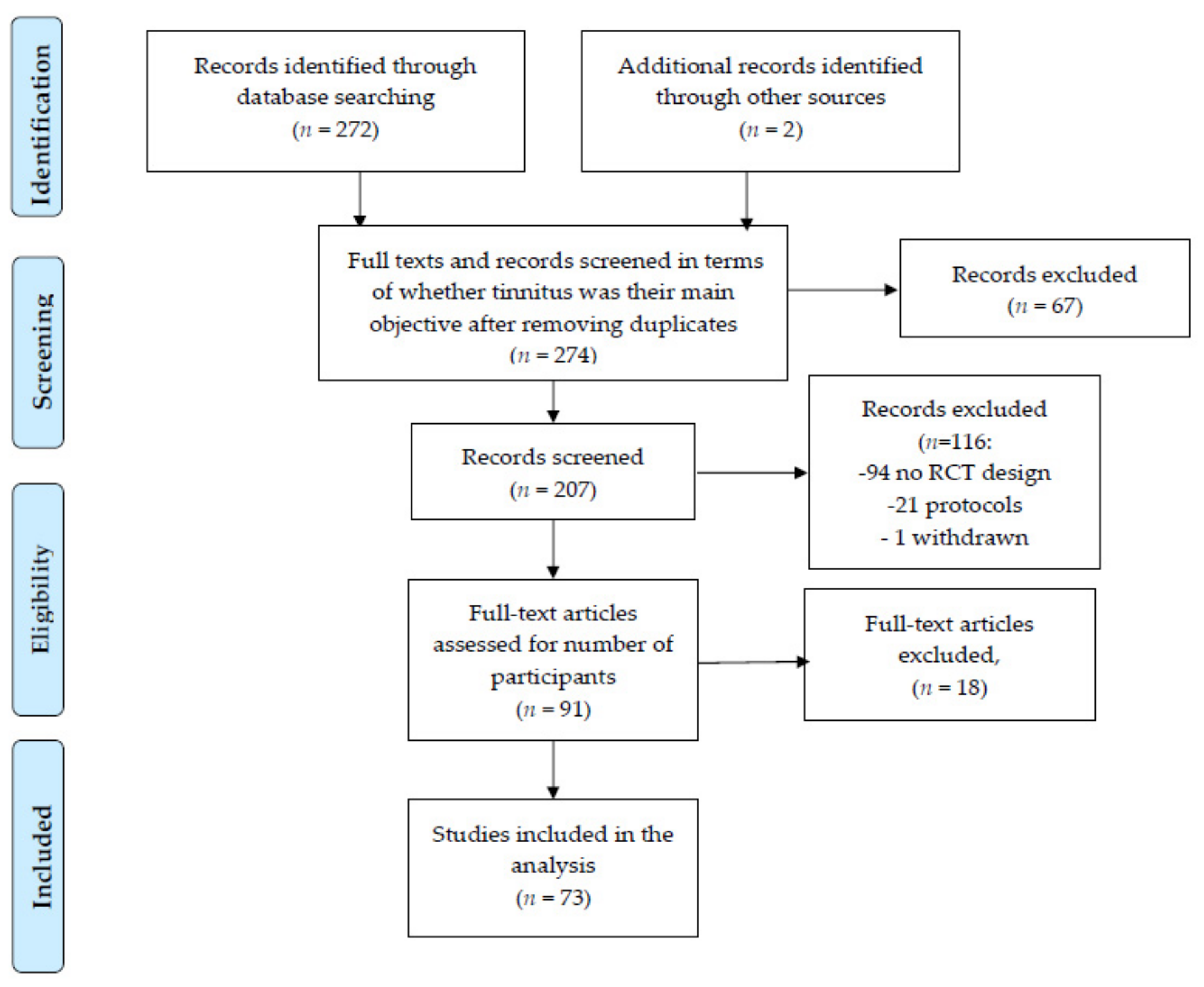
3.1. Study Selection
3.2. Study Characteristics
3.3. Results of Individuals Studies
3.3.1. Methods and Inclusion Criteria
3.3.2. Methods and Study Procedures
3.3.3. Methods and Outcome Measures
4. Discussion
4.1. Tinnitus Duration and Intermittent Character
4.2. Level of Perceived Annoyance
4.3. Tinnitus Audiological Characteristics
4.4. Tinnitus and Hearing Loss
4.5. Remarks on Study Methodology
4.6. Outcome Measures
4.7. Time Course
4.8. Trial Design and Results
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Cima, R.F.F.; Mazurek, B.; Haider, H.; Kikidis, D.; Lapira, A.; Noreña, A.; Hoare, D.J. A Multidisciplinary European Guideline for Tinnitus: Diagnostics, Assessment, and Treatment. HNO 2019, 67, 10–42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Ridder, D.; Schlee, W.; Vanneste, S.; Londero, A.; Weisz, N.; Kleinjung, T.; Shekhawat, G.S.; Elgoyhen, A.B.; Song, J.-J.; Andersson, G.; et al. Chapter 1—Tinnitus and tinnitus disorder: Theoretical and operational definitions (an international multidisciplinary proposal). In Progress in Brain Research; Schlee, W., Langguth, B., Kleinjung, T., Vanneste, S., De Ridder, D., Eds.; Tinnitus—An Interdisciplinary Approach Towards Individualized Treatment: From Heterogeneity to Personalized Medicine; Elsevier: Amsterdam, The Netherlands, 2021; Volume 260, pp. 1–25. [Google Scholar]
- Cima, R.F.F. Bothersome Tinnitus. HNO 2018, 66, 369–374. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bhatt, J.M.; Lin, H.W.; Bhattacharyya, N. Tinnitus Epidemiology: Prevalence, Severity, Exposures And Treatment Patterns In The United States. JAMA Otolaryngol. Head Neck Surg. 2016, 142, 959–965. [Google Scholar] [CrossRef]
- Hesse, G. Evidence and Evidence Gaps in Tinnitus Therapy. GMS Curr. Top. Otorhinolaryngol. Head Neck Surg. 2016, 15. [Google Scholar] [CrossRef]
- Hoare, D.J.; Kowalkowski, V.L.; Kang, S.; Hall, D.A. Systematic Review and Meta-Analyses of Randomized Controlled Trials Examining Tinnitus Management. Laryngoscope 2011, 121, 1555–1564. [Google Scholar] [CrossRef] [Green Version]
- Simoes, J.; Neff, P.; Schoisswohl, S.; Bulla, J.; Schecklmann, M.; Harrison, S.; Vesala, M.; Langguth, B.; Schlee, W. Toward Personalized Tinnitus Treatment: An Exploratory Study Based on Internet Crowdsensing. Front. Public Health 2019, 7. [Google Scholar] [CrossRef]
- Arienti, C.; Armijo-Olivo, S.; Minozzi, S.; Lazzarini, S.G.; Patrini, M.; Negrini, S. 60 Methodological Issues in Rehabilitation Research: A Scoping Review. BMJ EBM 2019, 24, A35. [Google Scholar] [CrossRef]
- Langguth, B.; Landgrebe, M.; Schlee, W.; Schecklmann, M.; Vielsmeier, V.; Steffens, T.; Staudinger, S.; Frick, H.; Frick, U. Different Patterns of Hearing Loss among Tinnitus Patients: A Latent Class Analysis of a Large Sample. Front. Neurol. 2017, 8. [Google Scholar] [CrossRef] [Green Version]
- Elgoyhen, A.B.; Langguth, B.; De Ridder, D.; Vanneste, S. Tinnitus: Perspectives from Human Neuroimaging. Nat. Rev. Neurosci. 2015, 16, 632–642. [Google Scholar] [CrossRef]
- Probst, T.; Pryss, R.C.; Langguth, B.; Rauschecker, J.P.; Schobel, J.; Reichert, M.; Spiliopoulou, M.; Schlee, W.; Zimmermann, J. Does Tinnitus Depend on Time-of-Day? An Ecological Momentary Assessment Study with the “TrackYourTinnitus” Application. Front. Aging Neurosci. 2017, 9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Winfried, S.; Stefan, S.; Susanne, S.; Axel, S.; Astrid, L.; Berthold, L.; Martin, S.; Jorge, S.; Patrick, N.; Steven, M.; et al. Towards a unification of treatments and interventions for tinnitus patients: The EU research and innovation action UNITI. In Progress in Brain Research; Elsevier: Amsterdam, The Netherlands, 2021. [Google Scholar]
- Shamseer, L.; Moher, D.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; The PRISMA-P Group. Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols (PRISMA-P) 2015: Elaboration and Explanation. BMJ 2015, 349, g7647. [Google Scholar] [CrossRef] [Green Version]
- Hopewell, S.; Clarke, M.; Lusher, A.; Lefebvre, C.; Westby, M. A Comparison of Handsearching versus MEDLINE Searching to Identify Reports of Randomized Controlled Trials. Stat. Med. 2002, 21, 1625–1634. [Google Scholar] [CrossRef]
- Buscemi, N.; Hartling, L.; Vandermeer, B.; Tjosvold, L.; Klassen, T.P. Single Data Extraction Generated More Errors than Double Data Extraction in Systematic Reviews. J. Clin. Epidemiol. 2006, 59, 697–703. [Google Scholar] [CrossRef] [PubMed]
- Anders, M.; Dvorakova, J.; Rathova, L.; Havrankova, P.; Pelcova, P.; Vaneckova, M.; Jech, R.; Holcat, M.; Seidl, Z.; Raboch, J. Efficacy of Repetitive Transcranial Magnetic Stimulation for the Treatment of Refractory Chronic Tinnitus: A Randomized, Placebo Controlled Study. Neuro Endocrinol. Lett. 2010, 31, 238–249. [Google Scholar]
- Biesinger, E.; Kipman, U.; Schätz, S.; Langguth, B. Qigong for the Treatment of Tinnitus: A Prospectiverandomized Controlled Study. J. Psychosom. Res. 2010, 69, 299–304. [Google Scholar] [CrossRef] [PubMed]
- Dehkordi, M.A.; Abolbashari, S.; Taheri, R.; Einolghozati, S. Efficacy of Gabapentin on Subjective Idiopathic Tinnitus: A Randomized, Double-Blind, Placebo-Controlled Trial. Ear Nose Throat J. 2011, 90, 150–158. [Google Scholar] [CrossRef] [Green Version]
- Sziklai, I.; Szilvássy, J.; Szilvássy, Z. Tinnitus Control by Dopamine Agonist Pramipexole in Presbycusis Patients: A Randomized, Placebo-Controlled, Double-Blind Study. Laryngoscope 2011, 121, 888–893. [Google Scholar] [CrossRef] [PubMed]
- Westin, V.Z.; Schulin, M.; Hesser, H.; Karlsson, M.; Noe, R.Z.; Olofsson, U.; Stalby, M.; Wisung, G.; Andersson, G. Acceptance and Commitment Therapy versus Tinnitus Retraining Therapy in the Treatment of Tinnitus: A Randomised Controlled Trial. Behav. Res. Ther. 2011, 49, 737–747. [Google Scholar] [CrossRef]
- Cima, R.F.F.; Maes, I.H.; Joore, M.A.; Scheyen, D.J.W.M.; El Refaie, A.; Baguley, D.M.; Anteunis, L.J.C.; van Breukelen, G.J.P.; Vlaeyen, J.W.S. Specialised Treatment Based on Cognitive Behaviour Therapy versus Usual Care for Tinnitus: A Randomised Controlled Trial. Lancet 2012, 379, 1951–1959. [Google Scholar] [CrossRef]
- Han, S.-S.; Nam, E.-C.; Won, J.Y.; Lee, K.U.; Chun, W.; Choi, H.K.; Levine, R.A. Clonazepam Quiets Tinnitus: A Randomised Crossover Study with Ginkgo Biloba. J. Neurol. Neurosurg. Psychiatry 2012, 83, 821–827. [Google Scholar] [CrossRef]
- Hesser, H.; Gustafsson, T.; Lundén, C.; Henrikson, O.; Fattahi, K.; Johnsson, E.; Zetterqvist Westin, V.; Carlbring, P.; Mäki-Torkko, E.; Kaldo, V.; et al. A Randomized Controlled Trial of Internet-Delivered Cognitive Behavior Therapy and Acceptance and Commitment Therapy in the Treatment of Tinnitus. J. Consult. Clin. Psychol. 2012, 80, 649–661. [Google Scholar] [CrossRef]
- Hoare, D.J.; Kowalkowski, V.L.; Hall, D.A. Effects of Frequency Discrimination Training on Tinnitus: Results from Two Randomised Controlled Trials. J. Assoc. Res. Otolaryngol. 2012, 13, 543–559. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jeon, S.W.; Kim, K.S.; Nam, H.J. Long-Term Effect of Acupuncture for Treatment of Tinnitus: A Randomized, Patient- and Assessor-Blind, Sham-Acupuncture-Controlled, Pilot Trial. J. Altern. Complement. Med. 2012, 18, 693–699. [Google Scholar] [CrossRef] [PubMed]
- Kreuzer, P.M.; Goetz, M.; Holl, M.; Schecklmann, M.; Landgrebe, M.; Staudinger, S.; Langguth, B. Mindfulness-and Body-Psychotherapy-Based Group Treatment of Chronic Tinnitus: A Randomized Controlled Pilot Study. BMC Complement. Altern. Med. 2012, 12, 235. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ngao, C.F.; Tan, T.S.; Narayanan, P.; Raman, R. The Effectiveness of Transmeatal Low-Power Laser Stimulation in Treating Tinnitus. Eur. Arch. Otorhinolaryngol. 2014, 271, 975–980. [Google Scholar] [CrossRef] [PubMed]
- Plewnia, C.; Vonthein, R.; Wasserka, B.; Arfeller, C.; Naumann, A.; Schraven, S.P.; Plontke, S.K. Treatment of Chronic Tinnitus with θ Burst Stimulation: A Randomized Controlled Trial. Neurology 2012, 78, 1628–1634. [Google Scholar] [CrossRef]
- Rocha, C.B.; Sanchez, T.G. Efficacy of Myofascial Trigger Point Deactivation for Tinnitus Control. Braz. J. Otorhinolaryngol. 2012, 78, 21–26. [Google Scholar] [CrossRef]
- Tass, P.A.; Adamchic, I.; Freund, H.-J.; von Stackelberg, T.; Hauptmann, C. Counteracting Tinnitus by Acoustic Coordinated Reset Neuromodulation. Restor. Neurol. Neurosci. 2012, 30, 137–159. [Google Scholar] [CrossRef] [Green Version]
- Choi, S.J.; Lee, J.B.; Lim, H.J.; In, S.M.; Kim, J.-Y.; Bae, K.H.; Choung, Y.-H. Intratympanic Dexamethasone Injection for Refractory Tinnitus: Prospective Placebo-Controlled Study. Laryngoscope 2013, 123, 2817–2822. [Google Scholar] [CrossRef]
- Coelho, C.; Witt, S.A.; Ji, H.; Hansen, M.R.; Gantz, B.; Tyler, R. Zinc to Treat Tinnitus in the Elderly: A Randomized Placebo Controlled Crossover Trial. Otol. Neurotol. 2013, 34, 1146–1154. [Google Scholar] [CrossRef]
- Hoekstra, C.E.L.; Versnel, H.; Neggers, S.F.W.; Niesten, M.E.F.; van Zanten, G.A. Bilateral Low-Frequency Repetitive Transcranial Magnetic Stimulation of the Auditory Cortex in Tinnitus Patients Is Not Effective: A Randomised Controlled Trial. Audiol. Neurootol. 2013, 18, 362–373. [Google Scholar] [CrossRef] [PubMed]
- Mollasadeghi, A.; Mirmohammadi, S.J.; Mehrparvar, A.H.; Davari, M.H.; Shokouh, P.; Mostaghaci, M.; Baradaranfar, M.H.; Bahaloo, M. Efficacy of Low-Level Laser Therapy in the Management of Tinnitus Due to Noise-Induced Hearing Loss: A Double-Blind Randomized Clinical Trial. Sci. World J. 2013, 2013. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nyenhuis, N.; Zastrutzki, S.; Weise, C.; Jäger, B.; Kröner-Herwig, B. The Efficacy of Minimal Contact Interventions for Acute Tinnitus: A Randomised Controlled Study. Cogn. Behav. Ther. 2013, 42, 127–138. [Google Scholar] [CrossRef] [PubMed]
- Sönmez, O.; Külahlı, I.; Vural, A.; Sahin, M.I.; Aydın, M. The Evaluation of Ozone and Betahistine in the Treatment of Tinnitus. Eur. Arch. Otorhinolaryngol. 2013, 270, 1999–2006. [Google Scholar] [CrossRef] [PubMed]
- Taslimi, S.; Vahidi, H.; Pourvaziri, A.; Modabbernia, A.; Fallah, A.Y.; Yazdani, N.; Taslimi, N.; Hosseini, M.; Zarandi, M.M. Ondansetron in Patients with Tinnitus: Randomized Double-Blind Placebo-Controlled Study. Eur. Arch. Otorhinolaryngol. 2013, 270, 1635–1641. [Google Scholar] [CrossRef] [PubMed]
- Dos Santos, G.M.; Bento, R.F.; de Medeiros, I.R.T.; Oiticcica, J.; da Silva, E.C.; Penteado, S. The Influence of Sound Generator Associated With Conventional Amplification for Tinnitus Control: Randomized Blind Clinical Trial. Trends Hear. 2014, 18, 233121651454265. [Google Scholar] [CrossRef] [Green Version]
- Hoare, D.J.; Van Labeke, N.; McCormack, A.; Sereda, M.; Smith, S.; Al Taher, H.; Kowalkowski, V.L.; Sharples, M.; Hall, D.A. Gameplay as a Source of Intrinsic Motivation in a Randomized Controlled Trial of Auditory Training for Tinnitus. PLoS ONE 2014, 9, e107430. [Google Scholar] [CrossRef] [Green Version]
- Jasper, K.; Weise, C.; Conrad, I.; Andersson, G.; Hiller, W.; Kleinstäuber, M. Internet-Based Guided Self-Help versus Group Cognitive Behavioral Therapy for Chronic Tinnitus: A Randomized Controlled Trial. Psychother. Psychosom. 2014, 83, 234–246. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shekhawat, G.S.; Searchfield, G.D.; Stinear, C.M. Randomized Trial of Transcranial Direct Current Stimulation and Hearing Aids for Tinnitus Management. Neurorehabilit. Neural Repair 2014, 28, 410–419. [Google Scholar] [CrossRef]
- Teismann, H.; Wollbrink, A.; Okamoto, H.; Schlaug, G.; Rudack, C.; Pantev, C. Combining Transcranial Direct Current Stimulation and Tailor-Made Notched Music Training to Decrease Tinnitus-Related Distress—A Pilot Study. PLoS ONE 2014, 9, e89904. [Google Scholar] [CrossRef] [Green Version]
- Dehkordi, M.A.; Einolghozati, S.; Ghasemi, S.M.; Abolbashari, S.; Meshkat, M.; Behzad, H. Effect of Low-Level Laser Therapy in the Treatment of Cochlear Tinnitus: A Double-Blind, Placebo-Controlled Study. Ear Nose Throat J. 2015, 94, 32–36. [Google Scholar] [PubMed]
- Bilici, S.; Yigit, O.; Taskin, U.; Gor, A.P.; Yilmaz, E.D. Medium-Term Results of Combined Treatment with Transcranial Magnetic Stimulation and Antidepressant Drug for Chronic Tinnitus. Eur. Arch. Otorhinolaryngol. 2015, 272, 337–343. [Google Scholar] [CrossRef] [PubMed]
- Folmer, R.L.; Theodoroff, S.M.; Casiana, L.; Shi, Y.; Griest, S.; Vachhani, J. Repetitive Transcranial Magnetic Stimulation Treatment for Chronic Tinnitus: A Randomized Clinical Trial. JAMA Otolaryngol. Head Neck Surg. 2015, 141, 716–722. [Google Scholar] [CrossRef] [Green Version]
- Kreuzer, P.M.; Lehner, A.; Schlee, W.; Vielsmeier, V.; Schecklmann, M.; Poeppl, T.B.; Landgrebe, M.; Rupprecht, R.; Langguth, B. Combined RTMS Treatment Targeting the Anterior Cingulate and the Temporal Cortex for the Treatment of Chronic Tinnitus. Sci. Rep. 2015, 5, 18028. [Google Scholar] [CrossRef] [Green Version]
- Malinvaud, D.; Londero, A.; Niarra, R.; Peignard, P.; Warusfel, O.; Viaud-Delmon, I.; Chatellier, G.; Bonfils, P. Auditory and Visual 3D Virtual Reality Therapy as a New Treatment for Chronic Subjective Tinnitus: Results of a Randomized Controlled Trial. Hear. Res. 2016, 333, 127–135. [Google Scholar] [CrossRef]
- Pal, N.; Maire, R.; Stephan, M.A.; Herrmann, F.R.; Benninger, D.H. Transcranial Direct Current Stimulation for the Treatment of Chronic Tinnitus: A Randomized Controlled Study. Brain Stimul. Basic Transl. Clin. Res. Neuromodulation 2015, 8, 1101–1107. [Google Scholar] [CrossRef]
- Thabit, M.N.; Fouad, N.; Shahat, B.; Youssif, M. Combined Central and Peripheral Stimulation for Treatment of Chronic Tinnitus: A Randomized Pilot Study. Neurorehabilit. Neural Repair 2015, 29, 224–233. [Google Scholar] [CrossRef] [PubMed]
- Albu, S.; Nagy, A.; Doros, C.; Marceanu, L.; Cozma, S.; Musat, G.; Trabalzini, F. Treatment of Meniere’s Disease with Intratympanic Dexamethazone plus High Dosage of Betahistine. Am. J. Otolaryngol. 2016, 37, 225–230. [Google Scholar] [CrossRef] [PubMed]
- Doi, M.Y.; Tano, S.S.; Schultz, A.R.; Borges, R.; de Moraes Marchiori, L.L. Effectiveness of Acupuncture Therapy as Treatment for Tinnitus: A Randomized Controlled Trial. Braz. J. Otorhinolaryngol. 2016, 82, 458–465. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Henry, J.A.; Stewart, B.J.; Griest, S.; Kaelin, C.; Zaugg, T.L.; Carlson, K. Multisite Randomized Controlled Trial to Compare Two Methods of Tinnitus Intervention to Two Control Conditions. Ear Hear. 2016, 37, e346–e359. [Google Scholar] [CrossRef]
- Laureano, M.R.; Onishi, E.T.; Bressan, R.A.; Neto, P.B.; Castiglioni, M.L.V.; Batista, I.R.; Reis, M.A.; Garcia, M.V.; de Andrade, A.N.; Sanchez, M.L.; et al. The Effectiveness of Acupuncture as a Treatment for Tinnitus: A Randomized Controlled Trial Using (99m)Tc-ECD SPECT. Eur. Radiol. 2016, 26, 3234–3242. [Google Scholar] [CrossRef] [PubMed]
- Lehner, A.; Schecklmann, M.; Greenlee, M.W.; Rupprecht, R.; Langguth, B. Triple-Site RTMS for the Treatment of Chronic Tinnitus: A Randomized Controlled Trial. Sci. Rep. 2016, 6, 22302. [Google Scholar] [CrossRef] [Green Version]
- Li, S.-A.; Bao, L.; Chrostowski, M. Investigating the Effects of a Personalized, Spectrally Altered Music-Based Sound Therapy on Treating Tinnitus: A Blinded, Randomized Controlled Trial. Audiol. Neurootol. 2016, 21, 296–304. [Google Scholar] [CrossRef]
- Lim, H.W.; Kim, T.S.; Kang, W.S.; Song, C.I.; Baek, S.; Chung, J.W. Effect of a 4-Week Treatment with Cilostazol in Patients with Chronic Tinnitus: A Randomized, Prospective, Placebo-Controlled, Double-Blind, Pilot Study. J. Int. Adv. Otol. 2016, 12, 170–176. [Google Scholar] [CrossRef] [PubMed]
- Rojas-Roncancio, E.; Tyler, R.; Jun, H.-J.; Wang, T.-C.; Ji, H.; Coelho, C.; Witt, S.; Hansen, M.R.; Gantz, B.J. Manganese and Lipoflavonoid Plus® to Treat Tinnitus: A Randomized Controlled Trial. J. Am. Acad. Audiol. 2016, 27, 661–668. [Google Scholar] [CrossRef] [PubMed]
- Roland, L.T.; Peelle, J.E.; Kallogjeri, D.; Nicklaus, J.; Piccirillo, J.F. The Effect of Noninvasive Brain Stimulation on Neural Connectivity in Tinnitus: A Randomized Trial. Laryngoscope 2016, 126, 1201–1206. [Google Scholar] [CrossRef] [Green Version]
- Singh, C.; Kawatra, R.; Gupta, J.; Awasthi, V.; Dungana, H. Therapeutic Role of Vitamin B12 in Patients of Chronic Tinnitus: A Pilot Study. Noise Health 2016, 18, 93–97. [Google Scholar] [CrossRef]
- Stein, A.; Wunderlich, R.; Lau, P.; Engell, A.; Wollbrink, A.; Shaykevich, A.; Kuhn, J.-T.; Holling, H.; Rudack, C.; Pantev, C. Clinical Trial on Tonal Tinnitus with Tailor-Made Notched Music Training. BMC Neurol. 2016, 16. [Google Scholar] [CrossRef] [Green Version]
- Weise, C.; Kleinstäuber, M.; Andersson, G. Internet-Delivered Cognitive-Behavior Therapy for Tinnitus: A Randomized Controlled Trial. Psychosom. Med. 2016, 78, 501–510. [Google Scholar] [CrossRef]
- Wise, K.; Kobayashi, K.; Magnusson, J.; Welch, D.; Searchfield, G.D. Randomized Controlled Trial of a Perceptual Training Game for Tinnitus Therapy. Games Health J. 2016, 5, 141–149. [Google Scholar] [CrossRef]
- Zarenoe, R.; Söderlund, L.L.; Andersson, G.; Ledin, T. Motivational Interviewing as an Adjunct to Hearing Rehabilitation for Patients with Tinnitus: A Randomized Controlled Pilot Trial. J. Am. Acad. Audiol. 2016, 27, 669–676. [Google Scholar] [CrossRef] [PubMed]
- Elzayat, S.; El-Sherif, H.; Hegazy, H.; Gabr, T.; El-Tahan, A.-R. Tinnitus: Evaluation of Intratympanic Injection of Combined Lidocaine and Corticosteroids. ORL J. Otorhinolaryngol. Relat. Spec. 2016, 78, 159–166. [Google Scholar] [CrossRef]
- Kallogjeri, D.; Piccirillo, J.F.; Spitznagel, E.; Hale, S.; Nicklaus, J.E.; Hardin, F.M.; Shimony, J.S.; Coalson, R.S.; Schlaggar, B.L. Cognitive Training for Adults With Bothersome Tinnitus. JAMA Otolaryngol. Head Neck Surg. 2017, 143, 443–451. [Google Scholar] [CrossRef] [PubMed]
- Kim, B.H.; Kim, K.; Nam, H.J. A Comparative Study on the Effects of Systemic Manual Acupuncture, Periauricular Electroacupuncture, and Digital Electroacupuncture to Treat Tinnitus: A Randomized, Paralleled, Open-Labeled Exploratory Trial. BMC Complement. Altern. Med. 2017, 17. [Google Scholar] [CrossRef] [Green Version]
- Landgrebe, M.; Hajak, G.; Wolf, S.; Padberg, F.; Klupp, P.; Fallgatter, A.J.; Polak, T.; Höppner, J.; Haker, R.; Cordes, J.; et al. 1-Hz RTMS in the Treatment of Tinnitus: A Sham-Controlled, Randomized Multicenter Trial. Brain Stimul. 2017, 10, 1112–1120. [Google Scholar] [CrossRef] [PubMed]
- McKenna, L.; Marks, E.M.; Hallsworth, C.A.; Schaette, R. Mindfulness-Based Cognitive Therapy as a Treatment for Chronic Tinnitus: A Randomized Controlled Trial. Psychother. Psychosom. 2017, 86, 351–361. [Google Scholar] [CrossRef] [Green Version]
- Arif, M.; Sadlier, M.; Rajenderkumar, D.; James, J.; Tahir, T. A Randomised Controlled Study of Mindfulness Meditation versus Relaxation Therapy in the Management of Tinnitus. J. Laryngol. Otol. 2017, 131, 501–507. [Google Scholar] [CrossRef] [PubMed]
- Beukes, E.W.; Baguley, D.M.; Allen, P.M.; Manchaiah, V.; Andersson, G. Guided Internet-Based versus Face-to-Face Clinical Care in the Management of Tinnitus: Study Protocol for a Multi-Centre Randomised Controlled Trial. Trials 2017, 18. [Google Scholar] [CrossRef] [Green Version]
- Sahlsten, H.; Virtanen, J.; Joutsa, J.; Niinivirta-Joutsa, K.; Löyttyniemi, E.; Johansson, R.; Paavola, J.; Taiminen, T.; Sjösten, N.; Salonen, J.; et al. Electric Field-Navigated Transcranial Magnetic Stimulation for Chronic Tinnitus: A Randomized, Placebo-Controlled Study. Int. J. Audiol. 2017, 56, 692–700. [Google Scholar] [CrossRef] [PubMed]
- Theodoroff, S.M.; Griest, S.E.; Folmer, R.L. Transcranial Magnetic Stimulation for Tinnitus: Using the Tinnitus Functional Index to Predict Benefit in a Randomized Controlled Trial. Trials 2017, 18. [Google Scholar] [CrossRef] [Green Version]
- Tyler, R.; Cacace, A.; Stocking, C.; Tarver, B.; Engineer, N.; Martin, J.; Deshpande, A.; Stecker, N.; Pereira, M.; Kilgard, M.; et al. Vagus Nerve Stimulation Paired with Tones for the Treatment of Tinnitus: A Prospective Randomized Double-Blind Controlled Pilot Study in Humans. Sci. Rep. 2017, 7. [Google Scholar] [CrossRef]
- Lee, H.-J.; Kim, M.-B.; Yoo, S.-Y.; Park, S.N.; Nam, E.-C.; Moon, I.S.; Lee, H.-K. Clinical Effect of Intratympanic Dexamethasone Injection in Acute Unilateral Tinnitus: A Prospective, Placebo-Controlled, Multicenter Study. Laryngoscope 2018, 128, 184–188. [Google Scholar] [CrossRef]
- Beukes, E.W.; Andersson, G.; Allen, P.M.; Manchaiah, V.; Baguley, D.M. Effectiveness of Guided Internet-Based Cognitive Behavioral Therapy vs Face-to-Face Clinical Care for Treatment of Tinnitus. JAMA Otolaryngol. Head Neck Surg. 2018, 144, 1126–1133. [Google Scholar] [CrossRef] [Green Version]
- Abtahi, H.; Okhovvat, A.; Heidari, S.; Gharagazarloo, A.; Mirdamadi, M.; Nilforoush, M.H.; Ghazavi, H. Effect of Transcranial Direct Current Stimulation on Short-Term and Long-Term Treatment of Chronic Tinnitus. Am. J. Otolaryngol. 2018, 39, 94–96. [Google Scholar] [CrossRef]
- El Beaino, M.; McCaskey, M.K.; Eter, E. Sulodexide Monotherapy in Chronic Idiopathic Subjective Tinnitus: A Randomized Controlled Trial. Otolaryngol. Head Neck Surg. 2018, 158, 1107–1112. [Google Scholar] [CrossRef] [PubMed]
- Hong, H.Y.; Karadaghy, O.; Kallogjeri, D.; Brown, F.T.; Yee, B.; Piccirillo, J.F.; Nagele, P. Effect of Nitrous Oxide as a Treatment for Subjective, Idiopathic, Nonpulsatile Bothersome Tinnitus: A Randomized Clinical Trial. JAMA Otolaryngol. Head Neck Surg. 2018, 144, 781–787. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Godbehere, J.; Sandhu, J.; Evans, A.; Twigg, V.; Scivill, I.; Ray, J.; Barker, A. Treatment of Tinnitus Using Theta Burst Based Repetitive Transcranial Magnetic Stimulation—A Single Blinded Randomized Control Trial. Otol. Neurotol. 2019, 40, S38. [Google Scholar] [CrossRef]
- Hall, D.A.; Ray, J.; Watson, J.; Sharman, A.; Hutchison, J.; Harris, P.; Daniel, M.; Millar, B.; Large, C.H. A Balanced Randomised Placebo Controlled Blinded Phase IIa Multi-Centre Study to Investigate the Efficacy and Safety of AUT00063 versus Placebo in Subjective Tinnitus: The QUIET-1 Trial. Hear. Res. 2019, 377, 153–166. [Google Scholar] [CrossRef]
- Li, J.; Jin, J.; Xi, S.; Zhu, Q.; Chen, Y.; Huang, M.; He, C. Clinical Efficacy of Cognitive Behavioral Therapy for Chronic Subjective Tinnitus. Am. J. Otolaryngol. 2019, 40, 253–256. [Google Scholar] [CrossRef] [PubMed]
- Noh, T.-S.; Kyong, J.-S.; Park, M.K.; Lee, J.H.; Oh, S.H.; Chung, C.K.; Kim, J.S.; Suh, M.-W. Treatment Outcome of Auditory and Frontal Dual-Site RTMS in Tinnitus Patients and Changes in Magnetoencephalographic Functional Connectivity after RTMS: Double-Blind Randomized Controlled Trial. Audiol. Neurootol. 2019, 24, 293–298. [Google Scholar] [CrossRef] [PubMed]
- Procházková, K.; Šejna, I.; Skutil, J.; Hahn, A. Ginkgo Biloba Extract EGb 761® versus Pentoxifylline in Chronic Tinnitus: A Randomized, Double-Blind Clinical Trial. Int. J. Clin. Pharm. 2018, 40, 1335–1341. [Google Scholar] [CrossRef] [Green Version]
- Radunz, C.L.; Okuyama, C.E.; Branco-Barreiro, F.C.A.; Pereira, R.M.S.; Diniz, S.N. Clinical Randomized Trial Study of Hearing Aids Effectiveness in Association with Ginkgo Biloba Extract (EGb 761) on Tinnitus Improvement. Braz. J. Otorhinolaryngol. 2019. [Google Scholar] [CrossRef]
- Sahlsten, H.; Holm, A.; Rauhala, E.; Takala, M.; Löyttyniemi, E.; Karukivi, M.; Nikkilä, J.; Ylitalo, K.; Paavola, J.; Johansson, R.; et al. Neuronavigated Versus Non-Navigated Repetitive Transcranial Magnetic Stimulation for Chronic Tinnitus: A Randomized Study. Trends Hear. 2019, 23, 2331216518822198. [Google Scholar] [CrossRef] [PubMed]
- Scherer, R.W.; Formby, C. Effect of Tinnitus Retraining Therapy vs Standard of Care on Tinnitus-Related Quality of Life. JAMA Otolaryngol. Head Neck Surg. 2019. [Google Scholar] [CrossRef]
- Yakunina, N.; Lee, W.H.; Ryu, Y.-J.; Nam, E.-C. Tinnitus Suppression Effect of Hearing Aids in Patients With High-Frequency Hearing Loss: A Randomized Double-Blind Controlled Trial. Otol. Neurotol. 2019, 40, 865–871. [Google Scholar] [CrossRef] [PubMed]
- Tutar, B.; Atar, S.; Berkiten, G.; Üstün, O.; Kumral, T.L.; Uyar, Y. The Effect of Transcutaneous Electrical Nerve Stimulation (TENS) on Chronic Subjective Tinnitus. Am. J. Otolaryngol. 2020, 41, 102326. [Google Scholar] [CrossRef]
- Chessum, L.; Matern, M.S.; Kelly, M.C.; Johnson, S.L.; Ogawa, Y.; Milon, B.; McMurray, M.; Driver, E.C.; Parker, A.; Song, Y.; et al. Helios Is a Key Transcriptional Regulator of Outer Hair Cell Maturation. Nature 2018, 563, 696–700. [Google Scholar] [CrossRef] [PubMed]
- Fettiplace, R. Hair Cell Transduction, Tuning, and Synaptic Transmission in the Mammalian Cochlea. In Comprehensive Physiology; Terjung, R., Ed.; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2017; pp. 1197–1227. ISBN 978-0-470-65071-4. [Google Scholar]
- Kreuzer, P.M.; Vielsmeier, V.; Poeppl, T.B.; Langguth, B. A Case Report on Red Ear Syndrome with Tinnitus Successfully Treated with Transcranial Random Noise Stimulation. Pain Physician 2017, 20, E199–E205. [Google Scholar] [CrossRef]
- Rauschecker, J.P.; May, E.S.; Maudoux, A.; Ploner, M. Frontostriatal Gating of Tinnitus and Chronic Pain. Trends Cogn. Sci. 2015, 19, 567–578. [Google Scholar] [CrossRef] [Green Version]
- Coelho, C.; Figueiredo, R.; Frank, E.; Burger, J.; Schecklmann, M.; Landgrebe, M.; Langguth, B.; Elgoyhen, A.B. Reduction of Tinnitus Severity by the Centrally Acting Muscle Relaxant Cyclobenzaprine: An Open-Label Pilot Study. Audiol. Neurootol. 2012, 17, 179–188. [Google Scholar] [CrossRef] [Green Version]
- Henry, J.A.; McMillan, G.; Dann, S.; Bennett, K.; Griest, S.; Theodoroff, S.; Silverman, S.P.; Whichard, S.; Saunders, G. Tinnitus Management: Randomized Controlled Trial Comparing Extended-Wear Hearing Aids, Conventional Hearing Aids, and Combination Instruments. J. Am. Acad. Audiol. 2017, 28, 546–561. [Google Scholar] [CrossRef] [PubMed]
- Hobson, J.; Chisholm, E.; El Refaie, A. Sound therapy (masking) in the management of tinnitus in adults. In Cochrane Database of Systematic Reviews; The Cochrane Collaboration, Ed.; John Wiley & Sons, Ltd.: Chichester, UK, 2010. [Google Scholar]
- Mahboubi, H.; Haidar, Y.M.; Kiumehr, S.; Ziai, K.; Djalilian, H.R. Customized Versus Noncustomized Sound Therapy for Treatment of Tinnitus: A Randomized Crossover Clinical Trial. Ann. Otol. Rhinol. Laryngol. 2017, 126, 681–687. [Google Scholar] [CrossRef]
- Schaette, R.; König, O.; Hornig, D.; Gross, M.; Kempter, R. Acoustic Stimulation Treatments against Tinnitus Could Be Most Effective When Tinnitus Pitch Is within the Stimulated Frequency Range. Hear. Res. 2010, 269, 95–101. [Google Scholar] [CrossRef]
- Folmer, R.L.; Carroll, J.R. Long-Term Effectiveness of Ear-Level Devices for Tinnitus. Otolaryngol. Head Neck Surg. 2006, 134, 132–137. [Google Scholar] [CrossRef]
- Langguth, B.; Goodey, R.; Azevedo, A.; Bjorne, A.; Cacace, A.; Crocetti, A.; Del Bo, L.; De Ridder, D.; Diges, I.; Elbert, T.; et al. Consensus for Tinnitus Patient Assessment and Treatment Outcome Measurement: Tinnitus Research Initiative Meeting, Regensburg, July 2006. Prog. Brain Res. 2007, 166, 525–536. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koops, E.A.; Husain, F.T.; van Dijk, P. Profiling Intermittent Tinnitus: A Retrospective Review. Int. J. Audiol. 2019, 58, 434–440. [Google Scholar] [CrossRef]
- Axelsson, A.; Ringdahl, A. Tinnitus—A Study of Its Prevalence and Characteristics. Br. J. Audiol. 1989, 23, 53–62. [Google Scholar] [CrossRef]
- Degeest, S.; Corthals, P.; Dhooge, I.; Keppler, H. The Impact of Tinnitus Characteristics and Associated Variables on Tinnitus-Related Handicap. J. Laryngol. Otol. 2016, 130, 25–31. [Google Scholar] [CrossRef] [PubMed]
- Hall, D.A.; Hibbert, A.; Smith, H.; Haider, H.F.; Londero, A.; Mazurek, B.; Fackrell, K. One Size Does Not Fit All: Developing Common Standards for Outcomes in Early-Phase Clinical Trials of Sound-, Psychology-, and Pharmacology-Based Interventions for Chronic Subjective Tinnitus in Adults. Trends Hear. 2019, 23. [Google Scholar] [CrossRef] [Green Version]
- Landgrebe, M.; Azevedo, A.; Baguley, D.; Bauer, C.; Cacace, A.; Coelho, C.; Dornhoffer, J.; Figueiredo, R.; Flor, H.; Hajak, G.; et al. Methodological Aspects of Clinical Trials in Tinnitus: A Proposal for an International Standard. J. Psychosom. Res. 2012, 73, 112–121. [Google Scholar] [CrossRef] [Green Version]
- Lan, L.; Li, J.; Chen, Y.; Chen, W.; Li, W.; Zhao, F.; Chen, G.; Liu, J.; Chen, Y.; Li, Y.; et al. Alterations of Brain Activity and Functional Connectivity in Transition from Acute to Chronic Tinnitus. Hum. Brain Mapp. 2020. [Google Scholar] [CrossRef] [PubMed]
- Schlee, W.; Hølleland, S.; Bulla, J.; Simoes, J.; Neff, P.; Schoisswohl, S.; Woelflick, S.; Schecklmann, M.; Schiller, A.; Staudinger, S.; et al. The Effect of Environmental Stressors on Tinnitus: A Prospective Longitudinal Study on the Impact of the COVID-19 Pandemic. J. Clin. Med. 2020, 9, 2756. [Google Scholar] [CrossRef] [PubMed]
- Vielsmeier, V.; Santiago Stiel, R.; Kwok, P.; Langguth, B.; Schecklmann, M. From Acute to Chronic Tinnitus: Pilot Data on Predictors and Progression. Front. Neurol. 2020, 11. [Google Scholar] [CrossRef]
- Phillips, J.S.; McFerran, D.J.; Hall, D.A.; Hoare, D.J. The Natural History of Subjective Tinnitus in Adults: A Systematic Review and Meta-Analysis of No-Intervention Periods in Controlled Trials. Laryngoscope 2018, 128, 217–227. [Google Scholar] [CrossRef] [Green Version]
- Castro, M. Placebo versus Best-Available-Therapy Control Group in Clinical Trials for Pharmacologic Therapies. Proc. Am. Thorac. Soc. 2007, 4, 570–573. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Author, Year | Primary Objective | N | Age (Years) | Tinnitus as Primary Complaint | Tinnitus Onset (Months) | Tinnitus Laterality Uni/Bilateral | Minimum Tinnitus Threshold | Hearing Loss | Use of Hearing Aids Considered |
|---|---|---|---|---|---|---|---|---|---|
| Anders, 2010 [16] | Evaluation of the efficacy of 1 Hz repetitive transcranial magnetic stimulation (rTMS) in the treatment of tinnitus. | 42 | 18–70 | No | >6 months | Both | No | Age-adjusted normal sensorineural hearing | No |
| Biesinger, 2010 [17] | Effect of a Qigong intervention on patients with tinnitus with somatosensoric components | 80 | Yes | >3 months | Not determined | No | Normal audiogram | No | |
| Dehkordi, 2011 [18] | Effect of gabapentin therapy on idiopathic tinnitus | 80 | 18–85 | No | >2 months | Unilateral | No | Not determined | No |
| Sziklai, 2011 [19] | Effect of pramipexole, a dopamine receptor agonist, influenced tinnitus associated with presbycusis | 40 | >50 | No | >1 year | Not determined | No | Bilateral SNHL | No |
| Westin, 2011 [20] | Comparison of acceptance and commitment therapy (ACT) with tinnitus retraining therapy (TRT) on tinnitus | 64 | ≥18 | Yes | ≥6 months | Not determined | THI ≥ 30 | Hearing thresholds which would allow for the use of wearable sound generators | No |
| Cima, 2012 [21] | Effect of cognitive behavioral therapy (CBT) versus usual care | 492 | >18 | No | Not determined | No | Not determined | No | |
| Han, 2012 [22] | Comparison between Clonazepam and gingko biloba | 38 | No | 2 months | Not determined | No | Not determined | No | |
| Hesser, 2012 [23] | Effects on global tinnitus severity of 2 Internet-delivered psychological treatments, acceptance, and commitment therapy (ACT) and CBT, in guided self-help format | 99 | >18 | No | >6 months | Not determined | THI ≥ 38 | Not determined | No |
| Hoare, 2012 [24] | Comparison between different methods of frequency discrimination training on tinnitus percept | 70 | No | 6 months | Not determined | No | <40 dB in at least one frequency | No | |
| Jeon, 2012 [25] | Effect of acupuncture versus sham | 33 | 18–60 | No | 6 months | Unilateral | No | Mean of 0.5, 1, and 2 kHz Audiogram > 50 dB | No |
| Kreuzer, 2012 [26] | Efficacy of a specific mindfulness- and body-psychotherapy based program in patients suffering from chronic tinnitus | 36 | 18–80 | No | >6 months | Not determined | No | Not determined | No |
| Ngao, 2012 [27] | Effect of transmeatal low-power laser stimulation (TLLS) | 43 | Yes | Not determined | No | Not determined | No | ||
| Plewnia, 2012 [28] | Safety and efficacy of bilateral CTBS to the temporal and temporoparietal cortex in the treatment of chronic tinnitus. | 48 | No | <5 years | Not determined | No | Not determined | No | |
| Rocha, 2012 [29] | Efficacy of myofascial trigger point (MTP) deactivation for tinnitus relief in patients with myofascial pain syndrome | 71 | No | >3 months | Not determined | No | Not determined | No | |
| Tass, 2012 [30] | Comparison between CR (4 different groups) vs. placebo | 63 | >18 | No | 6 months | Not determined | No | <50 dB in all frequencies | No |
| Choi, 2013 [31] | Comparison between intratympanic steroids and placebo | 30 | No | Not determined | No | Not determined | No | ||
| Coelho, 2013 [32] | Effect of zinc versus placebo | 115 | >60 | No | 6 months | Not determined | No | Not determined | No |
| Hoekstra, 2013 [33] | Effect of repetitive transcranial magnetic stimulation(rTMS) on tinnitus | 50 | No | >2 months | Not determined | No | Not determined | No | |
| Mollasadeghi, 2013 [34] | Effect of low laser beam in tinnitus | 89 | ≤50 | No | Not determined | No | >15 dB at least at one of 3, 4, and 6 kHz | No | |
| Nyenhuis, 2013 [35] | The efficacy of CBT-oriented interventions for acute tinnitus on a broader data basis. | 185 | 18–75 | No | 2–26 weeks | Not determined | No | Not determined | No |
| Sönmez, 2013 [36] | Comparison between ozone and betahistine | 68 | 18–75 | No | 6 months | Not determined | No | No | No |
| Taslimi, 2013 [37] | Effect of ondansedron | 53 | 18–70 | No | 3 months | Not determined | No | Not determined | No |
| Dos Santos, 2014 [38] | Evaluation of combined use of amplification and sound generator and their combination | 49 | No | At least 6 months | Not determined | THI > 20 | Mild to moderate symmetrical sensorineural hl | No | |
| Hoare, 2014 [39] | Frequency discrimination training (FDT) delivered in a gaming format have significant therapeutic benefit in tinnitus | 60 | No | Not determined | No | ≥20 dB in at least one frequency, ≤40 dB average | No | ||
| Jasper, 2014 [40] | Effects of conventional face-to-face group cognitive behavioral therapy (GCBT) and an Internet-delivered guided self-help treatment iCBT on tinnitus distress | 128 | ≥18 | Yes | ≥6 months | Not determined | THI ≥ 18 or mini-TQ ≥ 8 | Not determined | No |
| Shekhawat, 2014 [41] | Comparison of multisession anodal transcranial direct current stimulation (TDCS) of the left temporoparietal area would enhance sound therapy from hearing aids. | 40 | No | >2 years | Not determined | TFI > 25 | Aidable HL | No | |
| Teismann, 2014 [42] | Combine (TMNMT) with transcranial direct current stimulation (TDCS) in an effort to modulate TMNMT efficacy in the treatment of tinnitus | 34 | No | ≥3 months | Both | No | Not determined | No | |
| Dehkordi, 2015 [43] | Effect of low-dose laser therapy on chronic cochlear tinnitus | 66 | No | Not determined | No | Not mentioned | No | ||
| Bilici, 2015 [44] | 5 groups: 3 types of rTMS, paroxetine, placebo | 75 | No | 1 year | Not determined | No | Normal hearing | No | |
| Folmer, 2015 [45] | Effect of repeated transcranial magnetic stimulation | 61 | No | Not determined | No | Not determined | No | ||
| Kreuzer, 2015 [46] | Comparison of medial frontal stimulation with double cone coil and conventional prefrontal left dorsolateral prefrontal cortex (DLPFC)-stimulation (study arm 2/control group) both followed by stimulation of the left temporo-parietal junction area | 40 | No | >6 months | Not determined | No | Not determined | No | |
| Malinvaud, 2015 [47] | Comparison between CBT and virtual reality interactive intervention | 148 | 18–70 | No | 12 months | Unilateral | No | Normal to mild | No |
| Pal, 2015 [48] | Investigation of the efficacy and safety of repeated sessions of a novel transcranial direct current stimulation (TDCS) protocol by combining bilateral cathodal TDCS to the auditory cortex (AC) with anodal stimulation of the prefrontal cortex (PFC). | 42 | No | ≥1 year | Not determined | No | Age-adjusted normal hearing according to the presbycusis scale | No | |
| Thabit, 2015 [49] | Effect of different types of rTMS and their combination | 30 | >18 | No | 6 months | Both | No | Not determined | No |
| Albu, 2016 [50] | Effectiveness of intratympanic (IT) steroids and melatonine versus melatonine only in acute tinnitus | 60 | No | Acute (within 3 months) | Unilateral | No | Not mentioned | No | |
| Doi, 2016 [51] | Effectiveness of acupuncture therapy for tinnitus | 50 | No | Not determined | Not determined | THI: moderate to severe | Not determined | No | |
| Henry, 2016 [52] | Effect on tinnitus severity by using tm-TRT-ted | 148 | No | Not determined | No | Not determined | No | ||
| Laureano, 2016 [53] | Effect of acupuncture on brain perfusion using (99m) ethyl cysteinate dimer single-photon emission computed tomography ((99m) Tc-ECD SPECT) in patients with tinnitus | 57 | 18–60 | No | >3 months | Both | No | Up to 25 dB | No |
| Lehner, 2016 [54] | Comparison between two types of rTMS | 49 | 18–70 | No | 6 months | Not determined | THI > 38 | Not determined | No |
| Li, 2016 [55] | Compare the effects of personalized, altered music to unaltered music on subjective tinnitus | 34 | ≥18 | No | ≥12 months | Both | THI > 26 | Hearing loss ≤70 dB | No |
| Lim, 2016 [56] | Efficacy of cilostazol, a selective phosphodiesterase 3 inhibitor, in patients with chronic tinnitus | 50 | >19 | No | 3–12 months | Both | Vas ≥ 4 | Not determined | No |
| Rojas-roncancio, 2016 [57] | Effect of manganese and lipoflavonoid plus on tinnitus | 40 | No | >6 months | Not determined | Tinnitus loudness and annoyance > 50% | Not determined | No | |
| Roland, 2016 [58] | Evaluation of the neural network changes in patients with bothersome chronic tinnitus who underwent rTMS treatment targeting the left temporoparietal junction (TPJ), as compared to those who received sham therapy. | 30 | 18–60 | No | ≥6 months | Not determined | THI > 30 | Not determined | No |
| Singh, 2016 [59] | Effect of B12 versus placebo | 40 | 18–60 | No | 6 months | Not determined | No | Not determined | No |
| Stein, 2016 [60] | The effect of a sound therapy (tailor-made notched music training, TMNMT) against tinnitus | 100 | 18–70 | No | ≥3 months | Both | No | Hl ≤70 dB hl in the frequency ranges of one-half octave above and below the tinnitus frequency | No |
| Weise, 2016 [61] | Effect of iCBT | 61 | >18 | Yes | >6 months | Not determined | THI > 38 or mini-TQ > 13 | Not determined | No |
| Wise, 2016 [62] | Effects of an auditory attention training game with those of a control game across tinnitus, attention, and electrophysiological measures | 31 | 18–70 | No | >6 months | Not determined | Tinnitus problem rating scale > mild | <80 Db HL nonconductive HL | No |
| Zarenoe, 2016 [63] | Effects of motivational interview (MI) as an adjunct to regular HA fitting for patients with tinnitus and hearing loss. | 46 | No | Not determined | No | Not determined | No | ||
| Elzayat, 2016 [64] | To evaluate the effectiveness of adding lidocaine to intratympanic steroid in the patients with idiopathic subjective tinnitus (IST). | 44 | No | Not determined | No | Not determined | No | ||
| Kallogjeri, 2017 [65] | To evaluate the effect of the brain fitting program-tinnitus on tinnitus. | 60 | 20–65 | No | >6 months | Not determined | According to bothersome scale | Not determined | No |
| Kim, 2017 [66] | Effect of different approaches of acupuncture | 39 | 20–75 | No | 2 weeks | Not determined | No | Not determined | No |
| Landgrebe, 2017 [67] | Evaluation of the efficacy of a two-week 1-Hz-RTMS in patients with chronic tinnitus. | 146 | 18–70 | No | >6 months | Not determined | THI > 38 | Normal, age-adjusted hearing levels. Conductive hearing loss ≤ 15 db. | No |
| Mckenna, 2017 [68] | Effect of mindfulness based cognitive therapy (MBCT) in tinnitus severity, psychological distress, functional disability, avoidance, and negative cognitions and a greater increase in tinnitus acceptance. | 75 | ≥18 | No | >6 months | Not determined | No | Hearing levels allowing participation in group discussions | No |
| Arif, 2017 [69] | Relaxation therapy and mindfulness | 61 | >18 | Yes | Not determined | No | Not determined | No | |
| Beukes, 2017 [70] | Efficacy of guided internet based cognitive behavioral treatment (iCBT) | 146 | >18 | No | >3 months | Both | TFI > 25 | Not determined | No |
| Sahlsten, 2017 [71] | E-field navigation should versus non-navigated rTMS | 39 | 18–65 | No | 6 months–10 years | Both | No | Not determined | No |
| Theodoroff, 2017 [72] | To determine if an acoustic stimulus mimicking the tinnitus perception delivered during sleep from the Otoharmonics corporation’s LEVO system reduces tinnitus-related distress and/or perceived loudness of tinnitus during awake hours for people who experience bothersome tinnitus | 58 | 30–72 | No | >6 months | Not determined | TFI > 25 | <70 dB hl, in all frequencies between 0.25 and 8 kHz | No |
| Tyler, 2017 [73] | Effect of vagus nerve stimulation (VNS) paired with sounds in chronic tinnitus patients | 30 | 22–65 | No | >1 year | Both | No | Not determined | No |
| Lee, 2018 [74] | Effect of intratympanic steroids on acute tinnitus | 54 | No | Acute (one month) | Unilateral | No | Not determined | No | |
| Beukes, 2018 [75] | Evaluation of an Internet-based cognitive behavioral therapy intervention versus face to face | 92 | >18 | No | Not determined | Not determined | No | Not determined | Yes |
| Abtahi, 2018 [76] | Effectiveness of anodal and cathodal methods in reducing the intensity of tinnitus | 51 | 18–80 | No | >1 year | Not determined | No | Not determined | No |
| El Beaino, 2018 [77] | Effect of sulodexide (heparin and dermatan) vs. placebo | 124 | >18 | No | 12 months | Not determined | No | Not determined | No |
| Hong, 2018 [78] | Effect of nitrous oxide on tinnitus | 18–65 | No | >6 months | Not determined | According to bothersome scale | Not determined | No | |
| Godbehere, 2019 [79] | Theta burst TMS are an effective treatment for chronic tinnitus | 40 | >18 | No | Not determined | Both | No | No HL, mild and moderate HL | No |
| Hall, 2019 [80] | Effect of AUTt00063, a novel centrally acting drug) potent and selective modulator of kv3.1 and kv3.2 voltage-gated potassium channels) vs. placebo | 76 | >18 | Yes | >6, <18 months | Both | TFI > 24 and <68 | <60 db in 0.5,1,2,4 kHz | No |
| Li, 2019 [81] | Clinical efficacy of cognitive behavioral therapy (CBT) for treatment of chronic subjective tinnitus | 100 | No | >3 months | Not determined | No | Not determined | No | |
| Noh, 2019 [82] | To investigate the effects of active dual-site rTMS treatment on reducing tinnitus using a double-blind randomized controlled trial. | 30 | No | Not determined | No | Not determined | No | ||
| Prozchazkova, 2019 [83] | Comparison between gingko biloba and pentoxifylline | 197 | >30 | No | 3 months | Not determined | Mini TQ > 5 | Not determined | No |
| Radunz, 2019 [84] | Comparison between ginkgo biloba, HA, and their combination | 35 | >18 | No | 3 months | Both | No | All types of hearing loss | No |
| Sahlsten, 2019 [85] | Comparison of neuronavigated versus non-navigated repetitive transcranial magnetic stimulation | 40 | 18–65 | No | 6 months–10 years | Both | Numeric scale > 4 | Not determined | No |
| Scherer, 2019 [86] | To compare the efficacy of tinnitus retraining therapy (TRT) and its components, ST, and TC, with the standard of care (SOC) in reducing the negative effect of tinnitus on quality of life. | 98 | No | >1 year | Not determined | TQ > 40 | Functionally adequate hearing sensitivity without requirement of amplification | No | |
| Yakunina, 2019 [87] | Evaluation of the effects on tinnitus of hearing aids (HA) alone without accompanying counseling or any other therapy additionally, whether FL techniques (LFT and FT) performed compared with conventional WDRC in the same open-fit HA in terms of tinnitus suppression for patients with high frequency hearing loss (HFHL). | 94 | >18 | No | ≥3 months | Not determined | THI > 18 Vas ≥ 50% | SNHL | No |
| Tutar, 2020 [88] | Efficacy of transcutaneous electric stimulation applied to the auricula | 60 | 18–65 | No | >3 months | Not determined | No | Not determined | No |
| Author, Year | Treatment | Control Group Intervention | Randomization | Outcome Measures | Monitoring Duration | Power Analysis | Results | Is Treatment Effective? |
|---|---|---|---|---|---|---|---|---|
| Abtahi, 2018 [76] | Anodal Stimulation, Cathodal Stimulation | Sham Stimulation | Unclear | Tinnitus Intensity Variations on A Scale Between −4 and +4. In This Scale, −4 Indicated Worsening Conditions, +4 Meant Full Recovery, And Zero Conveyed No Change in The Tinnitus Intensity. | 2 Months | No | Anodal Stimulation Was More Effective Than the Cathodal and Control Stimulation in Reducing the Intensity of Tinnitus in The Short Term | Yes, Between Two Versions of The Same Treatment |
| Albu, 2016 [50] | Intratympanic (IT) Steroid and Melatonin | Melatonin | Unclear | THI, PSQI, BDI | 3 Months | No | Better Response in The Combined Group of Melatonine And IT In Acute Tinnitus Patients | Yes |
| Anders, 2010 [16] | Active or Sham repetitive transcranial magnetic stimulation (rTMS) | Sham Rtms | Unclear | VAS, THI | 26 Weeks | No | 1 Hz Rtms Treatment Was Capable of Significantly Reducing the Total Baseline Score of Basic Scales That Measure Tinnitus Severity | No |
| Arif, 2017 [69] | Relaxation Therapy or Mindfulness Meditation Treatment Over A Period Of 15 Weeks | Relaxation Procedure | Clear | Primary: TRQ Secondary VAS and A Health State Thermometer. | 15 Weeks | No | Changes in Tinnitus Loudness and THI (but not TRQ) with the Customized Sound Therapy Were Statistically Greater Than Those of The Broadband Noise Therapy | No |
| Beukes, 2017 [70] | Internet-based cognitive behavioral treatment (iCBT) Intervention | ICBT After 8 Weeks | Algorithm Implemented by Independent Researcher | Primary: TFI, Secondary: ISI, GAD-7, PHQ-9, HHIA-S, HQ, CFQ, SWLS | 2 Months | 80% | Guided ICBT For Tinnitus Using Audiological Support Resulted in Statistically Significant Reductions in Tinnitus Distress and Comorbidities (Insomnia, Depression, Hyperacusis, Cognitive Failures) And Improved Quality of Life. | Yes |
| Beukes, 2018 [75] | Internet- Based Intervention | Face-To-Face Tinnitus Care | Unclear | THI, TFI | 2 Months | 90% | ICBT And F2F Interventions Are not Effective for Reducing Tinnitus Distress and Most Tinnitus-Related Difficulties. | No |
| Biesinger, 2010 [17] | 10 Qigong Training Sessions | No Treatment | Unclear | VAS, TBF-12 | 3 Months | No | No Statistically Significant Changes in Both Groups | No |
| Bilici, 2013 [44] | rTMS | Paroxetine, Placebo | Unclear | THI, TSI, BAS, PSS | 6 Months | No | No Significant Improvement Neither for Rtms Groups nor For Controls | No |
| Choi, 2013 [31] | IT Steroids | Placebo | Clear | THI. VAS | 1 Month | No | No Significant Difference Between IT Steroids and Placebo | No |
| Cima, 2012 [21] | CBT | Usual Care | Clear | HUI, HADS, TFQ | 12 Months | No | Superiority Of CBT | Yes |
| Coelho, 2013 [32] | Zinc | Placebo | Unclear | THQ | 4 Months | 90% | No Significant Differences Between Zinc and Placebo | No |
| Dehkordi, 2011 [18] | Gabapentin | Placebo | Unclear | TSI | 26 Months | No | No Statistically Significant Difference Between the Two Groups In TSI. | No |
| Dehkordi, 2015 [43] | Active Laser Treatment | Inactive Dummy Treatment | Unclear | TSI | 4 Weeks | No | No Statistically Significant Improvement Neither in Laser nor In Control Group | No |
| Doi, 2016 [51] | Acupuncture | No Treatment | Randomization Was Carried Out with The Aid of Computerized Table of Random Numbers Created by A Microsoft Excel Spreadsheet. | VAS, THI | 5 Weeks | No | Treatment with Acupuncture Improves the Perception of Tinnitus, Decreases the Intensity Level, Hence There Is No Comparison Between Levels of Improvement | Yes, Against Placebo In 5 Weeks, However No Comparison of Decrease |
| Dos Santos, 2014 [38] | Hearing Aids + Sound Generator | Hearing Aids | Unclear | THI | 3 Months | 80,0% | No Superiority of The Combined Use of Amplification and Sound Generator Over Conventional Amplification Alone in Reducing the Discomfort of Tinnitus. Both Groups Presented Similar Responses in Both Reduction of Discomfort Caused by Tinnitus | No |
| El Beaino, 2018 [77] | Sulodexide | Placebo | Unclear | THI, Mini TQ | Right After Treatment | 80% | Improvement in THI and Mini TQ Right After the End of Treatment with Sulodexide | Yes |
| Elzayat, 2018 [64] | Group A Was Injected with Combined Lidocaine 2% And Dexamethasone 8 Mg/2 mL (ITLD). Group B Was Injected Only by Dexamethasone 8 Mg/2 ML. (ITD). | ITD As A Controlled Group | Clear | THI, VAS, ATQ | 6 Months | No | Both Treatments Were Effective but No Difference Between Groups Was Found | Yes |
| Folmer, 2015 [45] | rTMS Daily For 2 Weeks | Sham Rtms With A Same Looking Coil | Unclear | TFI | 26 Months | No | Significant Improvement in Active Compared to Placebo Group | Yes |
| Godbehere, 2019 [79] | Theta Burst TMS | Placebo Arm | Unclear | TFI | 4 Weeks | No | No Significant Difference in Scores Between the Active Treatment Group and The Sham Control Group | No |
| Hall, 2019 [80] | AUT00063 | Placebo | Clear | TFI, VAS | 28 Days | 90% | No Significant Improvement for Both Groups (Channel Blocker and Placebo) | No |
| Han, 2012 [22] | Clonazepam | Ginkgo Biloba | Unclear | THI, VAS, Loudness Scale | No | Improvement with Use of Clonazepam and Not Gingko Biloba, but Right After Treatment | Yes | |
| Henry, 2016 [52] | TM-TRT-TED | No Treatment | Clear | THI | 18 Months | 80% | No Statistically Significant Improvement In THI. By 6 Months, The TED Group Showed Significant Improvement from Baseline and Its Improvement Was Not Significantly Different from That Shown in TM Or TRT. | No |
| Hesser, 2012 [23] | CBT Or ACT | Monitored Internet Discussion Forum | Clear | Primary: THI, Secondary: HADS | 1 Year | 80% | The Effect of ACT Compared with The Control Condition at Posttreatment on The Primary Outcome Was in The Moderate Range and Comparable to The Effect Observed Following CBT (D = 0.68 vs. D = 0.70). | No |
| Hoare, 2012 [24] | Frequency Training | Different Frequency Training | THQ | 4 Weeks | 80% | Statistically and Clinically Meaningful Improvement in All Groups. No Difference Between Groups | Yes | |
| Hoare, 2014 [39] | To Play A Tailored Video Game For 30 Minutes, 5 Days A Week For 4 Weeks | Another Type Of FDT | Clear | THQ | 4 Weeks | 80% | Statistically but Not Clinically Significant Changes in One of The Games Used | No |
| Hoekstra, 2013 [33] | rTMS in 1000Hz | Placebo | Unclear | Primary: TQ. Secondary THI, VAS | 6 Months | 80% | No Significant Difference Between Groups | No |
| Hong, 2018 [78] | 40 Minutes Session of Nitrous Oxide Under General Anesthesia | Same Procedure Without Nitrous Oxide | Clear | TFI | 2 Weeks | 81% | No Significant Differences Between Intervention and Control Group. Neither Groups Had Clinical or Statistically Significant Improvement | No |
| Jasper, 2014 [40] | GCBT, iCBT | Web-Based Discussion Forum (DF) | Unclear | THI, Mini-TQ, Secondary: HADS, ISI, TAQ | 6 Months | No | ICBT And Conventional GCBT Do Not Have Significant Differences Effects on Tinnitus Distress and Associated Problems. | No |
| Jeon, 2012 [25] | Acupuncture | Sham | Unclear | THI, VAS | No | No Significant Differences Between Acupuncture and Sham | No | |
| Kallogjeri, 2017 [65] | Brain fitness program tinnitus (BFP-T) | No Treatment | Unclear | THI, TFI, Global Bother Score | 8 Weeks | 85% | No Statistically Significant Changes Between Study Groups. | No |
| Kim, 2017 [66] | Manual Acupuncture | Electroacupuncture | Unclear | THI, VAS | 80% | No Significant Improvement for Any Acupuncture Group In Regards To THI and Loudness | No | |
| Kreuzer, 2012 [26] | Mindfulness and Body Group Therapy | Waiting List (Therapy After 24 Weeks) | Unclear | TQ | 24 Weeks | No | A Significant Reduction in The TQ Score (Baseline vs. Week 9) Compared to The Waiting List Control Group, However Difference Was Not Stable in Long Term F/U | No |
| Kreuzer, 2015 [46] | Medial Frontal Stimulation with Double Cone Coil + Stimulation of The Left Temporo-Parietal Junction Area | Conventional Prefrontal Left DLPFC-Stimulation + Stimulation of The Left Temporo-Parietal Junction Area | Unclear | TQ, Secondary: THI, CGI-CHANGE, Whoqol-Bref-Questionnaire | 12 Weeks | No | ΤICDC-Stimulation Non-Superior to Standard Rtms Regarding Both Primary and Secondary Outcome Measures. | No |
| Landgrebe, 2017 [67] | 2 Week Treatment Real 1-Hz-Rtms vs. Sham Rtms | Sham Rtms | Clear | Primary: The Change of Tinnitus Severity Assessed by Means of The Change of The TQ Sum Score Between Baseline Score vs. Day 12. Secondary: Changes of The TQ Sum Score, The THI and TSS During the Treatment and The Follow-Up Period. Further: Changes of Overall Illness Severity, Changes in Depressive Symptoms, Changes in Quality of Life and Changes in Psychoacoustic Measures of Tinnitus. | 26 Weeks | No | Real 1-Hz-Rtms Applied to The Left Temporal Cortex Did Not Provide Any Therapeutic Benefit as Compared to Sham Treatment in Patients with Chronic Tinnitus. | No |
| Laureano, 2016 [53] | True Acupuncture 99mTC-ECD SPECT | Sham Acupuncture | Unclear | Primary: SPECT Measurements, Secondary: THI, VAS, HAS, BDI | 12 Weeks | 80% | No Significant Differences After Treatment Were Observed with Regard to the VAS, HAS or BDI Between the Treatment Groups. | No |
| Lee, 2018 [74] | IT Steroids | Placebo (Saline) | Clear | THI, VAS | 1 Month | 80% | No Difference Between IT And Placebo Groups | No |
| Lehner, 2016 [54] | High Frequency rTMS | Single Site Rtms | Clear | TQ, THI, | 6 Months | 80% | No Difference Between Groups | No |
| Li, 2016 [55] | Music Altered by The Software to Treat Tinnitus | Unaltered Music | Unclear | THI, TFI, HADS | 12 Months | 80% | Statistically Significant and Clinically Meaningful Effects of The Therapy as Indicated by The Consistent Treatment-Control Group Difference in THI Score and The Significant Reduction in THI Score Within the Treatment Group During The 12-Month Period. | Yes |
| Li, 2019 [81] | Masking Therapy+ Sound Treatment + CBT | Masking Therapy + Sound Treatment (Tinni Test) | Unclear | THI, SCL-90 | 6 Months | No | Effective Rate in Intervention Group Was Significantly Higher Than That in Control Group (P < 0.01) | Yes |
| Lim, 2016 [56] | Oral 100 mg Cilostazol | Placebo | Unclear | VAS, THI, SF-36 | 4 Weeks | No | THI Failed to Show A Significant Drug Effect of Cilostazol | No |
| Malinvaud, 2015 [47] | Virtual reality (VR) | CBT | Clear | STSS, THI, THQ, VAS | No | Both VR And BT Groups Improved | Yes | |
| Mckenna, 2017 [68] | RT Or MBCT Treatment vs. Waiting Period Without Treatment | RT Treatment Group | Clear | Primary: TQ, CORE-NR, Secondary: CORE-OM, VAS, TFI, HADS, TCS, T-FAS, TAQ, MAAS, WSAS | 6 Months | 80.0% | MBCT Is More Effective in Reducing Tinnitus Severity Than Both A Waiting Period and An Active Treatment of Equal Intensity (RT) | Yes |
| Mollasadeh, 2013 [34] | Low Laser Beam | Placebo | Unclear | THI, VAS, Loudness Scale | 3 Months | No | Larger Improvement in Low Beam Laser Compared to Placebo, Hence More Than 50% Of Intervention Group Without Improvement | Yes |
| Ngao, 2012 [27] | TLLS | Sham | Unclear | THI, VAS | Right After Intervention | No | No Significant Difference Between TLLS And Sham | No |
| Noh, 2019 [82] | Dual-Site Rtms Or Sham Rtms | Sham Rtms | Unclear | Primary: THI, Secondary: VAS | 8 Weeks | No | A Beneficial Effect of Rtms On Tinnitus Suppression Was Found in The Dual-Site Active Rtms Group, but Not in The Sham Rtms Group. | Yes |
| Nyenhuis, 2013 [35] | Internet Training, Bibliotherapy, Group Treatment or An Information-Only Condition. | Information Only | Clear | Primary: TQ, Secondary: BL, PHQ-D | 9 Months | 80.0% | Improvement Rates Were Higher in The Active Training Conditions Than in The Control Condition, And Deterioration Rates Were Generally Lower in The Training Conditions In TQ. | Yes |
| Pal, 2015 [48] | transcranial direct current stimulation (TDCS) | Unclear | Primary: THI, Secondary: STSS, HAD, VAS, CGI | 3 Months | 80.0% | This TDCS Protocol Did Not Show A Beneficial Effect on Tinnitus. | No | |
| Plewnia, 2012 [28] | CTBS Over the Secondary Auditory Cortex (SAC), The Temporoparietal Association Cortex (TAC), Or Sham Stimulation [Placebo (PLC)]. | Placebo | Clear | TQ | 3 Months | 80% | No Difference Between Real and Sham Treatments nor Between Temporal and Temporoparietal Ctbs. | No |
| Prozchazkova, 2019 [83] | Ginkgo Biloba | Pentoxifylline | Unclear | VAS, Mini TQ, HADS | 3 Months | No | Both Gingko Biloba and Pentoxifylline Improve Mini TQ. No Difference Between Groups | Yes |
| Radunz, 2019 [84] | Gingko Biloba | HA | Unclear | THI, VAS | 6 Months | No | Both Gingko Biloba Improved Compared to Baseline, No Difference Between Groups Though, Apart from Long Lasting Tinnitus | Yes |
| Rocha, 2012 [29] | 10 Sessions of Myofascial Trigger Point Deactivation | 10 Sessions with Sham Deactivation | Unclear | THI | 3 Months | No | MTP Deactivation Through Digital Pressure Was Deemed Effective in Each and Every Tinnitus Variable Under Evaluation and In the Medium Run Responsiveness to Treatment Remained Stable In 75.8% Patients. | Yes |
| Rojas-Roncancio, 2016 [57] | Manganese and Lipoflavonoid Plus | Lipoflavonoid Plus | Unclear | THQ, TPFQ | 6 Months | No | No Significant Improvement in Both Groups | No |
| Roland, 2016 [58] | Sham or Active Treatment rTMS to TPJ | Sham Rtms to TPJ | Clear | 2 or 4 Weeks | No | No Changes in Neural Connectivity Following Rtms Therapy. Results Suggest Instead That the TPJ May Not Be an Ideal Target for Tinnitus Treatment. | No | |
| Sahlsten, 2017 [71] | rTMS | Placebo Rtms | Unclear | THI, VAS | 6 Months | 80% | Improvement for The VAS Scores (Intensity, Annoyance, Distress) And THI Scores Both in The Active Rtms Group and The Placebo Group. | No |
| Sahlsten, 2019 [85] | rTMS With and Without Neuronavigation for 2 Weeks In 2000 Hz | With and Without Neurostimulation | Unclear | THI, Global Impression of Change | 3 Months | No | No Significant Difference Between Groups, However Significant Improvement in Both | No |
| Scherer, 2019 [86] | TRT, including tinnitus specific counseling (TC) and sound-therapy (ST) Implemented with Ear- Level sound generators (SGS); Partial TRT, Including TC and Placebo SGS; Or Standard of Care (SoC) | Placebo SGS Or Standard of Care (Soc) | Clear | Primary: TQ, Secondary: TFI, THI, VAS | 18 Months | 80.0% | No Meaningful Differences Between TRT And Soc (Our Primary Comparison) Or Between Partial TRT And Soc Or TRT (Our Secondary Comparisons). | No |
| Shekhawat, 2014 [41] | Transcranial direct current stimulation (TDCS) | Sham Stimulation | Clear | TFI, THI, THQ, MML | 7 Months | No | No Significant Differences for Any of The Questionnaires; Decrease in MML For the RTMS Group | No |
| Singh, 2016 [59] | B12 | Placebo | Unclear | Matching, TSI | 1 Month | No | Improvement in Patients with B12 Insufficiency, Hence in A Very Small Sample | No |
| Sönmez, 2013 [36] | Ozone | Betahistine | Unclear | THI, Loudness Scale | 6 Months | No | No Differences Between Ozone and Betahistine, Both Showed Improvement Compared to Baseline Though | Yes |
| Stein, 2016 [60] | Fixed Notch-TMNMT | Placebo (Moving Notch) | Clear | THQ, VAS | 4 Months | 90.0% | Tinnitus Loudness and Other Measures of Tinnitus Distress Do Not Show Relevant Changes. | No |
| Sziklai, 2011 [19] | Pramipexole | Placebo | Clear | THI | 4 Weeks | No | No Cumulative Analysis. Greater Proportion of Patients Reporting Tinnitus Disappearance in The Interventional Group. Results Not Confirmed by Electrocochleography. | Unclear |
| Taslimi, 2013 [37] | Ondansedron | Placebo | Clear | THI, TSI, VAS, HADS | No | No Significant Differences Between Ondansedron And Placebo | No | |
| Tass, 2012 [30] | CR | Placebo | VAS, TQ | 12 Weeks | No | Improvement Before and After Treatment and Also Compared to Placebo | Yes | |
| Teismann, 2014 [42] | Anodal TDCS, Cathodal TDCS + TMNMT | Sham Stimulation + TMNMT | Unclear | THQ, THI, TQ | 31 Days | No | No Significant Modulating Effect of TDCS Polarity: Significant Main Effects or Interactions of TDCS Condition Were Neither Found in The Primary Outcome Measure nor In Any of The Secondary Outcome Measures (THI, TQ, Or Loudness VAS; | No |
| Thabit, 2015 [49] | rTMS | RTMS | Unclear | THI, VAS | 1 Month | No | Combination Treatment Significantly Better | Yes |
| Theodoroff, 2017 [72] | LEVO System with A Tinnitus-Matched Stimulus (TM Group) vs. LEVO System with A Noise Stimulus (NS Group; White Noise And/or Band Noise) vs. Marsona 1288 Sound Conditioner/Tinnitus Masker (Bedside Sound Generator Device; BSG Group). | BSG And NS Groups, but Not in The Same Manner as A Placebo-Controlled Group | Unclear | TFI, NRS, And LM at 1 kHz | 3 Months | No | Greater Average Improvement in Reactions to Tinnitus with TM or NS Devices Compared to The BSG Device. | Yes |
| Tutar, 2020 [88] | 10 Sessions Of 30 Minutes in One Month | Placebo | Unclear | THI, DASS | 4 Weeks | No | Significant Improvement in Uni- And Bilateral Groups Compared to Placebo | Yes |
| Tyler, 2017 [73] | VNS Implant-Paired | VNS Implant-Unpaired (Paired After 6 Weeks) | Clear | THI, TFI, THQ | 1 Year | No | No Significant Differences for Any of The Outcome Measures | No |
| Weise, 2016 [61] | 10-Week Guided Internet-Based Self-Help Program | DF | Unclear | Primary: THI, Mini-TQ, Secondary: HADS | 1 Year | No | ICBT Resulted to Significantly Better THI Scores Compared to Participation in An Online Forum | Yes |
| Westin, 2011 [20] | ACT, TRT | Wait List Control | Unclear | Primary: THI, Secondary: ISI, QOLI, HADS, CGI-I | 18 Months | 80% | ACT Is More Effective in Reducing Tinnitus Impact Than Tinnitus Retraining Therapy or Being on A Wait List. | Yes |
| Wise, 2016 [62] | Experimental Attention Training Game (“Terrain”) | A Control Game (“Tetris”) | Unclear | TFI, Secondary: THI, Tinnitus Severity Numeric Scales | 20 Days | 92% | TFI Scores Improved Following The 20-Day Use for the “Terrain” Program Compared with The Nonauditory “Tetris” Group. | Yes |
| Yakunina, 2019 [87] | HAs With WDRC, HAs With FT, Or HAs With LFT | FL Techniques (LFT and FT) Group | Clear | Primary: THI, Secondary: VAS | 6 Months | 80.0% | No Significant Differences Were Found Between Conventional Has And FL-Type Has in Terms of Tinnitus Relief Among Patients With HFHL. | No |
| Zarenoe, 2016 [63] | MI Group Received A Brief MI Program, Whereas Patients in The SP Group Underwent Conventional Hearing Aid Fitting. | Conventional Hearing Aid Fitting Group | Unclear | THI, IOI-HA | 3 Months | No | The MI Intervention Did Not Appear to Have Any Additional Effect on Hearing Aid Fitting Compared to Conventional Hearing Rehabilitation. | No |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kikidis, D.; Vassou, E.; Schlee, W.; Iliadou, E.; Markatos, N.; Triantafyllou, A.; Langguth, B. Methodological Aspects of Randomized Controlled Trials for Tinnitus: A Systematic Review and How a Decision Support System Could Overcome Barriers. J. Clin. Med. 2021, 10, 1737. https://doi.org/10.3390/jcm10081737
Kikidis D, Vassou E, Schlee W, Iliadou E, Markatos N, Triantafyllou A, Langguth B. Methodological Aspects of Randomized Controlled Trials for Tinnitus: A Systematic Review and How a Decision Support System Could Overcome Barriers. Journal of Clinical Medicine. 2021; 10(8):1737. https://doi.org/10.3390/jcm10081737
Chicago/Turabian StyleKikidis, Dimitrios, Evgenia Vassou, Winfried Schlee, Eleftheria Iliadou, Nikolaos Markatos, Aikaterini Triantafyllou, and Berthold Langguth. 2021. "Methodological Aspects of Randomized Controlled Trials for Tinnitus: A Systematic Review and How a Decision Support System Could Overcome Barriers" Journal of Clinical Medicine 10, no. 8: 1737. https://doi.org/10.3390/jcm10081737