
Severe Tachycardia Associated with Psychotropic Medications in Psychiatric Inpatients: A Study of Hospital Medical Emergency Team Activation

 , ,
, ,
Abstract
:1. Introduction
2. Methods
2.1. Study Design and Setting
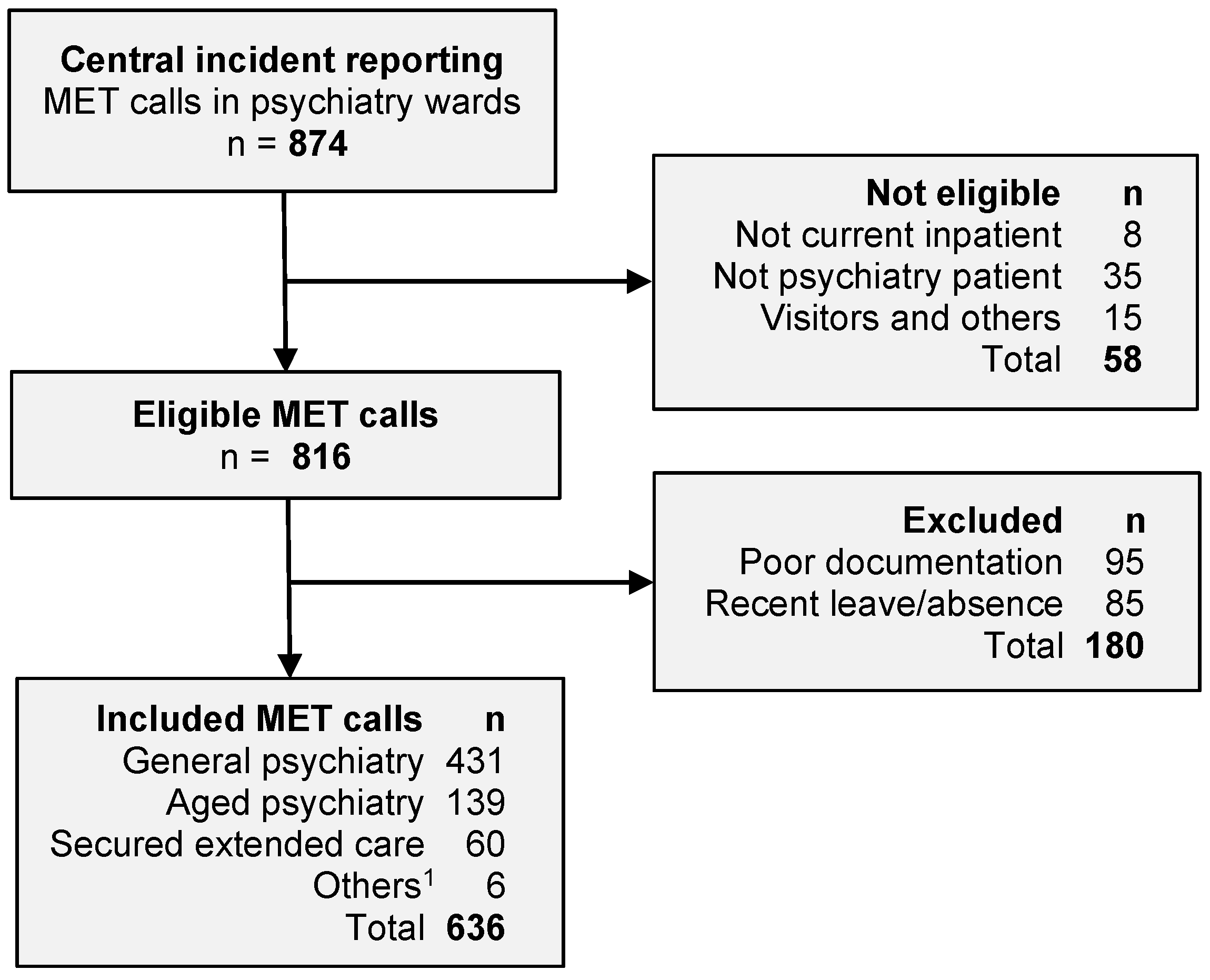
2.2. Participants and Ethics Approval
2.3. Medical Emergency Team
2.4. Study Outcome and Variable Definitions
2.5. Statistics
3. Results
3.1. Patient Characteristics
3.2. Tachycardia
3.3. Factors Associated with Tachycardia
3.4. Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Leucht, S.; Leucht, C.; Huhn, M.; Chaimani, A.; Mavridis, D.; Helfer, B.; Samara, M.; Rabaioli, M.; Bacher, S.; Cipriani, A.; et al. Sixty Years of Placebo-Controlled Antipsychotic Drug Trials in Acute Schizophrenia: Systematic Review, Bayesian Meta-Analysis, and Meta-Regression of Efficacy Predictors. Am. J. Psychiatry 2017, 174, 927–942. [Google Scholar] [CrossRef]
- Paton, C.; Duffett, R.; Harrington, M.; Lelliott, P.; Okocha, C.; Sensky, T. Patterns of antipsychotic and anticholinergic prescribing for hospital inpatients. J. Psychopharmacol. 2003, 17, 223–229. [Google Scholar] [CrossRef]
- Leung, J.Y.; Barr, A.M.; Procyshyn, R.M.; Honer, W.G.; Pang, C.C. Cardiovascular side-effects of antipsychotic drugs: The role of the autonomic nervous system. Pharmacol. Ther. 2012, 135, 113–122. [Google Scholar] [CrossRef] [PubMed]
- Jones, D.; Bellomo, R.; DeVita, M.A. Effectiveness of the Medical Emergency Team: The importance of dose. Crit. Care 2009, 13, 313. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, C.S.; Tsai, Y.T.; Tsai, H.J. Antipsychotic drugs and the risk of ventricular arrhythmia and/or sudden cardiac death: A nation-wide case-crossover study. J. Am. Heart Assoc. 2015, 4. [Google Scholar] [CrossRef] [PubMed]
- Liperoti, R.; Gambassi, G.; Lapane, K.L.; Chiang, C.; Pedone, C.; Mor, V.; Bernabei, R. Conventional and atypical antipsychotics and the risk of hospitalization for ventricular arrhythmias or cardiac arrest. Arch. Intern. Med. 2005, 165, 696–701. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chou, R.H.; Lo, L.W.; Liou, Y.J.; Shu, J.H.; Hsu, H.C.; Liang, Y.; Huang, C.C.; Huang, P.H.; Lin, S.J.; Chen, J.W.; et al. Antipsychotic treatment is associated with risk of atrial fibrillation: A nationwide nested case-control study. Int. J. Cardiol. 2017, 227, 134–140. [Google Scholar] [CrossRef] [PubMed]
- Nilsson, B.M.; Lindstrom, L.; Mohsen, I.; Holmlov, K.; Boden, R. Persistent tachycardia in clozapine treated patients: A 24-hour ambulatory electrocardiogram study. Schizophr. Res. 2018, 199, 403–406. [Google Scholar] [CrossRef]
- Gopal, S.; Hough, D.; Karcher, K.; Nuamah, I.; Palumbo, J.; Berlin, J.A.; Baseman, A.; Xu, Y.; Kent, J. Risk of cardiovascular morbidity with risperidone or paliperidone treatment: Analysis of 64 randomized, double-blind trials. J. Clin. Psychopharmacol. 2013, 33, 157–161. [Google Scholar] [CrossRef] [PubMed]
- Gopinathannair, R.; Etheridge, S.P.; Marchlinski, F.E.; Spinale, F.G.; Lakkireddy, D.; Olshansky, B. Arrhythmia-Induced Cardiomyopathies: Mechanisms, Recognition, and Management. J. Am. Coll. Cardiol. 2015, 66, 1714–1728. [Google Scholar] [CrossRef] [Green Version]
- Huizar, J.F.; Ellenbogen, K.A.; Tan, A.Y.; Kaszala, K. Arrhythmia-Induced Cardiomyopathy: JACC State-of-the-Art Review. J. Am. Coll. Cardiol. 2019, 73, 2328–2344. [Google Scholar] [CrossRef]
- Donghua, Z.; Jian, P.; Zhongbo, X.; Feifei, Z.; Xinhui, P.; Hao, Y.; Fuqiang, L.; Yan, L.; Yong, X.; Xinfu, H.; et al. Reversal of cardiomyopathy in patients with congestive heart failure secondary to tachycardia. J. Interv. Card Electrophysiol. 2013, 36, 27–32; discussion 32. [Google Scholar] [CrossRef]
- Medi, C.; Kalman, J.M.; Haqqani, H.; Vohra, J.K.; Morton, J.B.; Sparks, P.B.; Kistler, P.M. Tachycardia-mediated cardiomyopathy secondary to focal atrial tachycardia: Long-term outcome after catheter ablation. J. Am. Coll. Cardiol. 2009, 53, 1791–1797. [Google Scholar] [CrossRef] [Green Version]
- Kavanaugh, M.; McDivitt, J.; Philip, A.; Froehner, J.W.; Rotruck, J.; Hemann, B.; Haigney, M.; Atwood, J.; Nations, J.A. Cardiomyopathy induced by sinus tachycardia in combat wounded: A case study. Mil. Med. 2014, 179, e1062–e1064. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Romeo, E.; Grimaldi, N.; Sarubbi, B.; D’Alto, M.; Santarpia, G.; Scognamiglio, G.; Russo, M.G.; Calabro, R. A pediatric case of cardiomyopathy induced by inappropriate sinus tachycardia: Efficacy of ivabradine. Pediatr. Cardiol. 2011, 32, 842–845. [Google Scholar] [CrossRef]
- Winum, P.F.; Cayla, G.; Rubini, M.; Beck, L.; Messner-Pellenc, P. A case of cardiomyopathy induced by inappropriate sinus tachycardia and cured by ivabradine. Pacing Clin. Electrophysiol. 2009, 32, 942–944. [Google Scholar] [CrossRef]
- Shabtaie, S.A.; Witt, C.M.; Asirvatham, S.J. Natural history and clinical outcomes of inappropriate sinus tachycardia. J. Cardiovasc. Electrophysiol. 2020, 31, 137–143. [Google Scholar] [CrossRef] [PubMed]
- Tajiri, M.; Suzuki, Y.; Sugai, T.; Tsuneyama, N.; Someya, T. Effects of olanzapine on resting heart rate in Japanese patients with schizophrenia. PLoS ONE 2018, 13, e0199922. [Google Scholar] [CrossRef]
- Agelink, M.W.; Majewski, T.; Wurthmann, C.; Lukas, K.; Ullrich, H.; Linka, T.; Klieser, E. Effects of newer atypical antipsychotics on autonomic neurocardiac function: A comparison between amisulpride, olanzapine, sertindole, and clozapine. J. Clin. Psychopharmacol. 2001, 21, 8–13. [Google Scholar] [CrossRef] [PubMed]
- Cohen, H.; Loewenthal, U.; Matar, M.; Kotler, M. Association of autonomic dysfunction and clozapine. Heart rate variability and risk for sudden death in patients with schizophrenia on long-term psychotropic medication. Br. J. Psychiatry 2001, 179, 167–171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nilsson, B.M.; Edstrom, O.; Lindstrom, L.; Wernegren, P.; Boden, R. Tachycardia in patients treated with clozapine versus antipsychotic long-acting injections. Int. Clin. Psychopharmacol. 2017, 32, 219–224. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tse, G.; Li, K.H.C.; Cheung, C.K.Y.; Letsas, K.P.; Bhardwaj, A.; Sawant, A.C.; Liu, T.; Yan, G.X.; Zhang, H.; Jeevaratnam, K.; et al. Arrhythmogenic mechanisms in hypokalaemia: Insights from pre-clinical models. Front. Cardiovasc. Med. 2021, 8, 620539. [Google Scholar] [CrossRef]
- Helfant, R.H. Hypokalemia and arrhythmias. Am. J. Med. 1986, 80 (Suppl. 1), 13–22. [Google Scholar] [CrossRef]
- DiNicolantonio, J.J.; Liu, J.; O’Keefe, J.H. Magnesium for the prevention and treatment of cardiovascular disease. Open Heart 2018, 5, e000775. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cooper, H.A.; Domanski, M.J.; Rosenberg, Y.; Norman, J.; Scott, J.H.; Assmann, S.F.; McKinlay, S.M.; Hochman, J.S.; Antman, E.M.; Magnesium in Coronaries trial Investigators. Acute ST-segment elevation myocardial infarction and prior stroke: An analysis from the Magnesium in Coronaries (MAGIC) trial. Am. Heart J. 2004, 148, 1012–1019. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Patient Characteristic | All MET Calls n = 636 | No Tachycardia n = 499 | Tachycardia n = 137 |
|---|---|---|---|
| Age, median (IQR), years | 42 (30–61) | 45 (31–64) | 36 (28–46) |
| Male, n (%) | 324 (50.9) | 260 (52.1) | 64 (46.7) |
| Body mass index <18 kg/m2, n (%) | 38 (6.0) | 31 (6.2) | 7 (5.1) |
| Diabetes mellitus, n (%) | 138 (21.7) | 112 (22.4) | 26 (19.0) |
| Cardiovascular disease, n (%) 1 | 85 (13.4) | 73 (14.6) | 12 (8.8) |
| Coronary artery disease | 52 (8.2) | 46 (9.2) | 6 (4.4) |
| Heart failure | 25 (3.9) | 19 (3.8) | 6 (4.4) |
| Stroke | 28 (4.4) | 24 (4.8) | 4 (2.9) |
| Atrial fibrillation, n (%) | 16 (2.5) | 8 (1.6) | 8 (5.8) |
| Chronic | 12 (1.9) | 6 (1.2) | 6 (4.4) |
| Acute onset | 4 (0.6) | 2 (0.4) | 2 (1.5) |
| Chronic lung disease, n (%) | 96 (15.1) | 71 (14.2) | 25 (18.3) |
| Smoking, n (%) | 296 (46.5) | 229 (45.9) | 67 (48.9) |
| Excessive alcohol, n (%) | 144 (22.6) | 106 (21.2) | 38 (27.7) |
| Illicit drug use, n (%) | 255 (40.1) | 189 (37.9) | 66 (48.2) |
| Recent ECT, n (%) | 40 (6.3) | 31 (6.2) | 9 (6.6) |
| Potassium, mean (SD), mmol/L 2 | 4.19 (0.52) | 4.20 (0.52) | 4.13 (0.52) |
| Hypokalemia, n (%) 2 | 23 (3.9) | 15 (3.2) | 8 (6.1) |
| Hyperkalemia, n (%) 2 | 16 (2.7) | 14 (3.0) | 2 (1.5) |
| Magnesium, mean (SD), mmol/L 3 | 0.83 (0.10) | 0.83 (0.10) | 0.82 (0.10) |
| Hypomagnesemia, n (%) 3 | 45 (8.8) | 37 (9.5) | 8 (6.6) |
| Hypermagnesemia, n (%) 3 | 4 (1.0) | 0 (0) | 4 (0.8) |
| Primary psychiatric diagnosis: | |||
| Schizophrenia/psychotic, n (%) | 249 (39.2) | 170 (34.1) | 79 (57.7) |
| Anxiety/depression, n (%) | 117 (18.4) | 89 (17.8) | 28 (20.4) |
| BPSD, n (%) | 64 (10.1) | 60 (12.0) | 4 (2.9) |
| Bipolar disorder, n (%) | 60 (9.4) | 51 (10.2) | 9 (6.6) |
| Alcohol & substance misuse, n (%) | 55 (8.6) | 50 (10.0) | 5 (3.6) |
| Stress & adjustment disorder, n (%) | 18 (2.8) | 16 (3.2) | 2 (1.5) |
| Other disorders, n (%) | 73 (11.5) | 63 (12.6) | 10 (7.3) |
| Medications, n (%) | All MET Calls n = 636 | No Tachycardia n = 499 | Tachycardia n = 137 |
|---|---|---|---|
| Antipsychotics: | |||
| Conventional (first-generation) | 63 (9.9) | 44 (8.8) | 19 (13.9) |
| Atypical (second-generation) | 443 (69.7) | 338 (67.7) | 105 (76.6) |
| Antidepressants: | |||
| SSRI or SNRI | 206 (32.4) | 170 (34.1) | 36 (26.3) |
| Tricyclic antidepressants | 38 (6.0) | 31 (6.2) | 7 (5.1) |
| Combination & others 1 | 25 (3.9) | 16 (3.2) | 9 (6.6) |
| Mood stabilizers: | |||
| Valproate | 126 (19.8) | 100 (20.0) | 26 (19.0) |
| Lithium | 28 (4.4) | 22 (4.4) | 6 (4.4) |
| Others 2 | 32 (5.0) | 30 (4.7) | 2 (1.5) |
| Other medications: | |||
| Benzodiazepines | 398 (62.6) | 320 (64.1) | 78 (56.9) |
| Anticholinergics | 51 (8.0) | 32 (6.4) | 19 (13.9) |
| Antiplatelets | 71 (11.2) | 64 (12.8) | 7 (5.1) |
| Anticoagulation | 44 (6.9) | 36 (7.2) | 8 (5.8) |
| Beta-blockers | 104 (16.4) | 82 (16.4) | 22 (16.1) |
| Renin-angiotensin system inhibitor | 78 (12.3) | 70 (14.0) | 8 (5.8) |
| Calcium channel blocker | 24 (3.8) | 24 (4.8) | 0 (0) |
| Diuretics | 37 (5.8) | 29 (5.8) | 7 (5.1) |
| Oral hypoglycemic or insulin | 102 (16.0) | 83 (16.6) | 20 (14.6) |
| Inhaled bronchodilators | 86 (13.5) | 65 (13.0) | 21 (15.3) |
| Opioid analgesics | 104 (16.4) | 89 (17.8) | 15 (11.0) |
| Electrocardiogram Findings | Number | Percent |
|---|---|---|
| Sinus tachycardia | 117 | 60.6 |
| Prolonged QTc interval | 21 | 10.9 |
| Atrial fibrillation | 16 | 8.3 |
| Conduction or T-wave abnormality | 16 | 8.3 |
| Sinus bradycardia | 14 | 7.3 |
| Supraventricular tachycardia | 6 | 3.1 |
| Other | 3 | 1.6 |
| Variable | Odds Ratio (95% CI) | p-Value |
|---|---|---|
| Age, per 10 years | 0.70 (0.58–0.84) | <0.001 |
| Female | 0.63 (0.33–1.22) | 0.173 |
| Body mass index: | ||
| 18 to 30 kg/m2 | 1.00 (reference) | 0.950 |
| <18 kg/m2 | 1.07 (0.27–4.31) | |
| >30 kg/m2 | 1.15 (0.48–2.77) | |
| Diabetes mellitus | 0.83 (0.37–1.86) | 0.645 |
| Cardiovascular disease | 0.42 (0.14–1.13) | 0.085 |
| Chronic lung disease | 1.59 (0.69–3.68) | 0.280 |
| Cigarette smoking | 1.18 (0.64–2.16) | 0.600 |
| Excessive alcohol intake | 1.27 (0.87–1.85) | 0.217 |
| History of illicit drug use | 1.85 (1.00–3.44) | 0.051 |
| Recent electroconvulsive treatment | 1.46 (0.73–2.91) | 0.283 |
| Antipsychotics vs. none | 4.71 (1.83–12.1) | 0.001 |
| Antipsychotics by class: | ||
| None | 1.00 (reference) | 0.004 |
| Conventional (first-generation) | 7.40 (2.09–26.2) | |
| Atypical (second-generation) | 4.42 (1.71–11.4) | |
| Antidepressants | 1.05 (0.84–1.32) | 0.651 |
| Mood stabilizers | 0.90 (0.75–1.09) | 0.289 |
| Benzodiazepines | 0.64 (0.35–1.17) | 0.149 |
| Anticholinergics | 4.09 (1.42–11.8) | 0.009 |
| Beta-blockers | 1.15 (0.49–2.70) | 0.739 |
| Inhaled bronchodilators | 1.06 (0.86–1.30) | 0.584 |
| Temperature >38 °C | 5.96 (2.19–16.2) | <0.001 |
| Diagnosis of infection | 1.90 (0.79–4.56) | 0.151 |
| Diagnosis of dehydration | 0.88 (0.31–2.45) | 0.789 |
| Venous thromboembolism | 1.14 (0.33–3.91) | 0.836 |
| Hypoglycemia | 0.23 (0.05–1.05) | 0.059 |
| Hypokalemia | 2.74 (0.61–12.3) | 0.187 |
| Hypomagnesemia | 0.60 (0.17–2.14) | 0.433 |
| Oxygen saturation <90% | 0.64 (0.23–1.75) | 0.380 |
| Model | Specification | OR (95% CI) | ICC (95% CI) |
|---|---|---|---|
| 1 | Main effects model 1 | 4.98 (2.19–12.8) | 0.39 (0.19–0.63) |
| 2 | Antipsychotics as nominal variable: 1 | ||
| No antipsychotics | 1.00 (reference) | 0.38 (0.18–0.63) | |
| Conventional | 6.54 (2.04–20.9) | ||
| Atypical | 5.01 (2.05–12.2) | ||
| 3 | Model 1 with VTE and infection excluded 2 | 4.40 (1.75–11.0) | 0.36 (0.16–0.63) |
| 4 | Model 3 with benzodiazepine dropped | 4.09 (1.64–10.2) | 0.37 (0.17–0.63) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lim, A.K.H.; Azraai, M.; Pham, J.H.; Looi, W.F.; Wirth, D.; Ng, A.S.L.; Babu, U.; Saluja, B. Severe Tachycardia Associated with Psychotropic Medications in Psychiatric Inpatients: A Study of Hospital Medical Emergency Team Activation. J. Clin. Med. 2021, 10, 1534. https://doi.org/10.3390/jcm10071534
Lim AKH, Azraai M, Pham JH, Looi WF, Wirth D, Ng ASL, Babu U, Saluja B. Severe Tachycardia Associated with Psychotropic Medications in Psychiatric Inpatients: A Study of Hospital Medical Emergency Team Activation. Journal of Clinical Medicine. 2021; 10(7):1534. https://doi.org/10.3390/jcm10071534
Chicago/Turabian StyleLim, Andy K. H., Meor Azraai, Jeanette H. Pham, Wenye F. Looi, Daniel Wirth, Ashley S. L. Ng, Umesh Babu, and Bharat Saluja. 2021. "Severe Tachycardia Associated with Psychotropic Medications in Psychiatric Inpatients: A Study of Hospital Medical Emergency Team Activation" Journal of Clinical Medicine 10, no. 7: 1534. https://doi.org/10.3390/jcm10071534