
Exploring the Biopsychosocial Pathways Shared by Obstructive Sleep Apnea (OSA) and Central Serous Chorioretinopathy (CSC): A Literature Overview


{kind=link}
Abstract
:1. Introduction
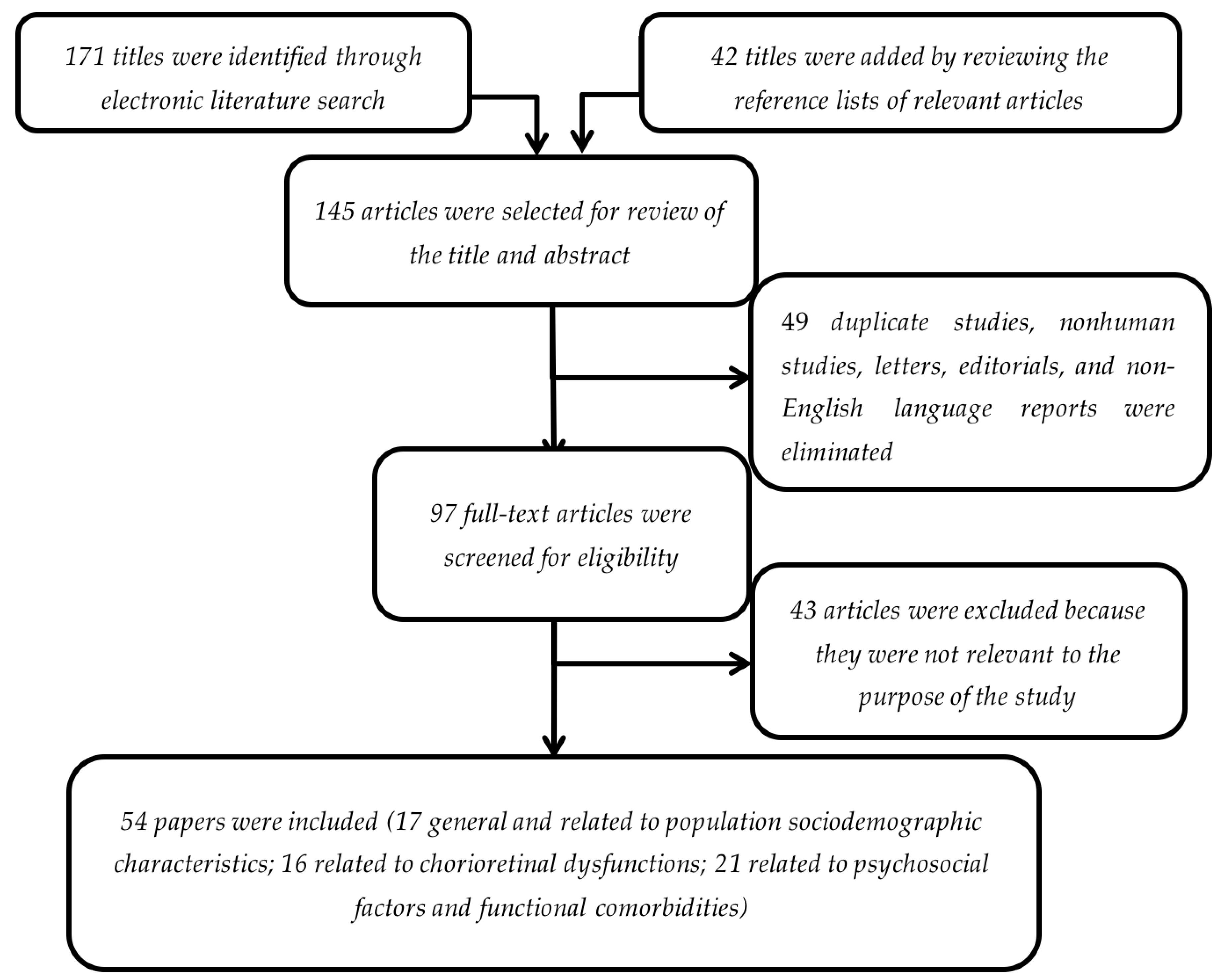
2. Methods
3. Results and Discussion
3.1. Sociodemographic Characteristics of OSA and CSC Populations
3.2. OSA- and CSC-Related Chorioretinal Dysfunctions
3.3. Psychosocial Factors and Functional Comorbidities Associated with Both OSA and CSC
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Engel, G.L. The need for a new medical model: A challenge for biomedicine. Science 1977, 196, 129–136. [Google Scholar] [CrossRef] [PubMed]
- Engel, G.L. The clinical application of the biopsychosocial model. J. Med. Philos. 1981, 6, 1–23. [Google Scholar] [CrossRef] [PubMed]
- Wade, D.T.; Halligan, P.W. The biopsychosocial model of illness: A model whose time has come. Clin. Rehabil. 2017, 31, 995–1004. [Google Scholar] [CrossRef] [PubMed]
- Karunamuni, N.; Imayama, I.; Goonetilleke, D. Pathways to well-being: Untangling the causal relationships among biopsychosocial variables. Soc. Sci. Med. 2020, 10, 112846. [Google Scholar] [CrossRef] [PubMed]
- AASM. International Classification of Sleep Disorders: Diagnostic and Coding Man; American Academy of Sleep Medicine: Westchester, IL, USA, 2005. [Google Scholar]
- Marin, J.M.; Carrizo, S.J.; Vicente, E.; Agusti, A.G. Long-term cardiovascular outcomes in men with obstructive sleep apnoea-hypopnoea with or without treatment with continuous positive airway pressure: An observational study. Lancet 2005, 365, 1046–1053. [Google Scholar] [CrossRef]
- Imani, M.M.; Sadeghi, M.; Khazaie, H.; Emami, M.; Sadeghi Bahmani, D.; Brand, S. Evaluation of Serum and Plasma Interleukin-6 Levels in Obstructive Sleep Apnea Syndrome: A Meta-Analysis and Meta-Regression. Front. Immunol. 2020, 11, 1343. [Google Scholar] [CrossRef]
- Imani, M.M.; Sadeghi, M.; Khazaie, H.; Emami, M.; Sadeghi Bahmani, D.; Brand, S. Serum and Plasma Tumor Necrosis Factor Alpha Levels in Individuals with Obstructive Sleep Apnea Syndrome: A Meta-Analysis and Meta-Regression. Life 2020, 10, 87. [Google Scholar] [CrossRef]
- Imani, M.M.; Sadeghi, M.; Khazaie, H.; Sanjabi, A.; Brand, S.; Brühl, A.; Sadeghi Bahmani, D. Associations between Morning Salivary and Blood Cortisol Concentrations in Individuals with Obstructive Sleep Apnea Syndrome: A Meta-Analysis. Front. Endocrinol. (Lausanne) 2020, 11, 568823. [Google Scholar] [CrossRef]
- Mohammadi, H.; Aarabi, A.; Rezaei, M.; Khazaie, H.; Brand, S. Sleep Spindle Characteristics in Obstructive Sleep Apnea Syndrome (OSAS). Front. Neurol. 2021, 12, 134. [Google Scholar] [CrossRef]
- Grover, D.P. Obstructive sleep apnea and ocular disorders. Curr. Opin. Ophthalmol. 2010, 21, 454–458. [Google Scholar] [CrossRef] [Green Version]
- Glacet-Bernard, A.; les Jardins, G.L.; Lasry, S.; Coscas, G.; Soubrane, G.; Souied, E.; Housset, B. Obstructive sleep apnea among patients with retinal vein occlusion. Arch. Ophthalmol. 2010, 128, 1533–1538. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, C.Y.; Riangwiwat, T.; Rattanawong, P.; Nesmith, B.L.W.; Deobhakta, A. Association of obstructive sleep apnea with central serous chorioretinopathy and choroidal thickness. Retina 2018, 38, 1642–1651. [Google Scholar] [CrossRef]
- Gass, J.D. Pathogenesis of disciform detachment of the neuroepithelium: II. Idiopathic central serous choroidopathy. Am. J. Ophthalmol. 1967, 63, 587–643. [Google Scholar]
- Daruich, A.; Matet, A.; Dirani, A.; Bousquet, E.; Zhao, M.; Farman, N.; Behar-Cohen, F. Central serous chorioretinopathy: Recent findings and new physiopathology hypothesis. Prog. Retin. Eye Res. 2015, 48, 82–118. [Google Scholar] [CrossRef] [Green Version]
- Leveque, T.K.; Yu, L.; Musch, D.C.; Chervin, R.D.; Zacks, D.N. Central serous chorioretinopathy and risk for obstructive sleep apnea. Sleep Breath. 2007, 11, 253–257. [Google Scholar] [CrossRef] [PubMed]
- Nicholson, B.P.; Atchison, E.; Idris, A.A.; Bakri, S.J. Central serous chorioretinopathy and glucocorticoids: An update on evidence for association. Surv. Ophthalmol. 2018, 63, 1–8. [Google Scholar] [CrossRef]
- Scarinci, F.; Ghiciuc, C.M.; Patacchioli, F.R.; Palmery, M.; Parravano, M. Investigating the Hypothesis of Stress System Dysregulation as A Risk Factor for Central Serous Chorioretinopathy: A Literature Mini-Review. Curr. Eye Res. 2019. [Google Scholar] [CrossRef] [PubMed]
- Muñoz, A.; Mayoralas, L.R.; Barbé, F.; Pericás, J.; Agusti, A.G. Long-term effects of CPAP on daytime functioning in patients with sleep apnoea syndrome. Eur. Respir. J. 2000, 15, 676–681. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chan, W.M.; Lai, T.Y.; Lai, R.Y.; Tang, E.W.; Liu, D.T.; Lam, D.S. Safety enhanced photodynamic therapy for chronic central serous chorioretinopathy: One-year results of a prospective study. Retina 2008, 28, 85–93. [Google Scholar] [CrossRef]
- Pamidi, S.; Knutson, K.L.; Ghods, F.; Mokhlesi, B. Depressive symptoms and obesity as predictors of sleepiness and quality of life in patients with REM-related obstructive sleep apnea: Cross-sectional analysis of a large clinical population. Sleep Med. 2011, 12, 827–831. [Google Scholar] [CrossRef]
- Siguan, C.S.; Aguilar, R.N. Psychological profile of patients with central serous retinopathy. Philipp. J. Ophthalmol. 2014, 39, 16–20. [Google Scholar]
- Grant, M.J.; Booth, A. A typology of reviews: An analysis of 14 review types and associated methodologies. Health Inf. Libr. J. 2009, 26, 91–108. [Google Scholar] [CrossRef] [PubMed]
- Liu, P.-K.; Chang, Y.-C.; Tai, M.-H.; Tsai, R.-K.; Chong, I.-W.; Wu, K.-Y.; Wu, W.-C.; Hsu, C.-Y.; Tsai, M.-J. The association between central serous chorioretinopathy and sleep apnea. Retina (Phila. PA) 2019, 1. [Google Scholar] [CrossRef] [PubMed]
- Brodie, F.L.; Charlson, E.S.; Aleman, T.S.; Salvo, R.T.; Gewaily, D.Y.; Lau, M.K.; Farren, N.D.; Engelhard, S.B.; Pistilli, M.; Brucker, A.J. Obstructive sleep apnea and central serous chorioretinopathy. Retina 2015, 35, 238–243. [Google Scholar] [CrossRef] [Green Version]
- Huon, L.K.; Liu, S.Y.; Camacho, M.; Guilleminault, C. The association between ophthalmologic diseases and obstructive sleep apnea: A systematic review and meta-analysis. Sleep Breath. 2016, 20, 1145–1154. [Google Scholar] [CrossRef]
- Pan, C.K.; Vail, D.; Bhattacharya, J.; Cao, M.; Mruthyunjaya, P. The Effect of Obstructive Sleep Apnea on Absolute Risk of Central Serous Chorioretinopathy. Am. J. Ophthalmol. 2020, 218, 148–155. [Google Scholar] [CrossRef]
- Jain, A.K.; Kaines, A.; Schwartz, S. Bilateral central serous chorioretinopathy resolving rapidly with treatment for obstructive sleep apnea. Graefe’s Arch. Clin. Exp. Ophthalmol. 2010, 248, 1037–1039. [Google Scholar] [CrossRef]
- Huang, T.; Lin, B.M.; Markt, S.C.; Stampfer, M.J.; Laden, F.; Hu, F.B.; Tworoger, S.S.; Redline, S. Sex differences in the associations of obstructive sleep apnoea with epidemiological factors. Eur. Respir. J. 2018, 51, 1702421. [Google Scholar] [CrossRef]
- Kaczmarek, E.; Bakker, J.P.; Clarke, D.N.; Csizmadia, E.; Kocher, O.; Veves, A.; Tecilazich, F.; O’Donnell, C.P.; Ferran, C.; Malhotra, A. Molecular Biomarkers of Vascular Dysfunction in Obstructive Sleep Apnea. PLoS ONE 2013, 8, e70559. [Google Scholar] [CrossRef] [Green Version]
- Piccolino, F.C.; Lupidi, M.; Cagini, C.; Fruttini, D.; Nicolò, M.; Eandi, C.M.; Tito, S. Choroidal Vascular Reactivity in Central Serous Chorioretinopathy. Investig. Opthalmol. Vis. Sci. 2018, 59, 3897–3905. [Google Scholar] [CrossRef] [Green Version]
- Chung, Y.-R.; Kim, J.W.; Kim, S.W.; Lee, K. Choroidal thickness in patients with central serous chorioretinopathy. Retina 2016, 36, 1652–1657. [Google Scholar] [CrossRef] [PubMed]
- Bayhan, H.A.; Bayhan, S.A.; Intepe, Y.S.; Muhafiz, E.; Gurdal, C. Evaluation of the macular choroidal thickness using spectral optical coherence tomography in patients with obstructive sleep apnea syndrome. Clin. Experiment. Ophthalmol. 2015, 43, 139–144. [Google Scholar] [CrossRef]
- Ekinci, M.; Hüseyinoğlu, N.; Çağatay, H.H.; Keleş, S.; Ceylan, E.; Gökçe, G. Choroidal Thickening in Patients with Sleep Apnea Syndrome. Neuro-Ophthalmol. 2014, 38, 8–13. [Google Scholar] [CrossRef] [PubMed]
- Kara, S.; Ozcimen, M.; Bekci, T.T.; Sakarya, Y.; Gencer, B.; Tufan, H.A.; Arikan, S. Evaluation of choroidal thickness in patients with obstructive sleep apnea/hypopnea syndrome. Arq. Bras. Oftalmol. 2014, 77, 280–284. [Google Scholar] [CrossRef] [PubMed]
- Karalezli, A.; Eroglu, F.C.; Kivanc, T.; Dogan, R. Evaluation of choroidal thickness using spectral-domain optical coherence tomography in patients with severe obstructive sleep apnea syndrome: A comparative study. Int. J. Ophthalmol. 2014, 7, 1030–1034. [Google Scholar] [PubMed]
- He, M.; Han, X.; Wu, H.; Huang, W. Choroidal thickness changes in obstructive sleep apnea syndrome: A systematic review and meta-analysis. Sleep Breath. 2016, 20, 369–378. [Google Scholar] [CrossRef]
- Kim, Y.T.; Kang, S.W.; Bai, K.H. Choroidal thickness in both eyes of patients with unilaterally active central serous chorioretinopathy. Eye 2011, 25, 1635–1640. [Google Scholar] [CrossRef] [Green Version]
- Yang, L.; Jonas, J.B.; Wei, W. Optical coherence tomography–as-sisted enhanced depth imaging of central serous chorioretinopathy. Investig. Ophthalmol. Vis. Sci. 2013, 54, 4659–4665. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davila, J.; Azar, A.; Pasricha, M.V.; Al-Moujahed, A.; Mruthyunjaya, P.; Pan, C.K. Impact of Obstructive Sleep Apnea Treatment on Choroidal Thickness in Patients with Central Serous Chorioretinopathy. Investig. Ophthalmol. Vis. Sci. 2020, 61, 3240. [Google Scholar]
- Chung, Y.-R.; Kim, J.W.; Choi, S.-Y.; Park, S.W.; Kim, J.H.; Lee, K. Subfoveal choroidal thickness and vascular diameter in active and resolved central serous chorioretinopathy. Retina 2018, 38, 102–107. [Google Scholar] [CrossRef] [PubMed]
- Karaca, E.E.; Ekici, F.; Yalcin, N.G.; Ciftci, T.U.; Ozdek, S. Macular choroidal thicknessmeasurements in patients with obstructive sleep apnea syndrome. Sleep Breath. 2014, 19, 335–341. [Google Scholar] [CrossRef] [PubMed]
- Zengin, M.O.; Oz, T.; Baysak, A.; Cinar, E.; Kucukerdonmez, C. Changes in choroidal thickness in patients with obstructive sleep apnea syndrome. Ophthalmic Surg. Lasers Imaging Retin. 2014, 45, 298–304. [Google Scholar] [CrossRef] [PubMed]
- Sun, J.H.; Tan, J.; Wang, Z.; Yang, H.; Zhu, X.; Li, L. Effect of catecholamine on central serous chorioretinopathy. J. Huazhong Univ. Sci. Technol. Med. Sci. 2003, 23, 313–316. [Google Scholar]
- Tien, P.T.; Lai, C.Y.; Lin, C.J.; Chen, W.L.; Lin, P.K.; Muo, C.H.; Tsai, Y.Y.; Wan, L.; Ho, W.C.; Lin, H.J. Increased Risk of Central Serous Chorioretinopathy among Patients with Nonorganic Sleep Disturbance. J. Ophthalmol. 2020, 12, 1712503. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kloos, P.; Laube, I.; Thoelen, A. Obstructive sleep apnea in patients with central serous chorioretinopathy. Graefes Arch. Clin. Exp. Ophthalmol. 2008, 246, 1225–1228. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cortelli, P.; Lombardi, C.; Montagna, P.; Parati, G. Baroreflex modulation during sleep and in obstructive sleep apnea syndrome. Auton. Neurosci. 2012, 169, 7–11. [Google Scholar] [CrossRef] [PubMed]
- Tomfohr, L.M.; Edwards, K.M.; Dimsdale, J.E. Is obstructive sleep apnea associated with cortisol levels? A systematic review of the research evidence. Sleep Med. Rev. 2012, 16, 243–249. [Google Scholar] [CrossRef] [Green Version]
- Scarinci, F.; Patacchioli, F.R.; Ghiciuc, C.M.; Pasquali, V.; Bercea, R.M.; Cozma, S.; Parravano, M. Psychological Profile and Distinct Salivary Cortisol Awake Response (CAR) in Two Different Study Populations with Obstructive Sleep Apnea (OSA) and Central Serous Chorioretinopathy (CSC). J. Clin. Med. 2020, 9, 2490. [Google Scholar] [CrossRef]
- Ghiciuc, C.M.; Dima Cozma, L.C.; Bercea, R.M.; Lupusoru, C.E.; Mihaescu, T.; Szalontay, A.; Gianfreda, A.; Patacchioli, F.R. Restoring the salivary cortisol awakening response through nasal continuous positive airway pressure therapy in obstructive sleep apnea. Chronobiol. Int. 2013, 30, 1024–1031. [Google Scholar] [CrossRef] [PubMed]
- Kumar, M.; Van Dijk, E.H.C.; Raman, R.; Mehta, P.; Boon, C.J.F.; Goud, A.; Bharani, S.; Chhablani, J. Stress and vision-related quality of life in acute and chronic central serous chorioretinopathy. BMC Ophthalmol. 2020, 20, 90. [Google Scholar] [CrossRef] [Green Version]
- Huang, Q.R.; Qin, Z.; Zhang, S.; Chow, C.M. Clinical patterns of obstructive sleep apnea and its comorbid conditions: A data mining approach. J. Clin. Sleep Med. 2008, 4, 543–550. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harris, M.; Glozier, N.; Ratnavadivel, R.; Grunstein, R.R. Obstructive sleep apnea and depression. Sleep Med. Rev. 2009, 13, 437–444. [Google Scholar] [CrossRef] [PubMed]
- Spahn, C.; Wiek, J.; Burger, T.; Hansen, L. Psychosomatic aspects in patients with central serous chorioretinopathy. Br. J. Ophthalmol. 2003, 87, 704–708. [Google Scholar] [CrossRef]
- Kim, H.M.; Ahn, J.; Kim, T.W. Psychological Factors Associated with Central Serous Chorioretinopathy. J. Psychol. Psychother. 2016, 6, 250. [Google Scholar] [CrossRef]
- Mansour, A.M.; Hamam, R. Operating room central serous chorioretinopathy. Sage Open Med. Case Rep. 2017, 5, 2050313X17740052. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Conrad, R.; Geiser, F.; Kleiman, A.; Zur, B.; Karpawitz-Godt, A. Temperament and character personality profile and illness-related stress in central serous chorioretinopathy. Sci. World J. 2014. [Google Scholar] [CrossRef]
- Bazzazi, N.; Ahmadpanah, M.; Akbarzadeh, S.; Seif Rabiei, M.A.; Holsboer-Trachsler, E.; Brand, S. In patients suffering from idiopathic central serous chorioretinopathy, anxiety scores are higher than in healthy controls, but do not vary according to sex or repeated central serous chorioretinopathy. Neuropsychiatr. Dis. Treat. 2015, 11, 1131–1136. [Google Scholar]
- Agarwal, A.; Garg, M.; Dixit, N.; Godara, R. Evaluation and correlation of stress scores with blood pressure, endogenous cortisol levels, and homocysteine levels in patients with central serous chorioretinopathy and comparison with age-matched controls. Indian J. Ophthalmol. 2016, 64, 803–805. [Google Scholar] [CrossRef]
- Schwartz, R.; Rozenberg, A.; Loewenstein, A.; Goldstein, M. The relation of somatotypes and stress response to central serous chorioretinopathy. Graefes Arch. Clin. Exp. Ophthalmol. 2017, 255, 2307–2315. [Google Scholar] [CrossRef]
- Piskunowicz, M.; Jaracz, M.; Lesiewska, H.; Malukiewicz, G.; Brożek-Pestka, M.; Borkowska, A. Temperament Profile in Patients with Central Serous Chorioretinopathy: A Case-Control Study. Eur. J. Ophthalmol. 2014, 24, 392–395. [Google Scholar] [CrossRef]
- Williams, N.; Wilkinson, C.; Stott, N.; Menkes, D.B. Functional illness in primary care: Dysfunction versus disease. BMC Fam. Pract. 2008, 9. [Google Scholar] [CrossRef] [Green Version]
- Köseoğlu, H.İ.; İnanır, A.; Kanbay, A.; Okan, S.; Demir, O.; Çeçen, O.; İnanır, S. Is There a Link Between Obstructive Sleep Apnea Syndrome and Fibromyalgia Syndrome? Turk. Thorac. J. 2017, 18, 40–46. [Google Scholar] [CrossRef] [PubMed]
- Vespa, A.; Meloni, C.; Giulietti, M.V.; Ottaviani, M.; Spatuzzi, R.; Merico, F. Evaluation of Depression in Women Affected by Fibromyalgia Syndrome. J. Depress Anxiety 2015, 4, 1000178. [Google Scholar] [CrossRef]
- Balkarli, B.; Erol, M.K.; Yucel, O.; Akar, Y. Frequency of fibromyalgia syndrome in patients with central serous chorioretinopathy. Arq. Bras. Oftalmol. 2017, 80. [Google Scholar] [CrossRef]
- Kim, Y.-K.; Woo, J.; Park, K.H.; Chi, Y.K.; Han, J.W.; Kim, K.W. Association of Central Serous Chorioretinopathy with psychosocial factors is dependent on its phase and subtype. Korean J. Ophthalmol. 2018, 32, 281–289. [Google Scholar] [CrossRef] [PubMed]
- Seixas, A.; Ramos, A.R.; Gordon-Strachan, G.M.; Fonseca, V.A.; Zizi, F.; Jean-Louis, G. Relationship between Visual Impairment, Insomnia, Anxiety/Depressive Symptoms among Russian Immigrants. J. Sleep Med. Disord. 2014, 1, 1009. [Google Scholar] [PubMed]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Scarinci, F.; Patacchioli, F.R.; Parravano, M. Exploring the Biopsychosocial Pathways Shared by Obstructive Sleep Apnea (OSA) and Central Serous Chorioretinopathy (CSC): A Literature Overview. J. Clin. Med. 2021, 10, 1521. https://doi.org/10.3390/jcm10071521
Scarinci F, Patacchioli FR, Parravano M. Exploring the Biopsychosocial Pathways Shared by Obstructive Sleep Apnea (OSA) and Central Serous Chorioretinopathy (CSC): A Literature Overview. Journal of Clinical Medicine. 2021; 10(7):1521. https://doi.org/10.3390/jcm10071521
Chicago/Turabian StyleScarinci, Fabio, Francesca Romana Patacchioli, and Mariacristina Parravano. 2021. "Exploring the Biopsychosocial Pathways Shared by Obstructive Sleep Apnea (OSA) and Central Serous Chorioretinopathy (CSC): A Literature Overview" Journal of Clinical Medicine 10, no. 7: 1521. https://doi.org/10.3390/jcm10071521