
The Effects of Silver-Releasing Foam Dressings on Diabetic Foot Ulcer Healing

 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Assessments and Procedures
2.3. Treatment and Follow-Up Evaluation
2.4. Statistical Analysis
3. Results
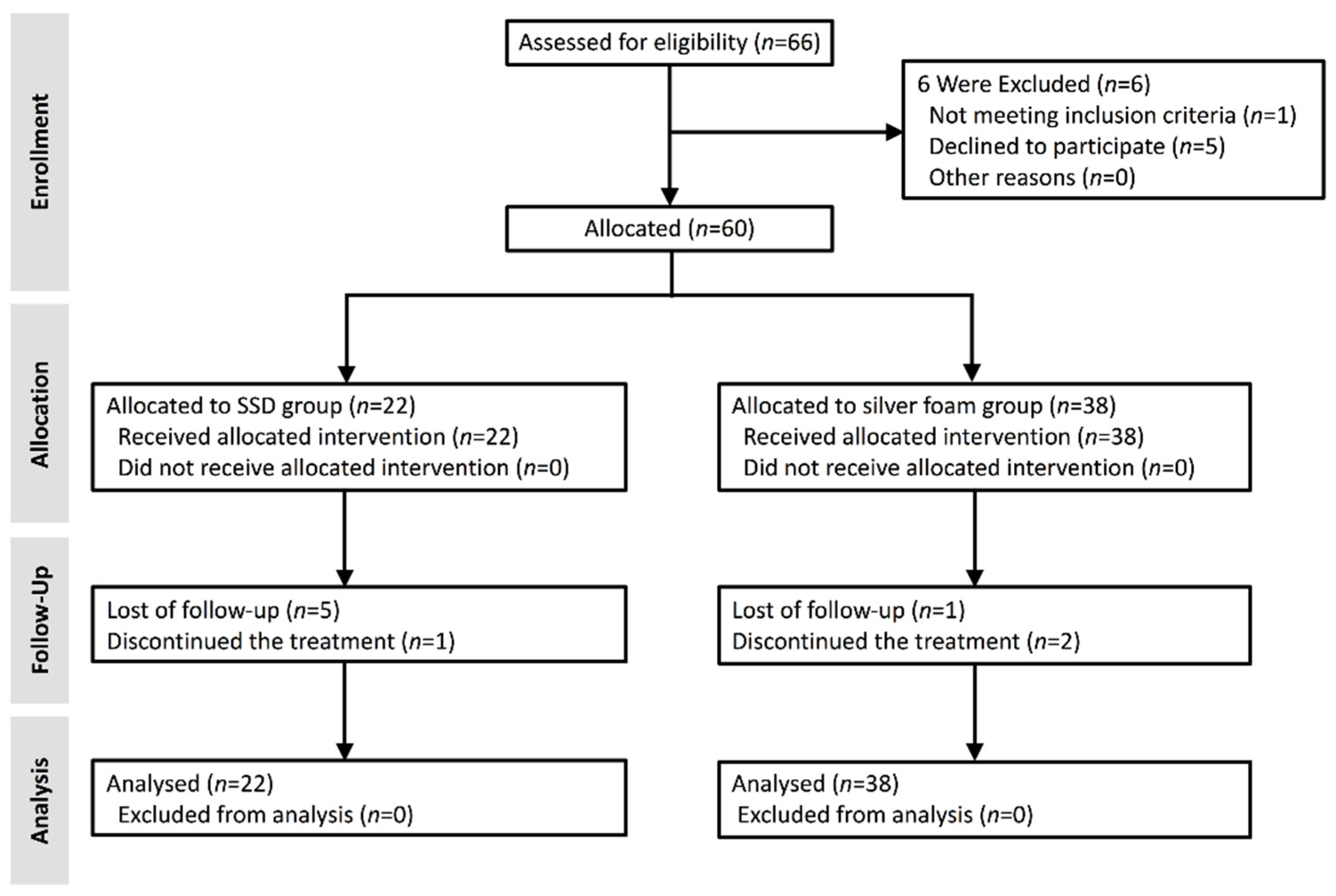
3.1. Trial Population
3.2. General Characteristics of the Participants
3.3. Wound Healing Efficacy Assessment
3.4. Factors Associated with Wound Healing
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zhang, P.; Lu, J.; Jing, Y.; Tang, S.; Zhu, D.; Bi, Y. Global epidemiology of diabetic foot ulceration: A systematic review and meta-analysis. Ann. Med. 2017, 49, 106–116. [Google Scholar] [CrossRef] [PubMed]
- Hobizal, K.B.; Wukich, D.K. Diabetic foot infections: Current concept review. Diabet. Foot Ankle 2012, 3. [Google Scholar] [CrossRef] [PubMed]
- Pecoraro, R.E.; Reiber, G.E.; Burgess, E.M. Pathways to diabetic limb amputation. Basis for prevention. Diabetes Care 1990, 13, 513–521. [Google Scholar] [CrossRef] [PubMed]
- Lipsky, B.A.; Aragon-Sanchez, J.; Diggle, M.; Embil, J.; Kono, S.; Lavery, L.; Senneville, E.; Urbancic-Rovan, V.; Van Asten, S.; Peters, E.J. IWGDF guidance on the diagnosis and management of foot infections in persons with diabetes. Diabetes/Metab. Res. Rev. 2016, 32 (Suppl. 1), 45–74. [Google Scholar] [CrossRef] [Green Version]
- Armstrong, D.G.; Boulton, A.J.M.; Bus, S.A. Diabetic Foot Ulcers and Their Recurrence. N. Engl. J. Med. 2017, 376, 2367–2375. [Google Scholar] [CrossRef]
- Peters, E.J.; Lipsky, B.A.; Aragon-Sanchez, J.; Boyko, E.J.; Diggle, M.; Embil, J.M.; Kono, S.; Lavery, L.A.; Senneville, E.; Urbancic-Rovan, V.; et al. Interventions in the management of infection in the foot in diabetes: A systematic review. Diabetes/Metab. Res. Rev. 2016, 32 (Suppl. 1), 145–153. [Google Scholar] [CrossRef]
- Wu, L.; Norman, G.; Dumville, J.C.; O’Meara, S.; Bell-Syer, S.E. Dressings for treating foot ulcers in people with diabetes: An overview of systematic reviews. Cochrane Database Syst. Rev. 2015, 7, Cd010471. [Google Scholar] [CrossRef] [Green Version]
- Leaper, D.J. Silver dressings: Their role in wound management. Int. Wound J. 2006, 3, 282–294. [Google Scholar] [CrossRef]
- Lansdown, A.B. Silver. I: Its antibacterial properties and mechanism of action. J. Wound Care 2002, 11, 125–130. [Google Scholar] [CrossRef]
- Carter, M.J.; Tingley-Kelley, K.; Warriner, R.A. Silver treatments and silver-impregnated dressings for the healing of leg wounds and ulcers: A systematic review and meta-analysis. J. Am. Acad. Dermatol. 2010, 63, 668–679. [Google Scholar] [CrossRef]
- Vermeulen, H.; van Hattem, J.M.; Storm-Versloot, M.N.; Ubbink, D.T. Topical silver for treating infected wounds. Cochrane Database Syst. Rev. 2007, 1, Cd005486. [Google Scholar] [CrossRef] [PubMed]
- Gilman, T. Wound outcomes: The utility of surface measures. Int. J. Low. Extrem. Wounds 2004, 3, 125–132. [Google Scholar] [CrossRef]
- Leaper, D.; Munter, C.; Meaume, S.; Scalise, A.; Mompo, N.B.; Jakobsen, B.P.; Gottrup, F. The use of biatain Ag in hard-to-heal venous leg ulcers: Meta-analysis of randomised controlled trials. PLoS ONE 2013, 8, e67083. [Google Scholar] [CrossRef] [Green Version]
- Jude, E.B.; Apelqvist, J.; Spraul, M.; Martini, J. Prospective randomized controlled study of Hydrofiber dressing containing ionic silver or calcium alginate dressings in non-ischaemic diabetic foot ulcers. Diabet. Med. J. Br. Diabet. Assoc. 2007, 24, 280–288. [Google Scholar] [CrossRef]
- Jorgensen, B.; Price, P.; Andersen, K.E.; Gottrup, F.; Bech-Thomsen, N.; Scanlon, E.; Kirsner, R.; Rheinen, H.; Roed-Petersen, J.; Romanelli, M.; et al. The silver-releasing foam dressing, Contreet Foam, promotes faster healing of critically colonised venous leg ulcers: A randomised, controlled trial. Int. Wound J. 2005, 2, 64–73. [Google Scholar] [CrossRef]
- Senet, P.; Bause, R.; Jorgensen, B.; Fogh, K. Clinical efficacy of a silver-releasing foam dressing in venous leg ulcer healing: A randomised controlled trial. Int. Wound J. 2014, 11, 649–655. [Google Scholar] [CrossRef]
- Warriner, R.; Burrell, R. Infection and the chronic wound: A focus on silver. Adv. Ski. Wound Care 2005, 18 (Suppl. 1), 2–12. [Google Scholar] [CrossRef]
- Lázaro-Martínez, J.L.; Álvaro-Afonso, F.J.; Sevillano-Fernánde, D.; Molines-Barroso, R.J.; García-Álvarez, Y.; García-Morales, E. Clinical and Antimicrobial Efficacy of a Silver Foam Dressing with Silicone Adhesive in Diabetic Foot Ulcers with Mild Infection. Int. J. Low. Extrem. Wounds 2019, 18, 269–278. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Munter, K.C.; Beele, H.; Russell, L.; Crespi, A.; Grochenig, E.; Basse, P.; Alikadic, N.; Fraulin, F.; Dahl, C.; Jemma, A.P. Effect of a sustained silver-releasing dressing on ulcers with delayed healing: The CONTOP study. J. Wound Care 2006, 15, 199–206. [Google Scholar] [CrossRef] [PubMed]
- Burd, A.; Kwok, C.H.; Hung, S.C.; Chan, H.S.; Gu, H.; Lam, W.K.; Huang, L. A comparative study of the cytotoxicity of silver-based dressings in monolayer cell, tissue explant, and animal models. Wound Repair Regen. Off. Publ. Wound Heal. Soc. Eur. Tissue Repair Soc. 2007, 15, 94–104. [Google Scholar] [CrossRef]
- Prompers, L.; Huijberts, M.; Apelqvist, J.; Jude, E.; Piaggesi, A.; Bakker, K.; Edmonds, M.; Holstein, P.; Jirkovska, A.; Mauricio, D.; et al. High prevalence of ischaemia, infection and serious comorbidity in patients with diabetic foot disease in Europe. Baseline results from the Eurodiale study. Diabetologia 2007, 50, 18–25. [Google Scholar] [CrossRef] [Green Version]
- Lawrence, J.R.; Swerhone, G.D.; Kuhlicke, U.; Neu, T.R. In situ evidence for microdomains in the polymer matrix of bacterial microcolonies. Can. J. Microbiol. 2007, 53, 450–458. [Google Scholar] [CrossRef] [PubMed]
- Singh, V.A.; Barbul, A. Bacterial biofilms in wounds. Wound Repair Regen. 2008, 16, 1. [Google Scholar] [CrossRef] [PubMed]
- Flemming, H.C.; Neu, T.R.; Wozniak, D.J. The EPS matrix: The “house of biofilm cells”. J. Bacteriol. 2007, 189, 7945–7947. [Google Scholar] [CrossRef] [Green Version]
- Bowler, P.G.; Jones, S.A.; Walker, M.; Parsons, D. Microbicidal properties of a silver-containing hydrofiber dressing against a variety of burn wound pathogens. J. Burn Care Rehabil. 2004, 25, 192–196. [Google Scholar] [CrossRef] [PubMed]
- Lo, S.F.; Hayter, M.; Chang, C.J.; Hu, W.Y.; Lee, L.L. A systematic review of silver-releasing dressings in the management of infected chronic wounds. J. Clin. Nurs. 2008, 17, 1973–1985. [Google Scholar] [CrossRef]
- Chaw, K.C.; Manimaran, M.; Tay, F.E. Role of silver ions in destabilization of intermolecular adhesion forces measured by atomic force microscopy in Staphylococcus epidermidis biofilms. Antimicrob. Agents Chemother. 2005, 49, 4853–4859. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dang, C.N.; Prasad, Y.D.; Boulton, A.J.; Jude, E.B. Methicillin-resistant Staphylococcus aureus in the diabetic foot clinic: A worsening problem. Diabet. Med. J. Br. Diabet. Assoc. 2003, 20, 159–161. [Google Scholar] [CrossRef]
- Loots, M.A.; Lamme, E.N.; Zeegelaar, J.; Mekkes, J.R.; Bos, J.D.; Middelkoop, E. Differences in cellular infiltrate and extracellular matrix of chronic diabetic and venous ulcers versus acute wounds. J. Investig. Dermatol. 1998, 111, 850–857. [Google Scholar] [CrossRef] [Green Version]
- Jude, E.B.; Boulton, A.J.; Ferguson, M.W.; Appleton, I. The role of nitric oxide synthase isoforms and arginase in the pathogenesis of diabetic foot ulcers: Possible modulatory effects by transforming growth factor beta 1. Diabetologia 1999, 42, 748–757. [Google Scholar] [CrossRef] [Green Version]
- Dinh, T.; Tecilazich, F.; Kafanas, A.; Doupis, J.; Gnardellis, C.; Leal, E.; Tellechea, A.; Pradhan, L.; Lyons, T.E.; Giurini, J.M.; et al. Mechanisms involved in the development and healing of diabetic foot ulceration. Diabetes 2012, 61, 2937–2947. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schaper, N.C.; van Netten, J.J.; Apelqvist, J.; Bus, S.A.; Hinchliffe, R.J.; Lipsky, B.A.; IWGDF Editorial Board. Practical Guidelines on the prevention and management of diabetic foot disease (IWGDF 2019 update). Diabetes Metab. Res. Rev. 2020, 36 (Suppl. 1), e3266. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Characteristics | SSD | Silver Foam | p-Value |
|---|---|---|---|
| Gender (n, %) | 0.325 | ||
| Male | 15 (68.18%) | 21 (55.26%) | |
| Female | 7 (31.82%) | 17 (44.74%) | |
| Age (years) | 66 (51–89) | 64 (35–88) | 0.365 |
| ABI, PT | 1.24 (0.72–1.72) | 1.15 (0.78–1.9) | 0.520 |
| ABI, DP | 1.13 (0.74–1.71) | 1.08 (0.7–1.9) | 0.706 |
| SPP (mmHg) | 52.01 (31.9–91.6) | 47.20 (32.1–109.7) | 0.951 |
| HbA1c (%) | 7.4% (5.3–17.7%) | 8.1% (5.4–13.1%) | 0.064 |
| ESRD | 0.093 | ||
| Yes | 8 (36.36%) | 6 (15.79%) | |
| No | 14 (63.63%) | 32 (84.21%) | |
| Previous angioplasty in affected limb (%) | 0.374 | ||
| Yes | 5 (22.72%) | 8 (21.05%) | |
| No | 17 (77.27%) | 30 (78.95%) | |
| Wound area (cm2) | 6.84 (1.44–19.25) | 7.78 (1–30) | 0.917 |
| Wagner classification (n, %) | 0.889 | ||
| Grade 1 | 7 (31.82%) | 14 (36.84%) | |
| Grade 2 | 15 (68.18%) | 24 (63.16%) | |
| Ulcer location (n, %) | 0.734 | ||
| Non-plantar | 10 (45.45%) | 19 (50.00%) | |
| Plantar | 12 (54.54%) | 19 (50.00%) | |
| Microbial isolate (n, %) | N/A | ||
| Enterococcus faecalis | 5 (41.67%) | 4 (26.67%) | |
| Staphylococcus aureus | 3 (25.00%) | 4 (26.67%) | |
| Proteus mirabilis | 1 (8.33%) | 3 (20.00%) | |
| Pseudomonas aeruginosa | 1 (8.33%) | 2 (13.33%) | |
| Escherichia coli | 1 (8.33%) | 1 (6.67%) | |
| Klebsiella pneumoniae | 1 (8.33%) | 1 (6.67%) |
| Proportion of Wound Healed (%) | SSD | Silver Foam | p-Value |
|---|---|---|---|
| Weekly | |||
| Week 0–1 | 7.58 ± 1.00 | 31.24 ± 3.8 | * 0.002 |
| Week 1–2 | 21.03 ± 3.00 | 50.41 ± 8.92 | * 0.043 |
| Week 2–3 | 21.31 ± 4.78 | 54.69 ± 6.44 | * 0.048 |
| Week 3–4 | 17.32 ± 4.94 | 24.92 ± 9.12 | 0.590 |
| Total | |||
| Week 0–4 | 27.00 ± 4.95 | 76.43 ±7.41 | * <0.001 |
| Predisposing Factors | Proportion of Wound Healed (%) | p-Value | |
|---|---|---|---|
| SSD | Silver Foam | ||
| Wound area at enrollment | |||
| ≥10 cm2 | 32.70 ± 16.20% | 52.01 ± 6.70% | 0.342 |
| <10 cm2 | 47.95 ± 9.01% | 59.96 ± 9.8% | 0.630 |
| HbA1c | |||
| >7% | 14.21 ± 3.72% | 59.94 ± 8.00% | * 0.027 |
| ≤7% | 47.75 ± 6.56% | 55.86 ± 8.50% | 0.763 |
| ESRD | |||
| Yes | 13.57 ± 5.37% | 47.05 ± 5.23% | 0.121 |
| No | 61.47 ± 7.91% | 61.09 ± 6.14% | 0.491 |
| Wound culture | |||
| Positive | 37.50 ± 5.89% | 60.87 ± 4.06% | * 0.020 |
| Negative | 49.02 ± 7.90% | 74.97 ± 5.25% | 0.061 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, Y.-C.; Lee, H.-C.; Chen, C.-L.; Kuo, M.-C.; Ramachandran, S.; Chen, R.-F.; Kuo, Y.-R. The Effects of Silver-Releasing Foam Dressings on Diabetic Foot Ulcer Healing. J. Clin. Med. 2021, 10, 1495. https://doi.org/10.3390/jcm10071495
Wang Y-C, Lee H-C, Chen C-L, Kuo M-C, Ramachandran S, Chen R-F, Kuo Y-R. The Effects of Silver-Releasing Foam Dressings on Diabetic Foot Ulcer Healing. Journal of Clinical Medicine. 2021; 10(7):1495. https://doi.org/10.3390/jcm10071495
Chicago/Turabian StyleWang, Yu-Chi, Hsiao-Chen Lee, Chien-Lin Chen, Ming-Chun Kuo, Savitha Ramachandran, Rong-Fu Chen, and Yur-Ren Kuo. 2021. "The Effects of Silver-Releasing Foam Dressings on Diabetic Foot Ulcer Healing" Journal of Clinical Medicine 10, no. 7: 1495. https://doi.org/10.3390/jcm10071495