
The Effect of Long-Term Low-Dose Atropine on Refractive Progression in Myopic Australian School Children



Abstract
:1. Introduction
2. Experimental Section
2.1. Subjects
2.2. Procedure
2.3. Ocular Measures
2.4. Analyses
3. Results
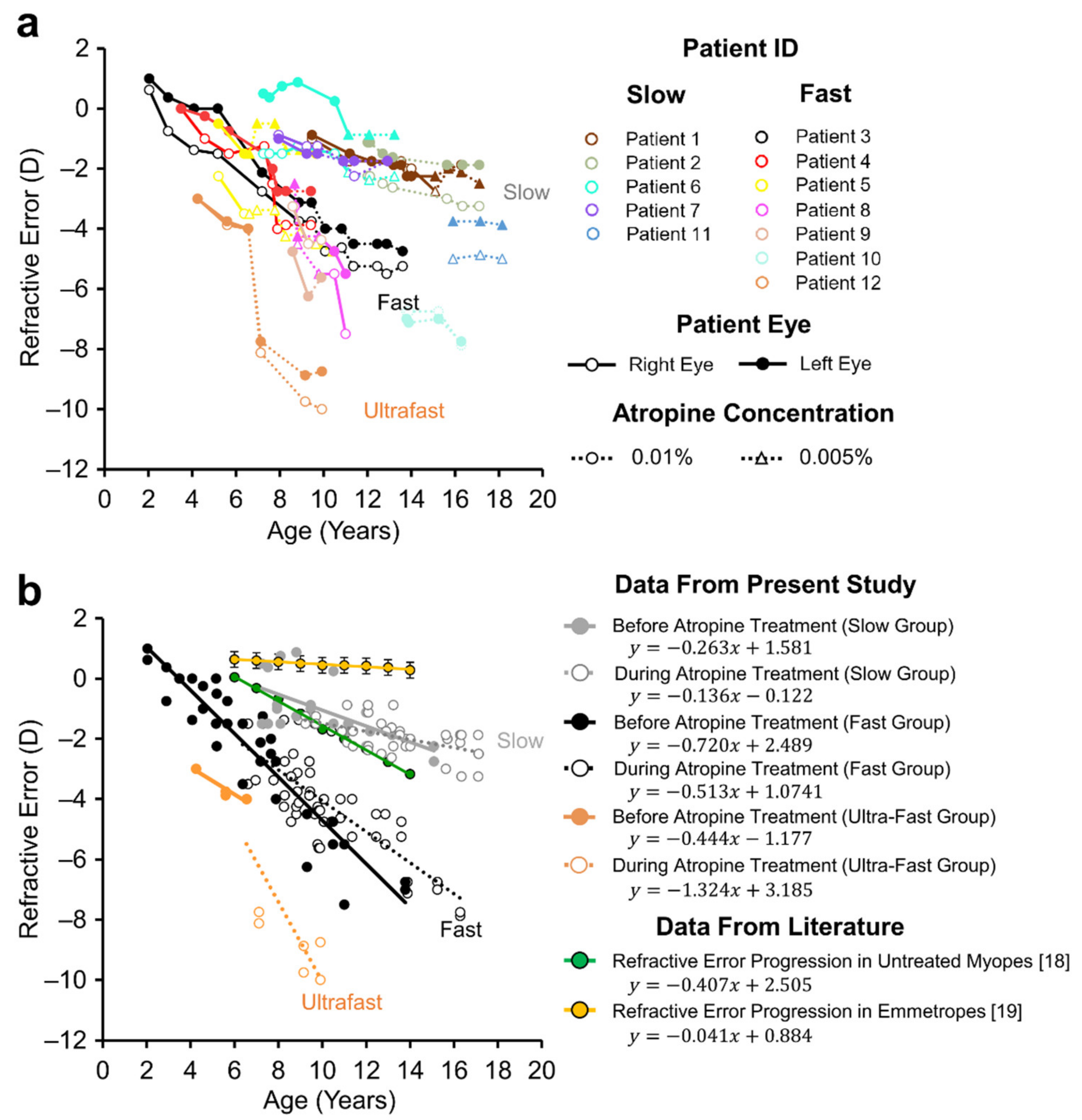
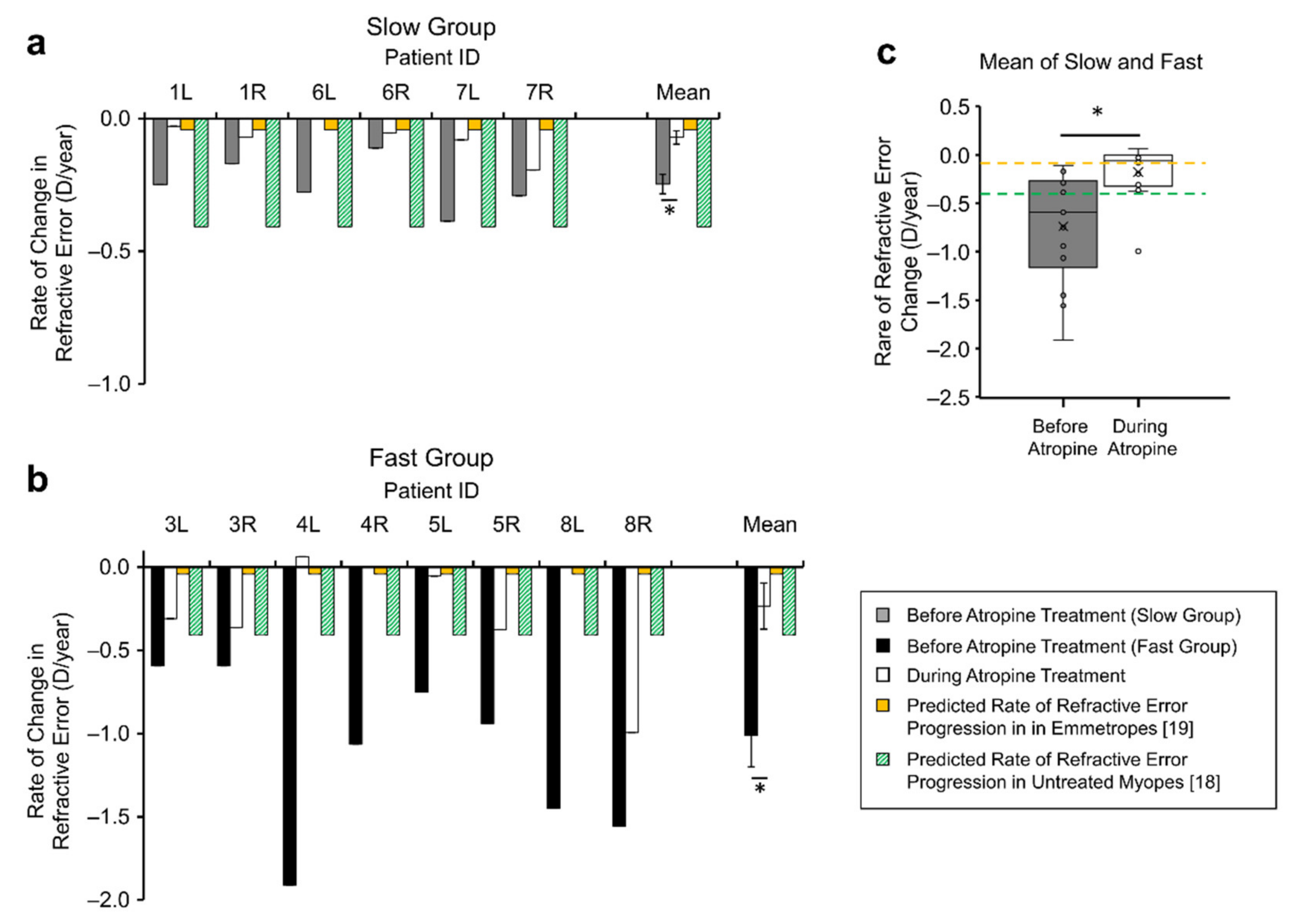
3.1. Daily Low-Dose Atropine Reduced the Progression Rate of Myopia
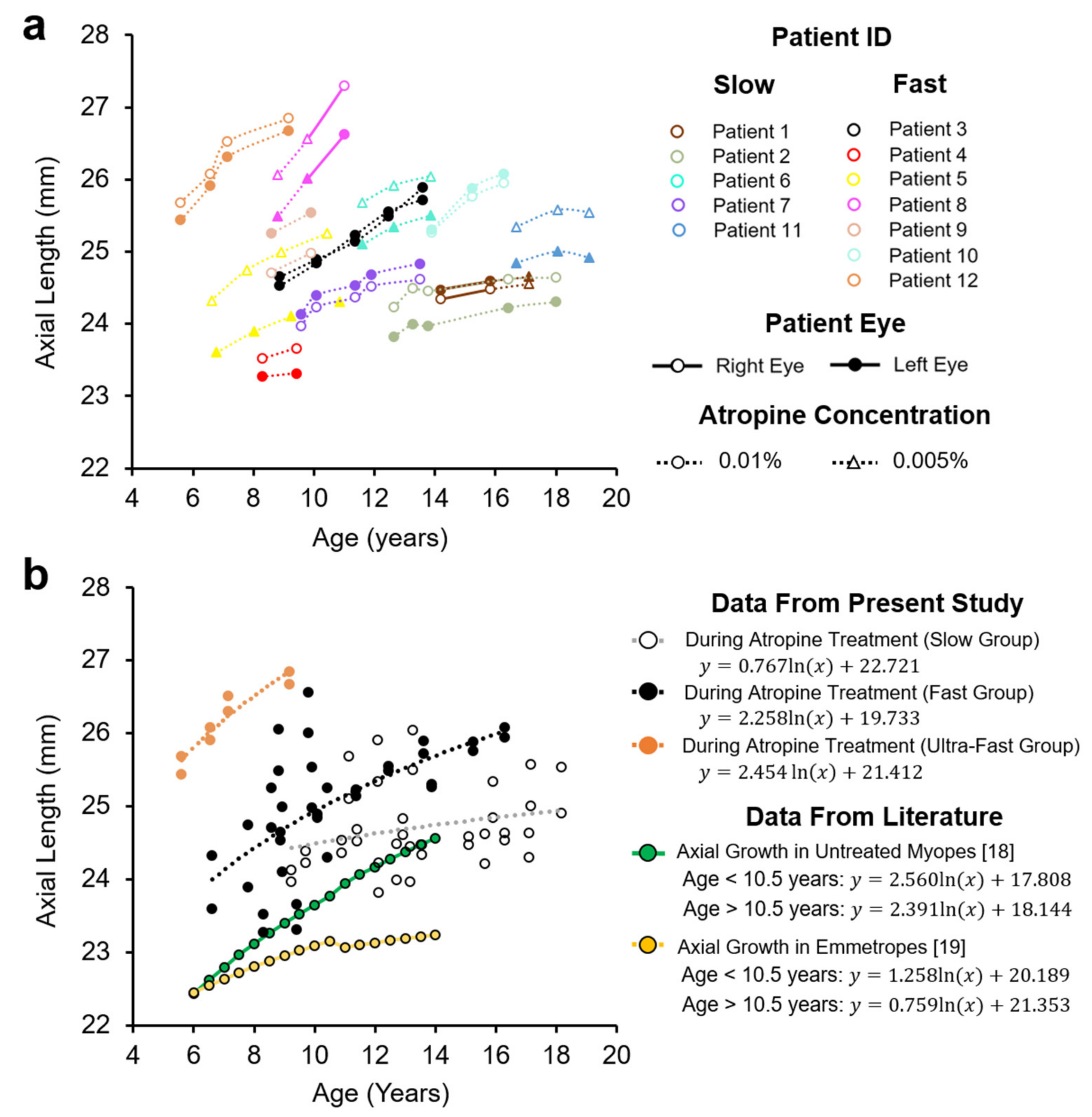
3.2. Axial Length in Myopes during Low- Dose Atropine Treatment
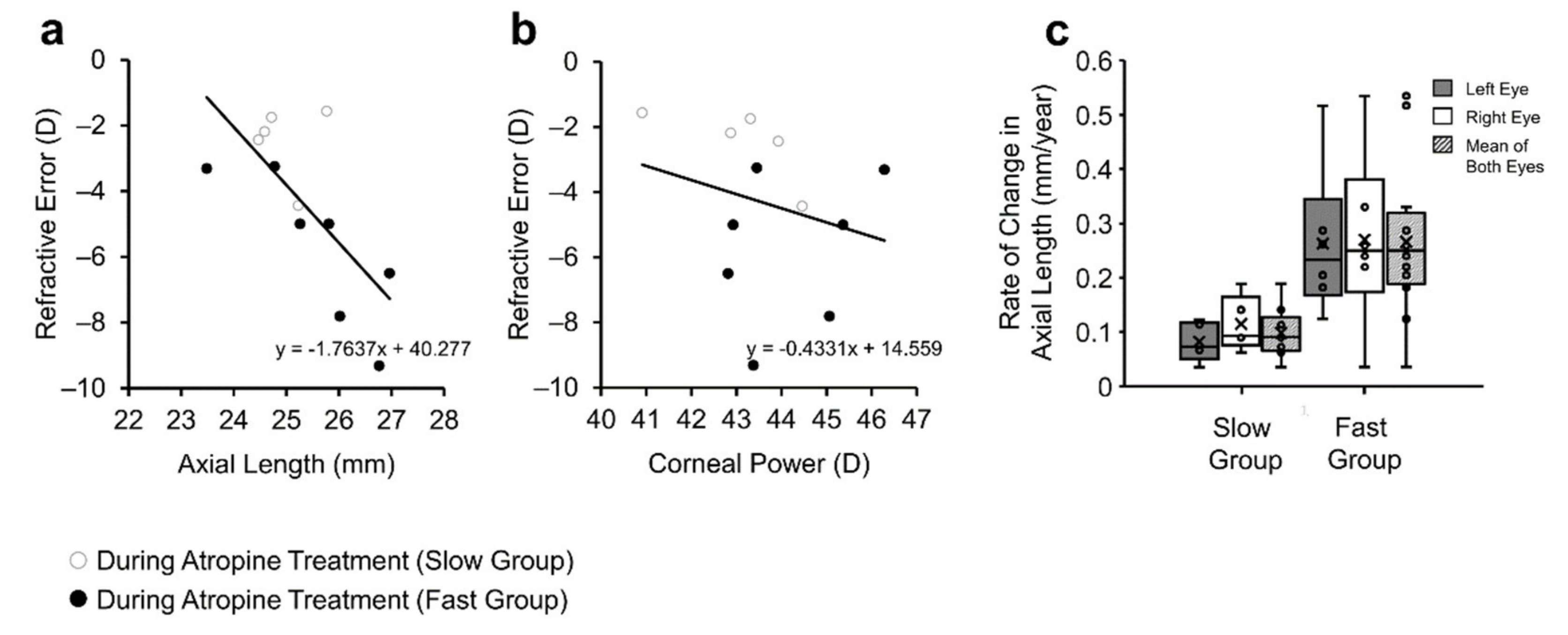
3.3. Axial Length Largely Accounted for Refractive Development
3.4. Adverse Effects of Low-Dose Atropine Treatment
4. Discussion
4.1. Low-Dose Atropine for the Treatment of Myopia
4.2. Effects of Low-Dose Atropine on Axial Length Progression Rates
4.3. Side-Effects of Atropine Treatment
4.4. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Holden, B.A.; Fricke, T.R.; Wilson, D.A.; Jong, M.; Naidoo, K.S.; Sankaridurg, P.; Wong, T.Y.; Naduvilath, T.J.; Resnikoff, S. Global Prevalence of Myopia and High Myopia and Temporal Trends from 2000 through 2050. Ophthalmology 2016, 123, 1036–1042. [Google Scholar] [CrossRef] [Green Version]
- Flitcroft, D.I.; He, M.; Jonas, J.B.; Jong, M.; Naidoo, K.; Ohno-Matsui, K.; Rahi, J.; Resnikoff, S.; Vitale, S.; Yannuzzi, L. IMI—Defining and Classifying Myopia: A Proposed Set of Standards for Clinical and Epidemiologic Studies. Investig. Ophthalmol. Vis. Sci. 2019, 60, M20–M30. [Google Scholar] [CrossRef] [Green Version]
- Xiao, O.; Guo, X.; Wang, D.; Jong, M.; Lee, P.Y.; Chen, L.; Morgan, I.G.; Sankaridurg, P.; He, M. Distribution and Severity of Myopic Maculopathy Among Highly Myopic EyesMyopic Maculopathy Among Highly Myopic Eyes. Investig. Ophthalmol. Vis. Sci. 2018, 59, 4880–4885. [Google Scholar] [CrossRef] [Green Version]
- Chen, H.; Wen, F.; Li, H.; Zuo, C.; Zhang, X.; Huang, S.; Luo, G. The types and severity of high myopic maculopathy in Chinese patients. Ophthalmic Physiol. Opt. 2012, 32, 60–67. [Google Scholar] [CrossRef]
- Huang, J.; Wen, D.; Wang, Q.; McAlinden, C.; Flitcroft, I.; Chen, H.; Saw, S.M.; Chen, H.; Bao, F.; Zhao, Y.; et al. Efficacy Comparison of 16 Interventions for Myopia Control in Children: A Network Meta-analysis. Ophthalmology 2016, 123, 697–708. [Google Scholar] [CrossRef] [Green Version]
- Galvis, V.; Tello, A.; Parra, M.M.; Merayo-Lloves, J.; Larrea, J.; Julian Rodriguez, C.; Camacho, P.A. Topical Atropine in the Control of Myopia. Med. Hypothesis Discov. Innov. Ophthalmol. 2016, 5, 78–88. [Google Scholar]
- Chua, W.H.; Balakrishnan, V.; Chan, Y.H.; Tong, L.; Ling, Y.; Quah, B.L.; Tan, D. Atropine for the treatment of childhood myopia. Ophthalmology 2006, 113, 2285–2291. [Google Scholar] [CrossRef]
- Yam, J.C.; Jiang, Y.; Tang, S.M.; Law, A.K.P.; Chan, J.J.; Wong, E.; Ko, S.T.; Young, A.L.; Tham, C.C.; Chen, L.J.; et al. Low-Concentration Atropine for Myopia Progression (LAMP) Study: A Randomized, Double-Blinded, Placebo-Controlled Trial of 0.05%, 0.025%, and 0.01% Atropine Eye Drops in Myopia Control. Ophthalmology 2019, 126, 113–124. [Google Scholar] [CrossRef] [PubMed]
- Chia, A.; Lu, Q.S.; Tan, D. Five-Year Clinical Trial on Atropine for the Treatment of Myopia 2: Myopia Control with Atropine 0.01% Eyedrops. Ophthalmology 2016, 123, 391–399. [Google Scholar] [CrossRef] [PubMed]
- Moon, J.S.; Shin, S.Y. The diluted atropine for inhibition of myopia progression in Korean children. Int. J. Ophthalmol. 2018, 11, 1657–1662. [Google Scholar] [CrossRef] [PubMed]
- Clark, T.Y.; Clark, R.A. Atropine 0.01% Eyedrops Significantly Reduce the Progression of Childhood Myopia. J. Ocul. Pharmacol. Ther. 2015, 31, 541–545. [Google Scholar] [CrossRef] [PubMed]
- Diaz-Llopis, M.; Pinazo-Durán, M.D. Superdiluted atropine at 0.01% reduces progression in children and adolescents. A 5 year study of safety and effectiveness. Archivos de la Sociedad Española de Oftalmología (Engl. Ed.) 2018, 93, 182–185. [Google Scholar] [CrossRef]
- Chia, A.; Chua, W.H.; Cheung, Y.B.; Wong, W.L.; Lingham, A.; Fong, A.; Tan, D. Atropine for the treatment of childhood myopia: Safety and efficacy of 0.5%, 0.1%, and 0.01% doses (Atropine for the Treatment of Myopia 2). Ophthalmology 2012, 119, 347–354. [Google Scholar] [CrossRef] [PubMed]
- Joachimsen, L.; Böhringer, D.; Gross, N.J.; Reich, M.; Stifter, J.; Reinhard, T.; Lagrèze, W.A. A Pilot Study on the Efficacy and Safety of 0.01% Atropine in German Schoolchildren with Progressive Myopia. Ophthalmol. Ther. 2019, 8, 427–433. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sacchi, M.; Serafino, M.; Villani, E.; Tagliabue, E.; Luccarelli, S.; Bonsignore, F.; Nucci, P. Efficacy of atropine 0.01% for the treatment of childhood myopia in European patients. Acta Ophthalmol. 2019, 97, e1136–e1140. [Google Scholar] [CrossRef]
- Salazar, M.; Shimada, K.; Patil, P.N. Iris pigmentation and atropine mydriasis. J. Pharmacol. Exp. Ther. 1976, 197, 79–88. [Google Scholar]
- Flitcroft, D.I. Emmetropisation and the aetiology of refractive errors. Eye 2014, 28, 169–179. [Google Scholar] [CrossRef] [Green Version]
- Jones, L.A.; Mitchell, G.L.; Mutti, D.O.; Hayes, J.R.; Moeschberger, M.L.; Zadnik, K. Comparison of ocular component growth curves among refractive error groups in children. Investig. Ophthalmol Vis. Sci. 2005, 46, 2317–2327. [Google Scholar] [CrossRef] [Green Version]
- Zadnik, K.; Mutti, D.O.; Mitchell, G.L.; Jones, L.A.; Burr, D.; Moeschberger, M.L. Normal eye growth in emmetropic schoolchildren. Optom. Vis. Sci. 2004, 81, 819–828. [Google Scholar] [CrossRef] [Green Version]
- Hu, D.N. Long-Term Treatment of Myopia with Atropine. In Myopia Updates: Proceedings of the 6th International Conference on Myopia, Tokyo; Tokoro, T., Ed.; Springer: Tokyo, Japan, 1998. [Google Scholar]
- Rozema, J.; Dankert, S.; Iribarren, R.; Lanca, C.; Saw, S.-M. Axial Growth and Lens Power Loss at Myopia Onset in Singaporean Children. Investig. Ophthalmol. Vis. Sci. 2019, 60, 3091–3099. [Google Scholar] [CrossRef]
- Mutti, D.O.; Hayes, J.R.; Mitchell, G.L.; Jones, L.A.; Moeschberger, M.L.; Cotter, S.A.; Kleinstein, R.N.; Manny, R.E.; Twelker, J.D.; Zadnik, K. Refractive error, axial length, and relative peripheral refractive error before and after the onset of myopia. Investig. Ophthalmol. Vis. Sci. 2007, 48, 2510–2519. [Google Scholar] [CrossRef]
- Loughman, J.; Flitcroft, D.I. The acceptability and visual impact of 0.01% atropine in a Caucasian population. Br. J. Ophthalmol. 2016, 100, 1525–1529. [Google Scholar] [CrossRef] [Green Version]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | All | Slow | Fast | p-Value | |
|---|---|---|---|---|---|
| Number of Patients | N | 12 | 5 | 7 | |
| Gender M/F | N/total | 6/6 | 2/3 | 4/3 | |
| At least 1 parent with myopia | N/total | 6/12 | 3/5 | 3/7 | |
| Age at Referral (years) | Mean | 7.9 ± 4.2 | 10.5 ± 3.5 | 6.6 ± 4.0 | 0.11 |
| Range | 2.0–15.8 | 7.25–15.8 | 2–13.8 | ||
| Observation time prior to treatment (years) | Mean | 2.0 ± 2.3 | 1.9 ± 2.0 | 2.1 ± 2.7 | 0.89 |
| Range | 0–6.8 | 0–4.1 | 0–6.8 | ||
| Age at Start of treatment (years) | Mean | 10.3 ± 3.0 | 12.4 ± 2.5 | 8.8 ± 2.5 | 0.03 |
| Range | 6.6–15.8 | 8.7–15.8 | 6.6–13.9 | ||
| Observation time during treatment (years) | Mean | 2.8 ± 1.3 | 3.2 ± 1.2 | 2.5 ± 1.4 | 0.28 |
| Range | 1.1–5.0 | 2.1–5.0 | 1.1–4.7 | ||
| Time between visits and measures (months) | Mean | 9.8 ± 6.0 | 10.1 ± 6.4 | 9.6 ± 5.8 | 0.62 |
| Range | 0.7–29.7 | 1.2–29.7 | 0.7–24.4 |
| Group | Eyes (N) | Before Atropine | During Atropine | p Value (Before vs. During) | Emme-Tropia | Untreated Myopia | p Value |
|---|---|---|---|---|---|---|---|
| Slow+ Fast | 22 | −0.16 ± 0.24 | −0.04 | −0.41 | |||
| 7 † | −0.74 ± 0.57 | −0.18 ± 0.28 | 0.03 | −0.04 | −0.41 | 0.31 * 0.02 ** | |
| Slow | 3 † | −0.25 ± 0.10 | −0.07 ± 0.07 | <0.01 | −0.04 | −0.41 | |
| Fast | 4 † | −1.10 ± 0.49 | −0.25 ± 0.35 | <0.01 | −0.04 | −0.41 |
| Group | Eyes (N) | During Atropine | Emmetropia | Untreated Myopia | p Value |
|---|---|---|---|---|---|
| Slow + Fast | 22 | 0.191 ± 0.136 | 0.084 ± 0.045 | 0.220 ± 0.045 | 0.07 * |
| Slow | 10 | 0.098 ± 0.043 | 0.051 ± 0.005 | 0.196 ± 0.041 | <0.01 * <0.01 ** |
| Fast | 12 | 0.265 ± 0.143 | 0.111 ± 0.043 | 0.245 ± 0.037 | 0.75 * 0.01 ** |
| Eye Colour | Patients (n) | Dilated Pupils | Photophobia | Irritation | Headaches | Side- Effects |
|---|---|---|---|---|---|---|
| All | 13 | 6/13 (46%) | 1/13 (8%) | 4/13 (31%) | 1/13 (8%) | 9/13 (69%) |
| Blue | 7 | 5/7 (71%) | 1/7 (14%) | 2/7 (29%) | 0 | 5/7 (83%) |
| Brown | 4 | 0 | 0 | 2/4 (50%) | 1/4 (25%) | 2/4 (50%) |
| Hazel | 2 | 1/2 (50%) | 0 | 0 | 0 | 1/2 (50%) |
| Fisher’s Exact Test p-value | 13 | 0.043 | 0.296 | 0.391 |
| Study | Geographic Location | Age Range (years) | Study Duration (years) | Atropine Dose (%) | N (Final) | Inclusion Criteria | RE Rate Change (0.01%) |
|---|---|---|---|---|---|---|---|
| Dan-Ning Hu, 1998 [20] | China | 9–18 | 1 | 1, 0.1, 0.01 | 536 | −0.5 D < S.E < −3.0 D | 26% |
| Chia et al., 2016 [9] | Singapore | 6–12 | 5 | 0.5, 0.1, 0.01 | 345 | S.E ≤ −2.0 D each eye | 38% |
| Clark and Clark, 2015 [11] | USA | 6–15 | 1.1 ± 0.3 | 0.01, control | 60 | −0.25 D < S.E < −8.0D Astigmatism < −2.0 D | 75% |
| Diaz-Llopia and Pinazo-Durán, 2018 [12] | Spain | 9–12 | 5 | 0.01, control | 200 | −0.5 D < S.E < −2.0 D Astigmatism < −1.5 D | 77% |
| Yam et al., 2018 [8] | Hong-Kong | 4–12 | 1 | 0.05, 0.025, 0.01, placebo | 383 | S.E < −1.0 D Astigmatism < −2.5 D | 27% |
| Moon and Shin, 2018 [10] | Korea | 5–15 | 1 | 0.05, 0.025, 0.01 | 285 | S.E > −6.0 D Astigmatism < −1.5 D | 48% |
| Joachimsen et al., 2019 [14] | Germany | 6–17 | 1 | 0.01 | 56 | ΔS.E > 0.5 D/year | 62% |
| Sacchi et al., 2019 [15] | Italy | 5–16 | 1 | 0.01 | 102 | ΔS.E > 0.5 D/year | 55% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Myles, W.; Dunlop, C.; McFadden, S.A. The Effect of Long-Term Low-Dose Atropine on Refractive Progression in Myopic Australian School Children. J. Clin. Med. 2021, 10, 1444. https://doi.org/10.3390/jcm10071444
Myles W, Dunlop C, McFadden SA. The Effect of Long-Term Low-Dose Atropine on Refractive Progression in Myopic Australian School Children. Journal of Clinical Medicine. 2021; 10(7):1444. https://doi.org/10.3390/jcm10071444
Chicago/Turabian StyleMyles, William, Catherine Dunlop, and Sally A. McFadden. 2021. "The Effect of Long-Term Low-Dose Atropine on Refractive Progression in Myopic Australian School Children" Journal of Clinical Medicine 10, no. 7: 1444. https://doi.org/10.3390/jcm10071444