
Longitudinal Changes on Optical Coherence Tomography Angiography in Retinal Vein Occlusion †


Abstract
:1. Background
2. Methods
2.1. Study Population
2.2. Study Procedures
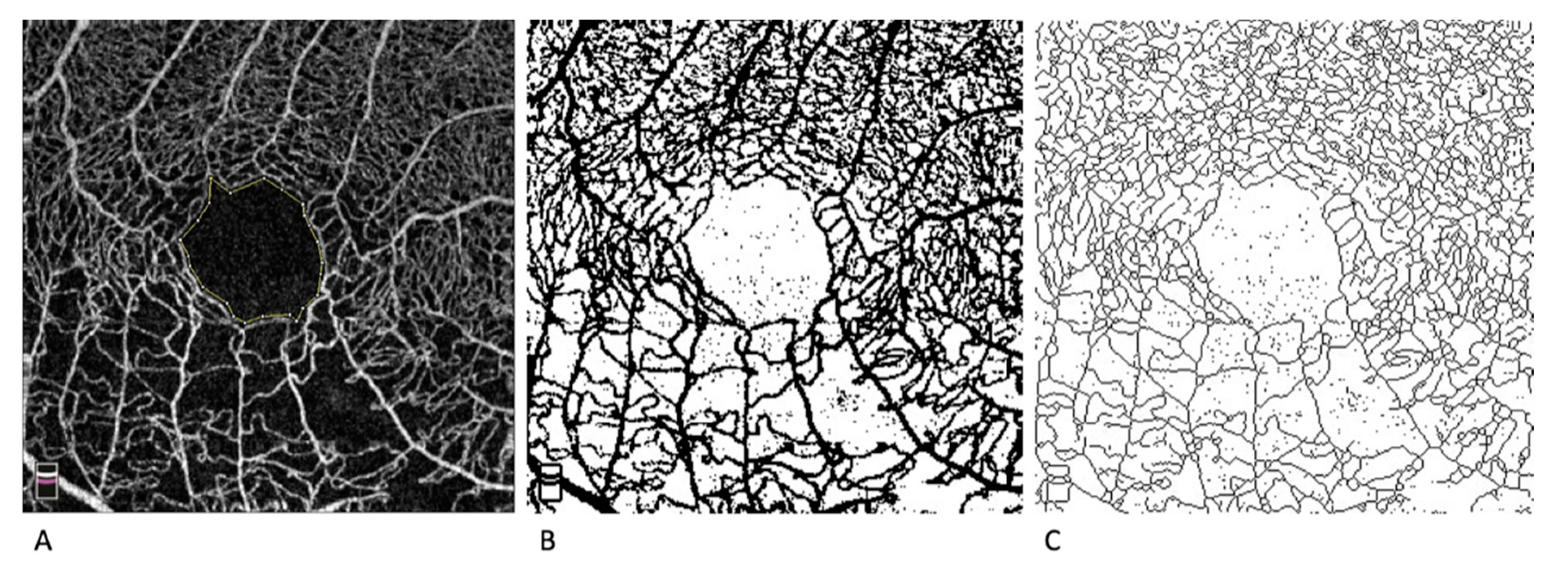
2.3. OCTA Measurements
2.4. Statistical Analysis
3. Results
3.1. OCTA Parameters
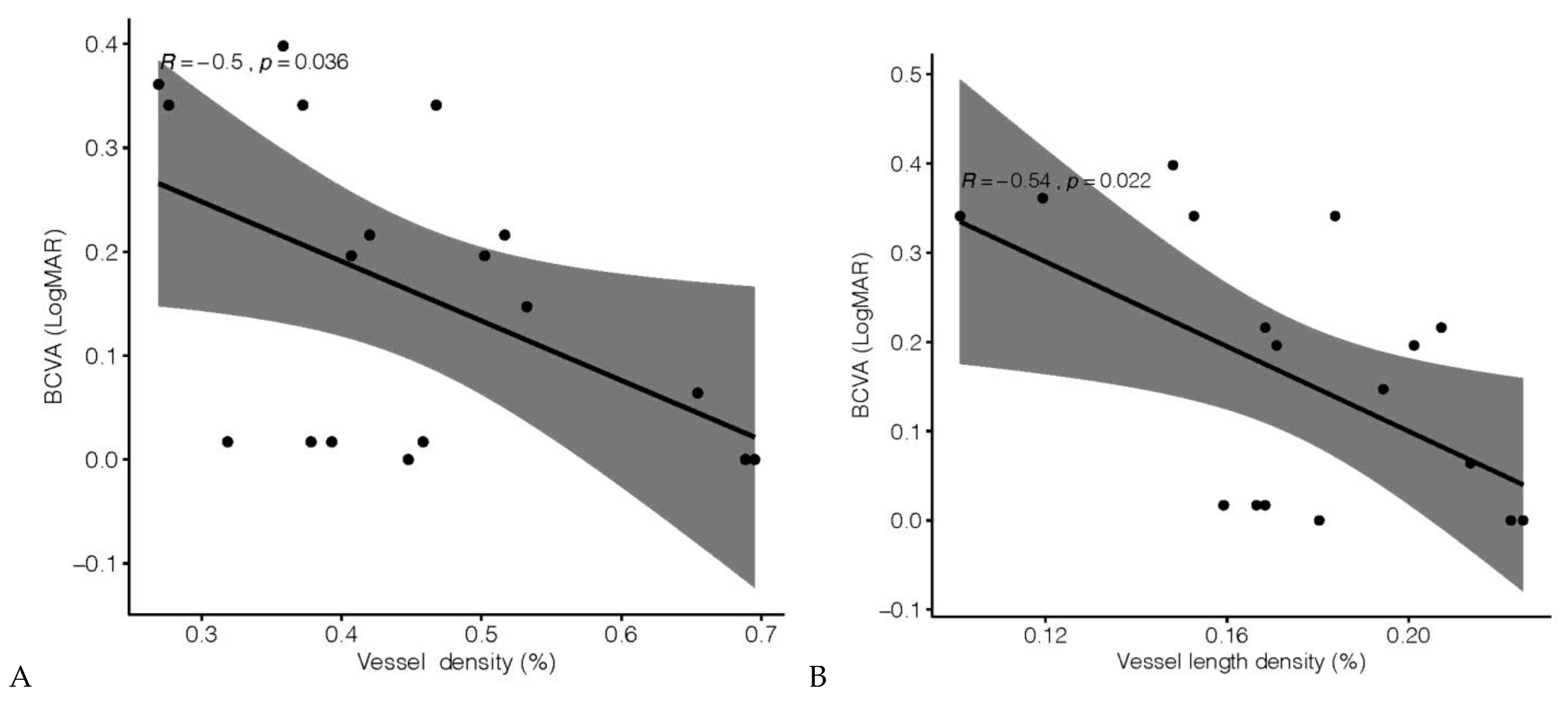
3.2. Visual Acuity and OCTA Parameters
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Ethics Approval and Consent to Participate
References
- Rogers, S.; McIntosh, R.L.; Cheung, N.; Lim, L.; Wang, J.J.; Mitchell, P.; Kowalski, J.W.; Nguyen, H.; Wong, T.Y. The prevalence of retinal vein occlusion: Pooled data from population studies from the United States, Europe, Asia, and Australia. Ophthalmology 2010, 117, 313–319. [Google Scholar] [CrossRef] [Green Version]
- The Central Vein Occlusion Study Group. Natural history and clinical management of central retinal vein occlusion. Arch. Ophthalmol. 1997, 115, 486–491. [Google Scholar] [CrossRef]
- Tsui, I.; Kaines, A.; Havunjian, M.A.; Hubschman, S.; Heilweil, G.; Prasad, P.S.; Oliver, S.C.N.; Yu, F.; Bitrian, E.; Hubschman, J.-P.; et al. Ischemic index and neovascularization in central retinal vein occlusion. Retina 2011, 31, 105–110. [Google Scholar] [CrossRef]
- Brown, D.M.; Campochiaro, P.A.; Singh, R.P.; Li, Z.; Gray, S.; Saroj, N.; Rundle, A.C.; Rubio, R.G.; Murahashi, W.Y. Ranibizumab for macular edema following central retinal vein occlusion: Six-month primary end point results of a phase III study. Ophthalmology 2010, 117, 1124–1133. [Google Scholar] [CrossRef]
- Kinge, B.; Stordahl, P.B.; Forsaa, V.; Fossen, K.; Haugstad, M.; Helgesen, O.H.; Seland, J.; Stene-Johansen, I. Efficacy of ranibizumab in patients with macular edema secondary to central retinal vein occlusion: Results from the sham-controlled ROCC study. Am. J. Ophthalmol. 2010, 150, 310–314. [Google Scholar] [CrossRef]
- Campochiaro, P.A.; Heier, J.S.; Feiner, L.; Gray, S.; Saroj, N.; Rundle, A.C.; Murahashi, W.Y.; Rubio, R.G. Ranibizumab for macular edema following branch retinal vein occlusion: Six-month primary end point results of a phase III study. Ophthalmology 2010, 117, 1102–1112. [Google Scholar] [CrossRef] [PubMed]
- Tan, M.H.; Mcallister, I.L.; Gillies, M.E.; Verma, N.; Banerjee, G.; Smithies, L.A.; Wong, W.-L.; Wong, T.Y. Randomized controlled trial of intravitreal ranibizumab versus standard grid laser for macular edema following branch retinal vein occlusion. Am. J. Ophthalmol. 2014, 157, 237–247. [Google Scholar] [CrossRef] [PubMed]
- De Carlo, T.E.; Romano, A.C.; Waheed, N.K.; Duker, J.S. A review of optical coherence tomography angiography (OCTA). Int. J. Retin. Vitr. 2015, 1, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jia, Y.; Tan, O.; Tokayer, J.; Potsaid, B.M.; Wang, Y.; Liu, J.J.; Kraus, M.F.G.; Subhash, H.; Fujimoto, J.G.; Hornegger, J.; et al. Split-spectrum amplitude-decorrelation angiography with optical coherence tomography. Opt. Express 2012, 20, 4710–4725. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuehlewein, L.; Tepelus, T.C.; An, L.; Durbin, M.K.; Srinivas, S.; Sadda, S.R. Noninvasive Visualization and Analysis of the Human Parafoveal Capillary Network Using Swept Source OCT Optical Microangiography. Investig. Ophthalmol. Vis. Sci. 2015, 56, 3984–3988. [Google Scholar] [CrossRef] [Green Version]
- Salles, M.C.; Kvanta, A.; Amrén, U.; Epstein, D. Optical Coherence Tomography Angiography in Central Retinal Vein Occlusion: Correlation between the Foveal Avascular Zone and Visual Acuity. Investig. Ophthalmol. Vis. Sci. 2016, 57. [Google Scholar] [CrossRef] [Green Version]
- Samara, W.A.; Shahlaee, A.; Sridhar, J.; Khan, M.A.; Ho, A.C.; Hsu, J. Quantitative Optical Coherence Tomography Angiography Features and Visual Function in Eyes With Branch Retinal Vein Occlusion. Am. J. Ophthalmol. 2016, 166, 76–83. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, N.; Hirano, Y.; Yoshida, M.; Tomiyasu, T.; Uemura, A.; Yasukawa, T.; Ogura, Y. Microvascular Abnormalities on Optical Coherence Tomography Angiography in Macular Edema Associated with Branch Retinal Vein Occlusion. Am. J. Ophthalmol. 2016, 161, 126–132. [Google Scholar] [CrossRef] [PubMed]
- Seknazi, D.; Coscas, F.; Sellam, A.; Rouimi, F.; Coscas, G.; Souied, E.H.; Glacet-Bernard, A. Optical Coherence Tomography Angiography in Retinal Vein Occlusion: Correlations between macular vascular density, visual acuity, and peripheral nonperfusion area on fluorescein angiography. Retina 2018, 38, 1562–1570. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Yuan, M.; Sun, L.; Wang, Y.; Chen, Y. Evaluation of microvascular network with optical coherence tomography angiography (OCTA) in branch retinal vein occlusion (BRVO). BMC Ophthalmol. 2020, 20, 154. [Google Scholar] [CrossRef]
- Brar, M.; Sharma, M.; Grewal, S.P.S.; Grewal, D.S. Quantification of retinal microvasculature and neurodegeneration changes in branch retinal vein occlusion after resolution of cystoid macular edema on optical coherence tomography angiography. Indian J. Ophthalmol. 2019, 67, 1864–1869. [Google Scholar] [CrossRef]
- Suzuki, N.; Hirano, Y.; Tomiyasu, T.; Esaki, Y.; Uemura, A.; Yasukawa, T.; Yoshida, M.; Ogura, Y. Retinal Hemodynamics Seen on Optical Coherence Tomography Angiography Before and After Treatment of Retinal Vein Occlusion. Investig. Ophthalmol. Vis. Sci. 2016, 57, 5681–5687. [Google Scholar] [CrossRef] [Green Version]
- Winegarner, A.; Wakabayashi, T.; Fukushima, Y.; Sato, T.; Hara-Ueno, C.; Busch, C.; Nishiyama, I.; Shiraki, N.; Sayanagi, K.; Nishida, K.; et al. Changes in Retinal Microvasculature and Visual Acuity After Antivascular Endothelial Growth Factor Therapy in Retinal Vein Occlusion. Investig. Ophthalmol. Vis. Sci. 2018, 59, 2708–2716. [Google Scholar] [CrossRef]
- Falavarjani, K.G.; Iafe, N.A.; Hubschman, J.-P.; Tsui, I.; Sadda, S.R.; Sarraf, D. Optical Coherence Tomography Angiography Analysis of the Foveal Avascular Zone and Macular Vessel Density After Anti-VEGF Therapy in Eyes with Diabetic Macular Edema and Retinal Vein Occlusion. Investig. Ophthalmol. Vis. Sci. 2017, 58, 30–34. [Google Scholar] [CrossRef]
- Choi, K.-E.; Yun, C.; Cha, J.; Kim, S.-W. OCT angiography features associated with macular edema recurrence after intravitreal bevacizumab treatment in branch retinal vein occlusion. Sci. Rep. 2019, 9, 14153. [Google Scholar] [CrossRef]
- Sophie, R.; Hafiz, G.; Scott, A.W.; Zimmer-Galler, I.; Nguyen, Q.D.; Ying, H.; Do, D.V.; Solomon, S.; Sodhi, A.; Gehlbach, P.; et al. Long-term outcomes in ranibizumab-treated patients with retinal vein occlusion; the role of progression of retinal nonperfusion. Am. J. Ophthalmol. 2013, 156, 693–705. [Google Scholar] [CrossRef] [Green Version]
- Campochiaro, P.A.; Bhisitkul, R.B.; Shapiro, H.; Rubio, R.G. Vascular endothelial growth factor promotes progressive retinal nonperfusion in patients with retinal vein occlusion. Ophthalmology 2013, 120, 795–802. [Google Scholar] [CrossRef]
- Terui, T.; Kondo, M.; Sugita, T.; Ito, Y.; Kondo, N.; Ota, I.; Miyake, K.; Terasaki, H. Changes in areas of capillary nonperfusion after intravitreal injection of bevacizumab in eyes with branch retinal vein occlusion. Retina 2011, 31, 1068–1074. [Google Scholar] [CrossRef]
- Nesper, P.L.; Roberts, P.K.; Onishi, A.C.; Chai, H.; Liu, L.; Jampol, L.M.; Fawzi, A.A. Quantifying Microvascular Abnormalities with Increasing Severity of Diabetic Retinopathy Using Optical Coherence Tomography Angiography. Investig. Ophthalmol. Vis. Sci. 2017, 58, BIO307–BIO315. [Google Scholar] [CrossRef]
- Zhang, Y.S.; Zhou, N.; Knoll, B.M.; Samra, S.; Ward, M.R.; Weintraub, S.; Fawzi, A.A. Parafoveal vessel loss and correlation between peripapillary vessel density and cognitive performance in amnestic mild cognitive impairment and early Alzheimer’s Disease on optical coherence tomography angiography. PLoS ONE 2019, 14, e0214685. [Google Scholar] [CrossRef] [PubMed]
- Nesper, P.L.; Lee, H.E.; Fayed, A.E.; Schwartz, G.W.; Yu, F.; Fawzi, A.A. Hemodynamic Response of the Three Macular Capillary Plexuses in Dark Adaptation and Flicker Stimulation Using Optical Coherence Tomography Angiography. Investig. Ophthalmol. Vis. Sci. 2019, 60, 694–703. [Google Scholar] [CrossRef] [Green Version]
- Onishi, A.C.; Nesper, P.L.; Roberts, P.K.; Moharram, G.A.; Chai, H.; Liu, L.; Jampol, L.M.; Fawzi, A.A. Importance of Considering the Middle Capillary Plexus on OCT Angiography in Diabetic Retinopathy. Investig. Ophthalmol. Vis. Sci. 2018, 59, 2167–2176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fawzi, A.A.; Fayed, A.E.; Linsenmeier, R.A.; Gao, J.; Yu, F. Improved Macular Capillary Flow on Optical Coherence Tomography Angiography After Panretinal Photocoagulation for Proliferative Diabetic Retinopathy. Am. J. Ophthalmol. 2019, 206, 217–227. [Google Scholar] [CrossRef]
- Gao, S.S.; Liu, G.; Huang, D.; Jia, Y. Optimization of the split-spectrum amplitude-decorrelation angiography algorithm on a spectral optical coherence tomography system. Opt. Lett. 2015, 40, 2305–2308. [Google Scholar] [CrossRef] [Green Version]
- Schindelin, J.; Arganda-Carreras, I.; Frise, E.; Kaynig, V.; Longair, M.; Pietzsch, T.; Preibisch, S.; Rueden, C.; Saalfeld, S.; Schmid, B.; et al. Fiji: An open-source platform for biological-image analysis. Nat. Methods 2012, 9, 676–682. [Google Scholar] [CrossRef] [Green Version]
- Babiuch, A.S.; Han, M.; Conti, F.F.; Wai, K.; Silva, F.Q.; Singh, R.P. Association of Disorganization of Retinal Inner Layers with Visual Acuity Response to Anti-Vascular Endothelial Growth Factor Therapy for Macular Edema Secondary to Retinal Vein Occlusion. JAMA Ophthalmol. 2019, 137, 38–46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kwan, C.C.; Lee, H.E.; Schwartz, G.; Fawzi, A.A. Acute Hyperglycemia Reverses Neurovascular Coupling During Dark to Light Adaptation in Healthy Subjects on Optical Coherence Tomography Angiography. Investig. Ophthalmol. Vis. Sci. 2020, 61, 38. [Google Scholar] [CrossRef] [PubMed]
- Adhi, M.; Filho, M.A.B.; Louzada, R.N.; Kuehlewein, L.; De Carlo, T.E.; Baumal, C.R.; Witkin, A.J.; Sadda, S.R.; Sarraf, D.; Reichel, E.; et al. Retinal Capillary Network and Foveal Avascular Zone in Eyes with Vein Occlusion and Fellow Eyes Analyzed with Optical Coherence Tomography Angiography. Investig. Ophthalmol. Vis. Sci. 2016, 57. [Google Scholar] [CrossRef]
- Spaide, R.F.; Fujimoto, J.G.; Waheed, N.K. Image Artifacts in Optical Coherence Tomography Angiography. Retina 2015, 35, 2163–2180. [Google Scholar] [CrossRef] [PubMed]
- Balaratnasingam, C.; Inoue, M.; Ahn, S.; McCann, J.; Dhrami-Gavazi, E.; Yannuzzi, L.A.; Freund, K.B. Visual Acuity Is Correlated with the Area of the Foveal Avascular Zone in Diabetic Retinopathy and Retinal Vein Occlusion. Ophthalmology 2016, 123, 2352–2367. [Google Scholar] [CrossRef]
- Bland, J.M.; Altman, D.G. Regression towards the mean. BMJ 1994, 308, 1499. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mastropasqua, R.; Toto, L.; Di Antonio, L.; Borrelli, E.; Senatore, A.; Di Nicola, M.; Di Martino, G.; Ciancaglini, M.; Carpineto, P. Optical coherence tomography angiography microvascular findings in macular edema due to central and branch retinal vein occlusions. Sci. Rep. 2017, 7, 40763. [Google Scholar] [CrossRef]
- Iida, Y.; Muraoka, Y.; Ooto, S.; Suzuma, K.; Murakami, T.; Iida-Miwa, Y.; Ghashut, R.; Tsujikawa, A. Morphologic and Functional Retinal Vessel Changes in Branch Retinal Vein Occlusion: An Optical Coherence Tomography Angiography Study. Am. J. Ophthalmol. 2017, 182, 168–179. [Google Scholar] [CrossRef] [Green Version]
- Fukami, M.; Iwase, T.; Yamamoto, K.; Kaneko, H.; Yasuda, S.; Terasaki, H. Changes in Retinal Microcirculation After Intravitreal Ranibizumab Injection in Eyes with Macular Edema Secondary to Branch Retinal Vein Occlusion. Investig. Ophthalmol. Vis. Sci. 2017, 58, 1246–1255. [Google Scholar] [CrossRef] [Green Version]
- Papadopoulou, D.N.; Mendrinos, E.; Mangioris, G.; Donati, G.; Pournaras, C.J. Intravitreal ranibizumab may induce retinal arteriolar vasoconstriction in patients with neovascular age-related macular degeneration. Ophthalmology 2009, 116, 1755–1761. [Google Scholar] [CrossRef]
- Mir, T.A.; Kherani, S.; Hafiz, G.; Scott, A.W.; Zimmer-Galler, I.; Wenick, A.S.; Solomon, S.; Han, I.; Poon, D.; He, L.; et al. Changes in Retinal Nonperfusion Associated with Suppression of Vascular Endothelial Growth Factor in Retinal Vein Occlusion. Ophthalmology 2016, 123, 625–634. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ciloglu, E.; Dogan, N. Optical coherence tomography angiography findings in patients with branch retinal vein occlusion treated with Anti-VEGF. Arq. Bras. Oftalmol. 2020, 83, 120–126. [Google Scholar] [CrossRef] [PubMed]
- Tsuboi, K.; Kamei, M. Longitudinal vasculature changes in branch retinal vein occlusion with projection-resolved optical coherence tomography angiography. Graefes Arch. Clin. Exp. Ophthalmol. 2019, 257, 1831–1840. [Google Scholar] [CrossRef] [PubMed]
- You, Q.S.; Freeman, W.R.; Weinreb, R.N.; Zangwill, L.; Manalastas, P.I.C.; Saunders, L.J.; Nudleman, E. Reproducibility of Vessel Density Measurement with Optical Coherence Tomography Angiography in Eyes with and without Retinopathy. Retina 2017, 37, 1475–1482. [Google Scholar] [CrossRef] [PubMed]
- Heier, J.S.; Campochiaro, P.A.; Yau, L.; Li, Z.; Saroj, N.; Rubio, R.G.; Lai, P. Ranibizumab for macular edema due to retinal vein occlusions: Long-term follow-up in the HORIZON trial. Ophthalmology 2012, 119, 802–809. [Google Scholar] [CrossRef]
- Tomita, R.; Iwase, T.; Goto, K.; Yamamoto, K.; Ra, E.; Terasaki, H. Correlation between macular vessel density and number of intravitreal anti-VEGF agents for macular edema associated with branch retinal vein occlusion. Sci. Rep. 2019, 9, 16388. [Google Scholar] [CrossRef] [Green Version]
- Nicolai, M.; Franceschi, A.; De Turris, S.; Rosati, A.; Pirani, V.; Mariotti, C. Papillary Vessel Density Changes After Intravitreal Anti-VEGF Injections in Hypertensive Patients with Central Retinal Vein Occlusion: An Angio-OCT Study. J. Clin. Med. 2019, 8, 1636. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Diagnosis (%) | |
| CRVO | 10 (83) |
| BRVO | 2 (17) |
| Gender (%) | |
| Male | 5 (58) |
| Female | 7 (42) |
| Age (median, IQR, years) | 72, 62–80 |
| Hypertension (%) | 9 (75) |
| Diabetes (%) | 3 (25) |
| Duration of RVO (median, IQR, months) | 17, 10–68 |
| Duration of follow-up (median, IQR, months) | 10, 9–13 |
| Anti-VEGF agent injections before inclusion (median, IQR) | 9, 6–16 |
| Anti-VEGF agent injections during follow-up (median, IQR) | 5, 3–8 |
| RVO Eyes | Control Eyes | RVO vs. Control Eyes | ||||
|---|---|---|---|---|---|---|
| Inclusion Visit | Last Follow-Up | Inclusion Visit | Last Follow-Up | p-Value (Inclusion Visit) | p-Value (Last Follow-Up) | |
| BCVA (LogMAR) | 0.23 ± 0.13 | 0.26 ± 0.13 | 0.02 ± 0.02 | 0.04 ± 0.03 | 0.01 * | 0.004 * |
| 0.4 | 0.3 | |||||
| FAZ area (mm2) | 0.41 ± 0.18 | 0.43 ± 0.19 | 0.34 ± 0.15 | 0.33 ± 0.16 | 0.1 | 0.07 |
| 0.04 * | 0.5 | |||||
| VD (%) | 41.4 ± 8.65 | 41.9 ± 7.49 | 57.1 ± 16.9 | 66.5 ± 16.7 | 0.07 | 0.002 * |
| 0.8 | 0.2 | |||||
| VLD (mm−1) | 16.5 ± 3.16 | 16.3 ± 2.91 | 19.5 ± 2.9 | 21.8 ± 1.62 | 0.04 * | <0.001 * |
| 0.8 | 0.06 | |||||
| AFI (%) | 44.9 ± 4.48 | 44.2 ± 5.25 | 44.4 ± 3.2 | 43.6 ± 4.51 | 0.6 | 0.8 |
| 0.6 | 0.6 | |||||
| Inclusion Visit | Last Follow-Up | |||
|---|---|---|---|---|
| OCTA Parameter | Time from RVO | Anti-VEGF Injections Received † | Time from RVO | Anti-VEGF Injections Received †† |
| FAZ area (mm2) | R = 0.54 | R = −0.07 | R = 0.50 | R = −0.12 |
| p = 0.07 | p = 0.8 | p = 0.1 | p = 0.7 | |
| VD (%) | R = −0.07 | R = −0.20 | R = −0.16 | R = 0.06 |
| p = 0.8 | p = 0.5 | p = 0.6 | p = 0.8 | |
| VLD (mm−1) | R = −0.03 | R = −0.12 | R = −0.02 | R = 0.003 |
| p = 0.9 | p = 0.7 | p = 0.9 | p = 0.9 | |
| AFI (%) | R = 0.49 | R = 0.09 | R = 0.63 | R = 0.06 |
| p = 0.1 | p = 0.8 | p = 0.02 * | p = 0.9 | |
| BCVA (LogMAR) | R = −0.53 | R = −0.24 | R = −0.16 | R = −0.13 |
| p = 0.07 | p = 0.4 | p = 0.6 | p = 0.6 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tripathy, S.; Le, H.-G.; Cicinelli, M.V.; Gill, M.K. Longitudinal Changes on Optical Coherence Tomography Angiography in Retinal Vein Occlusion. J. Clin. Med. 2021, 10, 1423. https://doi.org/10.3390/jcm10071423
Tripathy S, Le H-G, Cicinelli MV, Gill MK. Longitudinal Changes on Optical Coherence Tomography Angiography in Retinal Vein Occlusion. Journal of Clinical Medicine. 2021; 10(7):1423. https://doi.org/10.3390/jcm10071423
Chicago/Turabian StyleTripathy, Swetapadma, Hong-Gam Le, Maria Vittoria Cicinelli, and Manjot K. Gill. 2021. "Longitudinal Changes on Optical Coherence Tomography Angiography in Retinal Vein Occlusion" Journal of Clinical Medicine 10, no. 7: 1423. https://doi.org/10.3390/jcm10071423