
Two Decades from the Introduction of Microdissection Testicular Sperm Extraction: How This Surgical Technique Has Improved the Management of NOA


{kind=link}
{kind=link}
Abstract
:1. Introduction
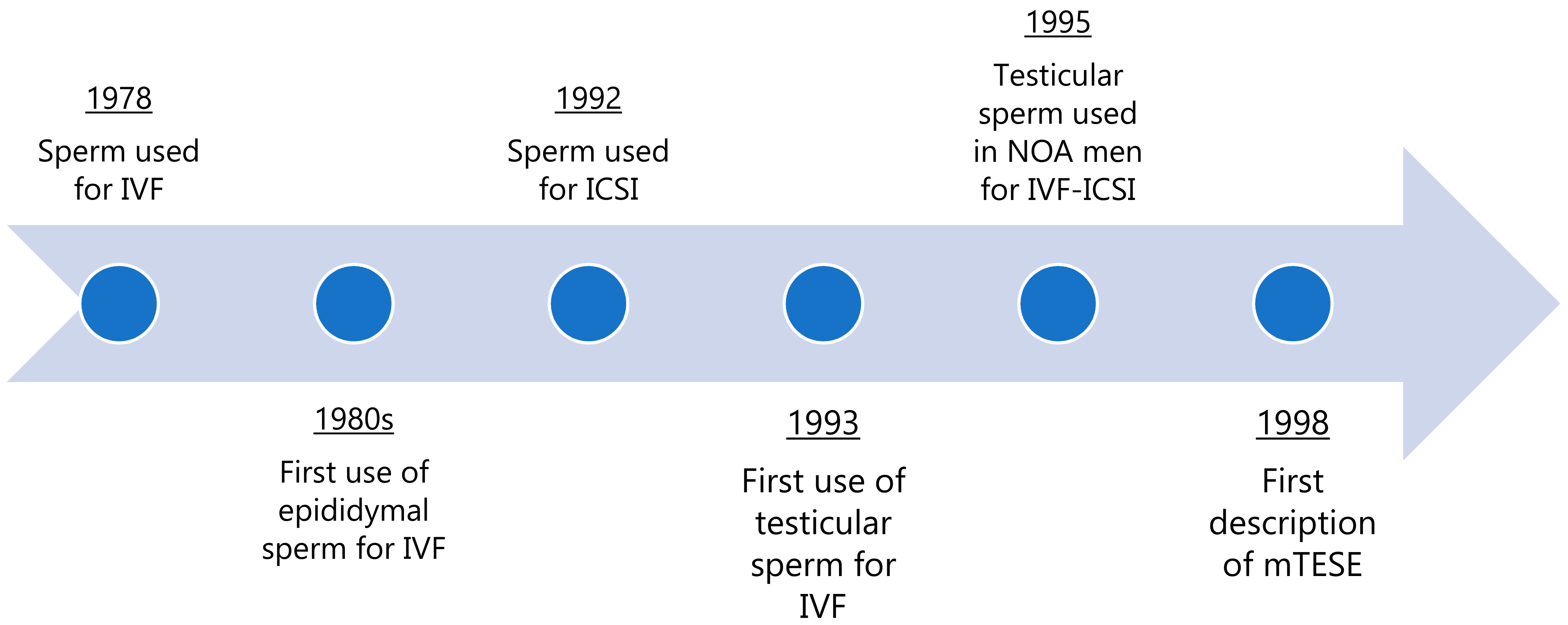
2. History of Surgical Sperm Retrieval
3. Surgical Testicular Sperm Extraction
4. Predictors of Sperm Retrieval in mTESE
4.1. Histopathology
4.2. Testis Size
4.3. Serum Follicle Stimulating Hormone Levels
4.4. Age
4.5. Genetics
4.6. History of Cryptorchidism/Orchiopexy
4.7. Other Factors
5. Outcomes of cTESE vs. mTESE
6. Optimizing Success
7. The Future of Sperm Retrieval in NOA Men
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Agarwal, A.; Mulgund, A.; Hamada, A.; Chyatte, M.R. A unique view on male infertility around the globe. Reprod. Biol. Endocrinol. 2015, 13, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Schlegel, P.N. Causes of azoospermia and their management. Reprod. Fertil. Dev. 2004, 16, 561. [Google Scholar] [CrossRef]
- Kumar, R. Medical management of non-obstructive azoospermia. Clinics 2013, 68, 75–79. [Google Scholar] [CrossRef]
- Esteves, S.C. Clinical management of infertile men with nonobstructive azoospermia. Asian J. Androl. 2015, 17, 459–470. [Google Scholar] [CrossRef]
- Fedder, J.; Crüger, D.; Oestergaard, B.; Petersen, G.B. Etiology of azoospermia in 100 consecutive nonvasectomized men. Fertil. Steril. 2004, 82, 1463–1465. [Google Scholar] [CrossRef]
- Matsumiya, K.; Namiki, M.; Takahara, S.; Kondoh, N.; Takada, S.; Kiyohara, H.; Okuyama, A. Clinical study of azoospermia. Int. J. Androl. 1994, 17, 140–142. [Google Scholar] [CrossRef] [PubMed]
- Das, A.; Halpern, J.A.; Darves-Bornoz, A.L.; Patel, M.; Wren, J.; Keeter, M.K.; Brannigan, R.E. Sperm retrieval success and testicular histopathology in idiopathic nonobstructive azoospermia. Asian J. Androl. 2020, 22, 555–559. [Google Scholar] [CrossRef] [PubMed]
- Krausz, C.; Riera-Escamilla, A.; Moreno-Mendoza, D.; Holleman, K.; Cioppi, F.; Algaba, F.; Pybus, M.; Friedrich, C.; Wyrwoll, M.J.; Casamonti, E.; et al. Genetic dissection of spermatogenic arrest through exome analysis: Clinical implications for the management of azoospermic men. Genet. Med. 2020, 22, 1956–1966. [Google Scholar] [CrossRef] [PubMed]
- Schlegel, P.N. Nonobstructive Azoospermia: A Revolutionary Surgical Approach and Results. Semin. Reprod. Med. 2009, 27, 165–170. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Sauer, M.V. In vitro fertilization (IVF): A review of 3 decades of clinical innovation and technological advancement. Ther. Clin. Risk Manag. 2006, 2, 355–364. [Google Scholar] [CrossRef] [Green Version]
- Temple-Smith, P.D.; Southwick, G.J.; Yates, C.A.; Trounson, A.O.; De Kretser, D.M. Human pregnancy by in vitro fertilization (IVF) using sperm aspirated from the epididymis. J. Assist. Reprod. Genet. 1985, 2, 119–122. [Google Scholar] [CrossRef]
- Palermo, G.; Joris, H.; Devroey, P.; Van Steirteghem, A.C. Pregnancies after intracytoplasmic injection of single spermatozoon into an oocyte. Lancet 1992, 340, 17–18. [Google Scholar] [CrossRef]
- Craft, I.; Bennett, V.; Nicholson, N. Fertilising ability of testicular spermatozoa. Lancet 1993, 342, 864. [Google Scholar] [CrossRef]
- Enatsu, N.; Chiba, K.; Fujisawa, M. The development of surgical sperm extraction and new challenges to improve the outcome. Reprod. Med. Biol. 2015, 15, 137–144. [Google Scholar] [CrossRef] [Green Version]
- Devroey, P.; Liu, J.; Nagy, Z.; Goossens, A.; Tournaye, H.; Camus, M.; Van Steirteghem, A.; Silber, S. Pregnancies after testicular sperm extraction and intracytoplasmic sperm injection in non-obstructive azoospermia. Hum. Reprod. 1995, 10, 1457–1460. [Google Scholar] [CrossRef]
- Schlegel, P.N.; Palermo, G.D.; Goldstein, M.; Menendez, S.; Zaninovic, N.; Veeck, L.L.; Rosenwaks, Z. Testicular sperm ex-traction with intracytoplasmic sperm injection for nonobstructive azoospermia. Urology 1997, 49, 435–440. [Google Scholar] [CrossRef]
- Tash, J.A.; Schlegel, P.N. Histologic effects of testicular sperm extraction on the testicle in men with nonobstructive azoo-spermia. Urology 2001, 57, 334–337. [Google Scholar] [CrossRef]
- Lewin, A.; Weiss, D.B.; Friedler, S.; Ben-Shachar, I.; Porat-Katz, A.; Meirow, D.; Schenker, J.G.; Safran, A. Delivery following intracytoplasmic injection of mature sperm cells recovered by testicular fine needle aspiration in a case of hypergonadotropic azoospermia due to maturation arrest. Hum. Reprod. 1996, 11, 769–771. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schlegel, P.N.; Li, P.S. Microdissection tese: Sperm retrieval in non-obstructive azoospermia. Hum. Reprod. Update 1998, 4, 439. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schlegel, P.N. Testicular sperm extraction: Microdissection improves sperm yield with minimal tissue excision. Hum. Reprod. 1999, 14, 131–135. [Google Scholar] [CrossRef] [PubMed]
- Ramasamy, R.; Yagan, N.; Schlegel, P.N. Structural and functional changes to the testis after conventional versus microdis-section testicular sperm extraction. Urology 2005, 65, 1190–1194. [Google Scholar] [CrossRef] [PubMed]
- Schlegel, P.N.; Sigman, M.; Collura, B.; De Jonge, C.J.; Eisenberg, M.L.; Lamb, D.J.; Mulhall, J.P.; Niederberger, C.; Sandlow, J.I.; Sokol, R.Z.; et al. Diagnosis and treatment of infertility in men: AUA/ASRM guideline part II. Fertil. Steril. 2021, 115, 62–69. [Google Scholar] [CrossRef] [PubMed]
- Tournaye, H.; Verheyen, G.; Nagy, P.; Ubaldi, F.; Goossens, A.; Silber, S.; Van Steirteghem, A.C.; Devroey, P. Are there any predictive factors for successful testicular sperm recovery in azoospermic patients? Hum. Reprod. 1997, 12, 80–86. [Google Scholar] [CrossRef]
- Schlegel, P.N.; Sigman, M.; Collura, B.; De Jonge, C.J.; Eisenberg, M.L.; Lamb, D.J.; Mulhall, J.P.; Niederberger, C.; Sandlow, J.I.; Sokol, R.Z.; et al. Diagnosis and Treatment of Infertility in Men: AUA/ASRM Guideline Part I. J. Urol. 2021, 205, 36–43. [Google Scholar] [CrossRef] [PubMed]
- Seo, J.T.; Ko, W.-J. Predictive factors of successful testicular sperm recovery in non-obstructive azoospermia patients. Int. J. Androl. 2001, 24, 306–310. [Google Scholar] [CrossRef] [PubMed]
- Raheem, A.A.; Garaffa, G.; Rushwan, N.; De Luca, F.; Zacharakis, E.; Raheem, T.A.; Freeman, A.; Serhal, P.; Harper, J.C.; Ralph, D. Testicular histopathology as a predictor of a positive sperm retrieval in men with non-obstructive azoospermia. BJU Int. 2013, 111, 492–499. [Google Scholar] [CrossRef] [Green Version]
- Schoor, R.A.; Elhanbly, S.; Niederberger, C.S.; Ross, L.S. The role of testicular biopsy in the modern management of male in-fertility. J. Urol. 2002, 167, 197–200. [Google Scholar] [CrossRef]
- Corona, G.; Minhas, S.; Giwercman, A.; Bettocchi, C.; Dinkelman-Smit, M.; Dohle, G.; Fusco, F.; Kadioglou, A.; Kliesch, S.; Kopa, Z.; et al. Sperm recovery and icsi outcomes in men with non-obstructive azoospermia: A systematic review and meta-analysis. Hum. Reprod. Update 2019, 25, 733–757. [Google Scholar] [CrossRef]
- Wang, T.; Li, H.; Chen, L.-P.; Yang, J.; Li, M.-C.; Chen, R.-B.; Lan, R.-Z.; Wang, S.-G.; Liu, J.-H. Predictive value of FSH, testicular volume, and histopathological findings for the sperm retrieval rate of microdissection TESE in nonobstructive azoospermia: A meta-analysis. Asian J. Androl. 2018, 20, 30–36. [Google Scholar] [CrossRef]
- Bryson, C.F.; Ramasamy, R.; Sheehan, M.; Palermo, G.D.; Rosenwaks, Z.; Schlegel, P.N. Severe Testicular Atrophy does not Affect the Success of Microdissection Testicular Sperm Extraction. J. Urol. 2014, 191, 175–178. [Google Scholar] [CrossRef] [Green Version]
- Ishikawa, T. Surgical recovery of sperm in non-obstructive azoospermia. Asian J. Androl. 2011, 14, 109–115. [Google Scholar] [CrossRef] [Green Version]
- Silber, S.J.; Van Steirteghem, A.; Nagy, Z.; Liu, J.; Tournaye, H.; Devroey, P. Normal pregnancies resulting from testicular sperm extraction and intracytoplasmic sperm injection for azoospermia due to maturation arrest. Fertil. Steril. 1996, 66, 110–117. [Google Scholar] [CrossRef]
- Ramasamy, R.; Lin, K.; Gosden, L.V.; Rosenwaks, Z.; Palermo, G.D.; Schlegel, P.N. High serum fsh levels in men with nonob-structive azoospermia does not affect success of microdissection testicular sperm extraction. Fertil. Steril. 2009, 92, 590–593. [Google Scholar] [CrossRef]
- Grunewald, S.; Glander, H.-J.; Paasch, U.; Kratzsch, J. Age-dependent inhibin B concentration in relation to FSH and semen sample qualities: A study in 2448 men. Reproduction 2013, 145, 237–244. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, B.; Yang, Q.; Huang, Y.-P.; Wang, H.-X.; Hu, K.; Wang, Y.-X.; Huang, Y.-R. Follicle-stimulating hormone as a predictor for sperm retrieval rate in patients with nonobstructive azoospermia: A systematic review and meta-analysis. Asian J. Androl. 2015, 17, 281–284. [Google Scholar] [CrossRef] [PubMed]
- Bakircioglu, M.E.; Erden, H.F.; Kaplancan, T.; Ciray, N.; Bener, F.; Bahceci, M. Aging may adversely affect testicular sperm recovery in patients with Klinefelter syndrome. Urology 2006, 68, 1082–1086. [Google Scholar] [CrossRef] [PubMed]
- Bernie, A.M.; Ramasamy, R.; Schlegel, P.N. Predictive factors of successful microdissection testicular sperm extraction. Basic Clin. Androl. 2013, 23, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hopps, C.V.; Mielnik, A.; Goldstein, M.; Palermo, G.D.; Rosenwaks, Z.; Schlegel, P.N. Detection of sperm in men with Y chromosome microdeletions of the AZFa, AZFb and AZFc regions. Hum. Reprod. 2003, 18, 1660–1665. [Google Scholar] [CrossRef] [Green Version]
- Stahl, P.J.; Masson, P.; Mielnik, A.; Marean, M.B.; Schlegel, P.N.; Paduch, D.A. A decade of experience emphasizes that testing for Y microdeletions is essential in American men with azoospermia and severe oligozoospermia. Fertil. Steril. 2010, 94, 1753–1756. [Google Scholar] [CrossRef]
- A Fakhro, K.; ElBardisi, H.; Arafa, M.; Robay, A.; Rodriguez-Flores, J.L.; Al-Shakaki, A.; Syed, N.; Mezey, J.G.; Khalil, C.A.; A Malek, J.; et al. Point-of-care whole-exome sequencing of idiopathic male infertility. Genet. Med. 2018, 20, 1365–1373. [Google Scholar] [CrossRef]
- Ramasamy, R.; Bakircioglu, M.E.; Cengiz, C.; Karaca, E.; Scovell, J.; Jhangiani, S.N.; Akdemir, Z.C.; Bainbridge, M.; Yu, Y.; Huff, C.; et al. Whole-exome sequencing identifies novel homozygous mutation in npas2 in family with nonobstructive azoo-spermia. Fertil. Steril. 2015, 104, 286–291. [Google Scholar] [CrossRef] [Green Version]
- Osaka, A.; Iwahata, T.; Kobori, Y.; Shimomura, Y.; Yoshikawa, N.; Onota, S.; Yamamoto, A.; Ide, H.; Sugimoto, K.; Okada, H. Testicular volume in non-obstructive azoospermia with a history of bilateral cryptorchidism may predict successful sperm re-trieval by testicular sperm extraction. Reprod. Med. Biol. 2020, 19, 372–377. [Google Scholar] [CrossRef]
- Ozan, T.; Karakeci, A.; Kaplancan, T.; Pirincci, N.; Firdolas, F.; Orhan, I. Are predictive factors in sperm retrieval and preg-nancy rates present in nonobstructive azoospermia patients by microdissection testicular sperm extraction on testicle with a history of orchidopexy operation? Andrologia 2019, 51, e13430. [Google Scholar] [CrossRef]
- Glina, S.; Vieira, M. Prognostic factors for sperm retrieval in non-obstructive azoospermia. Clinics 2013, 68, 121–124. [Google Scholar] [CrossRef]
- Ramasamy, R.; Padilla, W.O.; Osterberg, E.C.; Srivastava, A.; Reifsnyder, J.E.; Niederberger, C.; Schlegel, P.N. A comparison of models for predicting sperm retrieval before microdissection testicular sperm extraction in men with nonobstructive azoo-spermia. J. Urol. 2013, 189, 638–642. [Google Scholar] [CrossRef]
- Raman, J.D.; Schlegel, P.N. Testicular Sperm Extraction with Intracytoplasmic Sperm Injection is Successful for the Treatment of Nonobstructive Azoospermia Associated with Cryptorchidism. J. Urol. 2003, 170, 1287–1290. [Google Scholar] [CrossRef] [PubMed]
- Bernie, A.M.; Mata, D.A.; Ramasamy, R.; Schlegel, P.N. Comparison of microdissection testicular sperm extraction, conventional testicular sperm extraction, and testicular sperm aspiration for nonobstructive azoospermia: A systematic review and meta-analysis. Fertil. Steril. 2015, 104, 1099–1103.e3. [Google Scholar] [CrossRef]
- Colpi, G.M.; Colpi, E.M.; Piediferro, G.; Giacchetta, D.; Gazzano, G.; Castiglioni, F.M.; Magli, M.C.; Gianaroli, L. Microsurgical TESE versus conventional TESE for ICSI in non-obstructive azoospermia: A randomized controlled study. Reprod. Biomed. Online 2009, 18, 315–319. [Google Scholar] [CrossRef]
- Deruyver, Y.; Vanderschueren, D.; Van Der Aa, F. Outcome of microdissection TESE compared with conventional TESE in non-obstructive azoospermia: A systematic review. Andrology 2014, 2, 20–24. [Google Scholar] [CrossRef] [PubMed]
- Ron-El, R.; Strassburger, D.; Friedler, S.; Komarovski, D.; Bern, O.; Soffer, Y.; Raziel, A. Extended sperm preparation: An al-ternative to testicular sperm extraction in non-obstructive azoospermia. Hum. Reprod. 1997, 12, 1222–1226. [Google Scholar] [CrossRef]
- Practice Committee of the American Society for Reproductive Medicine in Collaboration with the Society for Male Reproduction and Urology. Evaluation of the azoospermic male: A committee opinion. Fertil. Steril. 2018, 109, 777–782. [Google Scholar] [CrossRef] [PubMed]
- Schlegel, P.N. Aromatase inhibitors for male infertility. Fertil. Steril. 2012, 98, 1359–1362. [Google Scholar] [CrossRef] [PubMed]
- Reifsnyder, J.E.; Ramasamy, R.; Husseini, J.; Schlegel, P.N. Role of Optimizing Testosterone Before Microdissection Testicular Sperm Extraction in Men with Nonobstructive Azoospermia. J. Urol. 2012, 188, 532–537. [Google Scholar] [CrossRef] [PubMed]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Punjani, N.; Kang, C.; Schlegel, P.N. Two Decades from the Introduction of Microdissection Testicular Sperm Extraction: How This Surgical Technique Has Improved the Management of NOA. J. Clin. Med. 2021, 10, 1374. https://doi.org/10.3390/jcm10071374
Punjani N, Kang C, Schlegel PN. Two Decades from the Introduction of Microdissection Testicular Sperm Extraction: How This Surgical Technique Has Improved the Management of NOA. Journal of Clinical Medicine. 2021; 10(7):1374. https://doi.org/10.3390/jcm10071374
Chicago/Turabian StylePunjani, Nahid, Caroline Kang, and Peter N. Schlegel. 2021. "Two Decades from the Introduction of Microdissection Testicular Sperm Extraction: How This Surgical Technique Has Improved the Management of NOA" Journal of Clinical Medicine 10, no. 7: 1374. https://doi.org/10.3390/jcm10071374