1. Introduction
Coronaviruses are a member of the Coronaviridae family from the Nidovirales order. The name stems from the presence of crown-like spikes on the surface of the virus, thus called coronavirus. These viruses are tiny (65–125 nm of diameter) and contain a single-stranded RNA as genetic material, with a size that varies from 26 to 32 kilobases (kb) of length. There are four subgroups within the coronavirus family: alpha (α), beta (β), gamma (γ), and delta (δ) [
1]. Several coronaviruses can infect human beings, such as the endemic human coronaviruses that exist worldwide (HCoV-229E, HCoV-NL63, HCoV-HKU1, and HCoVOC43) that tend to cause a mild respiratory disease, in addition to the Middle-East Respiratory Syndrome (MERS-CoV) and the Severe Acute Respiratory Syndrome (SARS-CoV) that present a higher case fatality rate [
2].
COVID-19 is a severe acute respiratory disease caused by the SARS-CoV-2 virus. On 11 March 2020, it was declared as a pandemic by the World Health Organization (WHO) given its high rate of infection, which represents a great threat to global public health. Scientists are still investigating the emergence and origin of SARS-CoV-2. Furthermore, its zoonotic source of transmission in humans has yet to be confirmed. However, the sequence-based analysis has resulted in bats being considered the key reservoir. Recombination of DNA was found to be involved in the spike glycoprotein that combined SARS-CoV (CoVZXC21 or CoVZC45) with the receptor-binding domain (RBD) of another Beta CoV. Hence, this could be the reason for interspecies transmission and rapid infection. Thus, the glycoprotein spikes on the outer surface of coronaviruses are responsible for the binding and entry of the virus into host cells. RBD is loosely bound between viruses, therefore the virus can infect multiple hosts. Other coronaviruses primarily recognize aminopeptidases or carbohydrates as a key receptor for entry into human cells, while SARS-CoV and MERS-CoV recognize exopeptidases [
3,
4].
Some recent studies have shown that this new coronavirus strain can lead to conjunctival findings and can be detected in tears and conjunctival secretions [
5,
6].
SARS-CoV-2 RNA has been detected through a RT-PCR on conjunctival samples in 0% to 15% of infected patients [
7,
8]. However, and although some studies have described the positivity of the virus genome in tear samples from patients with SARS-CoV-2, the relevance of these findings remains controversial [
9]. A total of 40% of patients with a positive conjunctival swab present with symptomatic conjunctivitis. Likewise, the appearance of ocular symptoms is frequently the first symptom, or they can appear along with other systemic pathologies [
10]. The notified manifestations and symptoms are as follows: bilateral/unilateral diffuse hyperemia, viscose white secretion in the conjunctival sac, foreign body sensation in the eye, and excessive tearing [
11,
12].
It must be highlighted that secondary conjunctivitis is the main ocular manifestation in COVID-19 patients and the main viral conjunctivitis is less frequent [
13]. The prevalence rate ranges from 0.8% to 31.6% of patients [
6,
14]. In a retrospective study carried out with 1099 samples from positive COVID-19 patients diagnosed by laboratories of 552 hospitals in 30 Chinese provinces, the conjunctivitis rate was 0.8% [
6]. In another study, it was found that 12 out of 38 COVID-19 patients showed conjunctival hyperemia, chemosis, epiphora, or increased conjunctival secretions. Thus, these manifestations were linked to conjunctivitis. However, only two patients yielded a positive RT-PCR finding in their conjunctival swabs [
14]. At a later stage, it was proved that a higher prevalence of conjunctivitis can be related to incomplete closure of the eyelids in sedated and semi-conscious patients in the intensive care unit [
15].
On the other hand, various studies have shown that epithelial cells from the ocular surface can selectively respond to specific components of ocular pathogenic bacteria by producing pro-inflammatory cytokines. On the contrary, it was shown that they do not respond to non-pathogenic bacteria, which favor colonization by a real microbiota. However, analysis of the composition of the ocular microbiome is essential to understand the pathophysiology of various ophthalmic diseases. Therefore, the alteration of the normal microbiota of the eye may have an important activity as a cofactor in the pathogenesis of ophthalmic diseases. In turn, recently the alteration of the microbiota of other body sites has been considered that it can favor the development of ophthalmic pathologies. In this sense, changes in the composition of the oral and intestinal microbiota have been associated with glaucoma, uveitis, and AMD, respectively. From this method, the analysis of the ocular microbiota is important to improve the knowledge that homeostatic microorganisms have in the prevention of various ophthalmic diseases and thus develop new therapeutic strategies, based above all on the intake of probiotics, to treat ocular pathologies [
16].
As a response to this pandemic, and to reduce the referral of patients to hospitals or health care centers, several studies have analyzed the feasibility and effectiveness of telemedicine in ophthalmology (teleophthalmology). Teleophthalmology has been successfully used in hospitalized patients and outpatient centers, and it has been implemented in a variety of socio-economic contexts. Although most of the successful initiatives so far have been focused on the screening and early detection of ophthalmological diseases, teleophthalmology has also a great potential for patients’ treatment and follow-up [
17,
18].
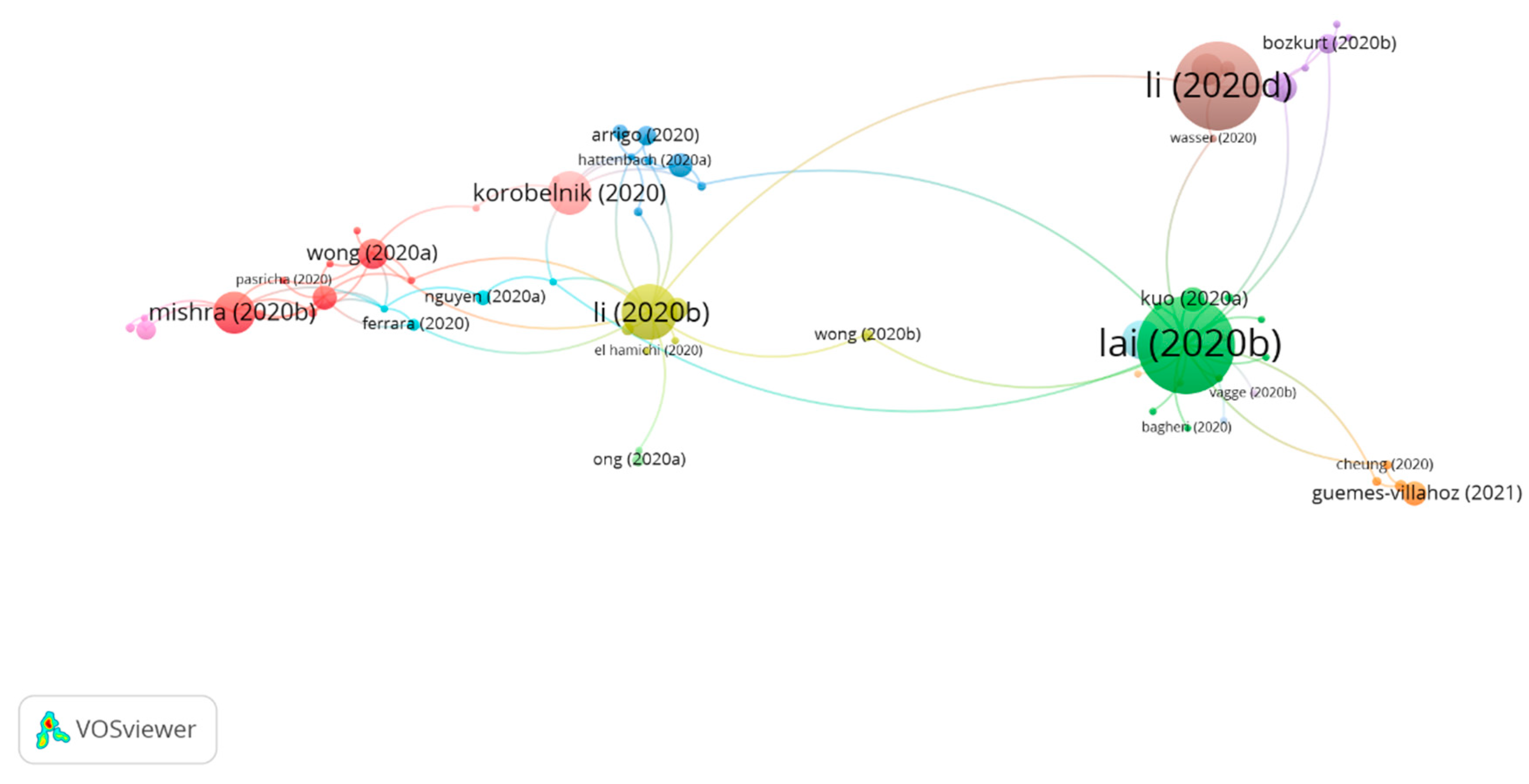
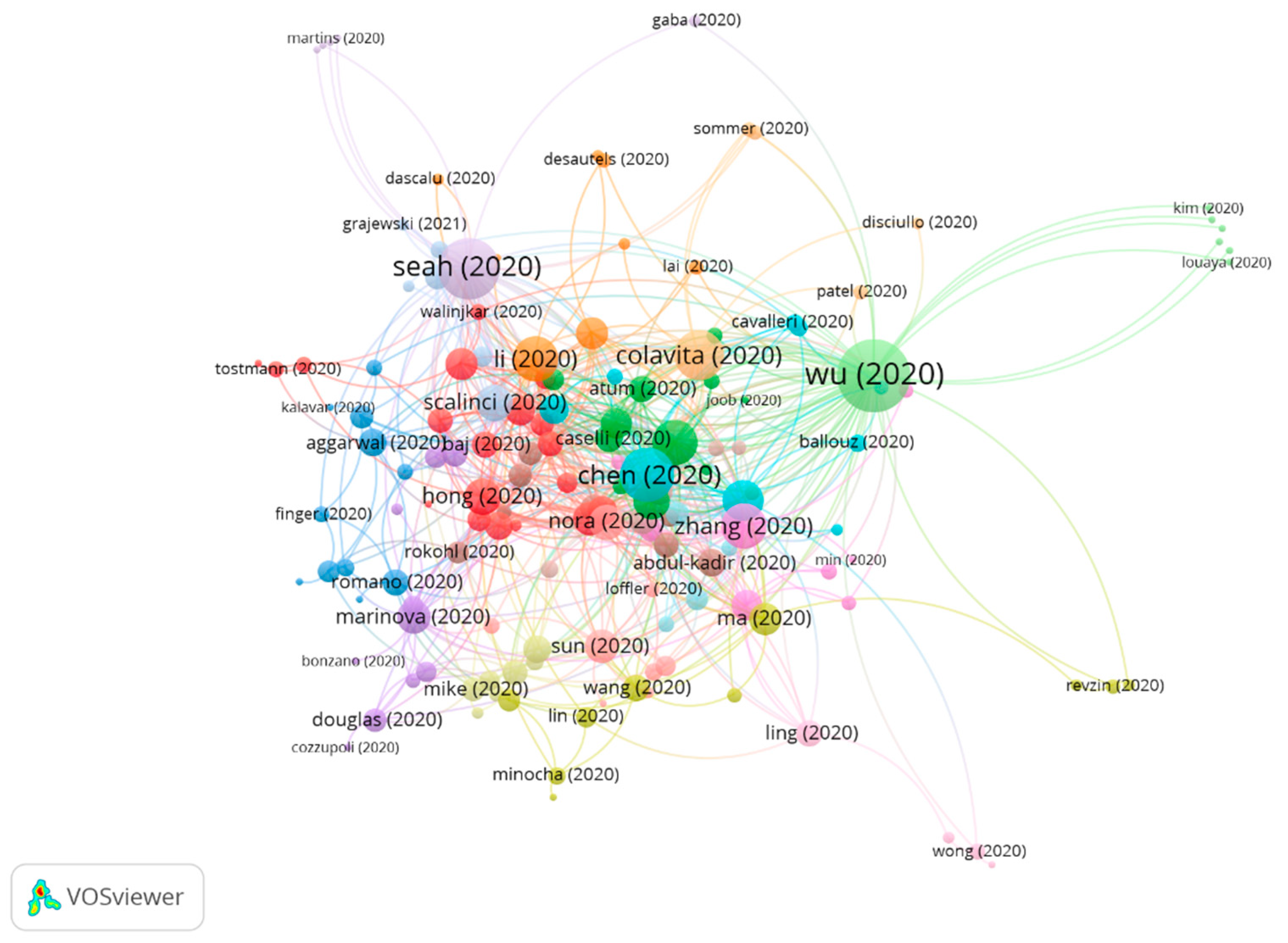
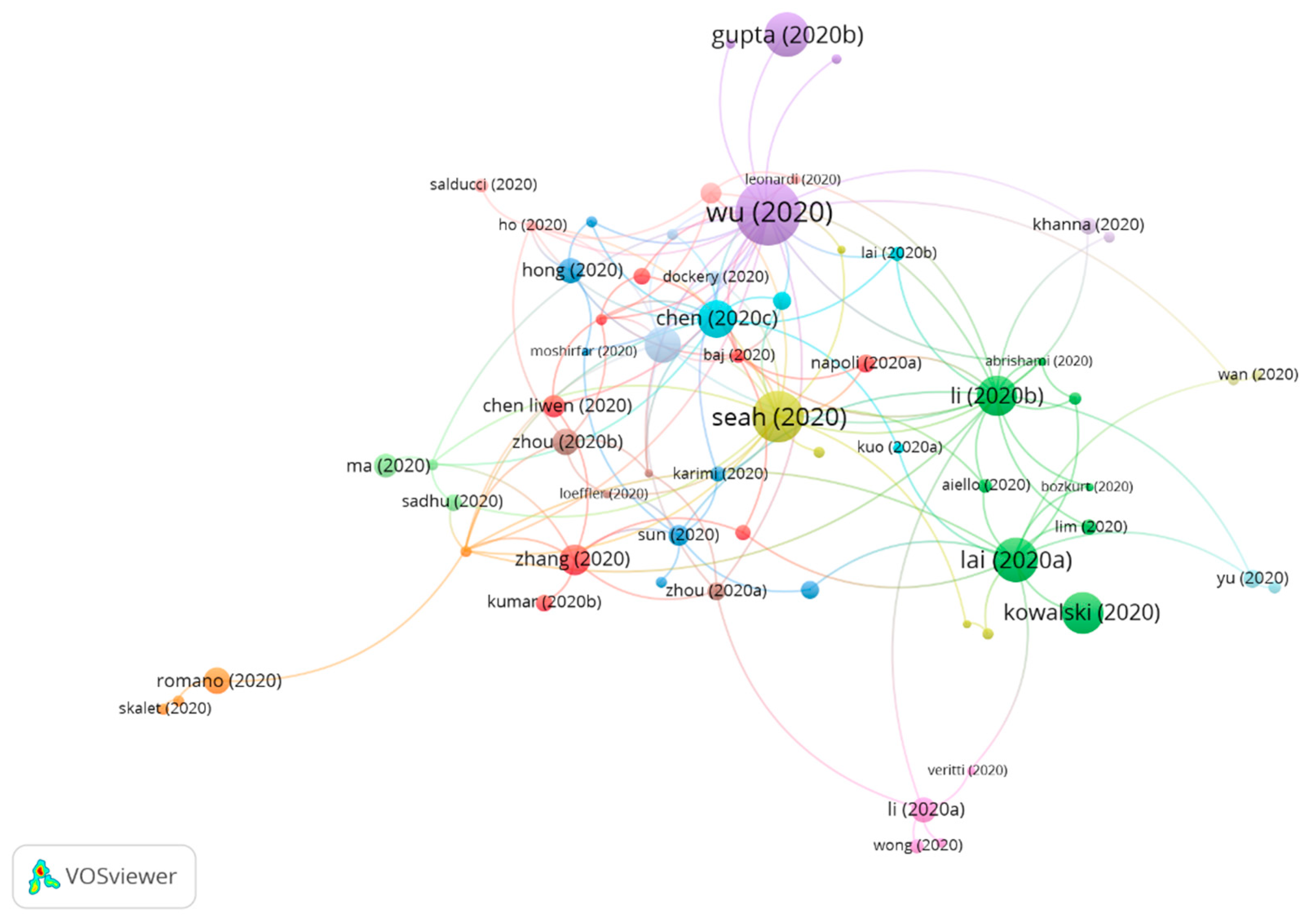
Citation network analysis is used to search scientific literature on a specific subject. That is, through a single publication, it is possible to find additional and relevant publications to prove qualitatively and quantitatively the relation between articles and authors while creating groups [
19]. Furthermore, it allows to measure the most cited publication within each group, as well as to study the development of a research field or to focus the search on a specific subject [
20,
21].
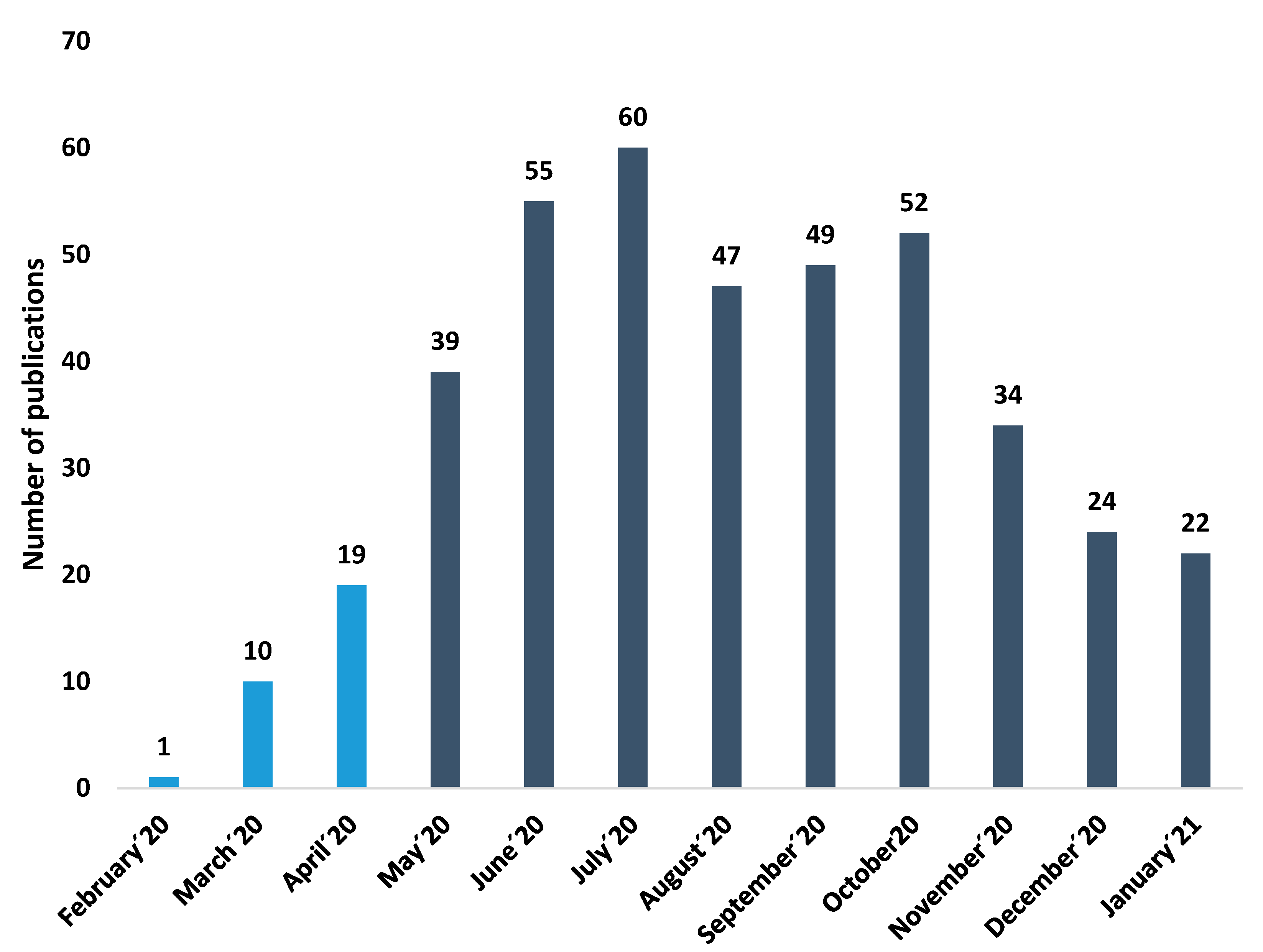
Thus, given the increasing number of publications about COVID-19 and its ocular consequences, this study aims is to identify the different research fields and to determine the most cited publication. In addition, the relation between the different publications and research groups will also be analyzed through the CitNetExplorer software, whose main objective is to study the development of scientific literature in a research field.
4. Discussion
The main databases, such as Web of Science or Scopus, allow the creation of citation networks. However, when conducting a systematic review of all the existing literature on a subject, their usefulness is limited, given that they do not provide a general overview of the connection between citations of a group of publications. Therefore, the CitNetExplorer and CiteSpace software were used to visualize, analyze, and explore citation networks of scientific publications, as these offer more detailed analysis when creating citation networks than databases such as Web of Science or Scopus [
21].
The main aim of this study was to analyze the existing literature about the impact of COVID-19 at the ocular level. To this effect, the Web of Science database was used. It presents one of the most extensive databases since its search range starts in 1900. However, it should be noted that Web of Science only accepts journals with an international presence that have passed a rigorous selection process.
Thus, by downloading the existing bibliography at WOS, the CitNetExplorer and CiteSpace software allowed us to collect and analyze all the available literature on the impact of COVID-19 in ocular disease. The connection between fields of study and different research groups was also assessed through citation network analysis. To obtain the results, the
clustering function was used. This function allows the grouping of the publications according to the relationship among citations. The
drilling down function was also used to conduct a deeper analysis of the existing bibliography of each group. The
core publications function shows the main publications, i.e., those with a minimum number of citations (≥4 citations). Therefore, these functions make it possible for a complete analysis and study of the research on the field of study to be conducted. The methodology was based on other citation network studies carried out by our research team [
49,
50,
51].
The first publication on eye symptoms in COVID-19 patients was published by Lu et al. [
52] in the
Lancet, in a letter to the editor where conjunctivitis was found as the first symptom in a pulmonologist, after having been in a hospital in Wuhan. Nevertheless, the first articles were only published in March 2020. One publication that should be noted is the one published by Chen et al. [
42] in
Acta Ophthalmologica, where they found that 27 out of the 535 patients with COVID-19 had conjunctival congestion (four of them as an initial symptom). The average duration of conjunctival congestion was 5.9 to 4.5 days. They also found that some patients with COVID-19 had chronic ocular diseases, such as conjunctivitis (6.2%), xerophthalmia (4.5%), and keratitis (2.6%). Therefore, conjunctival congestion is one of the ocular symptoms related to COVID-19 and could occur as an initial symptom. Frequent hand-to-eye contact may be a risk factor for conjunctival congestion in patients with COVID-19.
Another study was published by Li et al. [
32] in the
British Journal of Ophthalmology, comparing SARS-CoV-2 with other types of coronaviruses. In doing so, it was found that no ocular involvement has been described with either MERS-CoV or SARS-CoV, although PCR-RT on tears from patients with SARS-CoV infection demonstrated the presence of the virus. There is also evidence that some coronavirus can occasionally cause conjunctivitis in humans. Human coronavirus NL 63 (HCoV-NL63) was first detected in an infant with bronchiolitis and conjunctivitis. Subsequently, 17% of 28 cases of children with confirmed HCoV-NL63 infections had conjunctivitis [
53,
54,
55,
56,
57,
58].
One journal with a particularly high number of publications on the impact of COVID-19 at the ocular level is the Indian Journal of Ophthalmology, which occupies the 68th place in the ophthalmology category and has an impact factor of 1.25. This is related to the fact that India is one of the countries with the highest number of publications in this area of research, because of the potential for extensive nationwide transmission based on the current health management system and a population that rivals China [
59]. Furthermore, the journal with the highest impact factor is
Ophthalmology, 8.47. However, it must be noted that the impact factor is a critical index that informs about the importance of journals, but it is not an absolute measurement index. The main difference between both is that the latter is based on the impact of the research results, as well as the physical and intellectual contributions of the authors [
60]. At the beginning of the pandemic, the first articles were published in China. However, as it advanced, other countries such as India, Italy, and the United States increased their number of publications. This is related to increased concern among healthcare workers and front-line politicians due to the language barrier. Today, research is mainly focused on symptoms, as well as finding an effective treatment and vaccine against COVID-19. This explains why research is being done in this field in countries with higher incomes and therefore better infrastructures, leading to a growing number of publications. We assume that lower-income countries focus on other research fields, such as transmission or epidemiology, although with fewer publications [
26,
27].
Today, numerous studies analyze the transmission of SARS-CoV-2 at the ocular level.
This agrees with the results obtained in our study that the most cited publications are those that analyze the most frequent ocular symptoms in patients with COVID-19.
On the one hand, in a study by Sun et al. [
48], the authors considered that the risk of transmission of the virus by the ocular surface was unlikely, due to the low prevalence of SARS-CoV-2 on the ocular surface and because of conjunctivitis related with COVID-19. However, they warned that the virus can be transmitted during ophthalmic practice. In the study by Peng et al. [
61], the authors stated that the detection of SARS-CoV-2 RNA in the tears and conjunctival secretions of COVID-19 patients with conjunctivitis could be coincidental, instead of indicating SARS-CoV-2 conjunctiva infection as the cause of conjunctivitis. Despite this, there is enough anatomical evidence justifying the possibility that the ocular surface is a route of transmission of SARS-CoV-2 [
62]. Thus, in Dawood’s study [
63], the existence of ACE2 was shown in conjunctiva, cornea, and limbus after immunohistochemistry analysis. Moreover, conjunctival surgical specimens show ACE2 expression in the conjunctival epithelium. For this reason, ACE2 in the host cell is considered to act as a receptor for SARS-CoV-2. Likewise, cellular protease TMPRSS2 is confirmed to facilitate viral entry after the union of SARS-CoV-2 protein S with ACE2. More specifically, protein S is divided into two subunits, S1 and S2, by an extracellular protease. While S1 binds to ACE2, S2 cleaves further and is activated by TMPRSS2. On the other hand, it has also been related to the fact that the ocular surface, which is comprised of the tear film and the epithelium of the conjunctiva and cornea, is closely linked to the respiratory tract through the nasolacrimal duct. Thus, blinking spreads, mixes, and distributes tears and generates a pumping effect that attracts tears to the lacrimal sac and then into the inferior nasal meatal of the nose [
53,
64]. Thus, the nasolacrimal duct forms a conduct for viruses to spread between the eye and the upper respiratory tract. However, the direction in which SARS-CoV-2 would spread along in this conduct is unknown. In this regard, Tong et al. [
65] examined this connection, using conjunctival-upper respiratory tract irrigation to test for the presence of SARS-CoV nucleotides. Patients self-administered a drop of saline solution into each eye, blinked repeatedly, tilted their head back, and breathed to facilitate drainage into the nasopharynx. These samples were positive in two of the four patients confirmed with SARS-CoV-2.
The overall prevalence of ocular symptoms in patients with COVID-19 is 11.2%, which means that it is not a common finding. However, this prevalence could be an underestimation, since patients with COVID-19 present life-threatening clinical scenarios, which may prevent a detailed ocular examination or relevant background information. Furthermore, in large retrospective studies, ophthalmological examinations were not accurately detailed [
6]. The most frequent ocular symptom is conjunctivitis, together with hyperemia, foreign body sensation, chemosis, and epiphora, followed by ocular pain, dry eye, floaters, and palpebral dermatitis [
14]. However, other authors found no evidence of significant conjunctival expression of ACE-2 [
66]. A recent study showed that no consistent TMPRSS2 existence can be found in conjunctival samples, while it is present in some pterygium samples [
41].
A recent report analyzing findings in optical coherence tomography (OCT) in 12 patients who tested positive for COVID-19 showed hyperreflective lesions at the ganglion cell layer and inner plexiform layers. This finding was bilateral and was present in all patients, being more prominent in the papillomacular bundle [
67]. It should also be noted that elevated serum levels of complement C3 have also been related to an increased risk of developing diabetic retinopathy, nephropathy, and neuropathy, through endothelial dysfunction and thrombosis [
68]. Immunohistochemistry in the human eye has shown that the ciliary body, choroid, retina, and retinal pigment epithelium (RPE) contain significant levels of ACE receptors [
69]. Since COVID-19 can target vascular pericytes expressing ACE-2, a viral infection could lead to an endothelial cell dysfunction complement-mediated, microvascular damage and thus the involvement of the ocular circulation. C3a and C5a, small cleavage fragments (approximately 10 KDa) are released through complement activation. That is, they are powerful mediators of inflammation. They are considered anaphylatoxins and act as cell activators presenting nanomolar affinity. The interaction between C3a and C5a with their respective receptors on vascular endothelium is associated with over-expression of ICAM-1 by these vascular endothelial cells. ICAM-1 increases the activation of vascular endothelial cells [
70]. COVID-19-associated coagulopathy may predispose to a spectrum of thromboembolic events.
Neurological alterations in patients with COVID-19 include polyneuritis, Guillain–Barré syndrome (GBS), meningitis, encephalomyelitis, and encephalopathy [
71]. Oculomotor nerve palsy could be triggered by the direct invasion of the virus, inflammatory factors related to viral infection, or could be secondary to neurological complications such as GBS, acute disseminated encephalomyelitis, or transverse myelitis [
72]. SARS-CoV-2 can trigger GBS via the molecular mimicry mechanism due to similarities between amino acid sequences of SARS-CoV2 protein and neuronal membrane gangliosides. One of the prominent assumptions about the underlying pathological mechanisms of GBS is molecular mimicry. This is a process in which antibodies created to fight against viruses or other pathogens bind to gangliosides on the surface membranes of peripheral sensory and motor neurons. This causes immune-mediated damage to the myelin sheath and/or axons. The SARS-CoV-2 infection triggers an adaptive immune response in which interactions between T cells and B cells result in the production of specific antibodies against SARS-CoV-2, but a similarity in sequences or structure of viral peptides and gangliosides (molecular mimicry). This cross-reactivity in SARS-CoV-2 infected individuals, with appropriate HLA-typing due to similarity between amino acid sequences of SARS-CoV2 proteins and neuronal membrane gangliosides, lead to a loss of immunotolerance [
73].
Although animal models suggest that eye injuries could include optic neuritis, an increased incidence of cases of ischemic or inflammatory optic neuropathies associated with COVID-19 has not yet been reported in the literature [
29].
In turn, the most frequent ocular complications in ICU patients are superficial disorders, ranging from mild conjunctival irritation to severe infectious keratitis. This is because these patients have several risk factors for superficial disorders, some of them related to treatments, while others are related to the ICU environment, for example, exposure to many potentially multiresistant bacteria [
74,
75].
Chloroquine (CQ) and hydroxychloroquine (HCQ) have been widely adopted in the clinical setting for the treatment of SARS-CoV-2 infection. However, the proposed doses (CQ: 1000 mg/day for 10 days; HCQ: 800 mg on the first day and then 400 mg/day for 5 days) are much higher than the recommended maximum safe daily doses of both agents (CQ: ≤2.3 mg/kg/day; HCQ: ≤5.0 mg/kg/day). Exposure to safe doses can cause retinal toxicity within five years, so it is considered that exposure to high doses for a short period of time could also cause retinal damage [
76].
Second-generation antiretroviral drugs (lopanivir and ritnovaris) used for HIV treatment can cause long-term pigmentary changes in the macula, resulting in severe vision loss [
77]. However, in most cases of COVID-19, the of treatment lasts between five and seven days, so retinal toxicity is unlikely to occur [
78].
Thus, social distancing has led companies to perform operations remotely and it is speculated whether there will be a “new normality” after this pandemic. Hence, that would imply telehealth for medicine. Teleophthalmology has been repeatedly demonstrated to be of help in the detection and treatment of a variety of eye conditions in adults and children. It has the potential to increase access to primary and specialized care and overcome the unique barriers that the COVID-19 pandemic has created. Until now, tele-ophthalmology has been used primarily for screening for diabetic retinopathy, whose prevalence continues to increase, diagnosis of glaucoma, and macular degeneration monitoring. Ophthalmology clinics equipped with remote sensing devices, functional on their own or that could be operated by minimally trained staff, can bridge a gap in the availability of treatment in prolonged periods of quarantine and isolation, along with patients with COVID-19. Therefore, in the future, thanks to the improvements in image processing, as well as better integration with electronic medical records, teleophthalmology will probably become a much more accepted and more widely used modality, particularly in circumstances in which social distancing measures are recommended [
79].
5. Conclusions
In conclusion, this study offers a comprehensive and objective analysis of the main papers on the impact of COVID-19 at an ocular level. Furthermore, by using the Web of Science database and the Citation Network Explorer software, it was possible to visualize, analyze, and explore the most cited articles and the existing citation networks to date.
In this study, three main groups have been found on the impact of COVID-19 at the ocular level (ocular manifestations, teleophthalmology, and personal protective equipment). Eye symptoms being the most researched topic. In addition, it has been found that the most affected countries are those that present a greater number of publications.
Thus, ocular symptoms are a common finding in COVID-19 patients. These are more frequent in ICU patients due to various risk factors that can alter the ocular surface. That is, in patients with mild symptoms it is rare to find them. In addition, many articles have found the presence of COVID-19 in the tear, so it can be transmitted through this route.
For this reason, together with social distancing, teleophthalmology has been created, showing potential for the treatment and monitoring of patients.
The number of citation network studies has been increasing because it is the only method of analysis that provides a global overview of the different fields of study within a specific topic. Moreover, the CitNetExplorer software facilitates the analysis of all existing studies on a given matter, as it allows for more detailed research. This might change how research is conducted in different fields of study.


 ,
, 











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}