
Management of Dyspepsia and Gastroparesis in Patients with Diabetes. A Clinical Point of View in the Year 2021

 , and
, and 
Abstract
:1. Introduction
2. Dyspepsia: Definition and Clinical Classification
2.1. Organic Dyspepsia
2.2. Functional Dyspepsia
3. Dyspepsia in Diabetic Patients
4. H. pylori Infection in Patients with Diabetes
5. Diabetic Gastroparesis
6. Clinical Management of Dyspepsia
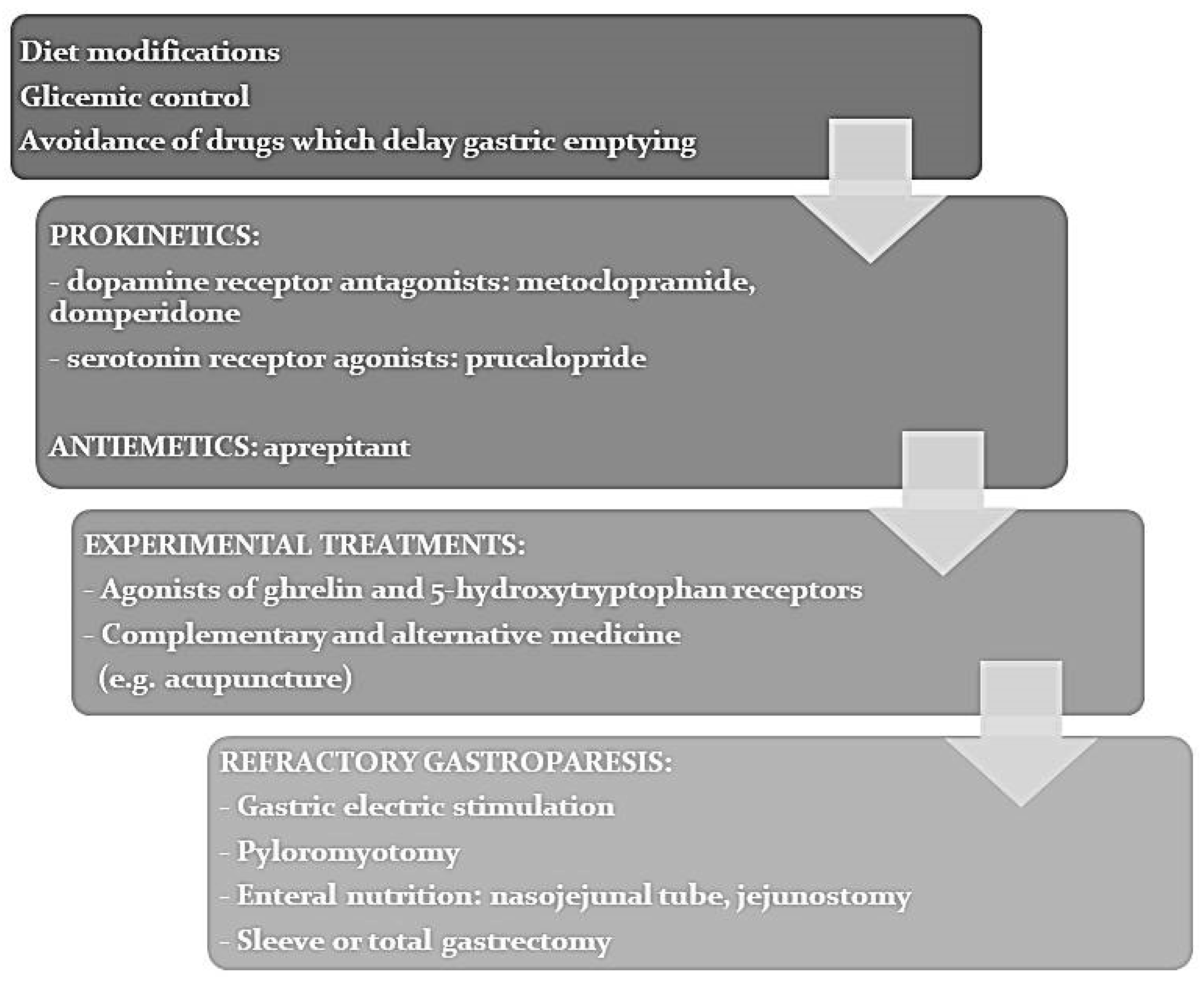
7. Clinical Management of Gastroparesis
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- International Diabetes Federation. IDF Diabetes Atlas, 9th ed.; International Diabetes Federation: Brussels, Belgium, 2019. [Google Scholar]
- Bharucha, A.E.; Kudva, Y.C.; Prichard, D.O. Diabetic gastroparesis. Endocr. Rev. 2019, 40, 1318–1352. [Google Scholar] [CrossRef] [PubMed]
- Pasricha, P.J.; Grover, M.; Yates, K.P.; Abell, T.L.; Bernard, C.E.; Koch, K.L.; McCallum, R.W.; Sarosiek, I.; Kuo, B.; Bulat, R.; et al. Functional dyspepsia and gastroparesis in tertiary care are interchangeable syndromes with common clinical and pathological features. Gastroenterology 2021. [Google Scholar] [CrossRef]
- Durazzo, M.; Lupi, G.; Cicerchia, F.; Ferro, A.; Barutta, F.; Beccuti, G.; Gruden, G.; Pellicano, R. Extra-esophageal presentation of gastroesophageal reflux disease: 2020 Update. J. Clin. Med. 2020, 9, 2559. [Google Scholar] [CrossRef] [PubMed]
- Moayyedi, P.; Lacy, B.E.; Andrews, C.N.; Enns, R.A.; Howden, C.W.; Vakil, N. ACG and CAG Clinical Guideline: Management of Dyspepsia. Am. J. Gastroenterol. 2017, 112, 988–1013. [Google Scholar] [CrossRef] [PubMed]
- Oustamanolakis, P.; Tack, J. Dyspepsia: Organic versus functional. J. Clin. Gastroenterol. 2012, 46, 175–190. [Google Scholar] [CrossRef]
- Sugano, K.; Tack, J.; Kuipers, E.J.; Graham, D.Y.; El-Omar, E.M.; Miura, S.; Haruma, K.; Asaka, M.; Uemura, N.; Malfertheiner, P. Faculty members of Kyoto Global Consensus Conference. Kyoto global consensus report on Helicobacter pylori gastritis. Gut 2015, 64, 1353–1367. [Google Scholar] [CrossRef] [Green Version]
- Drossman, D.A. Functional gastrointestinal disorders: History, pathophysiology, clinical features and Rome IV. Gastroenterology 2016, 150, 1262–1279. [Google Scholar] [CrossRef] [Green Version]
- Stanghellini, V.; Chan, F.K.; Hasler, W.L.; Malagelada, J.R.; Suzuki, H.; Tack, J.; Talley, N.J. Gastroduodenal disorders. Gastroenterology 2016, 150, 1380–1392. [Google Scholar] [CrossRef]
- Mosso, E.; Bonetto, S.; Longobardi, G.; Abenavoli, L.; Ribaldone, D.G.; Saracco, G.M.; Pellicano, R. Management of functional dyspepsia in the year 2020. A clinical point of view. Minerva Gastroenterol. Dietol. 2020, 66, 331–342. [Google Scholar]
- Koletzko, L.; Macke, L.; Schulz, C.; Malfertheiner, P. Helicobacter pylori eradication in dyspepsia: New evidence for symptomatic benefit. Best Pract. Res. Clin. Gastr. 2019, 40–41, 101637. [Google Scholar] [CrossRef]
- Walker, M.M.; Potter, M.D.; Talley, N.J. Tangible pathologies in functional dyspepsia. Best Pract. Res. Clin. Gastroent. 2019, 40, 101650. [Google Scholar] [CrossRef]
- Fagoonee, S.; Pellicano, R. Helicobacter pylori: Molecular basis for colonization and survival in gastric environment and resistance to antibiotics. A short review. Infect. Dis. 2019, 51, 399–408. [Google Scholar] [CrossRef]
- Marinoni, C.; Ribaldone, D.G.; Rosso, C.; Astegiano, M.; Caviglia, G.P. Diagnosis of Helicobacter pylori infection: A look into molecular aspects of urea breath test. Minerva Biotecnol. 2019, 31, 100–107. [Google Scholar] [CrossRef]
- Pellicano, R.; Ribaldone, D.G.; Fagoonee, S.; Astegiano, M.; Saracco, G.M.; Mégraud, F. A 2016 panorama of Helicobacter pylori infection: Key messages for clinicians. Panminerva Med. 2016, 58, 304–317. [Google Scholar] [PubMed]
- Buzás, G.M. Helicobacter pylori and non-alcoholic fatty liver disease. Minerva Gastroenterol. Dietol. 2020, 66, 267–279. [Google Scholar] [CrossRef] [PubMed]
- Yang, F.; Xu, Y.L.; Zhu, R.F. Helicobacter pylori infection and the risk of colorectal carcinoma: A systematic review and meta-analysis. Minerva Med. 2019, 110, 464–470. [Google Scholar] [CrossRef]
- Valenzano, M.; Bisio, A.; Grassi, G. Helicobacter pylori and diabetes mellitus: A controversial relationship. Minerva Endocrinol. 2019, 44, 301–309. [Google Scholar] [CrossRef]
- Santambrogio, E.; Orsucci, L. Helicobacter pylori and hematological disorders. Minerva Gastroenterol. Dietol. 2019, 65, 204–213. [Google Scholar] [CrossRef]
- Chuah, K.H.; Mahadeva, S. Cultural factors influencing functional gastrointestinal disorders in the East. J. Neurogastroenterol. Motil. 2018, 24, 536–543. [Google Scholar] [CrossRef] [Green Version]
- Stanghellini, V.; Tosetti, C.; Paternico, A.; Barbara, G.; Morselli-Labate, A.M.; Monetti, N.; Marengo, M.; Corinaldesi, R. Risk indicators of delayed gastric emptying of solids in patients with functional dyspepsia. Gastroenterology 1996, 110, 1036–1042. [Google Scholar] [CrossRef]
- Tack, J.; Van den Houte, K.; Carbone, F. The unfulfilled promise of prokinetics for functional dyspepsia/post-prandial distress syndrome. Am. J. Gastroenterol. 2019, 114, 204–206. [Google Scholar] [CrossRef] [PubMed]
- Miwa, H.; Oshima, T.; Tomita, T.; Fukui, H.; Kondo, T.; Yamasaki, T.; Watari, J. Recent understanding of the pathophysiology of functional dyspepsia: Role of the duodenum as the pathogenic center. J. Gastroenterol. 2019, 54, 305–311. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pellicano, R. Human microbiota and inflammatory bowel diseases: New pieces of an intricate puzzle. Minerva Gastroenterol. Dietol. 2019, 65, 171–172. [Google Scholar] [CrossRef]
- Korotkyi, O.; Vovk, A.; Galenova, T.; Vovk, T.; Dvorschenko, K.; Luzza, F.; Abenavoli, L.; Kobyliak, N.; Falalyeyeva, T. Effect of probiotic on serum cytokines and matrix metalloproteinases profiles during monoiodoacetate-induced osteoarthritis in rats. Minerva Biotecnol. 2019, 31, 68–73. [Google Scholar] [CrossRef]
- Korotkyi, O.; Dvorshchenko, K.; Falalyeyeva, T.; Sulaieva, O.; Kobyliak, N.; Abenavoli, L.; Fagoonee, S.; Pellicano, R.; Ostapchenko, L. Combined effects of probiotic and chondroprotector during osteoarthritis in rats. Panminerva Med. 2020, 62, 93–101. [Google Scholar] [CrossRef] [PubMed]
- Pasini, E.; Corsetti, G.; Assanelli, D.; Testa, C.; Romano, C.; Dioguardi, F.S.; Aquilani, R. Effects of chronic exercise on gut microbiota and intestinal barrier in human with type 2 diabetes. Minerva Med. 2019, 110, 3–11. [Google Scholar] [CrossRef]
- Caviglia, G.P.; Rosso, C.; Ribaldone, D.G.; Dughera, F.; Fagoonee, S.; Astegiano, M.; Pellicano, R. Physiopathology of intestinal barrier and the role of zonulin. Minerva Biotecnol. 2019, 31, 83–92. [Google Scholar] [CrossRef]
- Adriani, A.; Ribaldone, D.G.; Astegiano, M.; Durazzo, M.; Saracco, G.M.; Pellicano, R. Irritable bowel syndrome: The clinical approach. Panminerva Med. 2018, 60, 213–222. [Google Scholar] [CrossRef]
- Gotfried, J.; Priest, S.; Schey, R. Diabetes and the Small Intestine. Curr. Treat Options Gastroenterol. 2017, 15, 490–507. [Google Scholar] [CrossRef]
- Marathe, C.S.; Rayner, C.K.; Wu, T.; Jones, K.L.; Horowitz, M. Gastrointestinal Disorders in Diabetes. In Endotext [Internet]; Feingold, K.R., Anawalt, B., Boyce, A., Chrousos, G., de Herder, W.W., Dungan, K., Grossman, A., Hershman, J.M., Hofland, J., Kaltsas, G., et al., Eds.; MDText.com, Inc.: South Dartmouth, MA, USA, 2000. [Google Scholar]
- Devrajani, B.R.; Shah, S.Z.; Soomro, A.A.; Devrajani, T. Type 2 diabetes mellitus: A risk factor for Helicobacter pylori infection: A hospital based case-control study. Int. J. Diabetes Dev. Ctries. 2010, 30, 22–26. [Google Scholar] [CrossRef] [Green Version]
- Bener, A.; Ağan, A.F.; Al-Hamaq, A.O.A.A.; Barisik, C.C.; Öztürk, M.; Ömer, A. Prevalence of Helicobacter pylori infection among Type 2 Diabetes Mellitus. Adv. Biomed. Res. 2020, 9, 27. [Google Scholar] [CrossRef] [PubMed]
- Huang, J. Analysis of the Relationship between Helicobacter pylori infection and diabetic gastroparesis. Chin. Med. J. 2017, 130, 2680–2685. [Google Scholar] [CrossRef] [PubMed]
- Feldman, M.; Schiller, L.R. Disorders of gastrointestinal motility associated with diabetes mellitus. Ann. Intern. Med. 1983, 98, 378–384. [Google Scholar] [CrossRef]
- Choung, R.S.; Locke, G.R., III; Schleck, C.D.; Zinsmeister, A.R.; Melton, L.J., III; Talley, N.J. Risk of gastroparesis in subjects with type 1 and 2 diabetes in the general population. Am. J. Gastroenterol. 2012, 107, 82–88. [Google Scholar] [CrossRef] [PubMed]
- Tack, J.; van den Houte, K.; Carbone, F. Gastroduodenal motility disorders. Curr. Opin. Gastroenterol. 2018, 34, 428–435. [Google Scholar] [CrossRef]
- Halland, M.; Bharucha, A.E. Relationship between control of glycemia and gastric emptying disturbances in diabetes mellitus. Clin. Gastroenterol. Hepatol. 2016, 14, 929–936. [Google Scholar] [CrossRef] [Green Version]
- MacGregor, I.L.; Gueller, R.; Watts, H.D.; Meyer, J.H. The effect of acute hyperglycemia on gastric emptying in man. Gastroenterology 1976, 70, 190–196. [Google Scholar] [CrossRef]
- Bharucha, A.E.; Batey-Schaefer, B.; Cleary, P.A.; Murray, J.A.; Cowie, C.; Lorenzi, G.; Driscoll, M.; Harth, J.; Larkin, M.; Christofi, M.; et al. Diabetes Control and Complications Trial–Epidemiology of Diabetes Interventions and Complications Research Group. Delayed gastric emptying is associated with early and long-term hyperglycemia in type 1 diabetes mellitus. Gastroenterology 2015, 149, 330–339. [Google Scholar] [CrossRef] [Green Version]
- Alnasser, S.A.; Algeffari, M.A. Prevalence and risk factors of gastroparesis-related symptoms among patients with type 2 diabetes. Int. J. Health Sci. 2016, 10, 397–404. [Google Scholar]
- Laway, B.A.; Malik, T.S.; Khan, S.H.; Rather, T.A. Prevalence of abnormal gastric emptying in asymptomatic women with newly detected diabetes and its reversibility after glycemic control-a prospective case control study. J. Diabetes Complicat. 2013, 27, 78–81. [Google Scholar] [CrossRef]
- Jehangir, A.; Abdallah, R.T.; Parkman, H.P. Characterizing abdominal pain in patients with gastroparesis into neuropathic and nociceptive components. J. Clin. Gastroenterol. 2019, 53, 427–433. [Google Scholar] [CrossRef] [PubMed]
- Durazzo, M.; Gargiulo, G.; Pellicano, R. Non-cardiac chest pain: A 2018 update. Minerva Cardioangiol. 2018, 66, 770–783. [Google Scholar] [CrossRef] [PubMed]
- Roy, T.; Lloyd, C.E. Epidemiology of depression and diabetes: A systematic review. J. Affect Disord. 2012, 142, S8–S21. [Google Scholar] [CrossRef]
- Zahn, A.; Langhans, C.D.; Hoffner, S.; Haberkorn, U.; Rating, D.; Haass, M.; Enck, P.; Stremmel, W.; Rühl, A. Measurement of gastric emptying by 13C-octanoic acid breath test versus scintigraphy in diabetics. Z. Gastroenterol. 2003, 41, 383–390. [Google Scholar]
- Farrell, M.B. Gastric Emptying Scintigraphy. J. Nucl. Med. Technol. 2019, 47, 111–119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghoos, Y.F.; Maes, B.D.; Geypens, B.J.; Mys, G.; Hiele, M.I.; Rutgeerts, P.J.; Vantrappen, G. Measurement of gastric emptying rate of solids by means of a carbon-labeled octanoic acid breath test. Gastroenterology 1993, 104, 1640–1647. [Google Scholar] [CrossRef]
- Ziegler, D.; Schadewaldt, P.; Pour Mirza, A.; Piolot, R.; Schommartz, B.; Reinhardt, M.; Vosberg, H.; Brösicke, H.; Gries, F.A. [13C]octanoic acid breath test for non-invasive assessment of gastric emptying in diabetic patients: Validation and relationship to gastric symptoms and cardiovascular autonomic function. Diabetologia 1996, 39, 823–830. [Google Scholar] [CrossRef] [Green Version]
- Pinto-Sanchez, M.I.; Yuan, Y.; Hassan, A.; Bercik, P.; Moayyedi, P. Proton pump inhibitors and functional dyspepsia. Cochrane Database Syst. Rev. 2017, 11, CD01119. [Google Scholar]
- Jin, M.; Mo, Y.; Ye, K.; Chen, M.; Liu, Y.; He, C. Efficacy of serotonin receptor agonists in the treatment of functional dyspepsia: A meta-analysis. Arch Med. Sci. 2019, 15, 23–32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mansi, C.; Borro, P.; Giacomini, M.; Biagini, R.; Mele, M.R.; Pandolfo, N.; Savarino, V. Comparative effects of levosulpiride and cisapride on gastric emptying and symptoms in patients with functional dyspepsia and gastroparesis. Aliment Pharmacol. Ther. 2000, 14, 561–569. [Google Scholar] [CrossRef]
- Tack, J.; Masuy, I.; Van Den Houte, K.; Wauters, L.; Schol, J.; Vanuytsel, T.; Vandenberghe, A.; Carbone, F. Drugs under development for the treatment of functional dyspepsia and related disorders. Expert Opin. Investig. Drugs 2019, 28, 871–889. [Google Scholar] [CrossRef]
- Matsueda, K.; Hongo, M.; Tack, J.; Saito, Y.; Kato, H. A placebo-controlled trial of acotiamide for meal-related symptoms of functional dyspepsia. Gut 2012, 61, 821–828. [Google Scholar] [CrossRef] [Green Version]
- Talley, N.J.; Locke, G.R.; Saito, Y.A.; Almazar, A.E.; Bouras, E.P.; Howden, C.W.; Lacy, B.E.; DiBaise, J.K.; Prather, C.M.; Abraham, B.P.; et al. Effect of amitriptyline and escitalopram on functional dyspepsia: A multicenter, randomized controlled study. Gastroenterology 2015, 149, 340–349.e2. [Google Scholar] [CrossRef] [Green Version]
- Lacy, B.E.; Saito, Y.A.; Camilleri, M.; Bouras, E.; DiBaise, J.K.; Herrick, L.M.; Szarka, L.A.; Tilkes, K.; Zinsmeister, A.R.; Talley, N.J. Effects of antidepressants on gastric function in patients with functional dyspepsia. Am. J. Gastroenterol. 2018, 113, 216–224. [Google Scholar] [CrossRef] [PubMed]
- Tomita, T.; Oshima, T.; Miwa, H. New approaches to diagnosis and treatment of functional dyspepsia. Curr. Gastroenterol. Rep. 2018, 20, 55. [Google Scholar] [CrossRef]
- Tan, V.P.; Liu, K.S.; Lam, F.Y.; Hung, I.F.N.; Yuen, M.F.; Leung, W.K. Randomised clinical trial: Rifaximin versus placebo for the treatment of functional dyspepsia. Aliment Pharmacol Ther. 2017, 45, 767–776. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Igarashi, M.; Nakae, H.; Matsuoka, T.; Takahashi, S.; Hisada, T.; Tomita, J.; Koga, Y. Alteration in the gastric microbiota and its restoration by probiotics in patients with functional dyspepsia. BMJ Open Gastro 2017, 3, e000144. [Google Scholar] [CrossRef] [PubMed]
- Asha, M.Z.; Khalil, S.F.H. Pharmacological Approaches to Diabetic Gastroparesis: A systematic review of randomised clinical trials. Sultan Qaboos Univ. Med. J. 2019, 19, e291–e304. [Google Scholar] [CrossRef] [PubMed]
- Dhir, R.; Richter, J.E. Erythromycin in the short- and long-term control of dyspepsia symptoms in patients with gastroparesis. J. Clin. Gastroenterol. 2004, 38, 237–242. [Google Scholar] [CrossRef]
- Grover, M.; Farrugia, G.; Stanghellini, V. Gastroparesis: A turning point in understanding and treatment. Gut 2019, 68, 2238–2250. [Google Scholar] [CrossRef]
- Carbone, F.; Van den Houte, K.; Clevers, E.; Andrews, C.N.; Papathanasopoulos, A.; Holvoet, L.; Van Oudenhove, L.; Caenepeel, P.; Arts, J.; Vanuytsel, T.; et al. Prucalopride in Gastroparesis: A Randomized Placebo-Controlled Crossover Study. Am. J. Gastroenterol. 2019, 114, 1265–1274. [Google Scholar] [CrossRef]
- Camilleri, M.; McCallum, R.W.; Tack, J.; Spence, S.C.; Gottesdiener, K.; Fiedorek, F.T. Efficacy and Safety of Relamorelin in Diabetics With Symptoms of Gastroparesis: A Randomized, Placebo-Controlled Study. Gastroenterology 2017, 153, 1240–1250.e2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singh, R.; Ha, S.E.; Wei, L.; Jin, B.; Zogg, H.; Poudrier, S.M.; Jorgensen, B.G.; Park, C.; Ronkon, C.F.; Bartlett, A.; et al. miR-10b-5p Rescues Diabetes and Gastrointestinal Dysmotility. Gastroenterology 2021. [Google Scholar] [CrossRef] [PubMed]
- Lee, L.A.; Chen, J.; Yin, J. Complementary and alternative medicine for gastroparesis. Gastroenterol. Clin. N. Am. 2015, 44, 137–150. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Xu, J.J.; Liu, S.; Hou, X.H. Electroacupuncture at ST36 ameliorates gastric emptying and rescues networks of interstitial cells of Cajal in the stomach of diabetic rats. PLoS ONE 2013, 8, e83904. [Google Scholar] [CrossRef] [Green Version]
- Rangan, V.; Ukleja, A. Gastroparesis in the Hospital Setting. Nutr. Clin. Pract. 2021, 36, 50–66. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Functional Dyspepsia: |
b. Criteria fulfilled for the last 3 months with symptom onset at least 6 months before diagnosis. |
| Postprandial Distress Syndrome (PDS): |
| 1. One or both of the following for at least 3 days per week and severe enough to impact on usual activities: (a) postprandial fullness (b) early satiation 2. No evidence of organic, systemic, or metabolic disease which can explain symptoms. Criteria fulfilled for the last 3 months with symptom onset at least 6 months before diagnosis. Supportive remarks:
|
| Epigastric Pain Syndrome(EPS): |
| 1. One or both of the following for at least 1 day per week and severe enough to impact on usual activities: (a) epigastric pain (b) epigastric burning 2. No evidence of organic, systemic, or metabolic disease which can explain symptoms Criteria fulfilled for the last 3 months with symptom onset at least 6 months before diagnosis Supportive remarks:
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bonetto, S.; Gruden, G.; Beccuti, G.; Ferro, A.; Saracco, G.M.; Pellicano, R. Management of Dyspepsia and Gastroparesis in Patients with Diabetes. A Clinical Point of View in the Year 2021. J. Clin. Med. 2021, 10, 1313. https://doi.org/10.3390/jcm10061313
Bonetto S, Gruden G, Beccuti G, Ferro A, Saracco GM, Pellicano R. Management of Dyspepsia and Gastroparesis in Patients with Diabetes. A Clinical Point of View in the Year 2021. Journal of Clinical Medicine. 2021; 10(6):1313. https://doi.org/10.3390/jcm10061313
Chicago/Turabian StyleBonetto, Silvia, Gabriella Gruden, Guglielmo Beccuti, Arianna Ferro, Giorgio Maria Saracco, and Rinaldo Pellicano. 2021. "Management of Dyspepsia and Gastroparesis in Patients with Diabetes. A Clinical Point of View in the Year 2021" Journal of Clinical Medicine 10, no. 6: 1313. https://doi.org/10.3390/jcm10061313