
Feasibility of Implementing a Tai Chi Program in an Assisted Living Facility: Reducing Fall Risks and Improving Quality of Life

Abstract
:1. Introduction
1.1. Background
1.2. Tai Chi
1.3. Social Cognitive Theory
1.4. Purpose Statement
2. Methods
2.1. Ethical Consideration
2.2. Setting
2.3. Participants
2.4. Design
2.5. TC Intervention
2.6. Measures
2.7. Data Collection
2.8. Data Analysis
3. Results
3.1. Descriptive Analysis
3.2. Feasibility and Acceptability of the Program
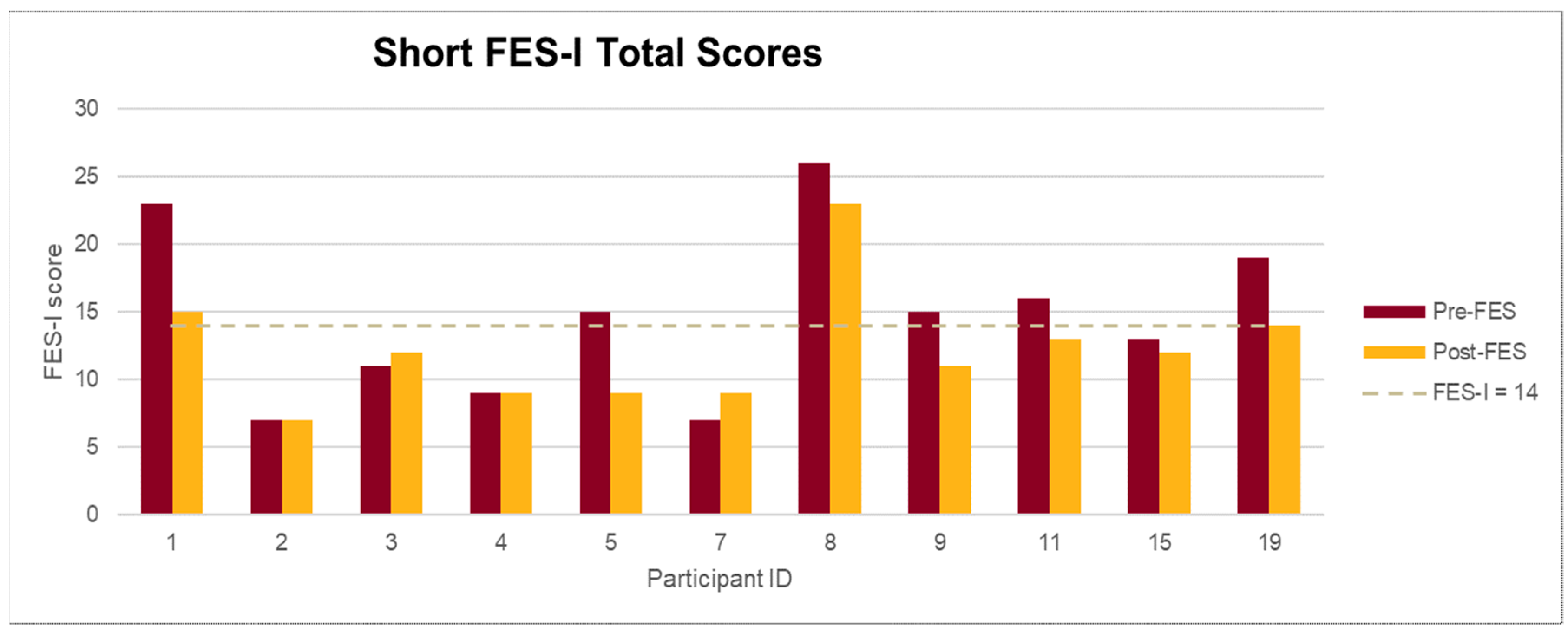
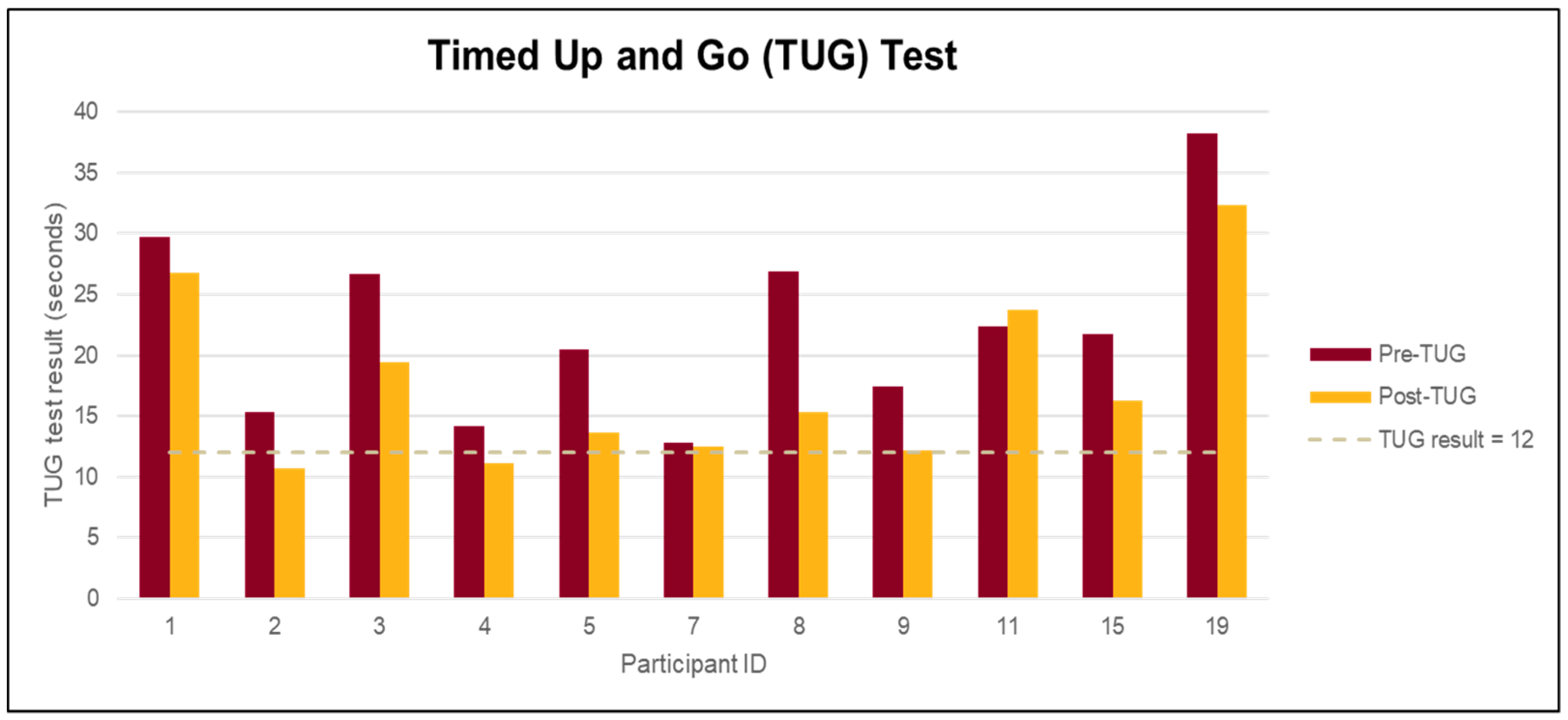
3.3. Differences in Outcomes
4. Discussion
5. Health Care Implications
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. Tai Chi Program Satisfaction Survey
| 1. How many Tai Chi classes did you attend? ________________ (1–12) |
| 2. What prevented you from attending some of the Tai Chi classes? |
| ☐ Sick (e.g., cold, flu, other health problems) |
| ☐ Hospitalization |
| ☐ Conflict with schedule (e.g.,: outings, doctor’s appointment, visitors) |
| ☐ Limited mobility |
| ☐ Others |
| 3. I enjoyed the weekly Tai Chi class very much. |
| ☐ Strongly agree |
| ☐ Agree |
| ☐ Disagree |
| ☐ Strongly disagree |
| 4. What was your favorite part of the Tai Chi classes? |
| ☐ Learning Tai Chi movements |
| ☐ Breathing exercise |
| ☐ Using Imagery (e.g.,: imagine you are a tree rooting down to the earth, imagine you are a flying goose opening up your wings) |
| ☐ Opportunity to engage in teaching (e.g., counting, naming a few tai chi movements you’d like to do) |
| ☐Social interaction |
| Other_________________________________________________________ |
| 5. What was your least favorite part of the Tai Chi classes? |
| ☐ Learning Tai Chi movements |
| ☐ Breathing exercise |
| ☐ Using Imagery (e.g.,: imagine you are a tree rooting down to the earth, imagine you are a flying goose opening up your wings) |
| ☐ Opportunity to engage in teaching (e.g., counting, naming a few tai chi movements you’d like to do) |
| ☐ Social interaction |
| Other_________________________________________________________ |
| 6. The weekly Tai Chi was very helpful to my health and wellbeing. |
| ☐ Strongly agree |
| ☐ Agree |
| ☐ Disagree |
| ☐ Strongly disagree |
| 7. How did the Tai Chi program benefit you? (select all that apply) |
| ☐ Improve strength |
| ☐ Improve flexibility |
| ☐ Improve balance |
| ☐ Improve mood |
| ☐ Improve energy |
| ☐ Reduce pain |
| ☐ Enhance relaxation/reduce stress |
| ☐ Add fun and joy to life |
| Other__________________________________________ |
| 8. Would you recommend this class to your friends and neighbors? |
| ☐ Yes |
| ☐ No |
| ☐ Maybe |
| 9. Would you like this Tai Chi program to continue? |
| ☐ Yes |
| ☐ No If no, why_______________________ |
| 10. What other comments do you have about the Tai Chi class? |
References
- Centers for Disease Control and Prevention. Important Facts about Falls; 2017. Available online: https://www.cdc.gov/homeandrecreationalsafety/falls/adultfalls.html (accessed on 22 December 2020).
- Kendrick, D.; Kumar, A.; Carpenter, H.; Zijlstra, G.A.R.; Skelton, D.A.; Cook, J.R.; Stevens, Z.; Belcher, C.M.; Haworth, D.; Gawler, S.J.; et al. Exercise for reducing fear of falling in older people living in the community (review). Cochrane Database Syst. Rev. 2014, 2014, CD009848. [Google Scholar] [CrossRef]
- Zijlstra, G.A.R.; Van Haastregt, J.C.M.; Van Rossum, E.; Van Eijk, J.T.M.; Yardley, L.; Kempen, G.I.J.M. Interventions to Reduce Fear of Falling in Community-Living Older People: A Systematic Review. J. Am. Geriatr. Soc. 2007, 55, 603–615. [Google Scholar] [CrossRef]
- Burns, E.R.; Stevens, J.A.; Lee, R. The direct costs of fatal and non-fatal falls among older adults—United States. J. Saf. Res. 2016, 58, 99–103. [Google Scholar] [CrossRef]
- Ambrose, A.F.; Paul, G.; Hausdorff, J.M. Risk factors for falls among older adults: A review of the literature. Maturitas 2013, 75, 51–61. [Google Scholar] [CrossRef]
- Avin, K.G.; Hanke, T.A.; Kirk-Sanchez, N.; McDonough, C.M.; Shubert, T.E.; Hardage, J.; Hartley, G. Management of Falls in Community-Dwelling Older Adults: Clinical Guidance Statement From the Academy of Geriatric Physical Therapy of the American Physical Therapy Association. Phys. Ther. 2015, 95, 815–834. [Google Scholar] [CrossRef] [Green Version]
- Stevens Judy, A.; Burns, E. A CDC Compendium of Effective Fall Interventions: What Works for Community-Dwelling Older Adults, 3rd ed.; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2015. [Google Scholar]
- Hackney, M.E.; Wolf, S.L. Impact of Tai Chi Chu’an Practice on Balance and Mobility in Older Adults. J. Geriatr. Phys. Ther. 2014, 37, 127–135. [Google Scholar] [CrossRef]
- Wayne, P.M.; Manor, B.; Novak, V.; Costa, M.D.; Hausdorff, J.M.; Goldberger, A.L.; Ahn, A.C.; Yeh, G.Y.; Peng, C.-K.; Lough, M.; et al. A systems biology approach to studying Tai Chi, physiological complexity and healthy aging: Design and rationale of a pragmatic randomized controlled trial. Contemp. Clin. Trials 2013, 34, 21–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, F. The public health benefits of Tai Ji Quan—Addressing the unmet needs of aging populations in the 21st century. J. Sport Health Sci. 2016, 5, 304–307. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ma, C.; Zhou, W.; Tang, Q.; Huang, S. The impact of group-based Tai chi on health-status outcomes among community-dwelling older adults with hypertension. Hear. Lung 2018, 47, 337–344. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Schmid, C.H.; Fielding, R.A.; Harvey, W.F.; Reid, K.F.; Price, L.L.; Driban, J.B.; Kalish, R.; Rones, R.; McAlindon, T. Effect of tai chi versus aerobic exercise for fibromyalgia: Comparative effectiveness randomized controlled trial. BMJ 2018, 360, k851. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, Z.-G.; Feng, Y.-H.; Li, Y.-H.; Lv, C.-S. Systematic review and meta-analysis: Tai Chi for preventing falls in older adults. BMJ Open 2017, 7, e013661. [Google Scholar] [CrossRef]
- Bubela, D.; Sacharko, L.; Chan, J.; Brady, M. Balance and Functional Outcomes for Older Community-Dwelling Adults Who Practice Tai Chi and Those Who Do Not: A Comparative Study. J. Geriatr. Phys. Ther. 2019, 42, 209–215. [Google Scholar] [CrossRef]
- Wooton, A.C. An Integrative Review of Tai Chi Research. Orthop. Nurs. 2010, 29, 108–116. [Google Scholar] [CrossRef]
- Liu, H.; Frank, A. Tai chi as a balance improvement exercise for older adults: A systematic review. J. Geriatr. Phys. Ther. 2010, 33, 103–109. [Google Scholar]
- Lomas-Vega, R.; Obrero-Gaitán, E.; Molina-Ortega, F.J.; Del-Pino-Casado, R. Tai Chi for Risk of Falls. A Meta-analysis. J. Am. Geriatr. Soc. 2017, 65, 2037–2043. [Google Scholar] [CrossRef] [PubMed]
- Li, F.; Harmer, P.; Fitzgerald, K.; Eckstrom, E.; Akers, L.; Chou, L.-S.; Pidgeon, D.; Voit, J.; Winters-Stone, K. Effectiveness of a TherapeuticTai Ji QuanIntervention vs a Multimodal Exercise Intervention to Prevent Falls Among Older Adults at High Risk of Falling. JAMA Intern. Med. 2018, 178, 1301–1310. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gallant, M.P.; Tartaglia, M.; Hardman, S.; Burke, K. Using Tai Chi to Reduce Fall Risk Factors Among Older Adults: An Evaluation of a Community-Based Implementation. J. Appl. Gerontol. 2019, 38, 983–998. [Google Scholar] [CrossRef]
- Bandura, A. Self-Efficacy: The Exercise of Control; Freeman: New York, NY, USA, 1997. [Google Scholar]
- Bandura, A. Social Foundations of Thought and Action: A Social Cognitive Theory; Prentice Hall: Englewood Cliffs, NJ, USA, 1986. [Google Scholar]
- Elizabeth, E.; Eckstrom, E.; Harmer, P.; Fitzgerald, K.; Voit, J.; Cameron, K.A. Exercise and Fall Prevention: Narrowing the Research-to-Practice Gap and Enhancing Integration of Clinical and Community Practice. J. Am. Geriatr. Soc. 2016, 64, 425–431. [Google Scholar] [CrossRef]
- Harmer, P.A. So much research, so little application: Barriers to dissemination and practical implementation of Tai Ji Quan. J. Sport Heal. Sci. 2014, 3, 16–20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tai Chi for Health Institute. Tai Chi for Arthritis for Fall Prevention. 2018. Available online: https://taichiforhealthinstitute.org/programs/tai-chi-for-fall-prevention/ (accessed on 19 December 2020).
- Tai Chi for Health Institute. Comparing Chen and Sun Styles. 2018. Available online: https://taichiforhealthinstitute.org/comparing-chen-and-sun-styles/ (accessed on 26 December 2020).
- Voukelatos, A.; Cumming, R.G.; Lord, S.R.; Rissel, C. A Randomized, Controlled Trial of tai chi for the Prevention of Falls: The Central Sydney tai chi Trial. J. Am. Geriatr. Soc. 2007, 55, 1185–1191. [Google Scholar] [CrossRef]
- Kempen, G.I.J.M.; Yardley, L.; Van Haastregt, J.C.M.; Zijlstra, G.A.R.; Beyer, N.; Hauer, K.; Todd, C. The Short FES-I: A shortened version of the falls efficacy scale-international to assess fear of falling. Age Ageing 2007, 37, 45–50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Podsiadlo, D.; Richardson, S. The Timed “Up & Go”: A Test of Basic Functional Mobility for Frail Elderly Persons. J. Am. Geriatr. Soc. 1991, 39, 142–148. [Google Scholar] [CrossRef]
- Kohler, A.; Kressig, R.W.; Schindler, C.G.U. Adherence rate in intervention programs for the promotion of physical activity in older adults: A systematic literature review. Praxis 2012, 101, 1535–1547. [Google Scholar] [CrossRef]
- Medley, A.; Thompson, M. Contribution of Age and Balance Confidence to Functional Mobility Test Performance. J. Geriatr. Phys. Ther. 2015, 38, 8–16. [Google Scholar] [CrossRef]
- Manor, B.; Lough, M.; Bs, M.M.G.; Cupples, A.; Wayne, P.M.; Lipsitz, L.A. Functional Benefits of Tai Chi Training in Senior Housing Facilities. J. Am. Geriatr. Soc. 2014, 62, 1484–1489. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mortazavi, H.; Tabatabaeichehr, M.; Golestani, A.; Armat, M.R.; Yousefi, M.R. The Effect of Tai Chi Exercise on the Risk and Fear of Falling in Older Adults: A Randomized Clinical Trial. Mater. Socio Medica 2018, 30, 38–42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tricco, A.C.; Thomas, S.M.; Veroniki, A.A.; Hamid, J.S.; Cogo, E.; Strifler, L.; Khan, P.A.; Robson, R.; Sibley, K.M.; Macdonald, H.; et al. Comparisons of Interventions for Preventing Falls in Older Adults. JAMA 2017, 318, 1687–1699. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Measures | FES-I | TUG | OPQOL | |||
|---|---|---|---|---|---|---|
| Pre | Post | Pre | Post | Pre | Post | |
| Mean (SD) | 15(6.2) | 12(4.3) | 22.4(7.62) | 17.6(7.14) | 54(7.2) | 55(7.3) |
| Range | 7–26 | 7–23 | 12.8–38.2 | 10.7–32.3 | 43–64 | 40–64 |
| Mean Change (absolute, units) | −3 | −5 | +1 | |||
| Mean Change (relative, %) | −20% | −21% | +1.9% | |||
| Pre | Post | |
|---|---|---|
| QOL Score, n (%) | (n = 11) | (n = 11) |
| 1—Very bad | 0 | 0 |
| 2—Bad | 0 | 0 |
| 3—Alright | 3(27%) | 1(10%) |
| 4—Good | 6(55%) | 5(45%) |
| 5—Very Good | 2(18%) | 5(45%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, Y.; Ringdahl, D.; Trelstad-Porter, R.; Gurvich, O.V. Feasibility of Implementing a Tai Chi Program in an Assisted Living Facility: Reducing Fall Risks and Improving Quality of Life. J. Clin. Med. 2021, 10, 1277. https://doi.org/10.3390/jcm10061277
Chen Y, Ringdahl D, Trelstad-Porter R, Gurvich OV. Feasibility of Implementing a Tai Chi Program in an Assisted Living Facility: Reducing Fall Risks and Improving Quality of Life. Journal of Clinical Medicine. 2021; 10(6):1277. https://doi.org/10.3390/jcm10061277
Chicago/Turabian StyleChen, Yingying, Deborah Ringdahl, Rachel Trelstad-Porter, and Olga V. Gurvich. 2021. "Feasibility of Implementing a Tai Chi Program in an Assisted Living Facility: Reducing Fall Risks and Improving Quality of Life" Journal of Clinical Medicine 10, no. 6: 1277. https://doi.org/10.3390/jcm10061277