
Acute Management Should Be Optimized in Patients with Less Specific Stroke Symptoms: Findings from a Retrospective Observational Study


 , ,
, ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
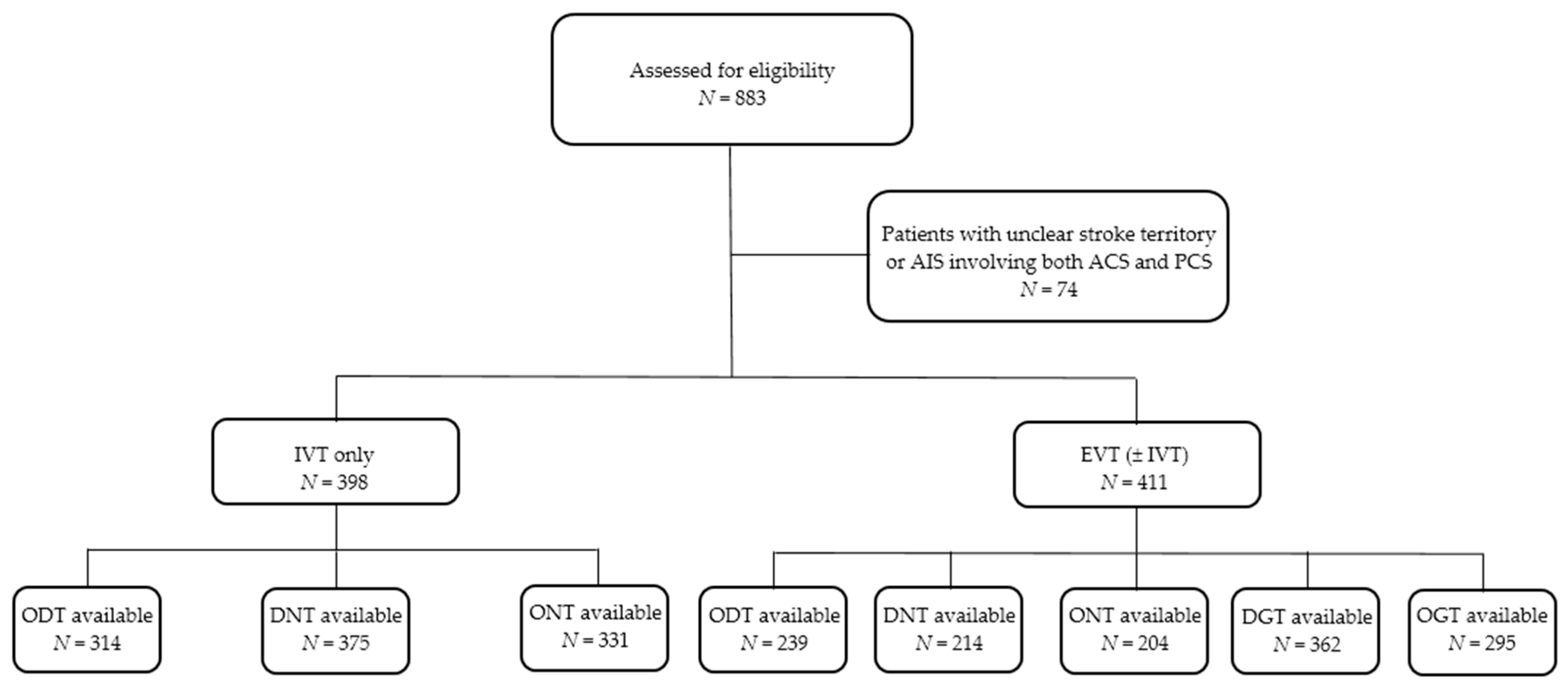
2.1. Data Source and Study Population
2.2. Neuroimaging
2.3. Recanalization Treatment
2.4. Observed Parameters
2.5. Statistical Analysis
2.6. Ethics
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- De Marchis, G.M.; Kohler, A.; Renz, N.; Arnold, M.; Mono, M.L.; Jung, S.; Fischer, U.; Karameshev, A.I.; Brekenfeld, C.; Gralla, J.; et al. Posterior versus anterior circulation strokes: Comparison of clinical, radiological and outcome characteristics. J. Neurol. Neurosurg. Psychiatry 2011, 82, 33–37. [Google Scholar] [CrossRef] [PubMed]
- Dorňák, T.; Herzig, R.; Kuliha, M.; Havlíček, R.; Školoudík, D.; Šaňák, D.; Köcher, M.; Procházka, V.; Lacman, J.; Charvát, F.; et al. Endovascular treatment of acute basilar artery occlusion: Time to treatment is crucial. Clin. Radiol. 2015, 70, e20–e27. [Google Scholar] [CrossRef] [Green Version]
- Zürcher, E.; Richoz, B.; Faouzi, M.; Michel, P. Differences in ischemic anterior and posterior circulation strokes: A clinico-radiological and outcome analysis. J. Stroke Cerebrovasc. Dis. 2019, 28, 710–718. [Google Scholar] [CrossRef] [PubMed]
- Frid, P.; Drake, M.; Giese, A.K.; Wasselius, J.; Schirmer, M.D.; Donahue, K.L.; Cloonan, L.; Irie, R.; Bouts, M.J.R.J.; McIntosh, E.C.; et al. Detailed phenotyping of posterior vs. anterior circulation ischemic stroke: A multi-center MRI study. J. Neurol. 2020, 267, 649–658. [Google Scholar] [CrossRef] [Green Version]
- Tao, W.D.; Liu, M.; Fisher, M.; Wang, D.R.; Li, J.; Furie, K.L.; Hao, Z.L.; Lin, S.; Zhang, C.F.; Zeng, Q.T.; et al. Posterior versus anterior circulation infarction: How different are the neurological deficits? Stroke 2012, 43, 2060–2065. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Emberson, J.; Lees, K.R.; Lyden, P.; Blackwell, L.; Albers, G.; Bluhmki, E.; Brott, T.; Cohen, G.; Davis, S.; Donnan, G.; et al. Effect of treatment delay, age, and stroke severity on the effects of intravenous thrombolysis with alteplase for acute ischaemic stroke: A meta-analysis of individual patient data from randomised trials. Lancet 2014, 384, 1929–1935. [Google Scholar] [CrossRef] [Green Version]
- Saver, J.L.; Goyal, M.; van der Lugt, A.; Menon, B.K.; Majoie, C.B.; Dippel, D.W.; Campbell, B.C.; Nogueira, R.G.; Demchuk, A.M.; Tomasello, A.; et al. Time to treatment with endovascular thrombectomy and outcomes from ischemic stroke: A meta-analysis. JAMA 2016, 316, 1279–1288. [Google Scholar] [CrossRef]
- Sarraj, A.; Medrek, S.; Albright, K.; Martin-Schild, S.; Bibars, W.; Vahidy, F.; Grotta, J.C.; Savitz, S.I. Posterior circulation stroke is associated with prolonged door-to-needle time. Int. J. Stroke 2015, 10, 672–678. [Google Scholar] [CrossRef]
- Baraban, E.; Lucas, L.; Bhatt, A. Initial presenting stroke symptoms impact treatment timeline among ischemic stroke patients [abstract]. Neurology 2018, 90 (Suppl. S15), P4.233. [Google Scholar]
- Goldstein, L.B.; Samsa, G.P. Reliability of the National Institutes of Health Stroke Scale. Extension to non-neurologists in the context of a clinical trial. Stroke 1997, 28, 307–310. [Google Scholar] [CrossRef]
- Krajíčková, D.; Krajina, A.; Herzig, R.; Lojík, M.; Chovanec, V.; Raupach, J.; Vítková, E.; Waishaupt, J.; Vyšata, O.; Vališ, M. Mechanical recanalization in ischemic anterior circulation stroke within an 8-hour time window. A real-world experience. Diagn. Interv. Radiol. 2017, 23, 465–471. [Google Scholar] [CrossRef] [Green Version]
- Campbell, B.C.; Christensen, S.; Levi, C.R.; Desmond, P.M.; Donnan, G.A.; Davis, S.M.; Parsons, M.W. Cerebral blood flow is the optimal CT perfusion parameter for assessing infarct core. Stroke 2011, 42, 3435–3440. [Google Scholar] [CrossRef]
- Jauch, E.C.; Saver, J.L.; Adams, H.P., Jr.; Bruno, A.; Connors, J.J.; Demaerschalk, B.M.; Khatri, P.; McMullan, P.W., Jr.; Qureshi, A.I.; Rosenfield, K.; et al. Guidelines for the early management of patients with acute ischemic stroke: A guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 2013, 44, 870–947. [Google Scholar] [CrossRef] [PubMed]
- Neumann, J.; Tomek, A.; Školoudík, D.; Škoda, O.; Mikulík, R.; Herzig, R.; Václavík, D.; Bar, M.; Šaňák, D. Doporučený postup pro intravenózní trombolýzu v léčbě akutního mozkového infarktu—Verze 2014. Cesk. Slov. Neurol. N. 2014, 77/110, 381–385. [Google Scholar]
- Powers, W.J.; Derdeyn, C.P.; Biller, J.; Coffey, C.S.; Hoh, B.L.; Jauch, E.C.; Johnston, K.C.; Johnston, S.C.; Khalessi, A.A.; Kidwell, C.S.; et al. 2015 American Heart Association/American Stroke Association focused update of the 2013 guidelines for the early management of patients with acute ischemic stroke regarding endovascular treatment: A guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 2015, 46, 3020–3035. [Google Scholar] [CrossRef] [Green Version]
- Šaňák, D.; Neumann, J.; Tomek, A.; Školoudík, D.; Škoda, O.; Mikulík, R.; Herzig, R.; Václavík, D.; Bar, M.; Roček, M.; et al. Doporučení pro rekanalizační léčbu akutního mozkového infarktu—Verze 2016. Cesk. Slov. Neurol. N. 2016, 79/112, 231–234. [Google Scholar] [CrossRef]
- Powers, W.J.; Rabinstein, A.A.; Ackerson, T.; Adeoye, O.M.; Bambakidis, N.C.; Becker, K.; Biller, J.; Brown, M.; Demaerschalk, B.M.; Hoh, B.; et al. 2018 guidelines for the early management of patients with acute ischemic stroke. A guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 2018, 49, e46–e110. [Google Scholar] [CrossRef] [PubMed]
- Sanák, D.; Nosál’, V.; Horák, D.; Bártková, A.; Zelenák, K.; Herzig, R.; Bucil, J.; Skoloudík, D.; Burval, S.; Cisariková, V.; et al. Impact of diffusion-weighted MRI-measured initial cerebral infarction volume on clinical outcome in acute stroke patients with middle cerebral artery occlusion treated by thrombolysis. Neuroradiology 2006, 48, 632–639. [Google Scholar] [CrossRef]
- Ferrari, J.; Knoflach, M.; Seyfang, L.; Lang, W. Austrian Stroke Unit Registry Collaborators. Differences in process management and in-hospital delays in treatment with iv thrombolysis. PLoS ONE 2013, 8, e75378. [Google Scholar] [CrossRef] [Green Version]
- Bhatt, A.; Lesko, A.; Lucas, L.; Kansara, A.; Baraban, E. Patients with low national institutes of health stroke scale scores have longer door-to-needle times: Analysis of a telestroke network. J. Stroke Cerebrovasc. Dis. 2016, 25, 2253–2258. [Google Scholar] [CrossRef]
- Birnbaum, L.A.; Rodriguez, J.S.; Topel, C.H.; Behrouz, R.; Misra, V.; Palacio, S.; Patterson, M.G.; Motz, D.S.; Goros, M.W.; Cornell, J.E.; et al. Older stroke patients with high stroke scores have delayed door-to-needle times. J. Stroke Cerebrovasc. Dis. 2016, 25, 2668–2672. [Google Scholar] [CrossRef] [PubMed]
- Kwei, K.T.; Liang, J.; Wilson, N.; Tuhrim, S.; Dhamoon, M. Stroke severity affects timing: Time from stroke code activation to initial imaging is longer in patients with milder strokes. Neurologist 2018, 23, 79–82. [Google Scholar] [CrossRef]
- Jahan, R.; Saver, J.L.; Schwamm, L.H.; Fonarow, G.C.; Liang, L.; Matsouaka, R.A.; Xian, Y.; Holmes, D.N.; Peterson, E.D.; Yavagal, D.; et al. Association between time to treatment with endovascular reperfusion therapy and outcomes in patients with acute ischemic stroke treated in clinical practice. JAMA 2019, 322, 252–263. [Google Scholar] [CrossRef] [Green Version]
- Sommer, P.; Seyfang, L.; Posekany, A.; Ferrari, J.; Lang, W.; Fertl, E.; Serles, W.; Töll, T.; Kiechl, S.; Greisenegger, S. Prehospital and intra-hospital time delays in posterior circulation stroke: Results from the Austrian Stroke Unit Registry. J. Neurol. 2017, 264, 131–138. [Google Scholar] [CrossRef] [Green Version]
- Varjoranta, T.; Raatiniemi, L.; Majamaa, K.; Martikainen, M.; Liisanantti, J.H. Prehospital and hospital delays for stroke patients treated with thrombolysis: A retrospective study from mixed rural-urban area in Northern Finland. Australas. Emerg. Care 2019, 22, 76–80. [Google Scholar] [CrossRef] [Green Version]
- Mowla, A.; Doyle, J.; Lail, N.S.; Rajabzadeh-Oghaz, H.; Deline, C.; Shirani, P.; Ching, M.; Crumlish, A.; Steck, D.A.; Janicke, D.; et al. Delays in door-to-needle time for acute ischemic stroke in the emergency department: A comprehensive stroke center experience. J. Neurol. Sci. 2017, 376, 102–105. [Google Scholar] [CrossRef]
- Hassan, A.E.; Adil, M.M.; Zacharatos, H.; Rahim, B.; Chaudhry, S.A.; Tekle, W.G.; Qureshi, A.I. Should ischemic stroke patients with aphasia or high National Institutes of Health Stroke Scale score undergo preprocedural intubation and endovascular treatment? J. Stroke Cerebrovasc. Dis. 2014, 23, e299–e304. [Google Scholar] [CrossRef]
- Gulli, G.; Markus, H.S. The use of FAST and ABCD2 scores in posterior circulation, compared with anterior circulation, stroke and transient ischemic attack. J. Neurol. Neurosurg. Psychiatry 2012, 83, 228–229. [Google Scholar] [CrossRef]
- Berglund, A.; von Euler, M.; Schenck-Gustafsson, K.; Castrén, M.; Bohm, K. Identification of stroke during the emergency call: A descriptive study of callers’ presentation of stroke. BMJ Open 2015, 5, e007661. [Google Scholar] [CrossRef] [Green Version]
- Arch, A.E.; Weisman, D.C.; Coca, S.; Nystrom, K.V.; Wira, C.R., III; Schindler, J.L. Missed ischemic stroke diagnosis in the emergency department by emergency medicine and neurology services. Stroke 2016, 47, 668–673. [Google Scholar] [CrossRef] [Green Version]
- Schneck, M.J. Current stroke scales may be partly responsible for worse outcomes in posterior circulation stroke. Stroke 2018, 49, 2565–2566. [Google Scholar] [CrossRef] [PubMed]
- Mikulík, R.; Bunt, L.; Hrdlicka, D.; Dusek, L.; Václavík, D.; Kryza, J. Calling 911 in response to stroke: A nationwide study assessing definitive individual behavior. Stroke 2008, 39, 1844–1849. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nordanstig, A.; Jood, K.; Rosengren, L. Public stroke awareness and intent to call 112 in Sweden. Acta Neurol. Scand. 2014, 130, 400–404. [Google Scholar] [CrossRef] [PubMed]
- Jung, S.; Rosini, J.M.; Nomura, J.T.; Caplan, R.J.; Raser-Schramm, J. Even faster door-to-alteplase times and associated outcomes in acute ischemic stroke. J. Stroke Cerebrovasc. Dis. 2019, 28, 104329. [Google Scholar] [CrossRef] [PubMed]
- Förster, A.; Gass, A.; Kern, R.; Griebe, M.; Hennerici, M.G.; Szabo, K. Thrombolysis in posterior circulation stroke: Stroke subtypes and patterns, complications and outcome. Cerebrovasc. Dis. 2011, 32, 349–353. [Google Scholar] [CrossRef] [PubMed]
- Inoa, V.; Aron, A.W.; Staff, I.; Fortunato, G.; Sansing, L.H. Lower NIH stroke scale scores are required to accurately predict a good prognosis in posterior circulation stroke. Cerebrovasc. Dis. 2014, 37, 251–255. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Characteristic | IVT Only Group | EVT (±IVT) Group | p |
|---|---|---|---|
| N | 398 (49.2) | 411 (50.8) | N/A |
| Age, (years) † | 71.17 ± 12.75 (72.0) | 71.99 ± 12.43 (74.0) | 0.2354 |
| Male sex | 223 (56.0) | 172 (41.8) | 0.0001 |
| NIHSS baseline † | 7.68 ± 5.00 (6.0) | 14.18 ± 6.04 (14.0) | <0.0001 |
| Vascular territory | 0.7798 | ||
| Anterior | 346 (86.9) | 361 (87.8) | |
| Posterior | 52 (13.1) | 50 (12.2) | |
| Clinical symptoms | |||
| Limb weakness (HEMIPAR) | 314 (78.9) | 388 (94.4) | <0.0001 |
| Drooping of the mouth corner (N VII) | 283 (71.1) | 342 (83.2) | 0.0001 |
| Speech difficulties (SPEECH) | 313 (78.6) | 341 (83.0) | 0.1582 |
| Sensory impairment (SENSATION) | 61 (15.3) | 18 (4.4) | <0.0001 |
| Visual problems (VISION) | 28 (7.0) | 14 (3.4) | 0.0363 |
| VERTIGO | 37 (9.3) | 9 (2.2) | 0.0001 |
| HEADACHE | 16 (4.0) | 2 (0.5) | 0.0020 |
| Nausea and/or vomiting (VOMIT) | 29 (7.3) | 9 (2.2) | 0.0015 |
| Loss of consciousness (COMA) | 3 (7.5) | 26 (6.3) | 0.0001 |
| IVT | 398 (100.0) | 253 (61.6) | <0.0001 |
| Time intervals (min) | |||
| Onset-to-door (ODT) † | 97.14 ± 57.35 (80.5) | 105.30 ± 70.82 (85.0) | 0.4089 |
| Onset-to-needle (ONT) † | 143.57 ± 64.99 (135.0) | 125.28 ± 45.51 (119.0) | 0.0005 |
| Door-to-needle (DNT) † | 50.10 ± 21.70 (47.0) | 41.17 ± 17.29 (40.0) | <0.0001 |
| Onset-to-groin (OGT) † | N/A | 207.13 ± 87.35 (185.0) | |
| Door-to-groin (DGT) † | N/A | 75.17 ± 40.74 (73.0) |
| Clinical Symptom | Circulation | p | |
|---|---|---|---|
| ACS (N = 707) | PCS (N = 102) | ||
| Limb weakness (HEMIPAR) | 636 (89.96) | 66 (64.71) | <0.0001 |
| Drooping of the mouth corner (N VII) | 588 (83.17) | 37 (36.27) | <0.0001 |
| Speech difficulties (SPEECH) | 593 (83.88) | 61 (59.8) | <0.0001 |
| Sensory impairment (SENSATION) | 64 (9.05) | 15 (14.71) | 0.105 |
| Visual problems (VISION) | 5 (0.71) | 37 (36.27) | <0.0001 |
| VERTIGO | 2 (0.28) | 44 (43.14) | <0.0001 |
| HEADACHE | 0 (0) | 18 (17.65) | N/A |
| Nausea and/or vomiting (VOMIT) | 1 (0.14) | 37 (36.27) | N/A |
| Loss of consciousness (COMA) | 9 (1.27) | 20 (19.61) | N/A |
| Explanatory Variable (Predictor) | ODT | ONT | DNT | OGT | DGT | |||
|---|---|---|---|---|---|---|---|---|
| IVT Only Group (N = 398) | EVT (±IVT) Group (N = 411) | IVT Only Group (N = 398) | EVT (±IVT) Group (N = 411) | IVT Only Group (N = 398) | EVT (±IVT) Group (N = 411) | EVT (±IVT) Group (N = 411) | EVT (±IVT) Group (N = 411) | |
| Age, (years) | −0.0050 (0.0026); 0.076 | −0.0021 (0.0030); 0.8174 | −0.0034 (0.0022); 0.125 | 0.0025 (0.0019); 0.197 | 6.215 × 10−5 (1.558 × 10−3); 0.968 | 0.0060 (0.0028); 0.0312 | −0.0004 (0.0018); 0.798 | 0.0042 (0.0021); 0.0476 |
| Male sex | −0.00007 (0.0661); 0.999 | −0.2142 (0.0751); 0.0517 | 0.0207 (0.0573); 0.718 | −0.0428 (0.0484); 0.377 | −0.0134 (0.0395); 0.734 | 0.0314 (0.0676); 0.642 | −0.1325 (0.0477); 0.0058 | 0.0275 (0.0553); 0.619 |
| NIHSS baseline | −0.0270 (0.0065); 0.0006 | −0.0111 (0.0068); 0.3363 | −0.0174 (0.0057); 0.0027 | −0.0033 (0.0049); 0.495 | −0.0052 (0.0038); 0.178 | 0.0045 (0.0063); 0.474 | −0.0047 (0.0041); 0.249 | 0.0026 (0.0047); 0.581 |
| Posterior vascular territory | 0.3190 (0.0927); 0.0021 | 0.2141 (0.1325); 0.3363 | 0.284 (0.0808); 0.0005 | 0.1889 (0.0866); 0.0304 | 0.1063 (0.0579); 0.0672 | 0.1701 (0.1277); 0.184 | 0.2232 (0.0791); 0.0051 | 0.1729 (0.0852); 0.0433 |
| Clinical symptoms | ||||||||
| Limb weakness (HEMIPAR) | −0.1927 (0.0785); 0.0271 | −0.0868 (0.1662); 0.8278 | −0.1673 (0.0681); 0.0146 | −0.1384 (0.1328); 0.298 | −0.0655 (0.0479); 0.173 | 0.0930 (0.1680); 0.58 | −0.2052 (0.1081); 0.0585 | −0.1231 (0.1217); 0.312 |
| Drooping of the mouth corner (N VII) | −0.1554 (0.0712); 0.0486 | −0.1816 (0.1060); 0.3363 | −0.1619 (0.0619); 0.0093 | −0.1678 (0.0694); 0.0165 | −0.0669 (0.0431); 0.122 | −0.1952 (0.0976); 0.0469 | −0.0674 (0.0640); 0.293 | −0.2539 (0.0763); 0.0009 |
| Speech difficulties (SPEECH) | −0.2164 (0.0758); 0.0100 | 0.0069 (0.1155); 0.9530 | −0.2275 (0.0662); 0.0006 | −0.0366 (0.0714); 0.609 | −0.1063 (0.0471); 0.0247 | −0.0525 (0.1000); 0.6 | −0.0752 (0.0675); 0.266 | −0.099 (0.0767); 0.198 |
| Sensory impairment (SENSATION) | 0.0039 (0.0887); 0.9990 | 0.4925 (0.1955); 0.0909 | 0.0624 (0.0781); 0.424 | −0.0707 (0.1121); 0.529 | −0.0197 (0.0538); 0.715 | 0.0250 (0.2233); 0.911 | 0.2102 (0.1080); 0.0526 | −0.1226 (0.1248); 0.327 |
| Visual problems (VISION) | 0.3724 (0.1180); 0.0046 | 0.2739 (0.2404); 0.5632 | 0.2694 (0.1039); 0.0099 | 0.1271 (0.1565); 0.418 | 0.0840 (0.0757); 0.268 | −0.0596 (0.2491); 0.811 | 0.2008 (0.1466); 0.172 | 0.2197 (0.1513); 0.148 |
| VERTIGO | 0.37064 (0.1037); 0.0019 | 0.3421 (0.2625); 0.5335 | 0.3434 (0.0923); 0.0002 | −0.0913 (0.1746); 0.602 | 0.1410 (0.0661); 0.0337 | 0.2770 (0.2484); 0.266 | 0.1908 (0.1688); 0.259 | 0.1165 (0.1744); 0.504 |
| HEADACHE | 0.2488 (0.1623); 0.1638 | −0.1691 (0.5841); 0.8939 | 0.238 (0.1447); 0.101 | −0.1183 (0.3468); 0.733 | 0.0359 (0.0970); 0.711 | −0.2124 (0.4945); 0.668 | −0.3638 (0.4105); 0.376 | 0.0696 (0.3666); 0.85 |
| Nausea and/or 666 vomiting (VOMIT) | 0.4029 (0.1135); 0.0019 | 0.1496 (0.2408); 0.8278 | 0.357 (0.1012); 0.0004 | 0.3517 (0.1547); 0.0241 | 0.1181 (0.0731); 0.107 | 0.1613 (0.2041); 0.43 | 0.0456 (0.1692); 0.787 | 0.2319 (0.1844); 0.209 |
| Loss of consciousness (COMA) | −0.2572 (0.4077); 0.6252 | −0.0876 (0.1662); 0.8278 | 0.0447 (0.3643); 0.902 | 0.2309 (0.1237); 0.0636 | 0.3891 (0.2192); 0.0767 | 0.4960 (0.1745); 0.0049 | 0.1814 (0.0992); 0.0685 | 0.2670 (0.1181); 0.0244 |
| Occlusion | ||||||||
| ICAe | N/A | −0.0803 (0.1091); 0.8174 | N/A | −0.0622 (0.0692); 0.37 | N/A | −0.0011 (0.0971); 0.991 | −0.0035 (0.0713); 0.96 | −0.1015 (0.0865); 0.242 |
| ICAi | N/A | −0.0085 (0.0991); 0.9530 | N/A | −0.0300 (0.0657); 0.648 | N/A | 0.0887 (0.0880); 0.315 | −0.0481 (0.0657); 0.465 | 0.0743 (0.0740); 0.315 |
| MCA/M1 | N/A | −0.0175 (0.0860); 0.9229 | N/A | −0.1082 (0.0554); 0.0524 | N/A | −0.0994 (0.0789); 0.209 | −0.1132 (0.0533); 0.0346 | −0.1206 (0.0608); 0.0481 |
| MCA/M2 | N/A | −0.1073 (0.1091); 0.654 | N/A | 0.0470 (0.0703); 0.504 | N/A | 0.0536 (0.1000); 0.593 | −0.0132 (0.0690); 0.848 | 0.0660 (0.0815); 0.418 |
| ACA | N/A | −0.3067 (0.2627); 0.5632 | N/A | −0.2934 (0.1736); 0.0925 | N/A | 0.1950 (0.2229); 0.383 | −0.1851 (0.1689); 0.274 | 0.0331 (0.1848); 0.858 |
| PCA | N/A | 0.0849 (0.2410); 0.8861 | N/A | 0.3438 (0.1548); 0.0275 | N/A | 0.2230 (0.2228); 0.318 | 0.1866 (0.1565); 0.234 | 0.2837 (0.1576); 0.0727 |
| VA | N/A | −0.1268 (0.2938); 0.8632 | N/A | 0.0970 (0.1565); 0.536 | N/A | 0.4025 (0.2476); 0.106 | 0.0744 (0.1691); 0.66 | 0.1508 (0.1656); 0.363 |
| BA | N/A | 0.3080 (0.1542); 0.2580 | N/A | 0.1902 (0.1114); 0.0894 | N/A | 0.0554 (0.1598); 0.729 | 0.2578 (0.0916); 0.0052 | 0.1518 (0.1049); 0.149 |
| IVT | N/A | −0.4410 (0.0798); <0.0001 | N/A | N/A | N/A | N/A | −0.0089 (0.0518); 0.863 | −0.1019 (0.0572); 0.0757 |
| Patient Group | Observed Time Interval (Outcome) | Explanatory Variable (Predictor) | Beta | Standard Error | p |
|---|---|---|---|---|---|
| IVT only | Onset-to-door time (ODT) | NIHSS | −1.741 | 0.687 | 0.0118 |
| Limb weakness (HEMIPAR) | −12.608 | 8.161 | 0.1233 | ||
| Speech difficulties (SPEECH) | −18.927 | 7.619 | 0.0135 | ||
| Nausea and/or vomiting (VOMIT) | 31.159 | 11.748 | 0.0084 | ||
| Onset-to-needle time (ONT) | NIHSS | −1.5934 | 0.7575 | 0.036 | |
| Limb weakness (HEMIPAR) | −15.0672 | 8.9026 | 0.092 | ||
| Speech difficulties (SPEECH) | −24.564 | 8.4185 | 0.004 | ||
| Nausea and/or vomiting (VOMIT) | 43.7237 | 13.1284 | 0.001 | ||
| Door-to-needle time (DNT) | Speech difficulties (SPEECH) | −5.163 | 2.737 | 0.060 | |
| VERTIGO | 8.575 | 3.84 | 0.026 | ||
| EVT (±IVT) | Onset-to-needle time (ONT) | Vascular territory—anterior | −24.76 | 12.99 | 0.058 |
| Drooping of the mouth corner (N VII) | −15.76 | 10.43 | 0.132 | ||
| Door-to-needle time (DNT) | Loss of consciousness (COMA) | 22.675 | 6.046 | 0.0002 | |
| Onset-to-groin time (OGT) | Vascular territory—anterior | −47.32 | 16.89 | 0.005 | |
| Door-to-groin time (DGT) | Drooping of the mouth corner (N VII) | −20.794 | 6.015 | 0.0006 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Halúsková, S.; Herzig, R.; Krajíčková, D.; Hamza, A.; Krajina, A.; Chovanec, V.; Lojík, M.; Raupach, J.; Renc, O.; Šimůnek, L.; et al. Acute Management Should Be Optimized in Patients with Less Specific Stroke Symptoms: Findings from a Retrospective Observational Study. J. Clin. Med. 2021, 10, 1143. https://doi.org/10.3390/jcm10051143
Halúsková S, Herzig R, Krajíčková D, Hamza A, Krajina A, Chovanec V, Lojík M, Raupach J, Renc O, Šimůnek L, et al. Acute Management Should Be Optimized in Patients with Less Specific Stroke Symptoms: Findings from a Retrospective Observational Study. Journal of Clinical Medicine. 2021; 10(5):1143. https://doi.org/10.3390/jcm10051143
Chicago/Turabian StyleHalúsková, Simona, Roman Herzig, Dagmar Krajíčková, Abduljabar Hamza, Antonín Krajina, Vendelín Chovanec, Miroslav Lojík, Jan Raupach, Ondřej Renc, Libor Šimůnek, and et al. 2021. "Acute Management Should Be Optimized in Patients with Less Specific Stroke Symptoms: Findings from a Retrospective Observational Study" Journal of Clinical Medicine 10, no. 5: 1143. https://doi.org/10.3390/jcm10051143