
Efficacy of Surgery for the Treatment of Gastric Cancer Liver Metastases: A Systematic Review of the Literature and Meta-Analysis of Prognostic Factors

 , , ,
, , ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Criteria for Considering Studies for This Review
2.1.1. Type of Studies
2.1.2. Type of Participants
2.1.3. Type of Interventions and Outcomes
2.2. Search Methods for Identification of Studies
2.2.1. Electronic Searches
2.2.2. Searching Other Resources
2.3. Data Collection and Analysis
Study Selection
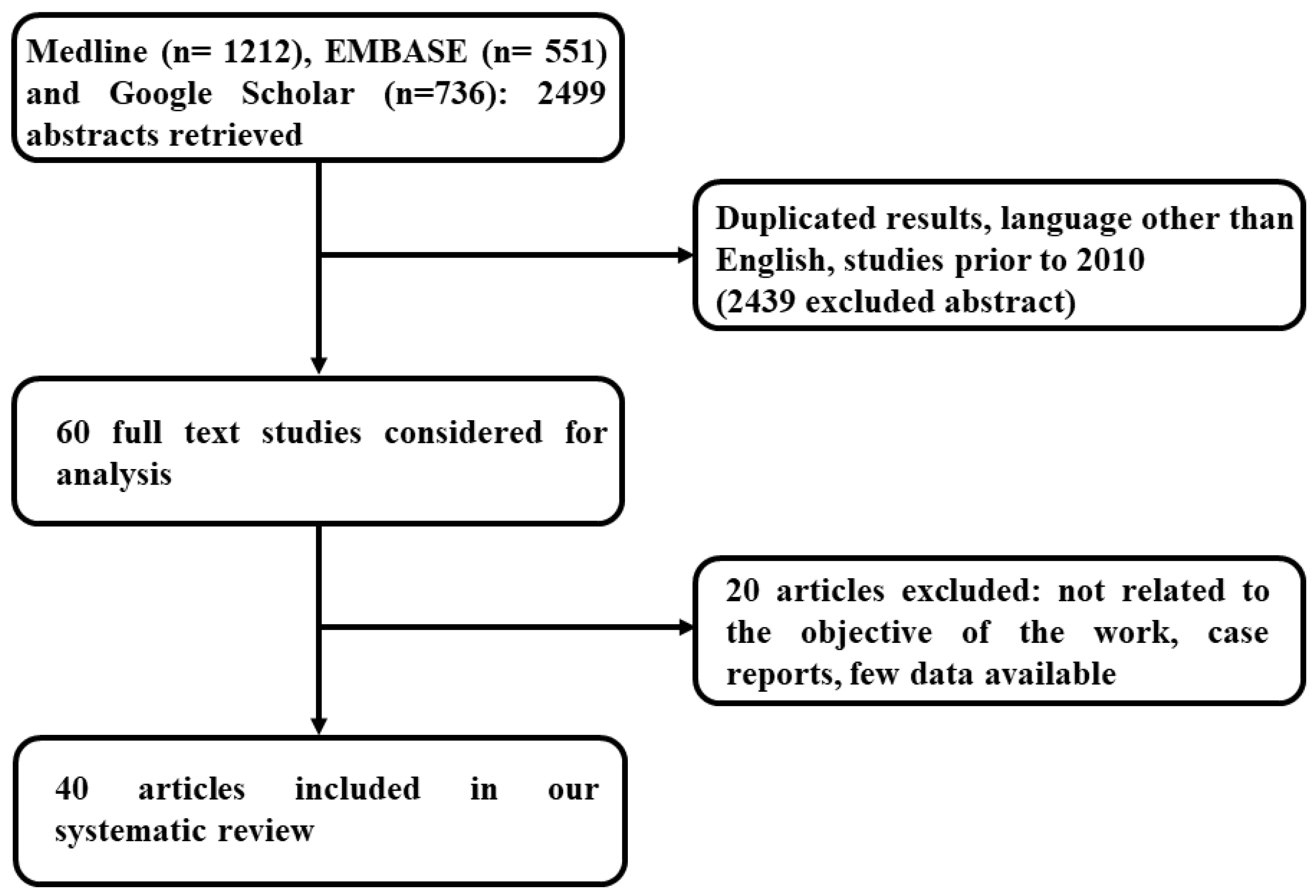
2.4. Literature Search
2.4.1. Data Extraction and Management
- Year of publication.
- Country of recruitment.
- Study interval (year(s) in which the trial was conducted).
- Inclusion and exclusion criteria.
- Population details, such as age, sex, characteristics of the primary tumor, and liver metastases.
- Outcomes (mentioned in ‘Type of interventions and outcomes’).
- Details of the prognostic factor(s).
2.4.2. Assessment of Risk of Bias in Included Studies
2.4.3. Data Synthesis
2.4.4. Subgroup Analysis
3. Results
3.1. Characteristics of the Included Studies
3.2. Characteristics of the Excluded Studies, Risk of Bias, and Applicability Concerns
3.3. Discrimination Results
3.3.1. Morbidity and Mortality
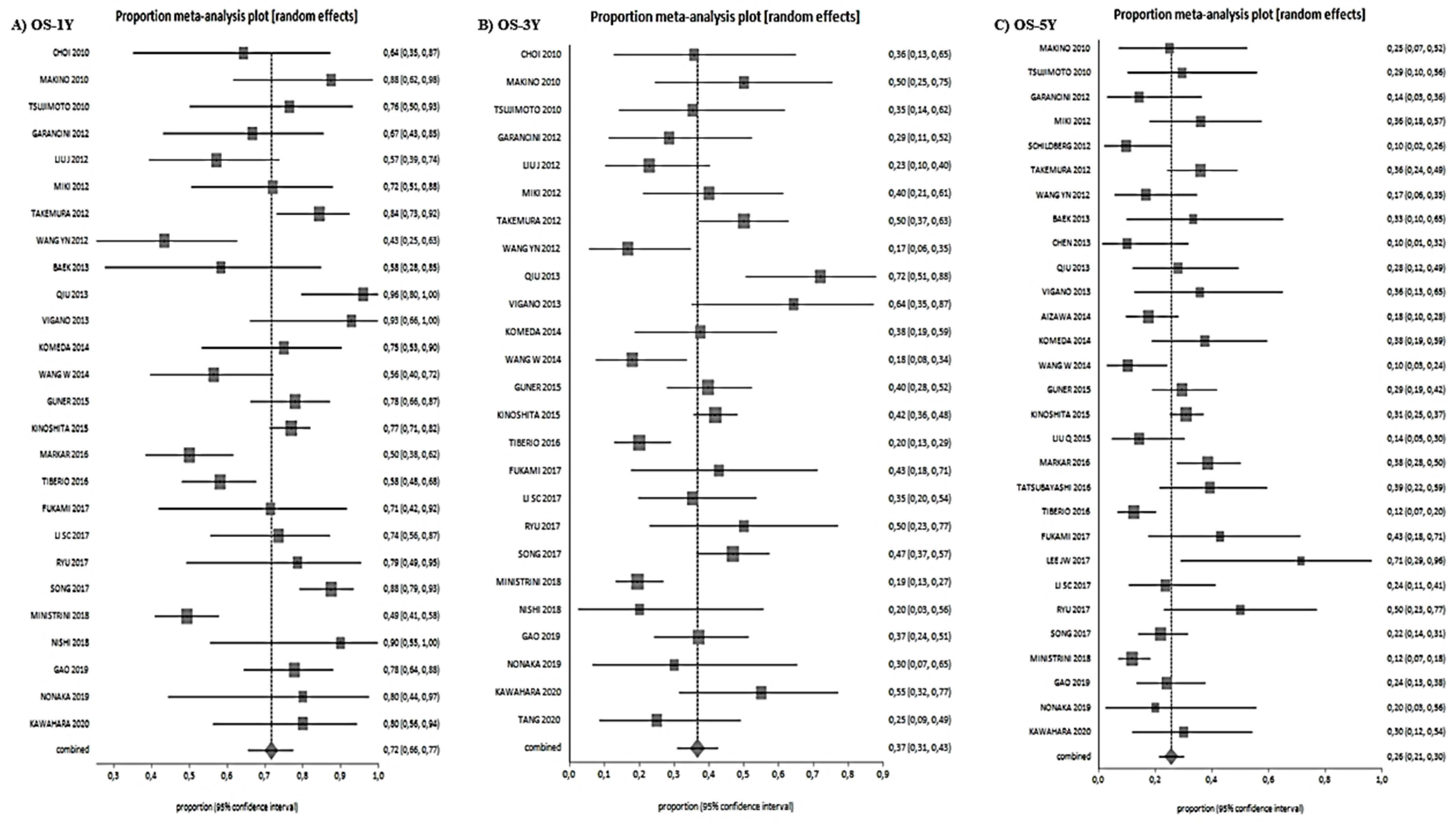
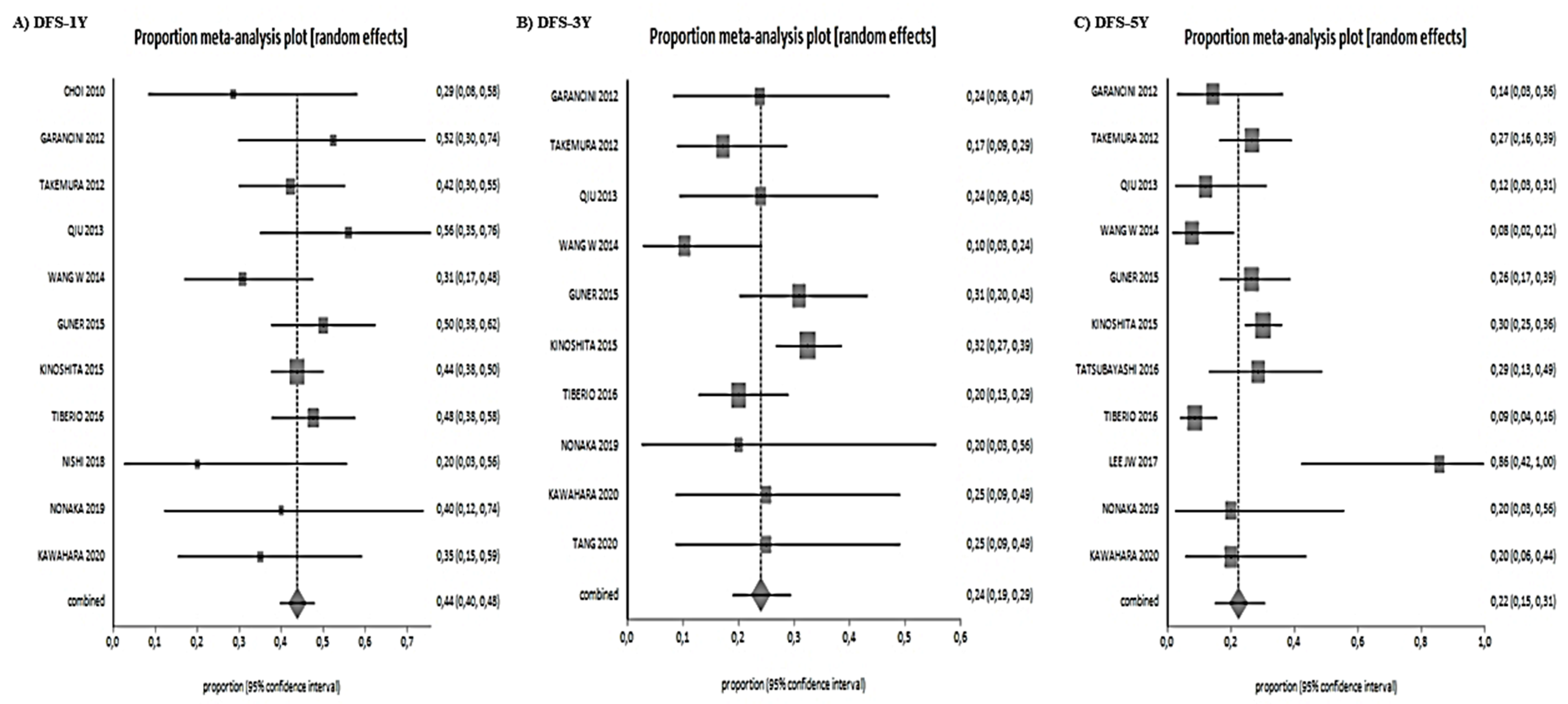
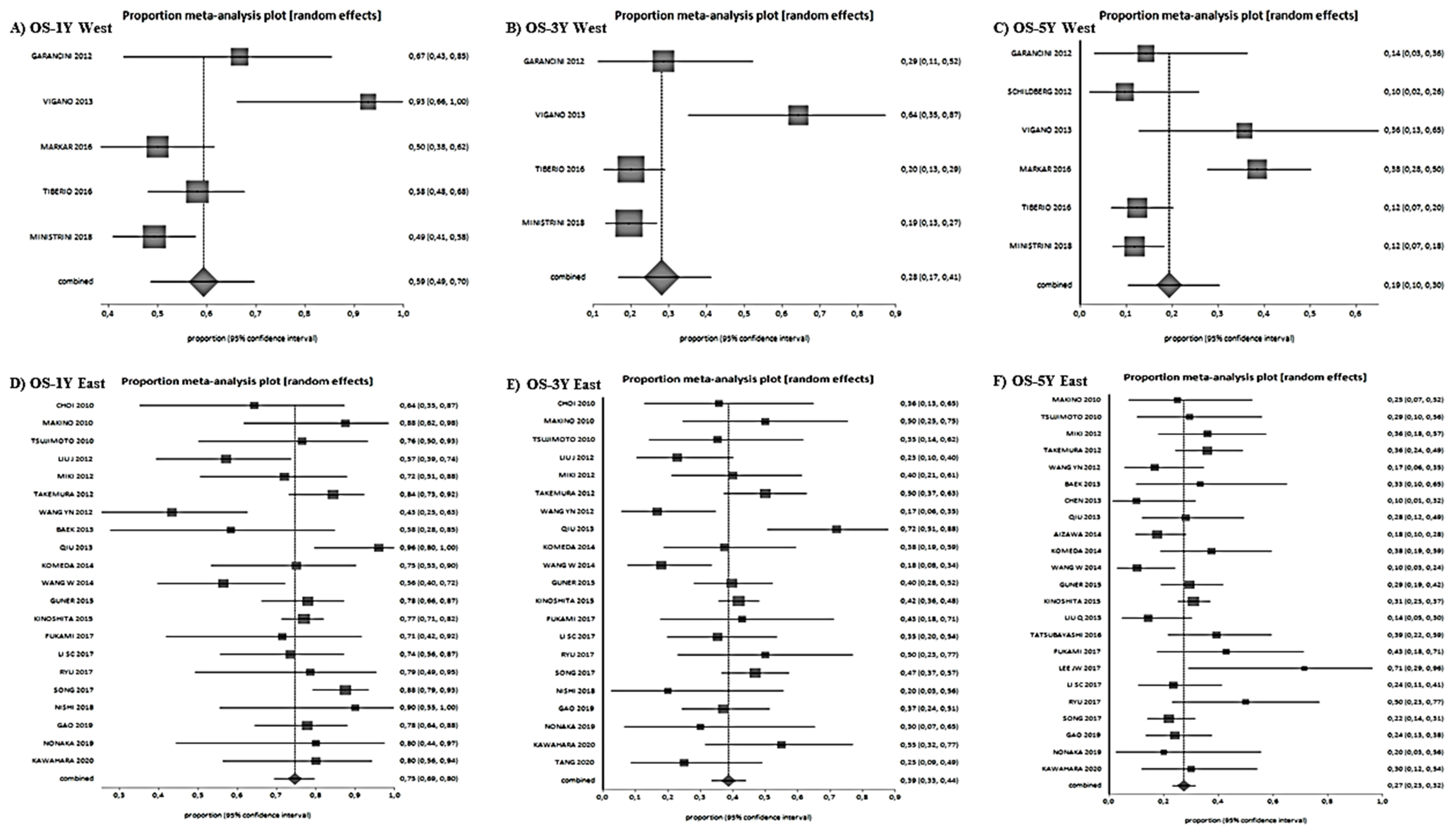
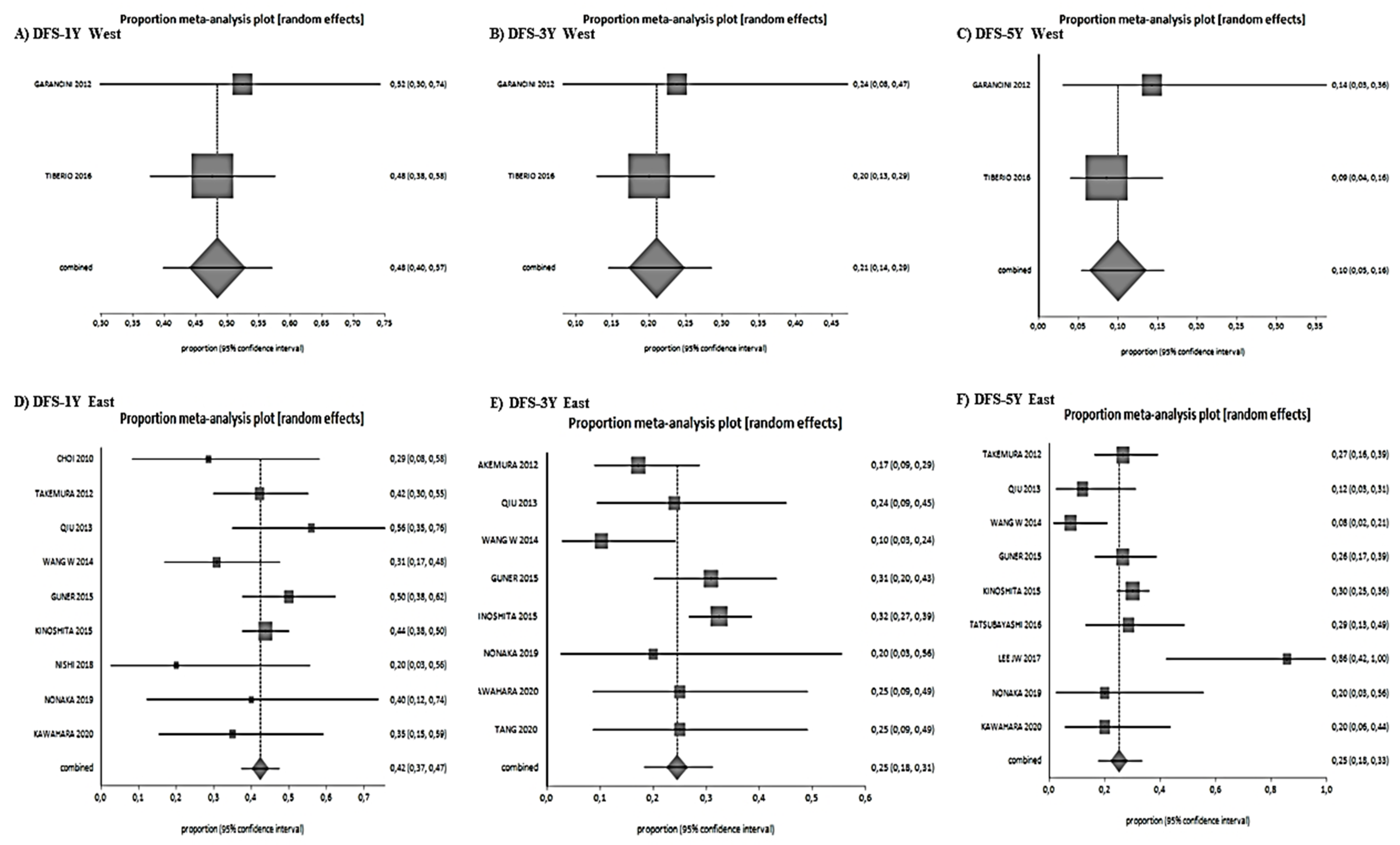
3.3.2. Survival Data
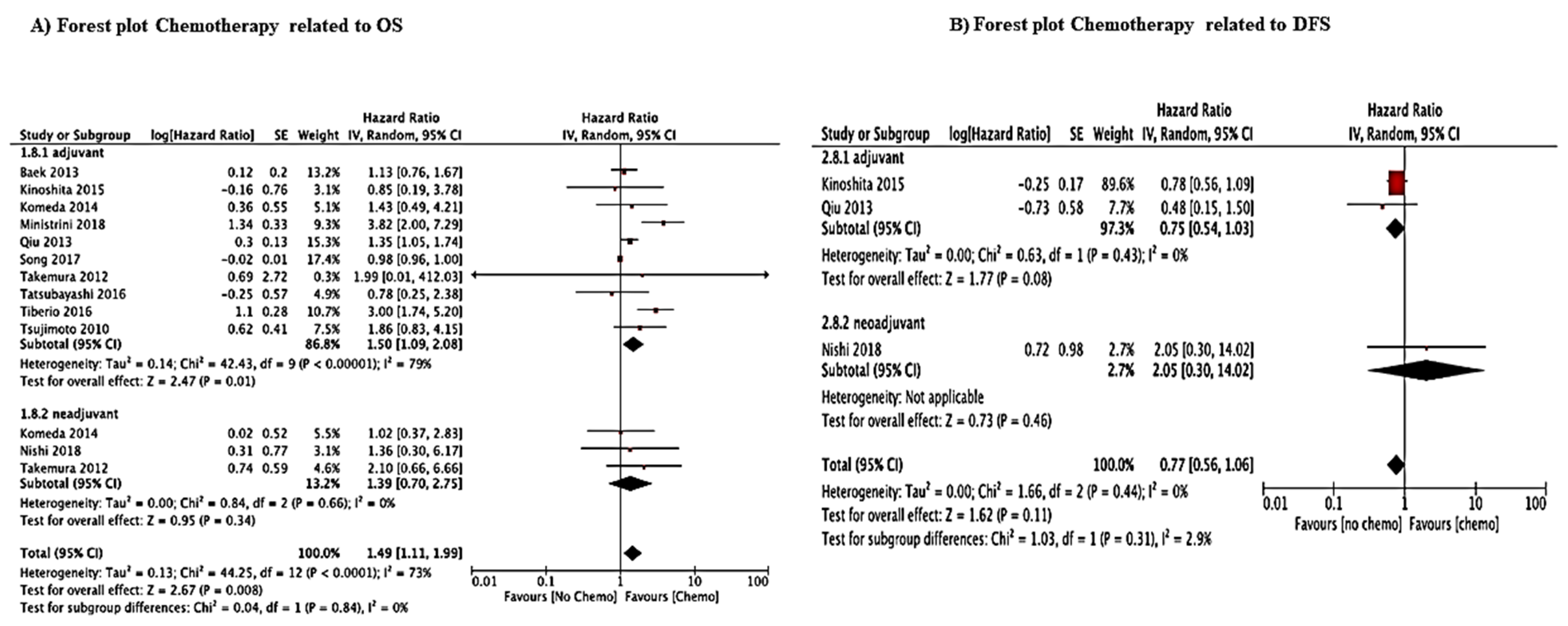
3.3.3. Analysis of Prognostic Factors
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Ferlay, J.; Shin, H.-R.; Bray, F.; Forman, D.; Mathers, C.; Parkin, D.M. Estimates of worldwide burden of cancer in 2008: GLOBOCAN 2008. Int. J. Cancer 2010, 127, 2893–2917. [Google Scholar] [CrossRef] [PubMed]
- Riihimäki, M.; Hemminki, A.; Sundquist, K.; Sundquist, J.; Hemminki, K. Metastatic spread in patients with gastric cancer. Oncotarget 2016, 7, 52307–52316. [Google Scholar] [CrossRef] [Green Version]
- Ajani, J.A.; D’Amico, T.A.; Almhanna, K.; Bentrem, D.J.; Chao, J.; Das, P.; Denlinger, C.S.; Fanta, P.; Farjah, F.; Fuchs, C.S.; et al. Gastric Cancer, Version 3.2016; Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. 2016, 14, 1286–1312. [Google Scholar] [CrossRef] [PubMed]
- Bang, Y.-J.; Van Cutsem, E.; Feyereislova, A.; Chung, H.C.; Shen, L.; Sawaki, A.; Lordick, F.; Ohtsu, A.; Omuro, Y.; Satoh, T.; et al. Trastuzumab in combination with chemotherapy versus chemotherapy alone for treatment of HER2-positive advanced gastric or gastro-oesophageal junction cancer (ToGA): A phase 3, open-label, randomised controlled trial. Lancet 2010, 376, 687–697. [Google Scholar] [CrossRef]
- Smyth, E.C.; Verheij, M.; Allum, W.; Cunningham, D.; Cervantes, A.; Arnold, D. Gastric cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2016, 27, v38–v49. [Google Scholar] [CrossRef]
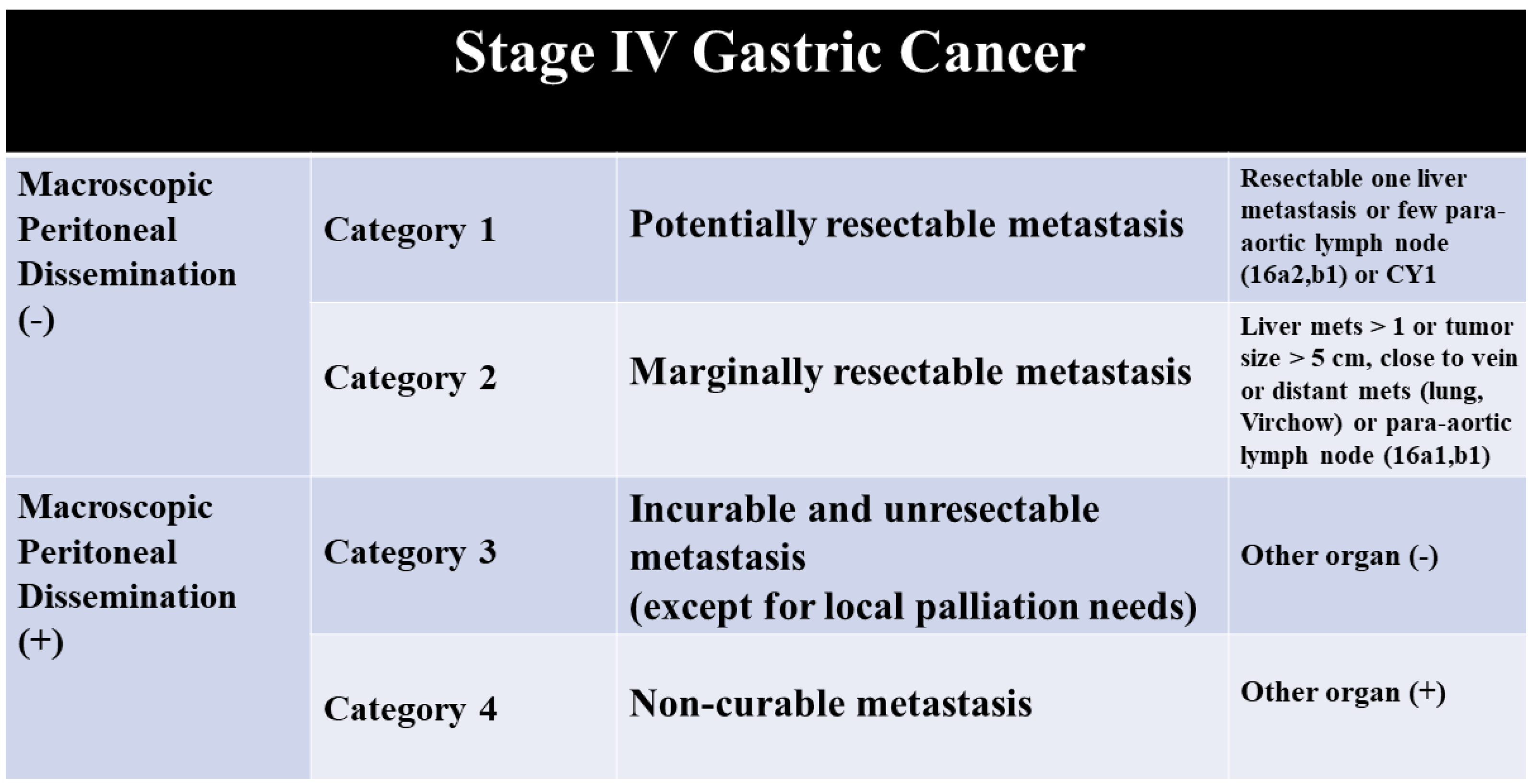
- Yoshida, K.; Yamaguchi, K.; Okumura, N.; Tanahashi, T.; Kodera, Y. Is conversion therapy possible in stage IV gastric cancer: The proposal of new biological categories of classification. Gastric Cancer 2015, 19, 329–338. [Google Scholar] [CrossRef] [Green Version]
- Kodera, Y.; Fujitani, K.; Fukushima, N.; Ito, S.; Muro, K.; Ohashi, N.; Yoshikawa, T.; Kobayashi, D.; Tanaka, C.; Fujiwara, M. Surgical resection of hepatic metastasis from gastric cancer: A review and new recommendation in the Japanese gastric cancer treatment guidelines. Gastric Cancer 2013, 17, 206–212. [Google Scholar] [CrossRef]
- Tiberio, G.; Ministrini, S.; Gardini, A.; Marrelli, D.; Marchet, A.; Cipollari, C.; Graziosi, L.; Pedrazzani, C.; Baiocchi, G.; La Barba, G.; et al. Factors influencing survival after hepatectomy for metastases from gastric cancer. Eur. J. Surg. Oncol. 2016, 42, 1229–1235. [Google Scholar] [CrossRef] [PubMed]
- Gadde, R.; Tamariz, L.; Hanna, M.; Avisar, E.; Livingstone, A.; Franceschi, D.; Yakoub, D. Metastatic gastric cancer (MGC) patients: Can we improve survival by metastasectomy? A systematic review and meta-analysis. J. Surg. Oncol. 2015, 112, 38–45. [Google Scholar] [CrossRef]
- Booth, A.; Clarke, M.; Dooley, G.; Ghersi, D.; Moher, D.; Petticrew, M.; Stewart, L. The nuts and bolts of PROSPERO: An international prospective register of systematic reviews. Syst. Rev. 2012, 1, 2. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. For the PRISMA Group Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, b2535. [Google Scholar] [CrossRef] [Green Version]
- University of Oxford. OCEBM Levels of Evidence Working Group, “The Oxford Levels of Evidence 1”; University of Oxford: Oxford, UK, 2009. [Google Scholar]
- Freemantle, N. CD: StatsDirect—Statistical Software for Medical Research in the 21st Century. BMJ 2000, 321, 1536. [Google Scholar] [CrossRef]
- The Cochrane Collaboration. Review Manager (RevMan) [Computer Program], version 5.3; Nordic Cochrane Centre: Copenhagen, Denmark, 2014. [Google Scholar]
- Parmar, M.K.B.; Torri, V.; Stewart, L. Extracting Summary Statistics to Perform Meta-Analyses of the Published Literature for Survival Endpoints. Stat. Med. 1998, 17, 2815–2834. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef]
- StatsDirect. StatsDirect Statistical Software. 2008. Available online: www.statsdirect.com (accessed on 26 November 2020).
- Makino, H.; Kunisaki, C.; Izumisawa, Y.; Tokuhisa, M.; Oshima, T.; Nagano, Y.; Fujii, S.; Kimura, J.; Takagawa, R.; Kosaka, T.; et al. Indication for hepatic resection in the treatment of liver metastasis from gastric cancer. Anticancer Res. 2010, 30, 2367–2376. [Google Scholar] [PubMed]
- TsujimotoTakashi, H.; Ichikura, T.; Ono, S.; Sugasawa, H.; Hiraki, S.; Sakamoto, N.; Yaguchi, Y.; Hatsuse, K.; Yamamoto, J.; Hase, K. Outcomes for patients following hepatic resection of metastatic tumors from gastric cancer. Hepatol. Int. 2010, 4, 406–413. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, L.; Song, M.-Q.; Lin, H.-Z.; Hao, L.-H.; Jiang, X.-J.; Li, Z.-Y.; Chen, Y.-X. Chemotherapy and resection for gastric cancer with synchronous liver metastases. World J. Gastroenterol. 2013, 19, 2097–2103. [Google Scholar] [CrossRef] [PubMed]
- Qiu, J.-L.; Deng, M.-G.; Li, W.; Zou, R.-H.; Li, B.-K.; Zheng, Y.; Lao, X.-M.; Zhou, K.; Yuan, Y.-F. Hepatic resection for synchronous hepatic metastasis from gastric cancer. Eur. J. Surg. Oncol. 2013, 39, 694–700. [Google Scholar] [CrossRef] [PubMed]
- Viganò, L.; Vellone, M.; Ferrero, A.; Giuliante, F.; Nuzzo, G.; Capussotti, L. Liver resection for gastric cancer metastases. Hepato Gastroenterol. 2013, 60, 557–562. [Google Scholar]
- Aizawa, M.; Nashimoto, A.; Yabusaki, H.; Nakagawa, S.; Matsuki, A. Clinical benefit of surgical management for gastric cancer with synchronous liver metastasis. Hepato Gastroenterol. 2014, 61, 1439–1445. [Google Scholar] [CrossRef]
- Komeda, K.; Hayashi, M.; Kubo, S.; Nagano, H.; Nakai, T.; Kaibori, M.; Wada, H.; Takemura, S.; Kinoshita, M.; Koga, C.; et al. High Survival in Patients Operated for Small Isolated Liver Metastases from Gastric Cancer: A Multi-institutional Study. World J. Surg. 2014, 38, 2692–2697. [Google Scholar] [CrossRef]
- Wang, W.; Liang, H.; Zhang, H.; Wang, X.; Xue, Q.; Zhang, R. Prognostic significance of radical surgical treatment for gastric cancer patients with synchronous liver metastases. Med. Oncol. 2014, 31, 258. [Google Scholar] [CrossRef] [PubMed]
- Guner, A.; Son, T.; Cho, I.; Kwon, I.G.; An, J.Y.; Kim, H.-I.; Cheong, J.-H.; Noh, S.H.; Hyung, W.J. Liver-directed treatments for liver metastasis from gastric adenocarcinoma: Comparison between liver resection and radiofrequency ablation. Gastric Cancer 2016, 19, 951–960. [Google Scholar] [CrossRef] [PubMed]
- Kinoshita, T.; Saiura, A.; Esaki, M.; Sakamoto, H.; Yamanaka, T. Multicentre analysis of long-term outcome after surgical resection for gastric cancer liver metastases. BJS 2014, 102, 102–107. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Fan, B.; Shan, F.; Tang, L.; Bu, Z.; Wu, A.; Zhang, L.; Wu, X.; Zong, X.; Li, S.; et al. Gastrectomy in comprehensive treatment of advanced gastric cancer with synchronous liver metastasis: A prospectively comparative study. World J. Surg. Oncol. 2015, 13, 212. [Google Scholar] [CrossRef] [Green Version]
- Liu, Q.; Bi, J.-J.; Tian, Y.-T.; Feng, Q.; Zheng, Z.-X.; Wang, Z. Outcome after Simultaneous Resection of Gastric Primary Tumour and Synchronous Liver Metastases: Survival Analysis of a Single-center Experience in China. Asian Pac. J. Cancer Prev. 2015, 16, 1665–1669. [Google Scholar] [CrossRef] [Green Version]
- Dittmar, Y.; Altendorf-Hofmann, A.; Rauchfuss, F.; Götz, M.; Scheuerlein, H.; Jandt, K.; Settmacher, U. Resection of liver metastases is beneficial in patients with gastric cancer: Report on 15 cases and review of literature. Gastric Cancer 2011, 15, 131–136. [Google Scholar] [CrossRef] [Green Version]
- Ohkura, Y.; Shinohara, H.; Haruta, S.; Ueno, M.; Hashimoto, M.; Sakai, Y.; Udagawa, H. Hepatectomy Offers Superior Survival Compared with Non-surgical Treatment for ≤3 Metastatic Tumors with Diameters. World J. Surg. 2015, 39, 2757–2763. [Google Scholar] [CrossRef]
- Shinohara, T.; Maeda, Y.; Hamada, T.; Futakawa, N. Survival Benefit of Surgical Treatment for Liver Metastases from Gastric Cancer. J. Gastrointest. Surg. 2015, 19, 1043–1051. [Google Scholar] [CrossRef] [PubMed]
- Markar, S.R.; MacKenzie, H.; Mikhail, S.; Mughal, M.; Preston, S.R.; Maynard, N.D.; Faiz, O.; Hanna, G.B. Surgical resection of hepatic metastases from gastric cancer: Outcomes from national series in England. Gastric Cancer 2017, 20, 379–386. [Google Scholar] [CrossRef] [Green Version]
- Oguro, S.; Imamura, H.; Yoshimoto, J.; Ishizaki, Y.; Kawasaki, S. Liver metastases from gastric cancer represent systemic disease in comparison with those from colorectal cancer. J. Hepato Biliary Pancreat. Sci. 2016, 23, 324–332. [Google Scholar] [CrossRef] [PubMed]
- Tatsubayashi, T.; Tanizawa, Y.; Miki, Y.; Tokunaga, M.; Bando, E.; Kawamura, T.; Sugiura, T.; Kinugasa, Y.; Uesaka, K.; Terashima, M. Treatment outcomes of hepatectomy for liver metastases of gastric cancer diagnosed using contrast-enhanced magnetic resonance imaging. Gastric Cancer 2017, 20, 387–393. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fukami, Y.; Kaneoka, Y.; Maeda, A.; Takayama, Y.; Takahashi, T.; Uji, M.; Kumada, T. Adjuvant hepatic artery infusion chemotherapy after hemihepatectomy for gastric cancer liver metastases. Int. J. Surg. 2017, 46, 79–84. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.W.; Choi, M.H.; Lee, Y.J.; Ali, B.; Yoo, H.M.; Song, K.Y.; Park, C.H. Radiofrequency ablation for liver metastases in patients with gastric cancer as an alternative to hepatic resection. BMC Cancer 2017, 17, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, J.; Xi, H.; Cui, J.; Zhang, K.; Gao, Y.; Liang, W.; Cai, A.; Wei, B.; Chen, L. Minimally invasive surgery as a treatment option for gastric cancer with liver metastasis: A comparison with open surgery. Surg. Endosc. 2017, 32, 1422–1433. [Google Scholar] [CrossRef] [PubMed]
- Li, S.C.; Lee, C.H.; Hung, C.L.; Wu, J.C.; Chen, J.H. Surgical resection of metachronous hepatic metastases from gastric cancer improves long-term survival: A population-based study. PLoS ONE 2017, 12, e0182255. [Google Scholar] [CrossRef]
- Ryu, T.; Takami, Y.; Wada, Y.; Tateishi, M.; Matsushima, H.; Yoshitomi, M.; Saitsu, H. Oncological outcomes after hepatic resection and/or surgical microwave ablation for liver metastasis from gastric cancer. Asian J. Surg. 2019, 42, 100–105. [Google Scholar] [CrossRef]
- Garancini, M.; Uggeri, F.; Degrate, L.; Nespoli, L.; Gianotti, L.; Nespoli, A.; Uggeri, F.; Romano, F. Surgical treatment of liver metastases of gastric cancer: Is local treatment in a systemic disease worthwhile? HPB 2012, 14, 209–215. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Song, A.; Zhang, X.; Yu, F.; Li, D.; Shao, W.; Zhou, Y. Surgical resection for hepatic metastasis from gastric cancer: A multi-institution study. Oncotarget 2017, 8, 71147–71153. [Google Scholar] [CrossRef] [Green Version]
- Ministrini, S.; Solaini, L.; Cipollari, C.; Sofia, S.; Marino, E.; D’Ignazio, A.; Bencivenga, M.; Tiberio, G.A.M. Surgical treatment of hepatic metastases from gastric cancer. Updates Surg. 2018, 70, 273–278. [Google Scholar] [CrossRef] [PubMed]
- Nishi, M.; Shimada, M.; Yoshikawa, K.; Higashijima, J.; Tokunaga, T.; Kashihara, H.; Takasu, C.; Ishikawa, D.; Wada, Y.; Eto, S. Results of Hepatic Resection for Liver Metastasis of Gastric Cancer—A single center experience. J. Med. Investig. 2018, 65, 27–31. [Google Scholar] [CrossRef] [Green Version]
- Shirasu, H.; Tsushima, T.; Kawahira, M.; Kawai, S.; Kawakami, T.; Kito, Y.; Yoshida, Y.; Hamauchi, S.; Todaka, A.; Yokota, T.; et al. Role of hepatectomy in gastric cancer with multiple liver-limited metastases. Gastric Cancer 2017, 21, 338–344. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gao, J.; Wang, Y.; Li, F.; Zhu, Z.; Han, B.; Wang, R.; Xie, R.; Xue, Y. Prognostic Nutritional Index and Neutrophil-to-Lymphocyte Ratio Are Respectively Associated with Prognosis of Gastric Cancer with Liver Metatasis Undergoing and without Hepatectomy. BioMed Res. Int. 2019, 2019, 4213623–4213627. [Google Scholar] [CrossRef] [PubMed]
- Nonaka, Y.; Hiramatsu, K.; Kato, T.; Shibata, Y.; Yoshihara, M.; Aoba, T.; Kamiya, T. Evaluation of Hepatic Resection in Liver Metastasis of Gastric Cancer. Indian J. Surg. Oncol. 2019, 10, 204–209. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kawahara, K.; Makino, H.; Kametaka, H.; Hoshino, I.; Fukada, T.; Seike, K.; Kawasaki, Y.; Otsuka, M. Outcomes of surgical resection for gastric cancer liver metastases: A retrospective analysis. World J. Surg. Oncol. 2020, 18, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Tang, K.; Zhang, B.; Dong, L.; Wang, L.; Tang, Z. Radiofrequency ablation versus traditional liver resection and chemotherapy for liver metastases from gastric cancer. J. Int. Med. Res. 2020, 48, 300060520940509. [Google Scholar] [CrossRef] [PubMed]
- Ceniceros, L.; Chopitea, A.; Pardo, F.; Rotellar, F.; Arbea, L.; Sangro, B.; Benito, A.; Rodríguez, J.; Sola, J.J.; Subtil, J.C.; et al. Intensified neoadjuvant multimodal approach in synchronous liver metastases from gastric cancer: A single institutional experience. Clin. Transl. Oncol. 2017, 20, 658–665. [Google Scholar] [CrossRef]
- Liu, J.; Li, J.-H.; Zhai, R.-J.; Wei, B.; Shao, M.-Z.; Chen, L. Predictive factors improving survival after gastric and hepatic surgical treatment in gastric cancer patients with synchronous liver metastases. Chin. Med. J. 2012, 125, 165–171. [Google Scholar]
- Miki, Y.; Fujitani, K.; Hirao, M.; Kurokawa, Y.; Mano, M.; Tsujie, M.; Miyamoto, A.; Nakamori, S.; Tsujinaka, T. Significance of surgical treatment of liver metastases from gastric cancer. Anticancer Res. 2012, 32, 665–670. [Google Scholar]
- Schildberg, C.W.; Croner, R.; Merkel, S.; Schellerer, V.; Müller, V.; Yedibela, S.; Hohenberger, W.; Peros, G.; Perrakis, A. Outcome of Operative Therapy of Hepatic Metastatic Stomach Carcinoma: A Retrospective Analysis. World J. Surg. 2012, 36, 872–878. [Google Scholar] [CrossRef] [PubMed]
- Takemura, N.; Saiura, A.; Koga, R.; Arita, J.; Yoshioka, R.; Ono, Y.; Hiki, N.; Sano, T.; Yamamoto, J.; Kokudo, N.; et al. Long-term outcomes after surgical resection for gastric cancer liver metastasis: An analysis of 64 macroscopically complete resections. Langenbeck Arch. Surg. 2012, 397, 951–957. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.-N.; Shen, K.-T.; Ling, J.-Q.; Gao, X.-D.; Hou, Y.-Y.; Wang, X.-F.; Qin, J.; Sun, Y.-H.; Qin, X.-Y. Prognostic analysis of combined curative resection of the stomach and liver lesions in 30 gastric cancer patients with synchronous liver metastases. BMC Surg. 2012, 12, 20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baek, H.-U.; Kim, S.B.; Cho, E.-H.; Jin, S.-H.; Yu, H.J.; Lee, J.-I.; Bang, H.-Y.; Lim, C.-S. Hepatic Resection for Hepatic Metastases from Gastric Adenocarcinoma. J. Gastric Cancer 2013, 13, 86–92. [Google Scholar] [CrossRef] [PubMed]
- Choi, S.B.; Song, J.; Kang, C.M.; Hyung, W.J.; Kim, K.S.; Choi, J.S.; Lee, W.J.; Noh, S.H.; Kim, C.B. Surgical outcome of metachronous hepatic metastases secondary to gastric cancer. Hepato Gastroenterol. 2010, 57, 29–34. [Google Scholar]
- Al-Batran, S.-E.; Homann, N.; Pauligk, C.; Illerhaus, G.; Martens, U.M.; Stoehlmacher, J.; Schmalenberg, H.; Luley, K.B.; Prasnikar, N.; Egger, M.; et al. Effect of Neoadjuvant Chemotherapy Followed by Surgical Resection on Survival in Patients With Limited Metastatic Gastric or Gastroesophageal Junction Cancer. JAMA Oncol. 2017, 3, 1237–1244. [Google Scholar] [CrossRef] [PubMed]
- Kokkola, A.; Louhimo, J.; Puolakkainen, P. Does non-curative gastrectomy improve survival in patients with metastatic gastric cancer? J. Surg. Oncol. 2012, 106, 193–196. [Google Scholar] [CrossRef] [PubMed]
- Oki, E.; Kyushu Study Group of Clinical Cancer; Tokunaga, S.; Emi, Y.; Kusumoto, T.; Yamamoto, M.; Fukuzawa, K.; Takahashi, I.; Ishigami, S.; Tsuji, A.; et al. Surgical treatment of liver metastasis of gastric cancer: A retrospective multicenter cohort study (KSCC1302). Gastric Cancer 2016, 19, 968–976. [Google Scholar] [CrossRef] [Green Version]
- Long, D.; Yu, P.-C.; Huang, W.; Luo, Y.-L.; Zhang, S. Systematic review of partial hepatic resection to treat hepatic metastases in patients with gastric cancer. Medicine 2016, 95, e5235. [Google Scholar] [CrossRef]
- Liao, Y.-Y.; Peng, N.-F.; Long, D.; Yu, P.-C.; Zhang, S.; Zhong, J.-H.; Li, L.-Q. Hepatectomy for liver metastases from gastric cancer: A systematic review. BMC Surg. 2017, 17, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Gavriilidis, P.; Roberts, K.J.; De’Angelis, N.; Sutcliffe, R.P. Gastrectomy Alone or in Combination with Hepatic Resection in the Management of Liver Metastases from Gastric Cancer: A Systematic Review Using an Updated and Cumulative Meta-Analysis. J. Clin. Med. Res. 2019, 11, 600–608. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Markar, S.R.; Mikhail, S.; Malietzis, G.; Athanasiou, T.; Mariette, C.; Sasako, M.; Hanna, G.B. Influence of Surgical Resection of Hepatic Metastases from Gastric Adenocarcinoma on Long-term Survival. Ann. Surg. 2016, 263, 1092–1101. [Google Scholar] [CrossRef]
- Griniatsos, J.; Trafalis, D. Differences in gastric cancer surgery outcome between East and West: Differences in surgery or different diseases? J. Buon 2018, 23, 1210–1215. [Google Scholar]
- Beom, S.-H.; Choi, Y.Y.; Baek, S.-E.; Li, S.-X.; Lim, J.S.; Son, T.; Kim, H.-I.; Cheong, J.-H.; Hyung, W.J.; Choi, S.H.; et al. Multidisciplinary treatment for patients with stage IV gastric cancer: The role of conversion surgery following chemotherapy. BMC Cancer 2018, 18, 1116. [Google Scholar] [CrossRef] [PubMed]
- Morgagni, P.; Solaini, L.; Framarini, M.; Vittimberga, G.; Gardini, A.; Tringali, D.; Valgiusti, M.; Monti, M.; Ercolani, G. Conversion surgery for gastric cancer: A cohort study from a western center. Int. J. Surg. 2018, 53, 360–365. [Google Scholar] [CrossRef] [PubMed]
- Cheon, S.H.; Rha, S.Y.; Jeung, H.-C.; Im, C.-K.; Kim, S.H.; Kim, H.R.; Ahn, J.B.; Roh, J.K.; Noh, S.H.; Chung, H.C. Survival benefit of combined curative resection of the stomach (D2 resection) and liver in gastric cancer patients with liver metastases. Ann. Oncol. 2008, 19, 1146–1153. [Google Scholar] [CrossRef] [PubMed]
- Montagnani, F.; Crivelli, F.; Aprile, G.; Vivaldi, C.; Pecora, I.; De Vivo, R.; Clerico, M.A.; Fornaro, L. Long-term survival after liver metastasectomy in gastric cancer: Systematic review and meta-analysis of prognostic factors. Cancer Treat. Rev. 2018, 69, 11–20. [Google Scholar] [CrossRef] [PubMed]
- Kurokawa, Y.; Shibata, T.; Sasako, M.; Sano, T.; Tsuburaya, A.; Iwasaki, Y.; Fukuda, H. Validity of response assessment criteria in neoadjuvant chemotherapy for gastric cancer (JCOG0507-A). Gastric Cancer 2013, 17, 514–521. [Google Scholar] [CrossRef] [Green Version]
- Li, M.-X.; Jin, Z.-X.; Zhou, J.-G.; Ying, J.-M.; Liang, Z.-Y.; Mao, X.-X.; Bi, X.-Y.; Zhao, J.-J.; Li, Z.-Y.; Huang, Z.; et al. Prognostic Value of Lymph Node Ratio in Patients Receiving Combined Surgical Resection for Gastric Cancer Liver Metastasis. Medicine 2016, 95, e3395. [Google Scholar] [CrossRef]
- Schmidt, B.; Look-Hong, N.; Maduekwe, U.N.; Chang, K.; Hong, T.S.; Kwak, E.L.; Lauwers, G.Y.; Rattner, D.W.; Mullen, J.T.; Yoon, S.S. Noncurative Gastrectomy for Gastric Adenocarcinoma Should only be Performed in Highly Selected Patients. Ann. Surg. Oncol. 2013, 20, 3512–3518. [Google Scholar] [CrossRef]
- Ambiru, S.; Miyazaki, M.; Ito, H.; Nakagawa, K.; Shimizu, H.; Yoshidome, H.; Shimizu, Y.; Nakajima, N. Benefits and limits of hepatic resection for gastric metastases. Am. J. Surg. 2001, 181, 279–283. [Google Scholar] [CrossRef]
- Sakamoto, Y.; Sano, T.; Shimada, K.; Esaki, M.; Saka, M.; Fukagawa, T.; Katai, H.; Kosuge, T.; Sasako, M. Favorable indications for hepatectomy in patients with liver metastasis from gastric cancer. J. Surg. Oncol. 2007, 95, 534–539. [Google Scholar] [CrossRef] [PubMed]
- Cui, J.-K.; Liu, M.; Shang, X.-K. Hepatectomy for Liver Metastasis of Gastric Cancer: A Meta-Analysis. Surg. Innov. 2019, 26, 692–697. [Google Scholar] [CrossRef] [PubMed]
- Kataoka, K.; Kinoshita, T.; Moehler, M.; Mauer, M.; Shitara, K.; Wagner, A.D.; Schrauwen, S.; Yoshikawa, T.; Roviello, F.; Tokunaga, M.; et al. Current management of liver metastases from gastric cancer: What is common practice? New challenge of EORTC and JCOG. Gastric Cancer 2017, 20, 904–912. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fujitani, K.; Yang, H.-K.; Mizusawa, J.; Kim, Y.-W.; Terashima, M.; Han-Kwang, Y.; Iwasaki, Y.; Hyung, W.J.; Takagane, A.; Park, D.J.; et al. Gastrectomy plus chemotherapy versus chemotherapy alone for advanced gastric cancer with a single non-curable factor (REGATTA): A phase 3, randomised controlled trial. Lancet Oncol. 2016, 17, 309–318. [Google Scholar] [CrossRef]
- Al-Batran, S.-E.; Hartmann, J.T.; Hofheinz, R.; Homann, N.; Rethwisch, V.; Probst, S.; Stoehlmacher, J.; Clemens, M.R.; Mahlberg, R.; Fritz, M.; et al. Biweekly fluorouracil, leucovorin, oxaliplatin, and docetaxel (FLOT) for patients with metastatic adenocarcinoma of the stomach or esophagogastric junction: A phase II trial of the Arbeitsgemeinschaft Internistische Onkologie. Ann. Oncol. 2008, 19, 1882–1887. [Google Scholar] [CrossRef]
- Salati, M.; Valeri, N.; Spallanzani, A.; Braconi, C.; Cascinu, S. Oligometastatic gastric cancer: An emerging clinical entity with distinct therapeutic implications. Eur. J. Surg. Oncol. 2019, 45, 1479–1482. [Google Scholar] [CrossRef] [Green Version]
- Al-Batran, S.-E.; Goetze, T.O.; Mueller, D.W.; Vogel, A.; Winkler, M.; Lorenzen, S.; Novotny, A.; Pauligk, C.; Homann, N.; Jungbluth, T.; et al. The RENAISSANCE (AIO-FLOT5) trial: Effect of chemotherapy alone vs. chemotherapy followed by surgical resection on survival and quality of life in patients with limited-metastatic adenocarcinoma of the stomach or esophagogastric junction—A phase III trial of the German AIO/CAO-V/CAOGI. BMC Cancer 2017, 17, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Han, D.-S.; Suh, Y.-S.; Kong, S.-H.; Lee, H.-J.; Im, S.-A.; Bang, Y.-J.; Kim, W.-H.; Yang, H.-K. Outcomes of surgery aiming at curative resection in good responder to induction chemotherapy for gastric cancer with distant metastases. J. Surg. Oncol. 2012, 107, 511–516. [Google Scholar] [CrossRef]
- Kinoshita, J.; Fushida, S.; Tsukada, T.; Oyama, K.; Okamoto, K.; Makino, I.; Nakamura, K.; Miyashita, T.; Tajima, H.; Takamura, H.; et al. Efficacy of conversion gastrectomy following docetaxel, cisplatin, and S-1 therapy in potentially resectable stage IV gastric cancer. Eur. J. Surg. Oncol. 2015, 41, 1354–1360. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sato, Y.; Ohnuma, H.; Nobuoka, T.; Hirakawa, M.; Sagawa, T.; Fujikawa, K.; Takahashi, Y.; Shinya, M.; Katsuki, S.; Takahashi, M.; et al. Conversion therapy for inoperable advanced gastric cancer patients by docetaxel, cisplatin, and S-1 (DCS) chemotherapy: A multi-institutional retrospective study. Gastric Cancer 2017, 20, 517–526. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yamaguchi, K.; Yoshida, K.; Tanahashi, T.; Takahashi, T.; Matsuhashi, N.; Tanaka, Y.; Tanabe, K.; Ohdan, H. The long-term survival of stage IV gastric cancer patients with conversion therapy. Gastric Cancer 2017, 21, 315–323. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ma, G. Japanese Gastric Cancer Treatment Guidelines 2018, 5th edition. Gastric Cancer 2020, 24, 1–21. [Google Scholar] [CrossRef] [Green Version]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author Year | Country | Study Design | Study Interval | N. Patients | Median Age | Female/Male | pT1–2/pT3–4 | pN0–1/pN2–3 | Lymphatic Invasion | Venous Invasion | Primary Tumor Median Size (cm) | Histology Well-Moderate/Poor Differentiated |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Choi 2010 [57] | Korea | Retro | 1986–2007 | 14 | 65 | NR | NR | NR | NR | NR | NR | NR |
| Makino 2010 [18] | Japan | Retro | 1992–2007 | 16 | NR | 3/13 | NR/8 | NR/13 | 12 | 14 | NR | 8/8 |
| Tsujimoto 2010 [19] | Japan | Retro | 1980–2007 | 17 | 66 | 1/16 | 12/5 | 12/5 | 8 | 9 | 5.7 | NR |
| Dittmar 2012 [30] | Germany | Retro | 1995–2009 | 10 | 57 | NR | NR | NR | 11 | NR | NR | NR |
| Garancini 2012 [41] | Italy | Retro | 1998–2007 | 21 | 64 | 7/14 | NR/8 | 19/11 | NR | 13 | NR | 8/13 |
| Liu J. 2012 [51] | China | Retro | 1995–2010 | 35 | NR | 8/29 | 19/16 | 12/23 | 10 | NR | NR | 0/25 |
| Miki 2012 [52] | Japan | Retro | 1995–2009 | 25 | 72 | 2/23 | 8/17 | 14/11 | NR | NR | NR | NR |
| Schildberg 2012 [53] | Germany | Retro | 1972–2008 | 31 | 65 | 11/20 | NR | NR | NR | NR | NR | NR |
| Takemura 2012 [54] | Japan | Retro | 1993–2011 | 64 | 65 | 49/15 | NR/49 | 22/42 | NR | NR | NR | 42/22 |
| Wang Y.N. 2012 [55] | China | Retro | 2003–2008 | 30 | 60 | 3/27 | 4/26 | 10/20 | NR | NR | 3.7 | NR |
| Baek 2013 [56] | Korea | Retro | 2003–2010 | 12 | 61 | 1/11 | 3/9 | 9/3 | 7 | 2 | NR | 9/1 |
| Chen 2013 [20] | China | Retro | 2007–2012 | 20 | 54 | 8/12 | 6/14 | 12/8 | NR | NR | NR | 16/4 |
| Qiu 2013 [21] | China | Retro | 1998–2009 | 25 | NR | 3/22 | 17/8 | 4/21 | NR | NR | NR | 9/16 |
| Vigano 2013 [22] | Italy | Retro | 1997–2008 | 14 | 61.5 | NR | NR | NR | NR | NR | NR | NR |
| Aizawa 2014 [23] | Japan | Retro | 1997–2010 | 74 | 66 | 18/56 | NR | NR | NR | NR | NR | NR |
| Komeda 2014 [24] | Japan | Retro | 2000–2012 | 24 | 69.5 | 3/21 | 17/7 | 10/14 | NR | NR | NR | NR |
| Wang W. 2014 [25] | China | Retro | 1996–2008 | 39 | 64 | 13/26 | 8/31 | 23/16 | NR | NR | NR | 23/16 |
| Guner 2015 [26] | Korea | Retro | 1998–2013 | 68 | 61 | 12/56 | 17/52 | 32/36 | 35 | 36 | NR | NR |
| Kinoshita 2015 [27] | Japan | Retro | 1990–2010 | 256 | 64 | 49/207 | 74 | 54/204 | 105 | 129 | NR | 173/NR |
| Li Z. 2015 [28] | China | Retro | 2008–2011 | 13 | NR | NR | NR | NR | NR | NR | NR | NR |
| Liu Q. 2015 [29] | China | Retro | 1990–2009 | 35 | 56 | 13/22 | 6/29 | 4/31 | 20 | NR | NR | 15/20 |
| Ohkura 2015 [31] | Japan | Retro | 1985–2014 | 13 | 63 | 0/13 | NR | NR | NR | NR | NR | NR |
| Shinohara 2015 [32] | Japan | Retro | 1995–2010 | 18 | NR | NR | NR | NR | NR | NR | NR | NR |
| Markar 2016 [33] | UK | Retro | 1997–2012 | 78 | 65 | 51/7 | NR | NR | NR | NR | NR | NR |
| Oguro 2016 [34] | Japan | Retro | 2002–2012 | 26 | 69.5 | 3/23 | 8/18 | NR/8 | NR | NR | NR | 18/8 |
| Tatsubayashi 2016 [35] | Japan | Retro | 2004–2014 | 28 | 72 | 5/23 | 8/20 | 3/25 | NR | NR | 5.6 | 22/6 |
| Tiberio 2016 [8] | Italy | Retro | 1990–2013 | 105 | 68 | 34/71 | 38/46 | 36/40 | NR | NR | NR | NR |
| Fukami 2017 [36] | Japan | Retro | 2001–2012 | 14 | 66 | 3/11 | 2/12 | NR/11 | NR | NR | NR | 11/3 |
| Lee J.W. 2017 [37] | Korea | Retro | 2000–2014 | 7 | 59.2 | 2/5 | NR | NR | NR | NR | NR | NR |
| Li J. 2017 [38] | China | Retro | 2006–2016 | 30 | NR | NR | NR | NR | NR | NR | NR | NR |
| Li S.C. 2017 [39] | Taiwan | Retro | 1996–2012 | 34 | 62 | 11/23 | NR | NR | NR | NR | NR | NR |
| Ryu 2017 [40] | Japan | Retro | 1997–2005 | 14 | NR | NR | NR | NR | NR | NR | NR | NR |
| Song 2017 [42] | China | Retro | 2001–2012 | 96 | 63 | 24/72 | 47/59 | 28/68 | NR | NR | NR | 62/34 |
| Ministrini 2018 [43] | Italy | Retro | 1990–2017 | 144 | 68 | 50/94 | 23/93 | 48/68 | NR | NR | NR | 13/22 |
| Nishi 2018 [44] | Japan | Retro | 2001–2013 | 10 | 71.7 | 1/9 | 8/2 | NR | NR | NR | NR | NR |
| Shirasu 2018 [45] | Japan | Retro | 2004–2015 | 9 | 74 | 1/8 | NR | NR | NR | NR | NR | 9/NR |
| Gao 2019 [50] | China | Retro | 1975–2013 | 54 | 57 | 11/43 | 29/25 | 18/36 | NR | NR | NR | NR |
| Nonaka 2019 [51] | Japan | Retro | 2016 | 10 | 68 | 1/9 | 3/7 | 7/3 | 8 | NR | NR | NR |
| Kawahara 2020 [48] | Japan | Retro | 2006–2016 | 20 | 73.5 | 7/13 | NR/4 | 8/12 | 14 | 13 | NR | 14/3 |
| Tang 2020 [49] | China | Retro | 2008–2018 | 20 | 61 | 4/16 | 2/18 | 10/10 | NR | NR | NR | 0/12 |
| Author Year | Synchronous/Metachronous | Solitary/Multiple | Unilobar/Bilobar | Median Size Liver Metastases (mm) | Minor/Major Hepatectomy | R0/R1/R2 Liver Resection Margin | Neoadjuvant/Adjuvant Chemotherapy |
|---|---|---|---|---|---|---|---|
| Choi 2010 [57] | 0/14 | 9/5 | NR | NR | NR | NR | NR |
| Makino 2010 [18] | 9/7 | 9/7 | 11/5 | NR | 14/2 | NR | 5/9 |
| Tsujimoto 2010 [19] | 9/8 | 13/4 | NR | 48 | NR | NR | 0/14 |
| Dittmar 2012 [30] | NR | NR | NR | 26 | 8/2 | NR | 0/NR |
| Garancini 2012 [41] | 12/9 | 12/9 | 16/5 | 30 | 17/4 | 19/2/0 | NR |
| Liu J 2012 [51] | NR | NR | NR | NR | NR | NR | NR |
| Miki 2012 [52] | 16/9 | 18/7 | 20/5 | 20 | NR | NR | 0/10 |
| Schildberg 2012 [53] | 17/14 | NR | NR | NR | 21/10 | 23/3/5 | 2/9 |
| Takemura 2012 [54] | 32/32 | 37/27 | NR | NR | 50/14 | 55/9/0 | 18/26 |
| Wang Y.N. 2012 [55] | 30/0 | 22/8 | 27/3 | 31 | 23/7 | NR | 0/30 |
| Baek 2013 [56] | 3/9 | 10/1 | NR | NR | 9/3 | 11/1/0 | NR/6 |
| Chen 2013 [20] | 20/0 | 8/12 | 11/9 | 41 | 6/14 | NR | 20/20 |
| Qiu 2013 [21] | 25/0 | 19/6 | 21/4 | 20 | NR | NR | 4/14 |
| Vigano 2013 [22] | 9/5 | 9/5 | NR | NR | NR | NR | 8/0 |
| Aizawa 2014 [23] | 74/0 | NR | NR | NR | NR | 53/0/21 | NR |
| Komeda 2014 [24] | 1/23 | 17/ | NR | NR | NR | NR | 11/15 |
| Wang W. 2014 [25] | 39/0 | 31/8 | 34/5 | 28 | NR | NR | 0/39 |
| Guner 2015 [26] | 26/42 | 45/23 | 60/8 | 27 | 47/21 | NR | 0/66 |
| Kinoshita 2015 [27] | 106/150 | 168/88 | NR | 30 | 183/73 | 230/26/0 | 45/84 |
| Li Z. 2015 [28] | 13/0 | NR | NR | NR | NR | NR | 13/NR |
| Liu Q. 2015 [29] | 35/0 | 27/8 | 30/5 | NR | 29/6 | 30/5/0 | 0/35 |
| Ohkura 2015 [31] | 9/4 | 4/9 | NR | NR | NR | NR | 0/12 |
| Shinohara 2015 [32] | NR | NR | NR | NR | NR | NR | NR |
| Markar 2016 [33] | 78/0 | NR | NR | NR | 66/12 | NR | NR |
| Oguro 2016 [34] | 6/20 | 16/10 | NR | 37 | NR | NR | NR |
| Tatsubayashi 2016 [35] | 15/13 | 20/8 | NR | 24.5 | 27/1 | NR | 3/12 |
| Tiberio 2016 [8] | 74/31 | NR | NR | NR | 94/11 | 89/7/9 | 0/29 |
| Fukami 2017 [36] | 1/13 | 9/5 | NR | 28 | NR | NR | NR/14 |
| Lee J.W. 2017 [37] | NR | 5/2 | 6/1 | NR | NR | NR | 0/6 |
| Li J. 2017 [38] | NR | NR | NR | NR | NR | 30/0/0 | NR |
| Li S.C. 2017 [39] | 0/34 | NR | NR | NR | NR | NR | NR |
| Ryu 2017 [40] | NR | NR | NR | 42 | 7/7 | NR | NR |
| Song 2017 [42] | 59/37 | 42/54 | 57/29 | NR | 61/35 | 91/5/0 | 0/58 |
| Ministrini 2018 [43] | 112/32 | NR | NR | NR | 132/12 | 117/14/13 | 20/32 |
| Nishi 2018 [44] | 6/4 | 6/4 | NR | 23.5 | 5/5 | NR | 2/6 |
| Shirasu 2018 [45] | 6/3 | 0/9 | 5/4 | 25 | NR | 9/0/0 | NR/3 |
| Gao 2019 [50] | NR | 38/16 | NR | NR | NR | NR | 0/24 |
| Nonaka 2019 [51] | 4/6 | 7/3 | NR | NR | NR | NR | 0/0 |
| Kawahara 2020 [48] | 11/9 | 11/9 | NR | 25 | NR | NR | 0/20 |
| Tang 2020 [49] | 19/1 | NR | 17/3 | 29 | NR | NR | 0/17 |
| Author Year | Post-Operative Morbidity (%) | Post-Operative 30-Day Mortality (%) | Overall Survival | Disease-Free Survival | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 1 Year (%) | 3 Years (%) | 5 Years (%) | MST (Months) | 1 Year (%) | 3 Years (%) | 5 Years (%) | MST (Months) | |||
| Choi 2010 [57] | NR | NR | 67 | 38.3 | NR | NR | 28.5 | NR | NR | NR |
| Makino 2010 [18] | NR | 0 | 82.3 | 46.4 | 37.1 | 31.2 | NR | NR | NR | NR |
| Tsujimoto 2010 [19] | NR | NR | 75 | 37.5 | 31.5 | 34 | NR | NR | NR | NR |
| Dittmar 2012 [30] | NR | 0 | NR | NR | NR | NR | NR | NR | NR | NR |
| Garancini 2012 [41] | 19 | 0 | 68 | 31 | 19 | 11 | 51 | 25 | 14 | NR |
| Liu J. 2012 [51] | NR | NR | 58.1 | 21.7 | NR | 15 | NR | NR | NR | NR |
| Miki 2012 [52] | NR | NR | 73.9 | 42.8 | 36.7 | 33.4 | NR | NR | NR | 5 |
| Schildberg 2012 [53] | 29 | 6 | NR | NR | 13 | NR | NR | NR | NR | NR |
| Takemura 2012 [54] | 27 | 0 | 84 | 50 | 37 | 34 | 42 | 27 | 27 | 9 |
| Wang Y.N. 2012 [55] | 13 | 0 | 43.3 | 16.7 | 16.7 | 11 | NR | NR | NR | NR |
| Baek 2013 [56] | NR | 0 | 65 | NR | 39 | 31 | NR | NR | NR | NR |
| Chen 2013 [20] | NR | 0 | NR | NR | 15 | 22.3 | NR | NR | NR | NR |
| Qiu 2013 [21] | NR | 0 | 96 | 70.4 | 29.4 | 38 | 56 | 22.3 | 11.1 | 18 |
| Vigano 2013 [22] | 40 | 0 | 95 | 63.2 | 33.2 | 52.3 | NR | NR | NR | NR |
| Aizawa 2014 [23] | NR | 0 | NR | NR | 17 | 13 | NR | NR | NR | NR |
| Komeda 2014 [24] | NR | 0 | 78.3 | 40.1 | 40.1 | 22.3 | NR | NR | NR | NR |
| Wang W 2014 [25] | 8 | 0 | 56.4 | 17.9 | 10.3 | 14 | 30.8 | 10.3 | 7.7 | 8 |
| Guner 2015 [26] | 28 | 1 | 79.1 | 40.6 | 30 | 24 | 49.3 | 30.4 | 26 | NR |
| Kinoshita 2015 [27] | 11 | 2 | 77.3 | 41.9 | 31.1 | 31.1 | 43.6 | 32.4 | 30.1 | 9.4 |
| Li Z. 2015 [28] | NR | NR | NR | NR | NR | 16.3 | NR | NR | NR | NR |
| Liu Q. 2015 [29] | 6 | 0 | NR | NR | 14.3 | 33 | NR | NR | NR | NR |
| Ohkura 2015 [31] | NR | 0 | NR | NR | NR | NR | NR | NR | NR | NR |
| Shinohara 2015 [32] | NR | 0 | NR | NR | NR | NR | NR | NR | NR | NR |
| Markar 2016 [33] | NR | 10 | 64.1 | NR | 38.5 | NR | NR | NR | NR | NR |
| Oguro 2016 [34] | NR | NR | NR | NR | 13.9 | 20.1 | NR | NR | NR | 16.8 |
| Tatsubayashi 2016 [35] | 4 | 0 | NR | NR | 32 | 49 | NR | NR | 29 | NR |
| Tiberio 2016 [8] | 13 | 1 | 58.2 | 20.3 | 13.1 | 14.6 | 48 | 20.2 | 8.6 | 10 |
| Fukami 2017 [36] | 21 | 0 | 71.4 | 42.9 | 42.9 | 27.9 | NR | NR | NR | NR |
| Lee J.W. 2017 [37] | 29 | NR | NR | NR | 68.6 | 67.5 | NR | NR | 80 | 74.1 |
| Li J. 2017 [38] | NR | 0 | - | - | - | - | - | - | - | - |
| Li S.C. 2017 [39] | NR | NR | 73.5 | 36.9 | 24.5 | 26.16 | NR | NR | NR | NR |
| Ryu 2017 [40] | NR | 0 | 84.6 | 51.3 | 51.3 | NR | NR | NR | NR | NR |
| Song 2017 [42] | 55 | 0 | 87.5 | 47.6 | 21.7 | 34 | NR | NR | NR | NR |
| Ministrini 2018 [43] | 22 | 2 | 49.5 | 19.4 | 11.6 | 12 | NR | NR | NR | NR |
| Nishi 2018 [44] | 10 | 0 | 88.9 | 17.8 | NR | 21.5 | 20 | NR | NR | 4.7 |
| SHIRASU 2018 [45] | 44 | 0 | NR | NR | NR | 24.8 | NR | NR | NR | 7.9 |
| Gao 2019 [50] | NR | NR | 77.8 | 37 | 25.9 | 29.3 | NR | NR | NR | NR |
| Nonaka 2019 [51] | NR | NR | 78 | 33.3 | 22.2 | 30 | 44.4 | 22.2 | 22.2 | NR |
| Kawahara 2020 [48] | 0 | 0 | 80 | 55.5 | 31.7 | 42 | 35 | 24 | 18 | 10.5 |
| Tang 2020 [49] | 25 | 15 | NR | 23.5 | NR | 20 | NR | 23.5 | NR | NR |
| Prognostic Factor | N. of Studies | Participants | HR (95% CI) | p | I2 |
|---|---|---|---|---|---|
| Male sex | 16 | 788 | 0.86 (0.68–1.09) | 0.21 | 0% |
| Age >65 | 19 | 896 | 0.86 (0.49–1.51) | 0.60 | 94% |
| Synchronous liver metastases | 14 | 730 | 1.62 (1.17–2.25) | 0.004 | 62% |
| Multiple liver metastases | 17 | 788 | 1.66 (1.44–1.91) | <0.00001 | 4% |
| Bilobar liver metastases | 9 | 495 | 1.96 (1.34–2.87) | 0.0005 | 69% |
| >3 cm liver metastases | 19 | 803 | 2.39 (1.14–5.04) | 0.02 | 98% |
| R + liver resection margin | 6 | 400 | 4.15 (2.37–7.26) | <0.00001 | 33% |
| Chemotherapy before/after liver resection | 11 | 781 | 1.49 (1.11–1.99) | 0.008 | 73% |
| Primary tumor Size >5 cm | 7 | 179 | 1.50 (0.99–2.26) | 0.06 | 14% |
| pT3–4 | 21 | 1084 | 1.77 (1.31–2.41) | 0.0002 | 51% |
| pN2–3 | 16 | 750 | 1.54 (1.28–1.85) | <0.00001 | 11% |
| Lymphatic invasion present | 9 | 467 | 1.28 (0.96–1.70) | 0.09 | 72% |
| Venous invasion present | 7 | 364 | 1.23 (0.93–1.62) | 0.15 | 0% |
| Primary tumor poorly differentiated | 17 | 796 | 1.34 (1.10–1.63) | 0.004 | 14% |
| Prognostic Factor | N. of Studies | Participants | HR (95% CI) | p | I2 |
|---|---|---|---|---|---|
| Male sex | 3 | 291 | 0.94 (0.65–1.36) | 0.76 | 0% |
| Age >65 | 4 | 301 | 0.96 (0.70–1.31) | 0.80 | 39% |
| Synchronous liver metastases | 4 | 302 | 1.50 (1.21–1.86) | 0.0002 | 0% |
| Multiple liver metastases | 4 | 301 | 2.34 (1.67–3.29) | <0.00001 | 0% |
| Bilobar liver metastases | 1 | 25 | 3.39 (1.09–10.56) | 0.04 | - |
| >3 cm liver metastases | 4 | 301 | 1.51 (1.10–2.07) | 0.01 | 0% |
| Chemotherapy before/after liver resection | 3 | 291 | 0.77 (0.56–1.06) | 0.11 | 0% |
| Primary tumor Size >5 cm | 1 | 10 | 3.22 (0.71–14.57) | 0.13 | - |
| pT3–4 | 4 | 301 | 1.43 (1.06–1.94) | 0.02 | 0% |
| pN2–3 | 3 | 292 | 1.35 (0.93–1.97) | 0.11 | 35% |
| Lymphatic invasion present | 3 | 291 | 1.46 (1.02–2.08) | 0.04 | 43% |
| Venous invasion present | 2 | 266 | 1.25 (0.92–1.70) | 0.16 | 0% |
| Primary tumor poorly differentiated | 4 | 317 | 1.27 (0.80–2.01) | 0.31 | 46% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marte, G.; Tufo, A.; Steccanella, F.; Marra, E.; Federico, P.; Petrillo, A.; Maida, P. Efficacy of Surgery for the Treatment of Gastric Cancer Liver Metastases: A Systematic Review of the Literature and Meta-Analysis of Prognostic Factors. J. Clin. Med. 2021, 10, 1141. https://doi.org/10.3390/jcm10051141
Marte G, Tufo A, Steccanella F, Marra E, Federico P, Petrillo A, Maida P. Efficacy of Surgery for the Treatment of Gastric Cancer Liver Metastases: A Systematic Review of the Literature and Meta-Analysis of Prognostic Factors. Journal of Clinical Medicine. 2021; 10(5):1141. https://doi.org/10.3390/jcm10051141
Chicago/Turabian StyleMarte, Gianpaolo, Andrea Tufo, Francesca Steccanella, Ester Marra, Piera Federico, Angelica Petrillo, and Pietro Maida. 2021. "Efficacy of Surgery for the Treatment of Gastric Cancer Liver Metastases: A Systematic Review of the Literature and Meta-Analysis of Prognostic Factors" Journal of Clinical Medicine 10, no. 5: 1141. https://doi.org/10.3390/jcm10051141