
Analysis of the Clinical and Epidemiological Meaning of Screening Test for SARS-CoV-2: Considerations in the Chronic Kidney Disease Patients during the COVID-19 Pandemic

 , ,
, ,
Abstract
:1. Introduction
2. COVID-19 Risk in Chronic Kidney Patients
3. SARS-CoV-2 and Screening Test
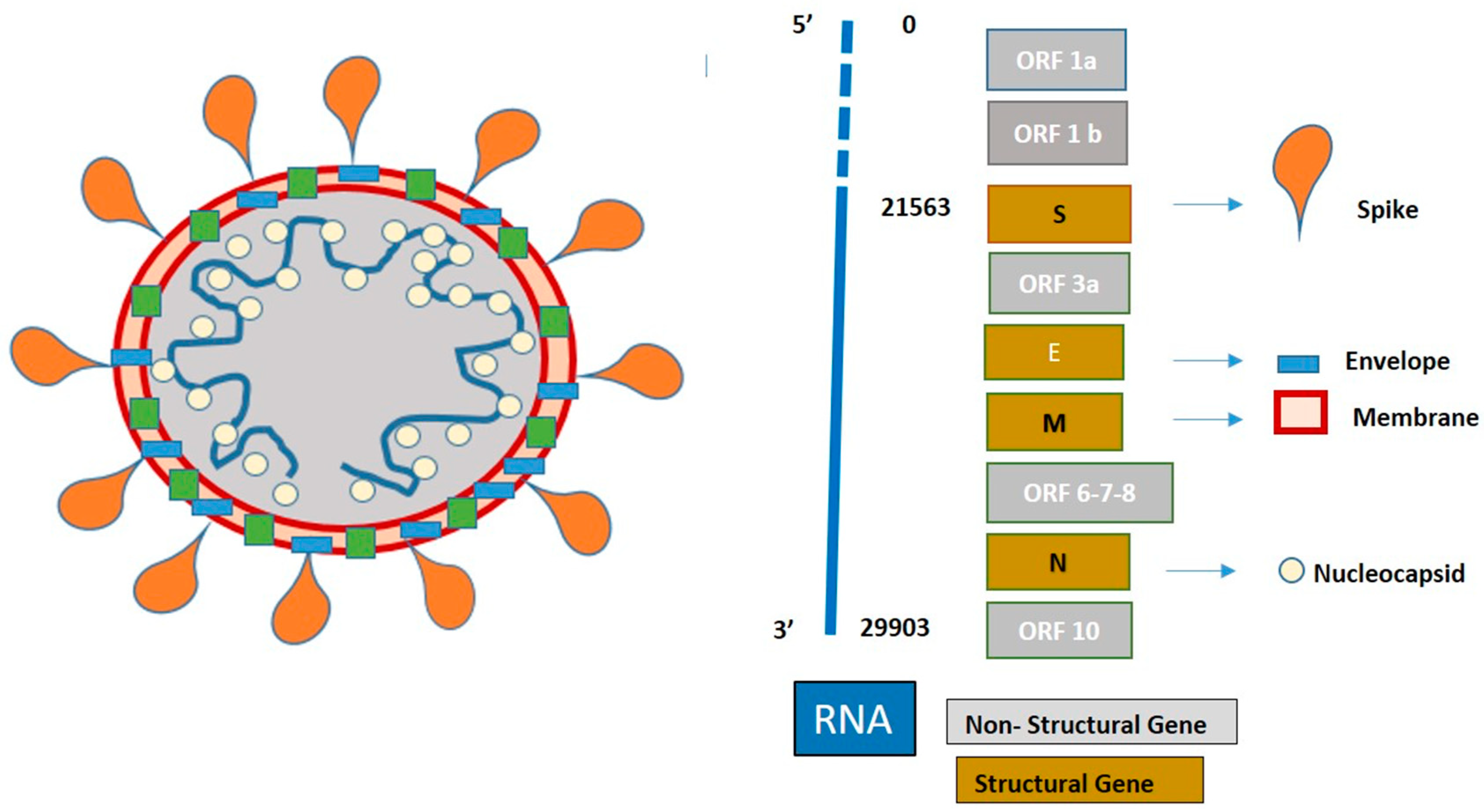
3.1. SARS-CoV-2 Structure
3.2. Screening Test Methods
- -
- Reverse transcription: a process where the enzyme reverse transcriptase converts RNA into complementary DNA (cDNA), which is suitable for PCR.
- -
- Amplification of cDNA target sequences, which requires the presence of a polymerase enzyme and primer. The polymerase amplifies the cDNA sequence, while the primer identifies the specific sequences to amplify.
3.3. Screening Test Accuracy
3.4. Specimen Type
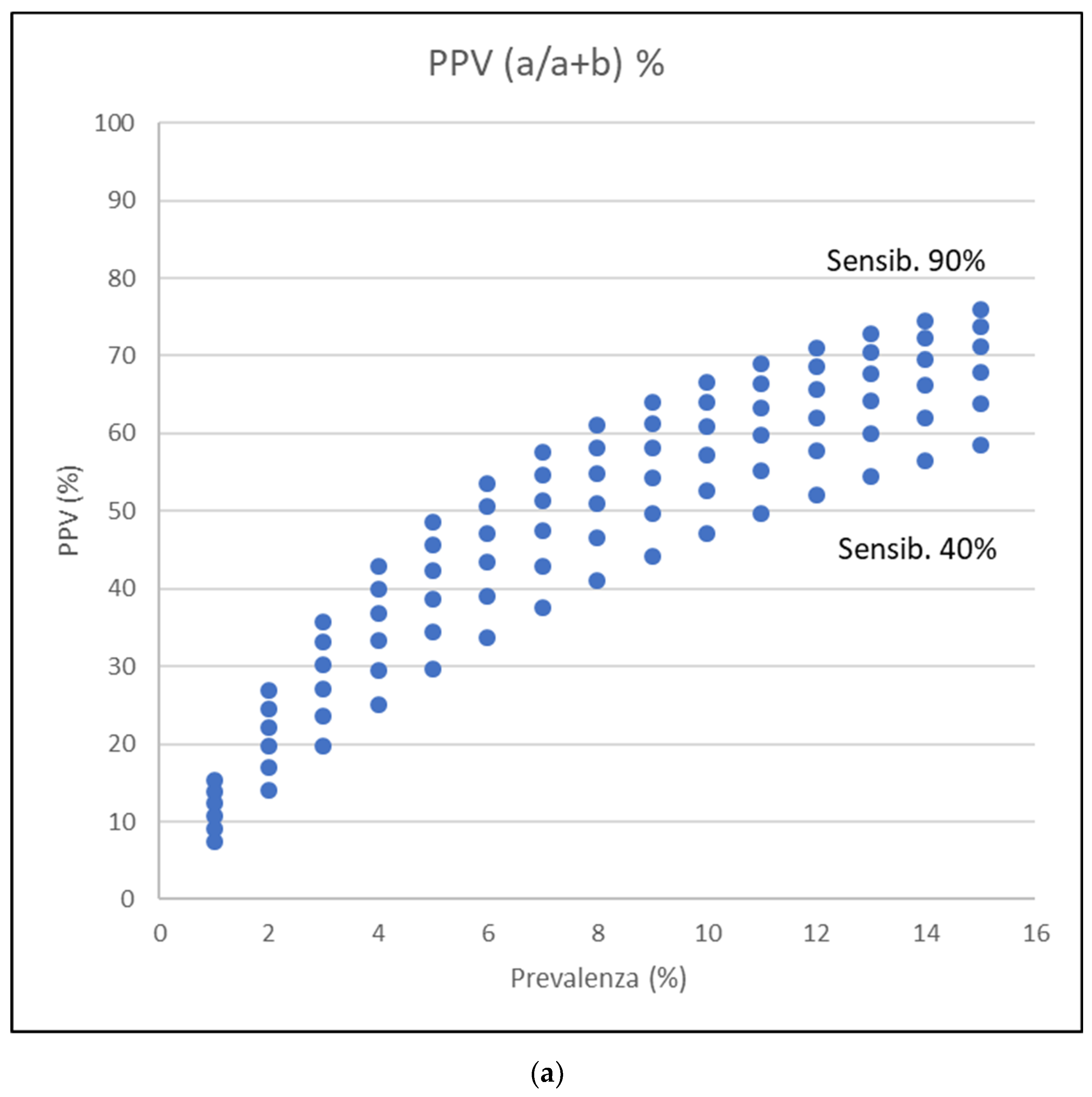
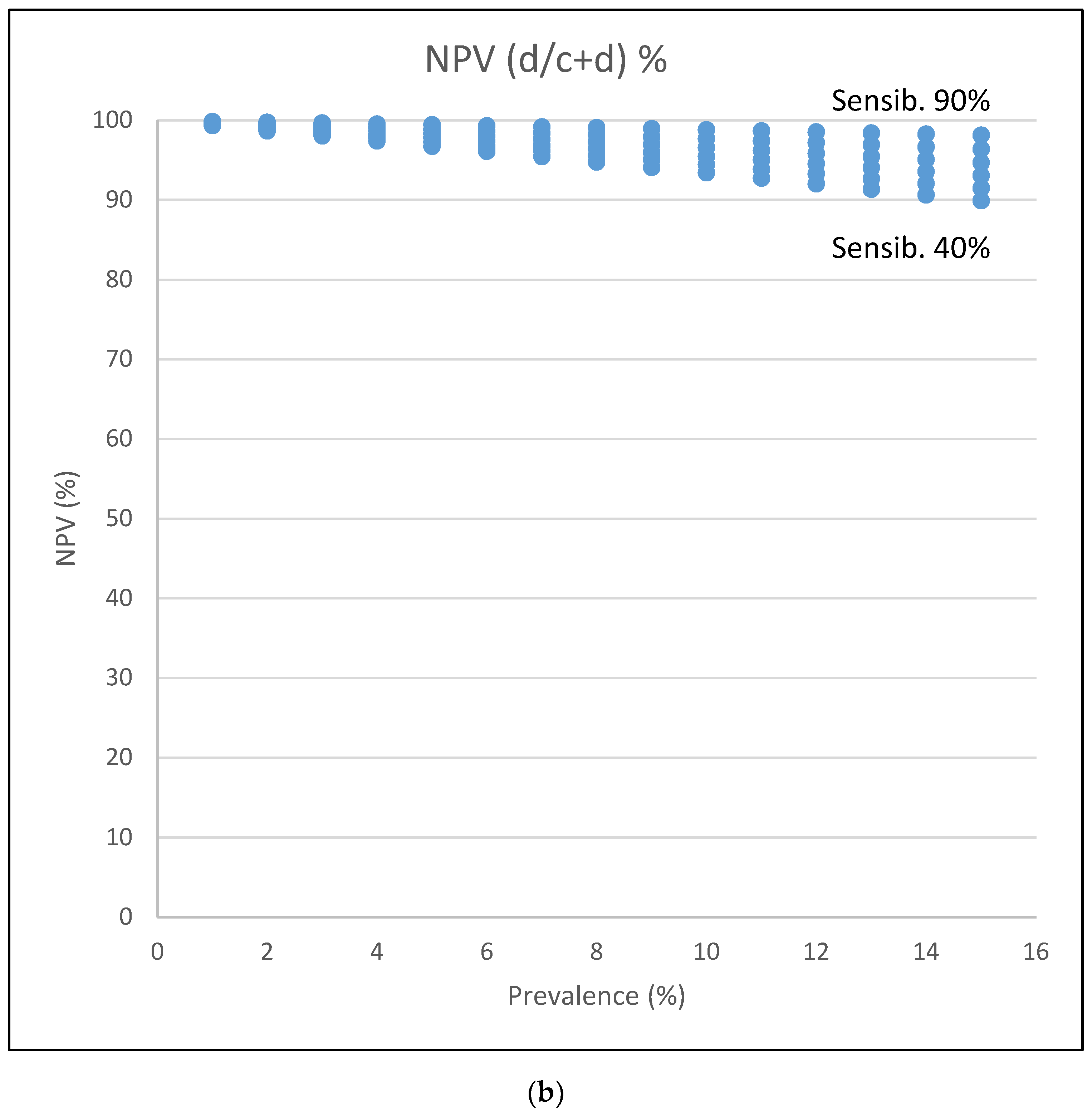
3.5. Statistical Insight on Screening Test
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
Appendix A.1. Insight Box 1

{kind=link}
{kind=link}
{kind=link}
| Disease | ||||
|---|---|---|---|---|
| Test | Present | Absent | ||
| positive | a | b | a+b | |
| negative | c | d | c+d | |
| a+c | b+d | N | ||
Appendix A.2. Insight Box 2: Tests Performance Examples in Different Scenarios of COVID-19 Pandemic
| Covid-19 | ||||
|---|---|---|---|---|
| Saliva | Present | Absent | ||
| positive | 16 | 2 | 18 | |
| negative | 30 | 179 | 182 | |
| 19 | 181 | 200 | ||
| Covid-19 | ||||
|---|---|---|---|---|
| Saliva | Present | Absent | ||
| positive | 60 | 22 | 82 | |
| negative | 12 | 1906 | 1918 | |
| 72 | 1928 | 2000 | ||
| Covid-19 | ||||
|---|---|---|---|---|
| Oro-pharyngeal swabs | Present | Absent | ||
| positive | 5 | 27 | 32 | |
| negative | 14 | 154 | 168 | |
| 19 | 181 | 200 | ||
| Covid-19 | ||||
|---|---|---|---|---|
| Oro-pharyngeal swabs | Present | Absent | ||
| positive | 19 | 292 | 311 | |
| negative | 53 | 1636 | 1689 | |
| 72 | 1928 | 2000 | ||
References
- Sokouti, M.; Sadeghi, R.; Pashazadeh, S.; Eslami, S.; Sokouti, M.; Ghojazadeh, M.; Sokouti, B. Comparative Global Epidemiological Investigation of SARS-CoV-2 and SARS-CoV Diseases Using Meta-MUMS Tool Through Incidence, Mortality, and Recovery Rates. Arch. Med Res. 2020, 51, 458–463. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.; Hu, B.; Hu, C.; Zhu, F.; Liu, X.; Zhang, J.; Wang, B.; Xiang, H.; Cheng, Z.; Xiong, Y.; et al. Clinical Characteristics of 138 Hospitalized Patients With 2019 Novel Coronavirus-Infected Pneumonia in Wuhan, China. JAMA 2020, 323, 1061–1069. [Google Scholar] [CrossRef]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Tammaro, A.; Adebanjo, G.A.R.; Parisella, F.R.; Pezzuto, A.; Rello, J. Cutaneous manifestations in COVID-19: The experiences of Barcelona and Rome. J. Eur. Acad. Dermatol. Venereol. 2020, 34, e306–e307. [Google Scholar] [CrossRef]
- He, R.; Lu, Z.; Zhang, L.; Fan, T.; Xiong, R.; Shen, X.; Feng, H.; Meng, H.; Lin, W.; Jiang, W.; et al. The clinical course and its correlated immune status in COVID-19 pneumonia. J. Clin. Virol. 2020, 127, 104361. [Google Scholar] [CrossRef] [PubMed]
- Cheng, Y.; Luo, R.; Wang, K.; Zhang, M.; Wang, Z.; Dong, L.; Li, J.; Yao, Y.; Ge, S.; Xu, G. Kidney disease is associated with in-hospital death of patients with COVID-19. Kidney Int. 2020, 97, 829–838. [Google Scholar] [CrossRef]
- Henry, B.M.; Lippi, G. Chronic kidney disease is associated with severe coronavirus disease 2019 (COVID-19) infection. Int. Urol. Nephrol. 2020, 52, 1193–1194. [Google Scholar] [CrossRef] [Green Version]
- Sánchez-Álvarez, J.E.; Pérez Fontán, M.; Jiménez Martín, C.; Blasco Pelícano, M.; Cabezas Reina, C.J.; Sevillano Prieto, Á.M.; Melilli, E.; Crespo Barrios, M.; Macía Heras, M.; Del Pino, Y.; et al. SARS-CoV-2 infection in patients on renal replacement therapy. Report of the COVID-19 Registry of the Spanish Society of Nephrology (SEN). Nefrologia 2020, 40, 272–278. [Google Scholar] [CrossRef] [PubMed]
- Alberici, F.; Delbarba, E.; Manenti, C.; Econimo, L.; Valerio, F.; Pola, A.; Maffei, C.; Possenti, S.; Lucca, B.; Cortinovis, R.; et al. A report from the Brescia Renal COVID Task Force on the clinical characteristics and short-term outcome of hemodialysis patients with SARS-CoV-2 infection. Kidney Int. 2020, 98, 20–26. [Google Scholar] [CrossRef]
- Craved, P.; Mothi, S.S.; Azzi, Y.; Haverly, M.; Farouk, S.S.; Pérez-Sáez, M.J.; Redondo-Pachón, M.D.; Murphy, B.; Florman, S.; Cyrino, L.G.; et al. COVID-19 and kidney transplantation: Results from the TANGO International Transplant Consortium. Am. J. Transplant. 2020, 20, 3140–3148. [Google Scholar] [CrossRef]
- Scarpioni, R.; Manini, A.; Valsania, T.; De Amicis, S.; Albertazzi, V.; Melfa, L.; Ricardi, M.; Rocca, C. Covid-19 and its impact on nephropathic patients: The experience at Ospedale “Guglielmo da Saliceto” in Piacenza. G. Ital. Nefrol. 2020, 37, 1–5. [Google Scholar]
- Meijers, B.; Messa, P.; Ronco, C. Safeguarding the Maintenance Hemodialysis Patient Population during the Coronavirus Disease 19 Pandemic. Blood Purif. 2020, 49, 259–264. [Google Scholar] [CrossRef]
- Park, H.C.; Kim, D.H.; Yoo, K.D.; Kim, Y.G.; Lee, S.H.; Yoon, H.E.; Kim, D.K.; Kim, S.N.; Kim, M.S.; Jung, Y.C.; et al. Korean Society of Nephrology COVID-19 Task Force Team. Korean clinical practice guidelines for preventing transmission of coronavirus disease 2019 (COVID-19) in hemodialysis facilities. Kidney Res. Clin. Pract. 2020, 39, 145–150. [Google Scholar] [CrossRef]
- Gandhi, M.; Yokoe, D.S.; Havlir, D.V. Asymptomatic Transmission, the Achilles’ Heel of Current Strategies to Control Covid-19. N. Engl. J. Med. 2020, 382, 2158–2160. [Google Scholar] [CrossRef] [PubMed]
- Ikizler, T.A. COVID-19 and Dialysis Units: What Do We Know Now and What Should We Do? Am. J. Kidney Dis. 2020, 76, 1–3. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.J.; Lin, C.Y.; Chiu, Y.W.; Hwang, S.J. Take proactive measures for the pandemic COVID-19 infection in the dialysis facilities. J. Formos. Med. Assoc. 2020, 119, 895–897. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.H.; Sun, R.H.; Zhao, M.Y.; Chen, E.Z.; Liu, J.; Wang, H.L.; Yang, R.L.; Chen, D.C. Expert recommendations on blood purification treatment protocol for patients with severe COVID-19: Recommendation and consensus. Chronic Dis. Transl. Med. 2020, 6, 106–114. [Google Scholar] [CrossRef]
- Quintaliani, G.; Reboldi, G.; Di Napoli, A.; Nordio, M.; Limido, A.; Aucella, F.; Messa, P.; Brunori, G. Italian Society of Nephrology COVID-19 Research Group. Exposure to novel coronavirus in patients on renal replacement therapy during the exponential phase of COVID-19 pandemic: Survey of the Italian Society of Nephrology. J. Nephrol. 2020, 33, 725–736. [Google Scholar] [CrossRef]
- Ozturk, S.; Turgutalp, K.; Arici, M.; Odabas, A.R.; Altiparmak, M.R.; Aydin, Z.; Cebeci, E.; Basturk, T.; Soypacaci, Z.; Sahin, G.; et al. Mortality analysis of COVID-19 infection in chronic kidney disease, haemodialysis and renal transplant patients compared with patients without kidney disease: A nationwide analysis from Turkey. Nephrol. Dial. Transplant. 2020, 35, 2083–2095. [Google Scholar] [CrossRef]
- Martino, F.; Plebani, M.; Ronco, C. Kidney transplant programmes during the COVID-19 pandemic. Lancet Respir. Med. 2020, 8, e39. [Google Scholar] [CrossRef]
- Rehman, M.F.U.; Fariha, C.; Anwar, A.; Shahzad, N.; Ahmad, M.; Mukhtar, S.; Farhan, U.L.; Haque, M. Novel coronavirus disease (COVID-19) pandemic: A recent mini review. Comput. Struct. Biotechnol. J. 2021, 19, 612–623. [Google Scholar] [CrossRef]
- Ahn, D.G.; Shin, H.J.; Kim, M.H.; Lee, S.; Kim, H.S.; Myoung, J.; Kim, B.T.; Kim, S.J. Current Status of Epidemiology, Diagnosis, Therapeutics, and Vaccines for Novel Coronavirus Disease 2019 (COVID-19). J. Microbiol. Biotechnol. 2020, 30, 313–324. [Google Scholar] [CrossRef]
- Novel Coronavirus Disease 2019 (COVID-19) Pandemic: Increased Transmission in the EU/EEA and the UK – Sixth Update. Available online: https://www.ecdc.europa.eu/sites/default/files/documents/RRA-sixth-update-Outbreak-of-novel-coronavirus-disease-2019-COVID-19.pdf (accessed on 12 March 2020).
- Ai, T.; Yang, Z.; Hou, H.; Zhan, C.; Chen, C.; Lv, W.; Tao, Q.; Sun, Z.; Xia, L. Correlation of Chest CT and RT-PCR Testing for Coronavirus Disease 2019 (COVID-19) in China: A Report of 1014 Cases. Radiology 2020, 296, E32–E40. [Google Scholar] [CrossRef] [Green Version]
- Lippi, G.; Simundic, A.M.; Plebani, M. Potential preanalytical and analytical vulnerabilities in the laboratory diagnosis of coronavirus disease 2019 (COVID-19). Clin. Chem. Lab. Med. 2020, 58, 1070–1076. [Google Scholar] [CrossRef] [Green Version]
- Cao, G.; Tang, S.; Yang, D.; Shi, W.; Wang, X.; Wang, H.; Li, C.; Wei, J.; Ma, L. The potential transmission of SARS-CoV-2 from patients with negative RT-PCR swab tests to others: Two related clusters of COVID-19 outbreak. Jpn. J. Infect. Dis. 2020. [Google Scholar] [CrossRef] [PubMed]
- Winichakoon, P.; Chaiwarith, R.; Liwsrisakun, C.; Salee, P.; Goonna, A.; Limsukon, A.; Kaewpoowat, Q. Negative Nasopharyngeal and Oropharyngeal Swabs Do Not Rule Out COVID-19. J. Clin. Microbiol. 2020, 58, e00297-e20. [Google Scholar] [CrossRef] [Green Version]
- Bwire, G.M.; Majigo, M.V.; Njiro, B.J.; Mawazo, A. Detection profile of SARS-CoV-2 using RT-PCR in different types of clinical specimens: A systematic review and meta-analysis. J. Med. Virol. 2020. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Tan, L.; Wang, X.; Liu, W.; Lu, Y.; Cheng, L.; Sun, Z. Comparison of nasopharyngeal and oropharyngeal swabs for SARS-CoV-2 detection in 353 patients received tests with both specimens simultaneously. Int. J. Infect. Dis. 2020, 94, 107–109. [Google Scholar] [CrossRef] [PubMed]
- Mohammadi, A.; Esmaeilzadeh, E.; Li, Y.; Bosch, R.J.; Li, J. SARS-CoV-2 Detection in Different Respiratory Sites: A Systematic Review and Meta-Analysis. medRxiv 2020. [Google Scholar] [CrossRef]
- McCormick-Baw, C.; Morgan, K.; Gaffney, D.; Cazares, Y.; Jaworski, K.; Byrd, A.; Molberg, K.; Cavuoti, D. Saliva as an Alternate Specimen Source for Detection of SARS-CoV-2 in Symptomatic Patients Using Cepheid Xpert Xpress SARS-CoV-2. J. Clin. Microbiol. 2020, 58, e01109-20. [Google Scholar] [CrossRef]
- Pasomsub, E.; Watcharananan, S.P.; Boonyawat, K.; Janchompoo, P.; Wongtabtim, G.; Suksuwan, W.; Sungkanuparph, S.; Phuphuakrat, A. Saliva sample as a non-invasive specimen for the diagnosis of coronavirus disease 2019: A cross-sectional study. Clin. Microbiol. Infect. 2020. [Google Scholar] [CrossRef]
- Lukassen, S.; Chua, R.L.; Trefzer, T.; Kahn, N.C.; Schneider, M.A.; Muley, T.; Winter, H.; Meister, M.; Veith, C.; Boots, A.W.; et al. SARS-CoV-2 receptor ACE2 and TMPRSS2 are primarily expressed in bronchial transient secretory cells. EMBO J. 2020, 39, e105114. [Google Scholar] [CrossRef]
- Zou, L.; Ruan, F.; Huang, M.; Liang, L.; Huang, H.; Hong, Z.; Yu, J.; Kang, M.; Song, Y.; Xia, J.; et al. SARS-CoV-2 Viral Load in Upper Respiratory Specimens of Infected Patients. N. Engl. J. Med. 2020, 382, 1177–1179. [Google Scholar] [CrossRef]
- Yang, J.R.; Deng, D.T.; Wu, N.; Yang, B.; Li, H.J.; Pan, X.B. Persistent viral RNA positivity during the recovery period of a patient with SARS-CoV-2 infection. J. Med. Virol. 2020. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Li, L. SARS-CoV-2: Virus dynamics and host response. Lancet Infect. Dis. 2020, 20, 515–516. [Google Scholar] [CrossRef] [Green Version]
- Song, F.; Zhang, X.; Zha, Y.; Liu, W. COVID-19: Recommended sampling sites at different stages of the disease. J. Med. Virol. 2020. [Google Scholar] [CrossRef] [PubMed]



| Symptoms/Signs | Increased Risk of ARDS | Increased Risk of Death |
|---|---|---|
| Cough | At onset ≈ | At onset + |
| Fever | At onset +++ | At onset +++ |
| Shortness of breath | At onset +++ | At onset ++ |
| Gastrointestinal symptoms nausea vomiting diarrhea | Not significant | Not significant |
| Pharyngitis | Not significant | Not significant |
| Shortness of breath | Not significant | Not significant |
| Myalgia | At onset ++ | Not significant |
| Blood examination | Not significant | Not significant |
| Lymphocytes decrease | Not significant | Not significant |
| Platelets decrease | Not significant | Not significant |
| C-RP increase | >50 mg/L + | >50 mg/L ++ |
| AST/ALT increase | >50 U/L + | Not significant |
| LDH increase | Not significant | Not significant |
| Infiltrates at the chest X-ray | At onset + | Pneumonia ++ |
| Company (Assay Name) | Gene Target | LoD | Specimen Types | Approval |
|---|---|---|---|---|
| Abbott Diagnostics (ID NOW COVID-19) | RdRp | 125 copies/mL | Nasal, throat, NPS | FDA (US) |
| Abbott Molecular (Abbott RealTime SARS-CoV-2 EUA Test) | RdRp, N | 100 virus copies/mL | NPS, OPS, nasal swab, BAL | FDA (US) CE-IVD |
| Cepheid (Xpert Xpress SARS CoV-2) | N2, E | 250 copies/mL | NPS, OPS, nasal, mid-turbinate swab, nasal wash/aspirate | FDA (US), Health Canada, Australia, Singapore, Philippines, Brazil |
| DiaSorin Molecular (LIAISON MDX) | ORF1ab, S gene | NPS: 500 copies/mL, Nasal swab: 242 copies/mL | Nasal swab, NPS, nasal wash/aspirate, BAL | CE-IVD |
| Tib Molbiol (Modular DX kit SARS-CoV-2) | E | 1–10 copies/reaction | OPS, NPS | RUO (research use only) |
| Roche Molecular System (Cobas 6800 SARS-CoV-2) | ORF-1a/b, E | 1000 RNA genome equivalents/mL | NPS, OPS | US-FDA, CE-IVD |
| Seegene (Allplex 2019-nCoV Assay) | RdRp, N, E | 100 RNA copies/rxn | NPS, NPA, OPS, sputum, BAL | Korea (Korea CDC), US-FDA, CE-IVD |
| bioMerieux (ARGENE SARS-CoV-2 R-GENE) | RdRp, N, E | 380 genomic copies/mL | NPS | RUO (research use only) |
| Sample Sites | Asymptomatic Phase | Onset of the Symptomatic Phase | Symptomatic Phase | Convalescence Phase |
|---|---|---|---|---|
| Naso-pharyngeal swabs | Unclear | Highly recommended Detection rate: 80% | Recommended Detection rate: 59% | Recommended Detection rate: 36% |
| Oro-pharyngeal swabs | Unclear | Highly recommended Detection rate: 75% | Not recommended Detection rate: 35% | Not recommended Detection rate: 12% |
| Saliva collection | Unclear | Highly recommended Detection rate: 82.2% | Unclear | Unclear |
| Sputum collection | Unclear | Highly recommended Detection rate: 98% | Highly recommended Detection rate: 69% | Not recommended Detection rate: 46% |
| Bronco-alveolar lavage | Unclear/not recommend | Unclear/not recommended | Highly recommended in intubated patients Detection rate: 94% | Not recommend |
| Fecal/anal swabs | Not recommend | Not recommended Detection rate: 48% | Not recommended | Recommended Detection rate: 73% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martino, F.; Amici, G.; Grandesso, S.; Ferraro Mortellaro, R.; Lo Cicero, A.; Novara, G. Analysis of the Clinical and Epidemiological Meaning of Screening Test for SARS-CoV-2: Considerations in the Chronic Kidney Disease Patients during the COVID-19 Pandemic. J. Clin. Med. 2021, 10, 1139. https://doi.org/10.3390/jcm10051139
Martino F, Amici G, Grandesso S, Ferraro Mortellaro R, Lo Cicero A, Novara G. Analysis of the Clinical and Epidemiological Meaning of Screening Test for SARS-CoV-2: Considerations in the Chronic Kidney Disease Patients during the COVID-19 Pandemic. Journal of Clinical Medicine. 2021; 10(5):1139. https://doi.org/10.3390/jcm10051139
Chicago/Turabian StyleMartino, Francesca, Gianpaolo Amici, Stefano Grandesso, Rosella Ferraro Mortellaro, Antonina Lo Cicero, and Giacomo Novara. 2021. "Analysis of the Clinical and Epidemiological Meaning of Screening Test for SARS-CoV-2: Considerations in the Chronic Kidney Disease Patients during the COVID-19 Pandemic" Journal of Clinical Medicine 10, no. 5: 1139. https://doi.org/10.3390/jcm10051139