
Prognostic Markers for Chorioamnionitis: IL-6, TNF-α, and MMP-8 in Vaginally Obtained Amniotic Fluid

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients and Samples
2.2. Statistical Analysis
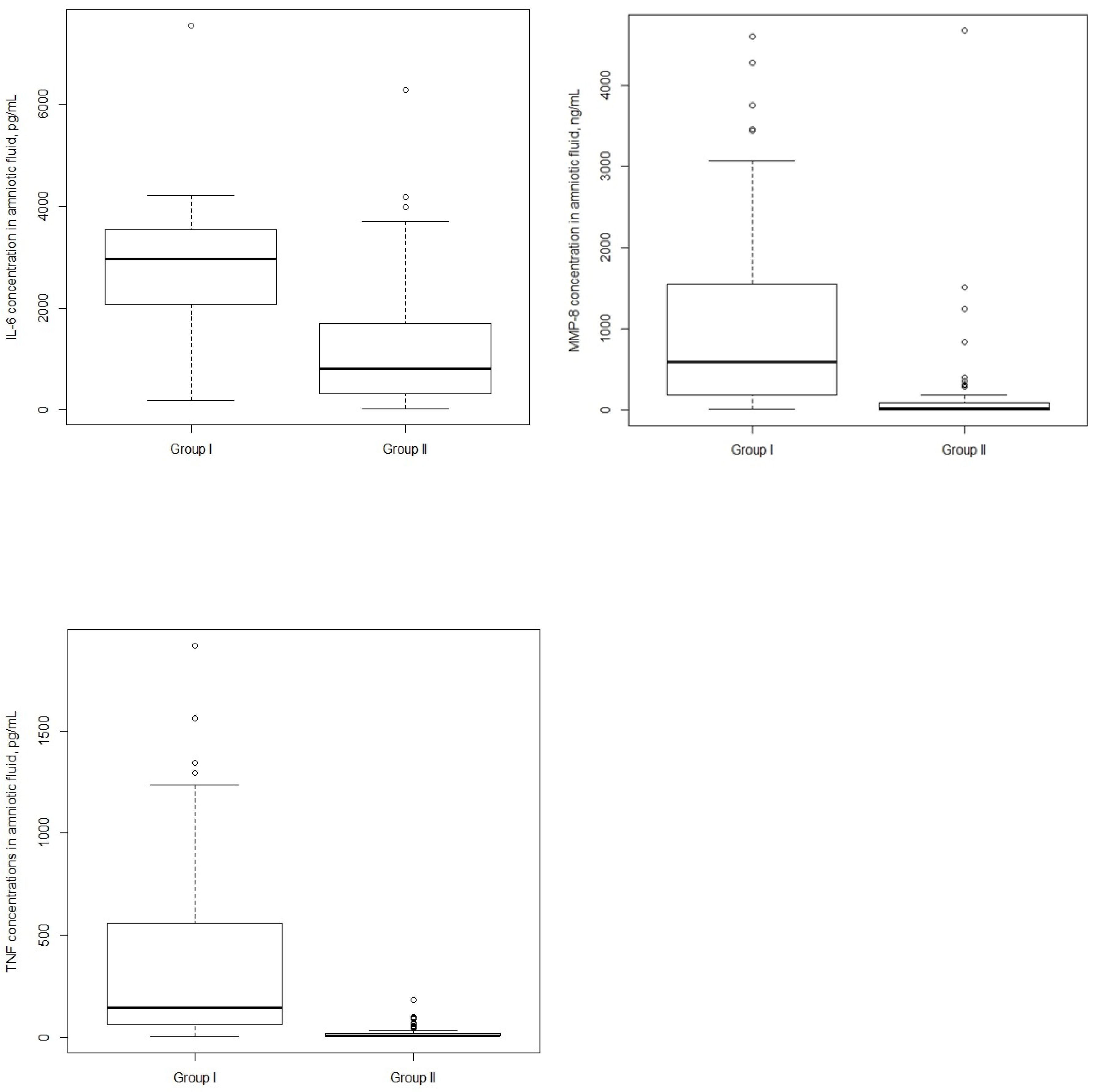
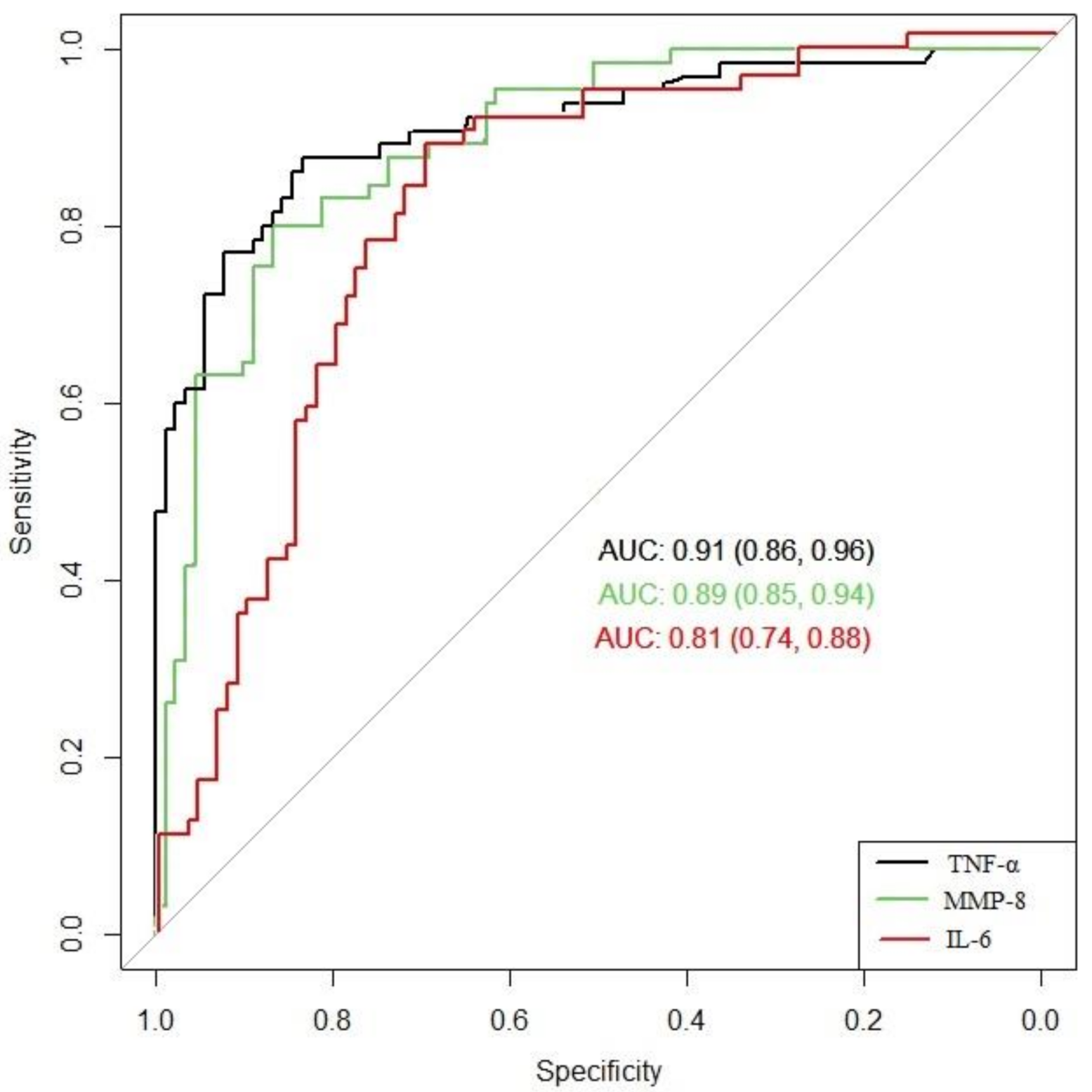
3. Results
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Tita, A.T.N.; Andrews, W.W. Diagnosis and Management of Clinical Chorioamnionitis. Clin. Perinatol. 2010, 37, 339–354. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mercer, B.M. Preterm premature rupture of the membranes. Obstet. Gynecol. 2003, 101, 178–193. [Google Scholar] [PubMed]
- Shatrov, J.G.; Birch, S.C.M.; Lam, L.T.; Quinlivan, J.A.; McIntyre, S.; Mendz, G.L. Chorioamnionitis and cerebral palsy: A meta-analysis. Obstet. Gynecol. 2010, 116, 387–392. [Google Scholar] [CrossRef] [PubMed]
- Ericson, J.E.; Laughon, M.M. Chorioamnionitis: Implications for the neonate. Clin. Perinatol. 2015, 42, 155–165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gibbs, R.S. Diagnosis of intra-amniotic infection. Semin. Perinatol. 1977, 1, 71–77. [Google Scholar] [PubMed]
- Sung, J.H.; Choi, S.J.; Oh, S.Y.; Roh, C.R.; Kim, J.H. Revisiting the diagnostic criteria of clinical chorioamnionitis in preterm birth. BJOG 2017, 5, 775–783. [Google Scholar] [CrossRef]
- Romero, R.; Chaemsaithong, P.; Korzeniewski, S.J.; Kusanovic, J.P.; Docheva, N.; Martinez-Varea, A.; Ahmed, A.I.; Yoon, B.H.; Hassan, S.S.; Chaiworapongsa, T.; et al. Clinical chorioamnionitis at term III: How well do clinical criteria perform in the identification of proven intra-amniotic infection? J. Perinat. Med. 2016, 44, 23–32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oh, K.J.; Kim, S.M.; Hong, J.S.; Maymon, E.; Erez, O.; Panaitescu, B.; Gomez-Lopez, N.; Romero, R.; Yoon, B.H. Twenty-four percent of patients with clinical chorioamnionitis in preterm gestations have no evidence of either culture-proven intraamniotic infection or intraamniotic inflammation. Am. J. Obstet. Gynecol. 2017, 216, 604.e1–604.e11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pugni, L.; Pietrasanta, C.; Acaia, B.; Merlo, D.; Ronchi, A.; Ossola, M.W.; Bosari, S.; Mosca, F. Chorioamnionitis and neonatal outcome in preterm infants: A clinical overview. J. Matern. Fetal Neonatal Med. 2016, 29, 1525–1529. [Google Scholar] [CrossRef] [PubMed]
- Ha, X.; Du, H.; Cao, Y.; Zhang, Y.; Zhang, J.; Zhang, L.; Li, Z.; Xu, Y.; Zou, H.; Sun, B. Association of histological and clinical chorioamnionitis with perinatal and neonatal outcome. J. Matern. Fetal Neonatal Med. 2019, 31, 1–9. [Google Scholar]
- Maki, Y.; Furukawa, S.; Nakayama, T.; Oohashi, M.; Shiiba, N.; Furuta, K.; Tokunaga, S.; Sameshima, H. Clinical chorioamnionitis criteria are not sufficient for predicting intraamniotic infection. J. Matern. Fetal Neonatal Med. 2020, 8, 1–6. [Google Scholar] [CrossRef]
- Liu, Y.; Liu, Y.; Du, C.; Zhang, R.; Feng, Z.; Zhang, J. Diagnostic value of amniotic fluid inflammatory biomarkers for subclinical chorioamnionitis. Int. J. Gynaecol. Obstet. 2016, 134, 160–164. [Google Scholar] [CrossRef]
- Soucek, O.; Kacerovsky, M.; Musilova, I.; Pliskova, L.; Bolehovska, R.; Andrys, C. Amniotic fluid CD11b levels in pregnancies complicated by preterm prelabor rupture of membranes. J. Matern. Fetal Neonatal Med. 2020, 19, 1–9. [Google Scholar] [CrossRef]
- Musilova, I.; Bestvina, T.; Stranik, J.; Stepan, M.; Jacobsson, B.; Kacerovsky, M. Transabdominal Amniocentesis Is a Feasible and Safe Procedure in Preterm Prelabor Rupture of Membranes. Fetal Diagn. Ther. 2017, 42, 257–261. [Google Scholar] [CrossRef] [PubMed]
- Le, J.M.; Vilcek, J. Interleukin 6: A multifunctional cytokine regulating immune reactions and the acute phase protein response. Lab. Invest. 1989, 61, 588–602. [Google Scholar]
- Dudley, D.J.; Trautman, M.S. Infection, inflammation, and contractions: The role of cytokines in the pathophysiology of preterm labor. Sem. Reprod. Endocrinol. 1994, 12, 263–272. [Google Scholar] [CrossRef]
- Kacerovsky, M.; Musilova, I.; Bestvina, T.; Stepan, M.; Cobo, C.; Jacobsson, B. Preterm Prelabor Rupture of Membranes between 34 and 37 Weeks: A Point-of-Care Test of Vaginal Fluid Interleukin-6 Concentrations for a Noninvasive Detection of Intra-Amniotic Inflammation. Fetal Diagn. Ther. 2018, 43, 175–183. [Google Scholar] [CrossRef] [PubMed]
- Kunze, M.; Klar, M.; Morfeld, C.A.; Thorns, B.; Schild, R.L.; Markfeld-Erol, F.; Rasenack, R.; Proempeler, H.; Hentschel, R.; Schaefer, V.R. Cytokines in noninvasively obtained amniotic fluid as predictors of fetal inflammatory response syndrome. Am. J. Obstet. Gynecol. 2016, 215, 96.e1–96.e8. [Google Scholar] [CrossRef]
- Kayem, G.; Batteux, F.; Girard, N.; Schmitz, T.; Willaime, M.; Maillard, F.; Jarreau, P.H.; Goffine, F. Predictive value of vaginal IL-6 and TNFα bedside tests repeated until delivery for the prediction of maternal-fetal infection in cases of premature rupture of membranes. Eur. J. Obstet. Gynecol. Reprod Biol. 2017, 211, 8–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soper, D.E.; Mayhall, C.G.; Dalton, H.P. Risk factors for intraamniotic infection: A prospective epidemiologic study. Am. J. Obstet. Gynecol. 1989, 161, 562–566. [Google Scholar] [CrossRef]
- Newton, E.R. Chorioamnionitis and intraamniotic infection. Clin. Obstet. Gynecol. 1993, 36, 795–808. [Google Scholar] [CrossRef]
- Park, K.H.; Chaiworapongsa, T.; Kim, Y.M.; Espinoza, J.; Yoshimatsu, J.; Edwin, S.; Gomez, R.; Yoon, B.H.; Romero, R. Affiliations expand Matrix metalloproteinase 3 in parturition, premature rupture of the membranes, and microbial invasion of the amniotic cavity. J. Perinat. Med. 2003, 31, 12–22. [Google Scholar] [CrossRef] [PubMed]
- Weiss, A.; Goldman, S.; Shalev, E. The matrix metalloproteinases (MMPS) in the decidua and fetal membranes. Front. Biosci. 2007, 12, 649–659. [Google Scholar] [CrossRef] [Green Version]
- Chaiyasit, N.; Romero, R.; Chaemsaithong, P.; Docheva, N.; Bhatti, G.; Kusanovic, J.P. Clinical chorioamnionitis at term VIII: A rapid MMP-8 test for the identification of intra-amniotic inflammation. J. Perinat. Med. 2017, 45, 539–550. [Google Scholar] [CrossRef]
- Kim, S.M.; Romero, R.; Park, J.W.; Oh, K.J.; Jun, J.K.; Yoon, B.H. The relationship between the intensity of intra-amniotic inflammation and the presence and severity of acute histologic chorioamnionitis in preterm gestation. J. Matern. Fetal Neonatal Med. 2015, 28, 1500–1509. [Google Scholar] [CrossRef] [Green Version]
- Kim, K.W.; Romero, R.; Park, H.S.; Park, C.W.; Shim, S.S.; Jun, J.K.; Yoon, B.H. A rapid matrix metalloproteinase-8 bedside test for the detection of intraamniotic inflammation in women with preterm premature rupture of membranes. Am. J. Obstet. Gynecol. 2007, 197, 292.e1–292.e5. [Google Scholar] [CrossRef]
- Chaemsaithong, P.; Romero, R.; Docheva, N.; Chaiyasit, N.; Bhatti, G.; Pacora, P. Comparison of rapid MMP-8 and interleukin-6 point-of-care tests to identify intra-amniotic inflammation/infection and impending preterm delivery in patients with preterm labor and intact membranes. J. Matern. Fetal Neonatal Med. 2018, 31, 228–244. [Google Scholar] [CrossRef]
- Holmström, E.; Myntti, T.; Sorsa, E.; Kruit, H.; Juhila, J.; Paavonen, J.; Rahkonen, L.; Stefanovic, V. Cervical and Amniotic Fluid Matrix Metalloproteinase-8 and Interleukin-6 Concentrations in Preterm Pregnancies with or without Preterm Premature Rupture of Membranes. Fetal Diagn. Ther. 2019, 46, 103–110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kacerovsky, M.; Musilova, I.; Stepan, M.; Andrys, C.; Drahosova, M.; Jacobsson, B. Detection of intraamniotic inflammation in fresh and processed amniotic fluid samples with the interleukin-6 point of care test. Am. J. Obstet. Gynecol. 2015, 213, 435–436. [Google Scholar] [CrossRef] [PubMed]
- Romero, R.; Chaemsaithong, P.; Docheva, N.; Korzeniewski, S.J.; Kusanovic, J.P.; Yoon, B.H.; Kim, J.S.; Chaiyasit, N.; Ahmed, A.I.; Qureshi, F.; et al. Clinical chorioamnionitis at term VI: Acute chorioamnionitis and funisitis according to the presence or absence of microorganisms and inflammation in the amniotic cavity. J. Perinat. Med. 2016, 44, 33–51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ocheke, N.; Ocheke, I.E.; Agaba, P.A.; Imadde, G.E.; Silas, O.A.; Ajetunmobi, O.I.; Godwins, E.J.; Ekere, C.; Sendeht, A.; Bitrus, J.; et al. Maternal and Neonatal Outcomes of Histological Chorioamnionitis. J. West. Afr. Coll Surg. 2016, 6, 1–14. [Google Scholar] [PubMed]



{kind=link}
{kind=link}
| Characteristics | Group I (n = 65) | Group II (n = 91) | p-Value |
|---|---|---|---|
| Age of mother (years) | 30.6 ± 6.4 | 31.2 ± 5.8 | 0.53 |
| Primiparous, n (%) | 32 (49.2) | 46 (50.6) | 0.87 |
| Multiparous, n (%) | 33 (50.8) | 45 (49.4) | 0.87 |
| Primigravida, n (%) | 27 (41.5) | 34 (37.4) | 0.59 |
| Multigravida, n (%) | 38 (58.5) | 57 (62.6) | 0.59 |
| Gestational age at birth (weeks) | 32+0 (27+2–33+0) | 33+0 (28+1–33+5) | 0.13 |
| Latency between PPROM and delivery (hours) | 43 (26–93) | 41 (20–78) | 0.29 |
| Clinical chorioamnionitis, n (%) | 6 (9.2) | 1 (1%) | 0.002 |
| Birthweight (g) | 1768.2 ± 669.1 | 1872.7 ± 603.2 | 0.51 |
| Apgar score <7 at 5 min, n (%) | 6 (9.2) | 1 (1.1) | 0.02 |
| Umbilical cord arterial pH | 7.31 ± 0.09 | 7.35 ± 0.09 | 0.003 |
| Group B Streptococcus, n (%) | 24 (36.9) | 15 (16.5) | 0.003 |
| Gestational diabetes, n (%) | 16 (17.6) | 11 (16.9) | 0.91 |
| Hypertensive disorders, n (%) | 12 (13.2) | 8 (12.3) | 0.87 |
| Cut-off Values | Sensitivity % (95% CI) | Specificity % (95% CI) | Positive Predictive Value % (95% CI) | Negative Predictive Value % (95% CI) |
|---|---|---|---|---|
| IL-6 (pg/mL) | ||||
| 1389.82 | 88 (77–94) | 70 (60–79) | 67 (56–77) | 89 (79–95) |
| 2844.43 | 57 (44–69) | 85 (76–91) | 73 (58–84) | 73 (64–81) |
| 3427.52 | 37 (25–50) | 90 (82–95) | 73 (54–87) | 67 (58–75) |
| 4195.68 | 17 (9–28) | 96 (89–99) | 73 (45–92) | 62 (53–70) |
| MMP-8 (ng/mL) | ||||
| 413.67 | 63 (50–75) | 96 (89–99) | 91 (79–98) | 78 (70–86) |
| 294.36 | 65 (52–76) | 90 (82–95) | 82 (69–92) | 78 (69–86) |
| 172.53 | 80 (68–89) | 87 (78–93) | 81 (70–90) | 86 (77–92) |
| 124.5 | 83 (72–91) | 81 (72–89) | 76 (64–85) | 87 (78–93) |
| TNF-α (pg/mL) | ||||
| 70.77 | 72 (60–83) | 95 (88–98) | 90 (79–97) | 83 (74–89) |
| 50.39 | 78 (67–88) | 89 (81–95) | 84 (72–92) | 85 (77–92) |
| 24.56 | 86 (75–93) | 85 (76–91) | 80 (69–89) | 90 (81–95) |
| 21.17 | 88 (77–95) | 84 (74–90) | 79 (68–88) | 90 (82–96) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Balciuniene, G.; Gulbiniene, V.; Dumalakiene, I.; Viliene, R.; Bartkeviciene, D.; Pilypiene, I.; Drasutiene, G.S.; Ramasauskaite, D. Prognostic Markers for Chorioamnionitis: IL-6, TNF-α, and MMP-8 in Vaginally Obtained Amniotic Fluid. J. Clin. Med. 2021, 10, 1136. https://doi.org/10.3390/jcm10051136
Balciuniene G, Gulbiniene V, Dumalakiene I, Viliene R, Bartkeviciene D, Pilypiene I, Drasutiene GS, Ramasauskaite D. Prognostic Markers for Chorioamnionitis: IL-6, TNF-α, and MMP-8 in Vaginally Obtained Amniotic Fluid. Journal of Clinical Medicine. 2021; 10(5):1136. https://doi.org/10.3390/jcm10051136
Chicago/Turabian StyleBalciuniene, Greta, Violeta Gulbiniene, Irena Dumalakiene, Rita Viliene, Daiva Bartkeviciene, Ingrida Pilypiene, Grazina S. Drasutiene, and Diana Ramasauskaite. 2021. "Prognostic Markers for Chorioamnionitis: IL-6, TNF-α, and MMP-8 in Vaginally Obtained Amniotic Fluid" Journal of Clinical Medicine 10, no. 5: 1136. https://doi.org/10.3390/jcm10051136