
Interstitial Lung Disease Worsens Short- and Long-Term Outcomes of Systemic Rheumatic Disease Patients Admitted to the ICU: A Multicenter Study

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
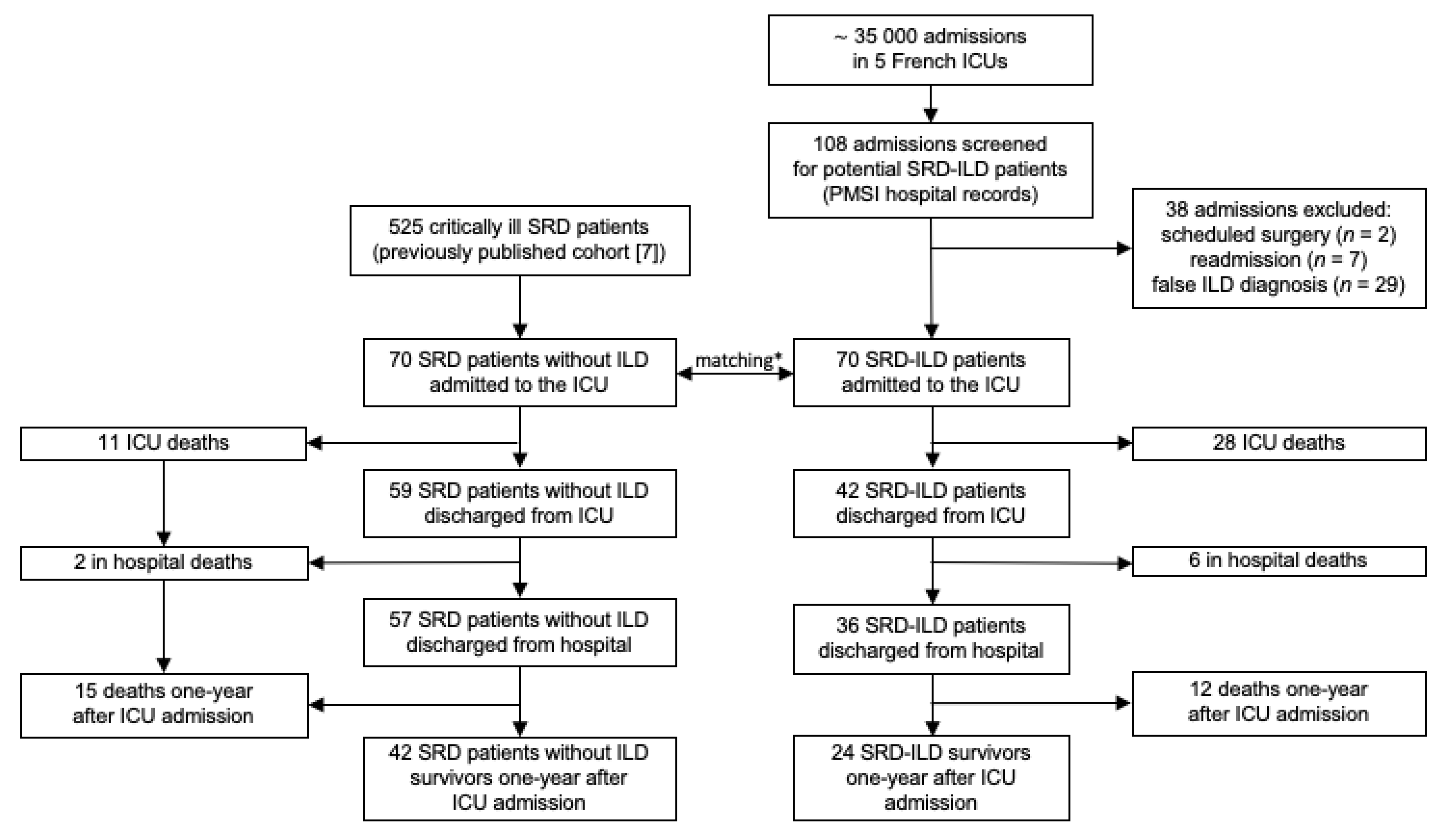
2.1. Patients
2.2. Data Collection
2.3. Outcomes
2.4. Statistical Analysis
2.5. Ethical Considerations
3. Results
3.1. General Characteristics of the Study Population
3.2. HRCT Patterns
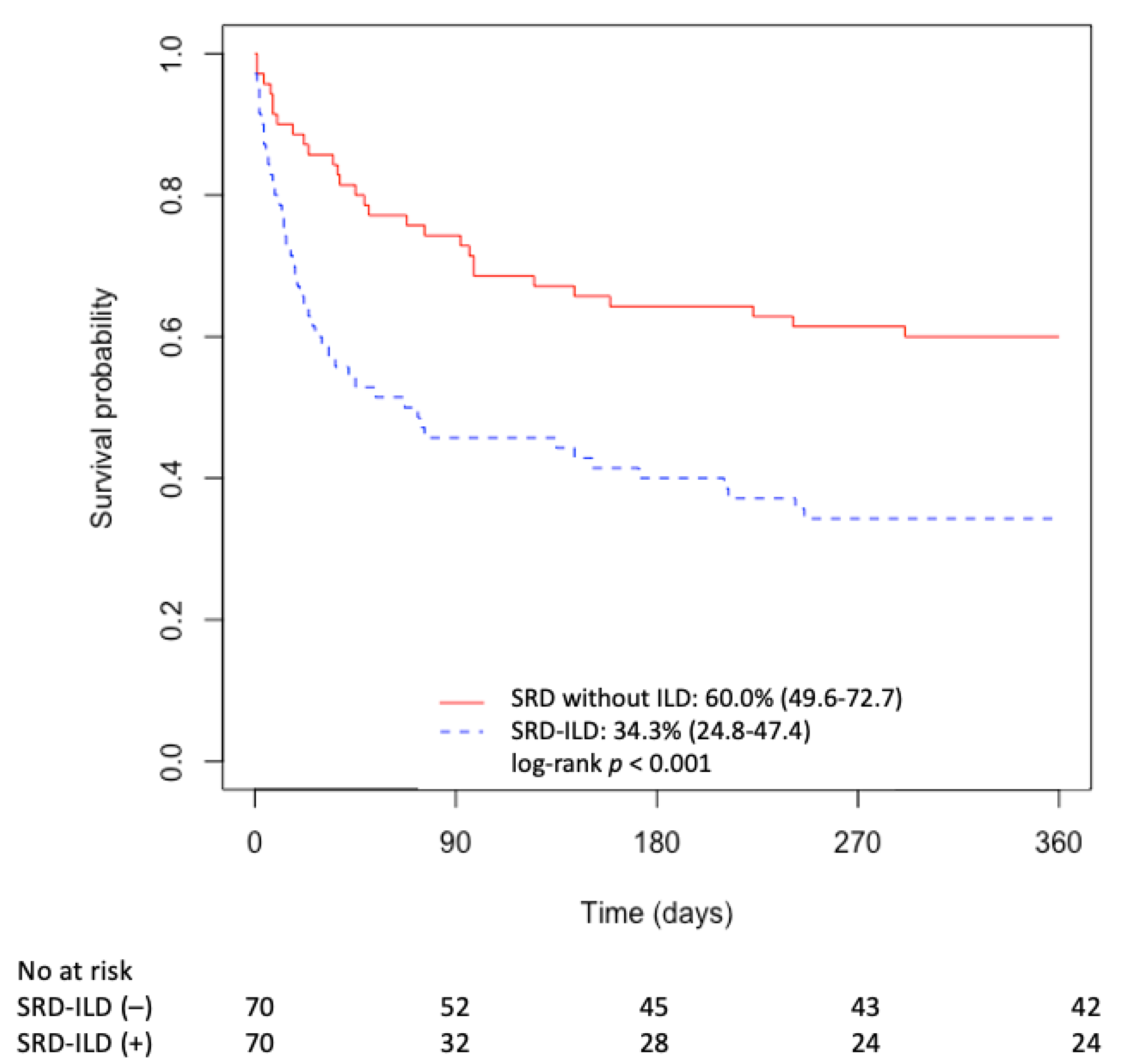
3.3. Outcomes
3.4. Prognostic Factors
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dumas, G.; Géri, G.; Montlahuc, C.; Chemam, S.; Dangers, L.; Pichereau, C.; Brechot, N.; Duprey, M.; Mayaux, J.; Schenck, M.; et al. Outcomes in Critically Ill Patients with Systemic Rheumatic Disease: A Multicenter Study. Chest 2015, 148, 927–935. [Google Scholar] [CrossRef] [PubMed]
- Fischer, A.; West, S.G.; Swigris, J.J.; Brown, K.K.; du Bois, R.M. Connective Tissue Disease-Associated Interstitial Lung Disease. Chest 2010, 138, 251–256. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Larcher, R.; de Chambrun, M.P.; Garnier, F.; Rubenstein, E.; Carr, J.; Charbit, J.; Chalard, K.; Mourad, M.; Amalric, M.; Platon, L.; et al. One-Year Outcome of Critically Ill Patients with Systemic Rheumatic Disease: A Multicenter Cohort Study. Chest 2020, 158, 1017–1026. [Google Scholar] [CrossRef]
- Fumeaux, T.; Rothmeier, C.; Jolliet, P. Outcome of Mechanical Ventilation for Acute Respiratory Failure in Patients with Pulmonary Fibrosis. Intensive Care Med. 2001, 27, 1868–1874. [Google Scholar] [CrossRef]
- Fernández-Pérez, E.R.; Yilmaz, M.; Jenad, H.; Daniels, C.E.; Ryu, J.H.; Hubmayr, R.D.; Gajic, O. Ventilator Settings and Outcome of Respiratory Failure in Chronic Interstitial Lung Disease. Chest 2008, 133, 1113–1119. [Google Scholar] [CrossRef] [Green Version]
- Vial-Dupuy, A.; Sanchez, O.; Douvry, B.; Guetta, L.; Juvin, K.; Wermert, D.; Guérot, E.; Israël-Biet, D. Outcome of Patients with Interstitial Lung Disease Admitted to the Intensive Care Unit. Sarcoidosis Vasc. Diffuse Lung Dis. Off. J. WASOG 2013, 30, 134–142. [Google Scholar]
- Huapaya, J.A.; Wilfong, E.M.; Harden, C.T.; Brower, R.G.; Danoff, S.K. Risk Factors for Mortality and Mortality Rates in Interstitial Lung Disease Patients in the Intensive Care Unit. Eur. Respir. Rev. 2018, 27, 180061. [Google Scholar] [CrossRef]
- Zafrani, L.; Lemiale, V.; Lapidus, N.; Lorillon, G.; Schlemmer, B.; Azoulay, E. Acute Respiratory Failure in Critically Ill Patients with Interstitial Lung Disease. PLoS ONE 2014, 9, e104897. [Google Scholar] [CrossRef]
- Hadley, R.; Hyzy, R. Critically Ill Patients with Interstitial Lung Disease. Clin. Chest Med. 2015, 36, 497–510. [Google Scholar] [CrossRef] [PubMed]
- Maillet, T.; Goletto, T.; Beltramo, G.; Dupuy, H.; Jouneau, S.; Borie, R.; Crestani, B.; Cottin, V.; Blockmans, D.; Lazaro, E.; et al. Usual Interstitial Pneumonia in ANCA-Associated Vasculitis: A Poor Prognostic Factor. J. Autoimmun. 2019, 102338. [Google Scholar] [CrossRef]
- Gannon, W.D.; Lederer, D.J.; Biscotti, M.; Javaid, A.; Patel, N.M.; Brodie, D.; Bacchetta, M.; Baldwin, M.R. Outcomes and Mortality Prediction Model of Critically Ill Adults with Acute Respiratory Failure and Interstitial Lung Disease. Chest 2018, 153, 1387–1395. [Google Scholar] [CrossRef]
- Mathai, S.C.; Danoff, S.K. Management of Interstitial Lung Disease Associated with Connective Tissue Disease. BMJ 2016, h6819. [Google Scholar] [CrossRef]
- van den Hoogen, F.; Khanna, D.; Fransen, J.; Johnson, S.R.; Baron, M.; Tyndall, A.; Matucci-Cerinic, M.; Naden, R.P.; Medsger, T.A.; Carreira, P.E.; et al. 2013 Classification Criteria for Systemic Sclerosis: An American College of Rheumatology/European League against Rheumatism Collaborative Initiative. Arthritis Rheum. 2013, 65, 2737–2747. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shiboski, C.H.; Shiboski, S.C.; Seror, R.; Criswell, L.A.; Labetoulle, M.; Lietman, T.M.; Rasmussen, A.; Scofield, H.; Vitali, C.; Bowman, S.J.; et al. 2016 American College of Rheumatology/European League Against Rheumatism Classification Criteria for Primary Sjögren’s Syndrome: A Consensus and Data-Driven Methodology Involving Three International Patient Cohorts. Arthritis Rheumatol. 2017, 69, 35–45. [Google Scholar] [CrossRef] [PubMed]
- Aletaha, D.; Neogi, T.; Silman, A.J.; Funovits, J.; Felson, D.T.; Bingham, C.O.; Birnbaum, N.S.; Burmester, G.R.; Bykerk, V.P.; Cohen, M.D.; et al. 2010 Rheumatoid Arthritis Classification Criteria: An American College of Rheumatology/European League Against Rheumatism Collaborative Initiative. Arthritis Rheum. 2010, 62, 2569–2581. [Google Scholar] [CrossRef] [PubMed]
- Hunder, G.G.; Arend, W.P.; Bloch, D.A.; Calabrese, L.H.; Fauci, A.S.; Fries, J.F.; Leavitt, R.Y.; Lie, J.T.; Lightfoot, R.W.; Masi, A.T. The American College of Rheumatology 1990 Criteria for the Classification of Vasculitis. Introduction. Arthritis Rheum. 1990, 33, 1065–1067. [Google Scholar] [CrossRef]
- Jennette, J.C.; Falk, R.J.; Bacon, P.A.; Basu, N.; Cid, M.C.; Ferrario, F.; Flores-Suarez, L.F.; Gross, W.L.; Guillevin, L.; Hagen, E.C.; et al. 2012 Revised International Chapel Hill Consensus Conference Nomenclature of Vasculitides. Arthritis Rheum. 2013, 65, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Sieper, J.; Rudwaleit, M.; Baraliakos, X.; Brandt, J.; Braun, J.; Burgos-Vargas, R.; Dougados, M.; Hermann, K.-G.; Landewé, R.; Maksymowych, W.; et al. The Assessment of SpondyloArthritis International Society (ASAS) Handbook: A Guide to Assess Spondyloarthritis. Ann. Rheum. Dis. 2009, 68 (Suppl. 2), ii1–ii44. [Google Scholar] [CrossRef]
- Fischer, A.; Antoniou, K.M.; Brown, K.K.; Cadranel, J.; Corte, T.J.; du Bois, R.M.; Lee, J.S.; Leslie, K.O.; Lynch, D.A.; Matteson, E.L.; et al. An Official European Respiratory Society/American Thoracic Society Research Statement: Interstitial Pneumonia with Autoimmune Features. Eur. Respir. J. 2015, 46, 976–987. [Google Scholar] [CrossRef] [Green Version]
- Aringer, M.; Costenbader, K.; Daikh, D.; Brinks, R.; Mosca, M.; Ramsey-Goldman, R.; Smolen, J.S.; Wofsy, D.; Boumpas, D.T.; Kamen, D.L.; et al. 2019 European League Against Rheumatism/American College of Rheumatology Classification Criteria for Systemic Lupus Erythematosus. Arthritis Rheumatol. 2019, 71, 1400–1412. [Google Scholar] [CrossRef] [Green Version]
- Bottai, M.; Tjärnlund, A.; Santoni, G.; Werth, V.P.; Pilkington, C.; de Visser, M.; Alfredsson, L.; Amato, A.A.; Barohn, R.J.; Liang, M.H.; et al. EULAR/ACR Classification Criteria for Adult and Juvenile Idiopathic Inflammatory Myopathies and Their Major Subgroups: A Methodology Report. RMD Open 2017, 3, e000507. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- American Thoracic Society; European Respiratory Society. American Thoracic Society/European Respiratory Society International Multidisciplinary Consensus Classification of the Idiopathic Interstitial Pneumonias: This Joint Statement of the American Thoracic Society (ATS), and the European Respiratory Society (ERS) Was Adopted by the ATS Board of Directors, June 2001 and by The ERS Executive Committee, June 2001. Am. J. Respir. Crit. Care Med. 2002, 165, 277–304. [Google Scholar] [CrossRef] [Green Version]
- Collard, H.R.; Ryerson, C.J.; Corte, T.J.; Jenkins, G.; Kondoh, Y.; Lederer, D.J.; Lee, J.S.; Maher, T.M.; Wells, A.U.; Antoniou, K.M.; et al. Acute Exacerbation of Idiopathic Pulmonary Fibrosis. An International Working Group Report. Am. J. Respir. Crit. Care Med. 2016, 194, 265–275. [Google Scholar] [CrossRef]
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.-D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801. [Google Scholar] [CrossRef]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A New Method of Classifying Prognostic Comorbidity in Longitudinal Studies: Development and Validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Vincent, J.L.; Moreno, R.; Takala, J.; Willatts, S.; De Mendonça, A.; Bruining, H.; Reinhart, C.K.; Suter, P.M.; Thijs, L.G. The SOFA (Sepsis-Related Organ Failure Assessment) Score to Describe Organ Dysfunction/Failure. On Behalf of the Working Group on Sepsis-Related Problems of the European Society of Intensive Care Medicine. Intensive Care Med. 1996, 22, 707–710. [Google Scholar] [CrossRef]
- Teasdale, G.; Jennett, B. Assessment of Coma and Impaired Consciousness. A Practical Scale. Lancet 1974, 2, 81–84. [Google Scholar] [CrossRef]
- Le Gall, J.R.; Lemeshow, S.; Saulnier, F. A New Simplified Acute Physiology Score (SAPS II) Based on a European/North American Multicenter Study. JAMA 1993, 270, 2957–2963. [Google Scholar] [CrossRef] [PubMed]
- The ARDS Definition Task Force. Acute Respiratory Distress Syndrome: The Berlin Definition. JAMA 2012, 307, 2526–2533. [Google Scholar] [CrossRef]
- Kidney Disease: Improving Global Outcomes (KDIGO) Acute Kidney Injury Work Group. KDIGO Clinical Practice Guideline for Acute Kidney Injury. Kidney Int. Suppl. 2012, 2, 1–138. [Google Scholar] [CrossRef]
- Vittinghoff, E.; McCulloch, C.E. Relaxing the Rule of Ten Events per Variable in Logistic and Cox Regression. Am. J. Epidemiol. 2007, 165, 710–718. [Google Scholar] [CrossRef] [Green Version]
- Janssen, N.M.; Karnad, D.R.; Guntupalli, K.K. Rheumatologic Diseases in the Intensive Care Unit: Epidemiology, Clinical Approach, Management, and Outcome. Crit. Care Clin. 2002, 18, 729–748. [Google Scholar] [CrossRef]
- Gaudry, S.; Vincent, F.; Rabbat, A.; Nunes, H.; Crestani, B.; Naccache, J.M.; Wolff, M.; Thabut, G.; Valeyre, D.; Cohen, Y.; et al. Invasive Mechanical Ventilation in Patients with Fibrosing Interstitial Pneumonia. J. Thorac. Cardiovasc. Surg. 2014, 147, 47–53. [Google Scholar] [CrossRef] [Green Version]
- Mallick, S. Outcome of Patients with Idiopathic Pulmonary Fibrosis (IPF) Ventilated in Intensive Care Unit. Respir. Med. 2008, 102, 1355–1359. [Google Scholar] [CrossRef] [Green Version]
- Nash, G.; Blennerhassett, J.B.; Pontoppidan, H. Pulmonary Lesions Associated with Oxygen Therapy and Artificial Ventilation. N. Engl. J. Med. 1967, 276, 368–374. [Google Scholar] [CrossRef] [PubMed]
- Kimmoun, A.; Baux, E.; Das, V.; Terzi, N.; Talec, P.; Asfar, P.; Ehrmann, S.; Geri, G.; Grange, S.; Anguel, N.; et al. Outcomes of Patients Admitted to Intensive Care Units for Acute Manifestation of Small-Vessel Vasculitis: A Multicenter, Retrospective Study. Crit. Care 2015, 20, 27. [Google Scholar] [CrossRef] [Green Version]
- Distler, O.; Highland, K.B.; Gahlemann, M.; Azuma, A.; Fischer, A.; Mayes, M.D.; Raghu, G.; Sauter, W.; Girard, M.; Alves, M.; et al. Nintedanib for Systemic Sclerosis–Associated Interstitial Lung Disease. N. Engl. J. Med. 2019, 380, 2518–2528. [Google Scholar] [CrossRef]
- Prieto-Peña, D.; Martínez-Meñaca, A.; Calderón-Goercke, M.; Mora-Cuesta, V.M.; Fernández-Rozas, S.; Iturbe-Fernández, D.; Gómez-Román, J.J.; Cifrián-Martínez, J.M.; Castañeda, S.; Hernández, J.L.; et al. Long-Term Survival of Lung Transplantation for Interstitial Lung Disease Associated with Connective Tissue Diseases: A Study of 26 Cases from a Referral Centre. Clin. Exp. Rheumatol. 2020, 38, 615–620. [Google Scholar]
- Park, J.E.; Kim, S.Y.; Song, J.H.; Kim, Y.S.; Chang, J.; Lee, J.G.; Paik, H.C.; Park, M.S. Comparison of Short-Term Outcomes for Connective Tissue Disease-Related Interstitial Lung Disease and Idiopathic Pulmonary Fibrosis after Lung Transplantation. J. Thorac. Dis. 2018, 10, 1538–1547. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gattinoni, L.; Tonetti, T.; Cressoni, M.; Cadringher, P.; Herrmann, P.; Moerer, O.; Protti, A.; Gotti, M.; Chiurazzi, C.; Carlesso, E.; et al. Ventilator-Related Causes of Lung Injury: The Mechanical Power. Intensive Care Med. 2016, 42, 1567–1575. [Google Scholar] [CrossRef]
- Brochard, L.; Slutsky, A.; Pesenti, A. Mechanical Ventilation to Minimize Progression of Lung Injury in Acute Respiratory Failure. Am. J. Respir. Crit. Care Med. 2017, 195, 438–442. [Google Scholar] [CrossRef]
- Slutsky, A.S.; Ranieri, V.M. Ventilator-Induced Lung Injury. N. Engl. J. Med. 2013, 369, 2126–2136. [Google Scholar] [CrossRef] [Green Version]
- Vianello, A.; Arcaro, G.; Paladini, L.; Iovino, S. Successful Management of Acute Respiratory Failure in an Idiopathic Pulmonary Fibrosis Patient Using an Extracorporeal Carbon Dioxide Removal System. Sarcoidosis Vasc. Diffuse Lung Dis. Off. J. WASOG 2016, 33, 186–190. [Google Scholar]
- Huang, J.; Liu, C.; Zhu, R.; Su, Y.; Lin, J.; Lu, J.; Wen, S.; Zuo, L. Combined Usage of Extracorporeal Membrane Oxygenation and Double Filtration Plasmapheresis in Amyopathic Dermatomyositis Patient with Severe Interstitial Lung Disease: A Case Report. Medicine 2018, 97, e10946. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| All Patients n = 70 | ICU Deceased n = 28 | ICU Survived n = 42 | p-Value (Univariate Analysis) | |
|---|---|---|---|---|
| Characteristics at admission | ||||
| Sex (Male), n (%) | 32 (45.7) | 13 (46.4) | 19 (45.2) | 1.00 |
| Age (years), median (IQR) | 65.0 (58.4–73.7) | 63.3 (57.4–70.6) | 65.9 (59.2–73.9) | 0.49 |
| BMI, median (IQR) | 25.1 (21.7–27.0) | 25.1 (23.2–26.1) | 25.1 (21.1–27.9) | 0.90 |
| Charlson index, median (IQR) | 4 (3–6) | 4 (3–6) | 5 (4–6) | 0.66 |
| SAPS II, median (IQR) | 43 (32–59) | 49 (41–66) | 40 (30–50) | 0.02 |
| SOFA score, median (IQR) | 7 (4–9) | 8 (5–13) | 6 (3–8) | 0.03 |
| Non-pulmonary SOFA score, median (IQR) | 4 (2–6) | 4 (1–10) | 4 (2–6) | 0.39 |
| Serum creatinine (µmol/L), median (IQR) | 146 (102–268) | 171 (109–252) | 127 (85–322) | 0.67 |
| SRD Type | ||||
| CTD, n (%) | 39 (55.7) | 19 (67.8) | 20 (47.6) | 0.05 |
| Vasculitis, n (%) | 20 (28.6) | 4 (14.3) | 16 (38.1) | |
| Sarcoidosis, n (%) | 9 (12.8) | 3 (10.7) | 6 (14.3) | |
| Spondylarthritis, n (%) | 2 (2.9) | 2 (7.1) | 0 (0.0) | |
| Treatment before admission | ||||
| Corticosteroids, n (%) | 38 (54.3) | 18 (64.3) | 20 (47.6) | 0.26 |
| Immunosuppressive, n (%) | 19 (27.1) | 9 (32.1) | 10 (23.8) | 0.62 |
| Treatment during hospitalization | ||||
| Corticosteroids, n (%) | 56 (80.0) | 23 (82.1) | 33 (78.6) | 0.95 |
| Dose of corticosteroids (mg/kg/day), median (IQR) | 1.00 (0.10–1.00) | 1.00 (0.11–1.37) | 0.50 (0.10–1.00) | 0.37 |
| Immunosuppressive, n (%) | 18 (25.7) | 11 (39.3) | 7 (16.7) | 0.06 |
| Plasma exchange, n (%) | 7 (10.0) | 3 (10.7) | 4 (9.5) | 1.00 |
| Reason for admission | ||||
| Acute respiratory failure related to a pulmonary disease, n (%) | 39 (55.7) | 21 (75.0) | 18 (42.9) | 0.02 |
| Other, n (%) | 31 (44.3) | 7 (25.0) | 24 (57.1) | |
| Diagnosis | ||||
| Infection, n (%) | 24 (34.3) | 9 (32.1) | 15 (35.7) | <0.01 |
| Acute exacerbation, n (%) | 25 (35.7) | 16 (57.1) | 9 (21.4) | |
| Other, n (%) | 21 (30.0) | 3 (10.7) | 18 (42.9) | |
| KDIGO stage | ||||
| 0, n (%) | 19 (27.1) | 6 (21.4) | 13 (31.0) | 0.26 |
| 1, n (%) | 12 (17.1) | 4 (14.3) | 8 (19.0) | |
| 2, n (%) | 6 (8.6) | 1 (3.6) | 5 (11.9) | |
| 3, n (%) | 33 (47.1) | 17 (60.7) | 16 (38.1) | |
| Worst PaO2/FiO2 | ||||
| <100 | 28 (40.0) | 20 (71.4) | 8 (19.0) | <0.01 |
| 100–199 | 15 (21.4) | 4 (14.3) | 11 (26.2) | |
| ≥200 | 27 (38.6) | 4 (14.3) | 23 (54.8) | |
| Organ support | ||||
| Vasoactive drugs, n (%) | 38 (54.3) | 21 (75.0) | 17 (40.5) | <0.01 |
| Invasive ventilation, n (%) | 44 (62.8) | 26 (92.8) | 18 (42.9) | <0.01 |
| Prone positioning, n (%) | 7 (10.0) | 5 (17.9) | 2 (4.8) | 0.17 |
| Renal replacement therapy, n (%) | 24 (34.3) | 14 (50.0) | 10 (23.8) | 0.04 |
| Outcomes | ||||
| Length of ICU stay (days), median (IQR) | 7 (3–20) | 11 (4–24) | 6 (2–16) | - |
| ICU-acquired infection, n (%) | 14 (20.0) | 5 (17.8) | 9 (21.4) | 0.95 |
| Death in ICU, n (%) | 28 (40.0) | 28 (100%) | 0 (0%) | - |
| Death at one year, n (%) | 46 (65.7) | - | 18 (43%) | - |
| Patients with HRCT n = 61 | Death in ICU n = 22 | Alive in ICU n = 39 | p-Value (Univariate Analysis) | |
|---|---|---|---|---|
| ILD radiologic pattern | ||||
| Unclassifiable, n (%) | 25 (41) | 6 (27.3) | 22 (56.4) | 0.05 |
| AIP, n (%) | 5 (8) | 4 (18.2) | 1 (2.6) | |
| NSIP, n (%) | 17 (28) | 8 (36.4) | 9 (23.1) | |
| UIP, n (%) | 11 (18) | 4 (18.2) | 7 (17.9) | |
| Fibrosis, n (%) | 40 (66) | 16 (72.7) | 24 (61.5) | 0.55 |
| Acute lung injury radiological pattern, n (%) | 37 (61) | 19 (86.4) | 18 (46.1) | 0.004 |
| SRD without ILD n = 70 | SRD with ILD n = 70 | p-Value (Univariate Analysis) | |
| Patient characteristics at admission | |||
| Sex (Male), n (%) | 32 (45,7) | 32 (45.7) | 1 |
| Age (years), median (IQR) | 64.6 (57.48–75.53) | 65.0 (58.3–73.6) | 0.85 |
| BMI, median (IQR) | 25.1 (21.2–28.6) | 25.1 (21.7–26.9) | 0.91 |
| Charlson score, median (IQR) | 5 (3–6) | 4 (3–6) | 0.99 |
| SOFA Score, median (IQR) | 7 (4–9) | 7 (4–9) | 0.89 |
| SRD Type, n (%) | |||
| CTD | 48 (68.6) | 39 (55.7) | 0.04 |
| Vasculitis | 10 (14,3) | 20 (28.6) | |
| Sarcoidosis | 5 (7.1) | 9 (12.8) | |
| AS | 7 (10.0) | 2 (2.9) | |
| Treatment before admission | |||
| Corticosteroids, n (%) | 46 (65.7) | 38 (54.3) | 0.23 |
| Immunosuppressive therapy, n (%) | 25 (35.7) | 19 (27.1) | 0.36 |
| Prognosis | |||
| Death in ICU, n (%) | 11 (15.7) | 28 (40.0) | <0.01 |
| Death in hospital, n (%) | 13 (18.6) | 34 (48.6) | <0.01 |
| Death at one year, n (%) | 28 (40.0) | 46 (65.7) | <0.01 |
| Variables | Adjusted OR | CI 95% | p-Value |
|---|---|---|---|
| SOFA Score | 1.75 | (1.16–2.52) | <0.01 |
| Worst PaO2/FiO2 | |||
| >200 | - | - | - |
| 101–200 | 1.73 | (0.33–9.05) | 0.51 |
| ≤100 | 19.60 | (2.41–159.20) | <0.01 |
| Diagnosis in ICU | |||
| Acute exacerbation (reference) | - | - | - |
| Infection | 0.02 | (0.0001–0.59) | <0.01 |
| Other | 0.01 | (0.0001–0.19) | <0.01 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Banuls, L.; Vanoverschelde, J.; Garnier, F.; Amalric, M.; Jaber, S.; Charbit, J.; Chalard, K.; Mourad, M.; Benchabane, N.; Benomar, R.; et al. Interstitial Lung Disease Worsens Short- and Long-Term Outcomes of Systemic Rheumatic Disease Patients Admitted to the ICU: A Multicenter Study. J. Clin. Med. 2021, 10, 1037. https://doi.org/10.3390/jcm10051037
Banuls L, Vanoverschelde J, Garnier F, Amalric M, Jaber S, Charbit J, Chalard K, Mourad M, Benchabane N, Benomar R, et al. Interstitial Lung Disease Worsens Short- and Long-Term Outcomes of Systemic Rheumatic Disease Patients Admitted to the ICU: A Multicenter Study. Journal of Clinical Medicine. 2021; 10(5):1037. https://doi.org/10.3390/jcm10051037
Chicago/Turabian StyleBanuls, Lorrain, Juliette Vanoverschelde, Fanny Garnier, Matthieu Amalric, Samir Jaber, Jonathan Charbit, Kevin Chalard, Marc Mourad, Nacim Benchabane, Racim Benomar, and et al. 2021. "Interstitial Lung Disease Worsens Short- and Long-Term Outcomes of Systemic Rheumatic Disease Patients Admitted to the ICU: A Multicenter Study" Journal of Clinical Medicine 10, no. 5: 1037. https://doi.org/10.3390/jcm10051037