
Washout and Awakening Times after Inhaled Sedation of Critically Ill Patients: Desflurane Versus Isoflurane

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Experimental Section
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sackey, P.V.; Martling, C.-R.; Granath, F.; Radell, P.J. Prolonged isoflurane sedation of intensive care unit patients with the Anesthetic Conserving Device. Crit. Care Med. 2004, 32, 2241–2246. [Google Scholar] [CrossRef] [PubMed]
- Jerath, A.; Parotto, M.; Wasowicz, M.; Ferguson, N.D. Volatile Anesthetics. Is a New Player Emerging in Critical Care Sedation? Am. J. Respir. Crit. Care Med. 2016, 193, 1202–1212. [Google Scholar] [CrossRef]
- Baron, R.; Binder, A.; Biniek, R.; Braune, S.; Buerkle, H.; Dall, P.; Demirakca, S.; Eckardt, R.; Eggers, V.; Eichler, I.; et al. Evidence and consensus based guideline for the management of delirium, analgesia, and sedation in intensive care medicine. Revision 2015 (DAS-guideline 2015)—Short version. GMS Ger. Med. Sci. 2015, 13, 2–42. [Google Scholar] [CrossRef]
- Celis-Rodríguez, E.; Birchenall, C.; de la Cal, M.Á.; Castorena Arellano, G.; Hernández, A.; Ceraso, D.; Díaz Cortés, J.C.; Dueñas Castell, C.; Jimenez, E.J.; Meza, J.C.; et al. Clinical practice guidelines for evidence-based management of sedoanalgesia in critically ill adult patients. Med. Intensiva 2013, 37, 519–574. [Google Scholar] [CrossRef] [PubMed]
- Intensive Care Society Review of Best Practice for Analgesia and Sedation in the Critical Care. Available online: https://www.theawsomecourse.co.uk/ICS/ICS%20Sedation%20(2014).pdf (accessed on 15 December 2020).
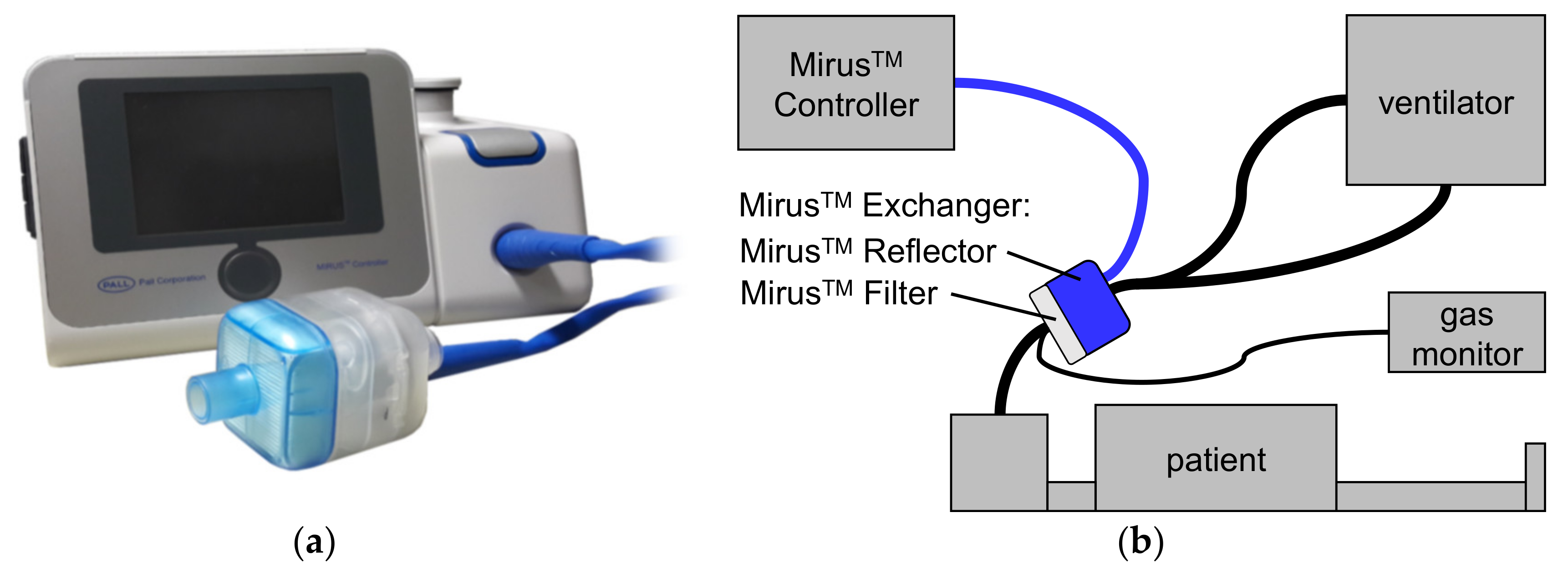
- Bomberg, H.; Glas, M.; Groesdonk, H.V.; Bellgardt, M.; Schwarz, J.; Volk, T.; Meiser, A. A novel device for target controlled administration and reflection of desflurane—The MirusTM. Anaesthesia 2014, 69, 1241–1250. [Google Scholar] [CrossRef] [Green Version]
- Smiley, R.M.; Ornstein, E.; Matteo, R.S.; Pantuck, E.J.; Pantuck, C.B. Desflurane and isoflurane in surgical patients: Comparison of emergence time. Anesthesiology 1991, 74, 425–428. [Google Scholar] [CrossRef]
- Agoliati, A.; Dexter, F.; Lok, J.; Masursky, D.; Sarwar, M.F.; Stuart, S.B.; Bayman, E.O.; Epstein, R.H. Meta-analysis of average and variability of time to extubation comparing isoflurane with desflurane or isoflurane with sevoflurane. Anesth. Analg. 2010, 110, 1433–1439. [Google Scholar] [CrossRef]
- Juvin, P.; Vadam, C.; Malek, L.; Dupont, H.; Marmuse, J.P.; Desmonts, J.M. Postoperative recovery after desflurane, propofol, or isoflurane anesthesia among morbidly obese patients: A prospective, randomized study. Anesth. Analg. 2000, 91, 714–719. [Google Scholar] [CrossRef] [Green Version]
- Juvin, P.; Servin, F.; Giraud, O.; Desmonts, J.M. Emergence of elderly patients from prolonged desflurane, isoflurane, or propofol anesthesia. Anesth. Analg. 1997, 85, 647–651. [Google Scholar] [CrossRef] [PubMed]
- Bennett, J.A.; Lingaraju, N.; Horrow, J.C.; McElrath, T.; Keykhah, M.M. Elderly patients recover more rapidly from desflurane than from isoflurane anesthesia. J. Clin. Anesth. 1992, 4, 378–381. [Google Scholar] [CrossRef]
- Beaussier, M.; Deriaz, H.; Abdelahim, Z.; Aissa, F.; Lienhart, A. Comparative effects of desflurane and isoflurane on recovery after long lasting anaesthesia. Can. J. Anaesth. 1998, 45, 429–434. [Google Scholar] [CrossRef] [Green Version]
- Meiser, A.; Sirtl, C.; Bellgardt, M.; Lohmann, S.; Garthoff, A.; Kaiser, J.; Hügler, P.; Laubenthal, H.J. Desflurane compared with propofol for postoperative sedation in the intensive care unit. Br. J. Anaesth. 2003, 90, 273–280. [Google Scholar] [CrossRef] [Green Version]
- Eger, E.I., 2nd; Saidman, L.J.; Brandstater, B. Minimum alveolar anesthetic concentration: A standard of anesthetic potency. Anesthesiology 1965, 26, 756–763. [Google Scholar] [CrossRef]
- Mapleson, W.W. Effect of age on MAC in humans: A meta-analysis. Br. J. Anaesth. 1996, 76, 179–185. [Google Scholar] [CrossRef] [PubMed]
- Sessler, C.N.; Gosnell, M.S.; Grap, M.J.; Brophy, G.M.; O’Neal, P.V.; Keane, K.A.; Tesoro, E.P.; Elswick, R.K. The Richmond Agitation-Sedation Scale: Validity and reliability in adult intensive care unit patients. Am. J. Respir. Crit. Care Med. 2002, 166, 1338–1344. [Google Scholar] [CrossRef]
- Behne, M.; Wilke, H.J.; Lischke, V. Recovery and pharmacokinetic parameters of desflurane, sevoflurane, and isoflurane in patients undergoing urologic procedures. J. Clin. Anesth. 1999, 11, 460–465. [Google Scholar] [CrossRef]
- Tempia, A.; Olivei, M.C.; Calza, E.; Lambert, H.; Scotti, L.; Orlando, E.; Livigni, S.; Guglielmotti, E. The anesthetic conserving device compared with conventional circle system used under different flow conditions for inhaled anesthesia. Anesth. Analg. 2003, 96, 1056–1061, table of contents. [Google Scholar] [CrossRef]
- Le Gall, J.R.; Lemeshow, S.; Saulnier, F. A new Simplified Acute Physiology Score (SAPS II) based on a European/North American multicenter study. JAMA 1993, 270, 2957–2963. [Google Scholar] [CrossRef]
- Vincent, J.L.; Moreno, R.; Takala, J.; Willatts, S.; De Mendonça, A.; Bruining, H.; Reinhart, C.K.; Suter, P.M.; Thijs, L.G. The SOFA (Sepsis-related Organ Failure Assessment) score to describe organ dysfunction/failure. On behalf of the Working Group on Sepsis-Related Problems of the European Society of Intensive Care Medicine. Intensive Care Med. 1996, 22, 707–710. [Google Scholar] [CrossRef] [PubMed]
- Romagnoli, S.; Chelazzi, C.; Villa, G.; Zagli, G.; Benvenuti, F.; Mancinelli, P.; Arcangeli, G.; Dugheri, S.; Bonari, A.; Tofani, L.; et al. The New MIRUS System for Short-Term Sedation in Postsurgical ICU Patients. Crit. Care Med. 2017, 45, e925–e931. [Google Scholar] [CrossRef] [PubMed]
- Bellgardt, M.; Georgevici, A.I.; Klutzny, M.; Drees, D.; Meiser, A.; Gude, P.; Vogelsang, H.; Weber, T.P.; Herzog-Niescery, J. Use of MIRUSTM for MAC-driven application of isoflurane, sevoflurane, and desflurane in postoperative ICU patients: A randomized controlled trial. Ann. Intensive Care 2019, 9, 118. [Google Scholar] [CrossRef]
- Bomberg, H.; Groesdonk, H.V.; Bellgardt, M.; Volk, T.; Meiser, A. AnaConDaTM and MirusTM for intensive care sedation, 24 h desflurane versus isoflurane in one patient. Springerplus 2016, 5, 420. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eger, E.I. 2nd Age, minimum alveolar anesthetic concentration, and minimum alveolar anesthetic concentration-awake. Anesth. Analg. 2001, 93, 947–953. [Google Scholar] [CrossRef]
- Meiser, A.; Bomberg, H.; Lepper, P.M.; Trudzinski, F.C.; Volk, T.; Groesdonk, H. V Inhaled Sedation in Patients With Acute Respiratory Distress Syndrome Undergoing Extracorporeal Membrane Oxygenation. Anesth. Analg. 2017, 125, 1235–1239. [Google Scholar] [CrossRef]
- Meiser, A.; Groesdonk, H.V.; Bonnekessel, S.; Volk, T.; Bomberg, H. Inhalation Sedation in Subjects With ARDS Undergoing Continuous Lateral Rotational Therapy. Respir. Care 2018, 63, 441–447. [Google Scholar] [CrossRef] [Green Version]
- Jabaudon, M.; Boucher, P.; Imhoff, E.; Chabanne, R.; Faure, J.-S.; Roszyk, L.; Thibault, S.; Blondonnet, R.; Clairefond, G.; Guérin, R.; et al. Sevoflurane for Sedation in Acute Respiratory Distress Syndrome. A Randomized Controlled Pilot Study. Am. J. Respir. Crit. Care Med. 2017, 195, 792–800. [Google Scholar] [CrossRef] [PubMed]
- Bellgardt, M.; Bomberg, H.; Herzog-Niescery, J.; Dasch, B.; Vogelsang, H.; Weber, T.P.; Steinfort, C.; Uhl, W.; Wagenpfeil, S.; Volk, T.; et al. Survival after long-term isoflurane sedation as opposed to intravenous sedation in critically ill surgical patients: Retrospective analysis. Eur. J. Anaesthesiol. 2016, 33, 6–13. [Google Scholar] [CrossRef]
- Belda, J.F.; Soro, M.; Badenes, R.; Meiser, A.; García, M.L.; Aguilar, G.; Martí, F.J. The predictive performance of a pharmacokinetic model for manually adjusted infusion of liquid sevofluorane for use with the Anesthetic-Conserving Device (AnaConDa): A clinical study. Anesth. Analg. 2008, 106, 1207–1214, table of contents. [Google Scholar] [CrossRef]
- Vollmer, M.K.; Rhee, T.S.; Rigby, M.; Hofstetter, D.; Hill, M.; Schoenenberger, F.; Reimann, S. Modern inhalation anesthetics: Potent greenhouse gases in the global atmosphere. Geophys. Res. Lett. 2015, 42, 1606–1611. [Google Scholar] [CrossRef] [Green Version]
- German Clinical Trials Registry Entry. Available online: https://www.drks.de/drks_web/navigate.do?navigationId=trial.HTML&TRIAL_ID=DRKS00011403 (accessed on 12 January 2021).




{kind=link}
{kind=link}
{kind=link}
| Desflurane | Isoflurane | p Value | |
|---|---|---|---|
| (n = 10) | (n = 10) | ||
| Male | 8 | 6 | 0.331 |
| Age (years) | 58 ± 16 | 66 ± 16 | 0.302 |
| Height (cm) | 170 ± 7 | 174 ± 6 | 0.212 |
| Body mass index (kg/m2) | 26.3 (23.5–33.4) | 27.4 (25.1–30) | 0.583 |
| Reason for admission: | 0.621 | ||
| Abdominal surgery | 4 | 5 | |
| Trauma | 1 | 2 | |
| Submandibular abscess | 1 | 0 | |
| Necrotizing fasciitis | 1 | 1 | |
| Erysipelas | 1 | 1 | |
| Pneumonia | 2 | 0 | |
| Pancreatitis | 0 | 1 | |
| SAPS II Score 4 on admission | 42.5 (35.0–45.0) | 48 (37.0–56.0) | 0.493 |
| Patients with sepsis | 5 | 7 | 0.361 |
| Reason for invasive ventilation | |||
| Airway | 2 | 0 | |
| Pulmonary | 8 | 10 | 0.141 |
| Oxygenation index (mmHg) | 197 ± 86 | 184 ± 46 | 0.692 |
| (at time of intubation) | |||
| SOFA Score 5 | 8.5 (6.5–9.0) | 8.0 (8.0–10.0) | 0.213 |
| (at time of intubation) | |||
| Duration of application of anesthetics (h) | 20 ± 1 | 21 ± 2 | 0.262 |
| MAC fraction 6 | 0.45 ± 0.14 | 0.37 ± 0.17 | 0.232 |
| RASS Scores 7 | −4 (−5; −4) | −4 (−4.9; −4) | 0.973 |
| Remifentanil dose (µg/kg/min) | 0.087 ± 0.072 | 0.082 ± 0.032 | 0.852 |
| (before study sedation) | |||
| Remifentanil dose (µg/kg/min) | 0.056 ± 0.033 | 0.037 ± 0.013 | 0.102 |
| (during study sedation) | |||
| Patients breathing spontaneously | 6 | 4 | 0.371 |
| (at start of study) | |||
| Time to start breathing spontaneously | 0.8 ± 0.9 | 0.9 ± 0.5 | 0.922 |
| in remaining patients (h) | |||
| Tidal volume (mL) | 580 ± 90 | 610 ± 130 | 0.582 |
| Respiratory rate (min−1) | 18 ± 6 | 19 ± 6 | 0.832 |
| Desflurane | Isoflurane | Number of Patients (Desflurane:Isoflurane) | p Value | |
|---|---|---|---|---|
| T30% | 0.1 (0.1–0.2) | 0.2 (0.2–0.5) | 10:10 | 0.034 |
| T40% | 0.2 (0.2–0.2) | 0.5 (0.4–1.1) | 10:10 | <0.001 |
| T50% | 0.3 (0.3–0.4) | 1.3 (0.4–2.3) | 10:10 | 0.002 |
| T60% | 0.7 (0.4–0.9) | 1.5 (0.8–2.9) | 10:8 | 0.006 |
| T70% | 1.1 (0.6–1.9) | 4.3 (2.0–8.2) | 9:8 | 0.005 |
| T80% | 2.5 (2.0–5.9) | 12.1 (5.1–20.2) | 7:6 | 0.022 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Daume, P.; Weis, J.; Bomberg, H.; Bellgardt, M.; Volk, T.; Groesdonk, H.V.; Meiser, A. Washout and Awakening Times after Inhaled Sedation of Critically Ill Patients: Desflurane Versus Isoflurane. J. Clin. Med. 2021, 10, 665. https://doi.org/10.3390/jcm10040665
Daume P, Weis J, Bomberg H, Bellgardt M, Volk T, Groesdonk HV, Meiser A. Washout and Awakening Times after Inhaled Sedation of Critically Ill Patients: Desflurane Versus Isoflurane. Journal of Clinical Medicine. 2021; 10(4):665. https://doi.org/10.3390/jcm10040665
Chicago/Turabian StyleDaume, Philipp, Johannes Weis, Hagen Bomberg, Martin Bellgardt, Thomas Volk, Heinrich V. Groesdonk, and Andreas Meiser. 2021. "Washout and Awakening Times after Inhaled Sedation of Critically Ill Patients: Desflurane Versus Isoflurane" Journal of Clinical Medicine 10, no. 4: 665. https://doi.org/10.3390/jcm10040665