
Hemodynamic and Radiological Classification of Ovarian Veins System Insufficiency


Abstract
:1. Introduction
2. Methods and Diagnostic Approach
3. Results
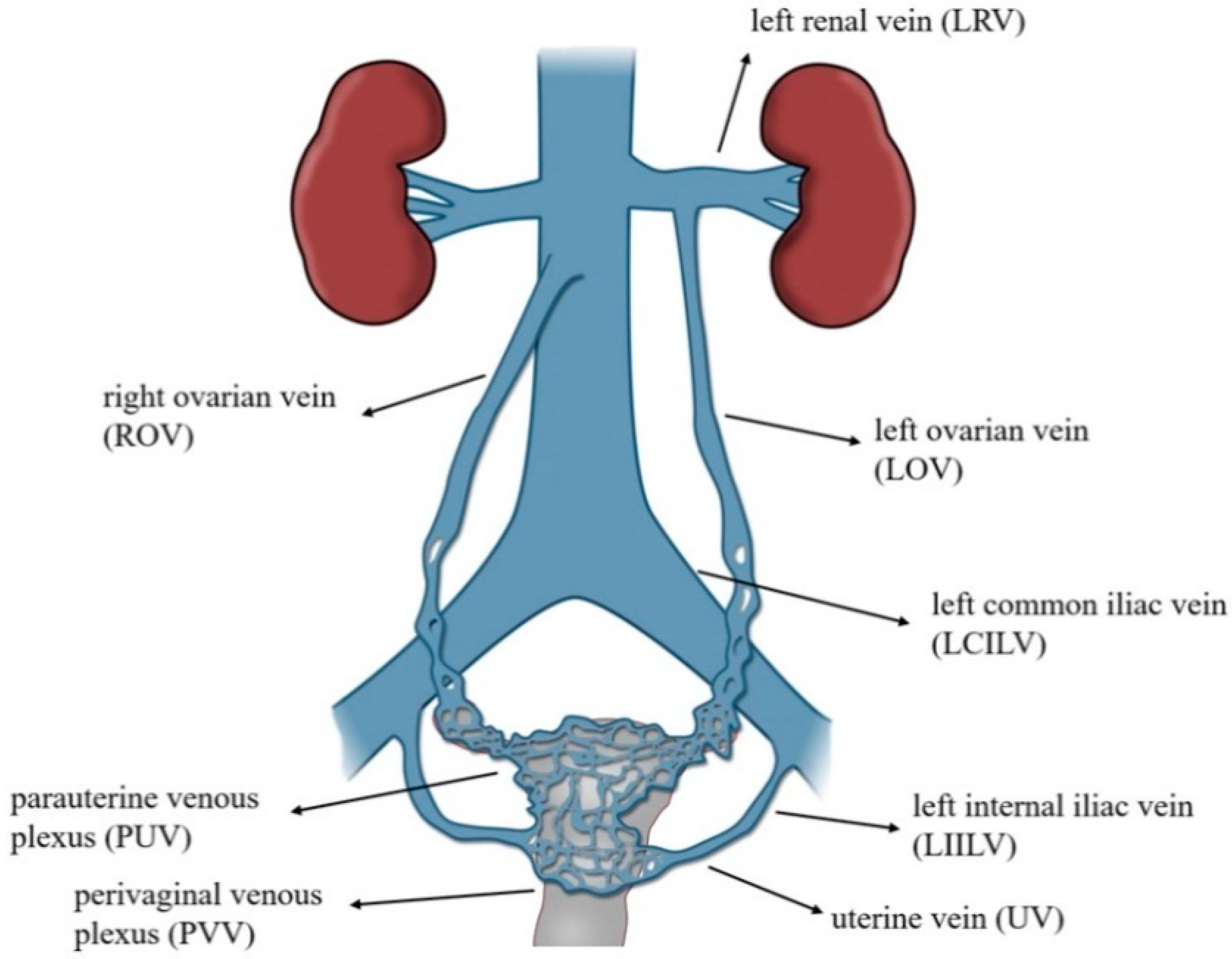
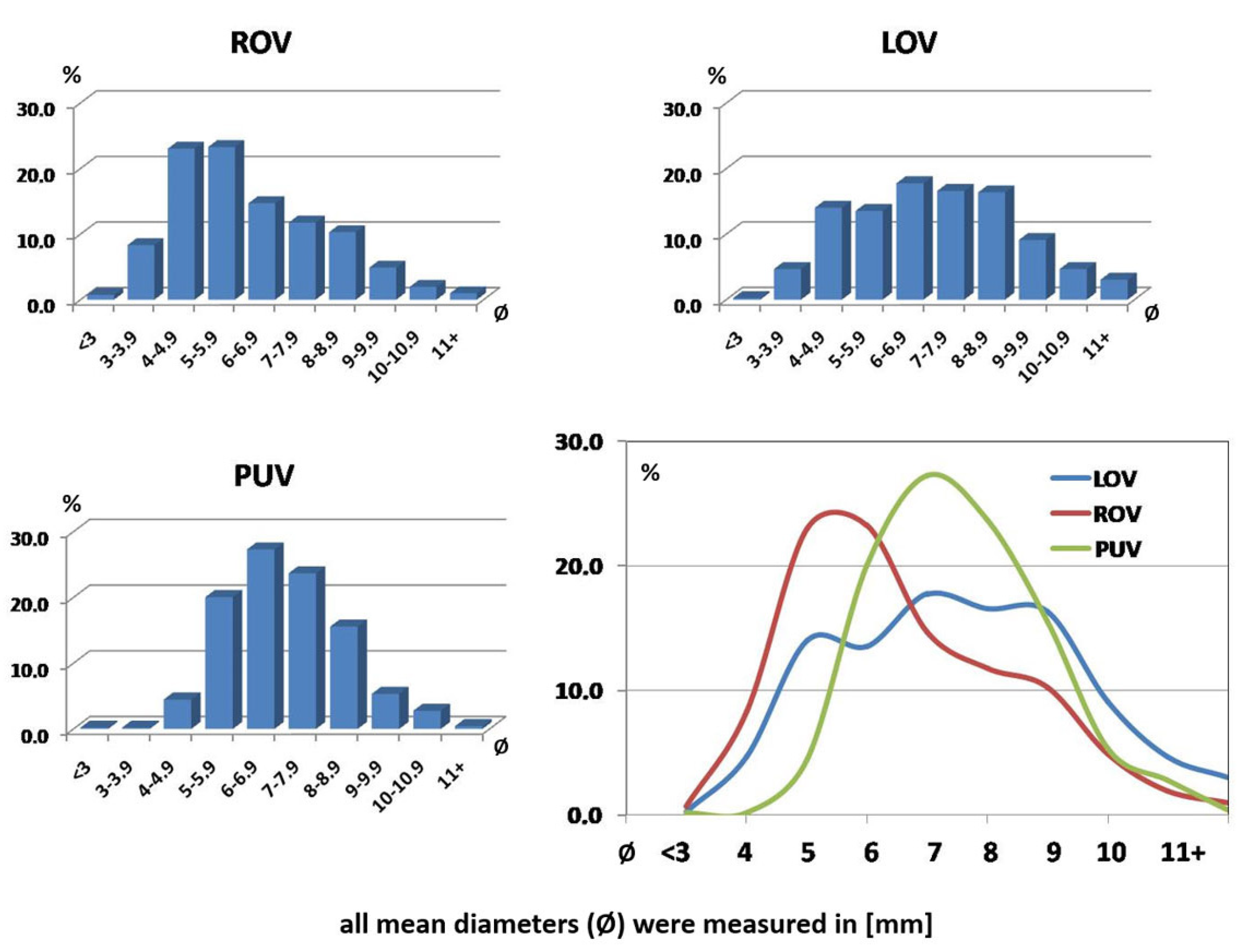
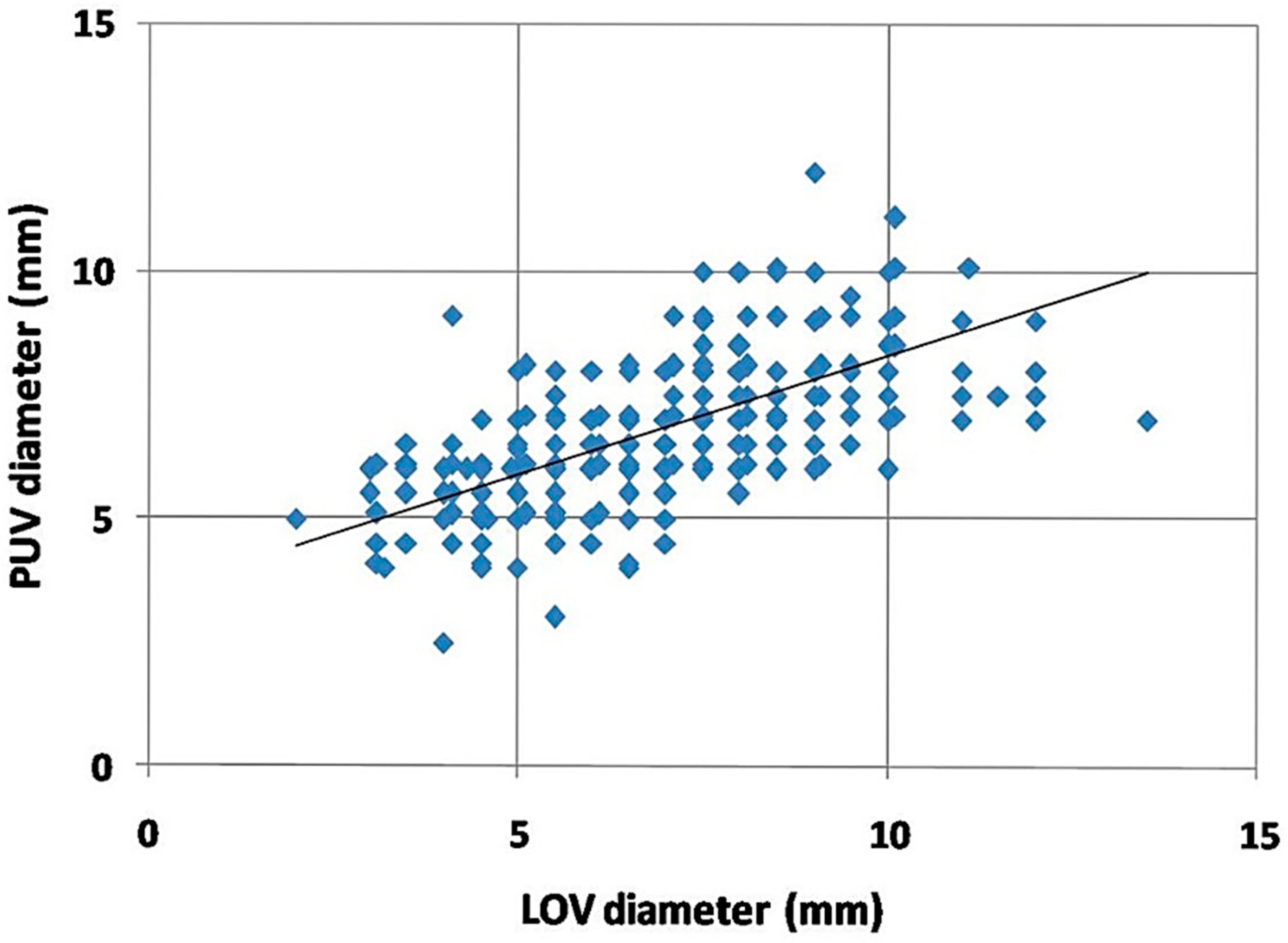
3.1. Ovarian Veins Morphology
3.2. Anatomical Variations
4. Proposal for a Hemodynamic and Radiological Classification of Ovarian Veins Insufficiency
4.1. Assumptions of the Ultrasound and Radiological Classification of Ovarian Veins System Insufficiency
- −
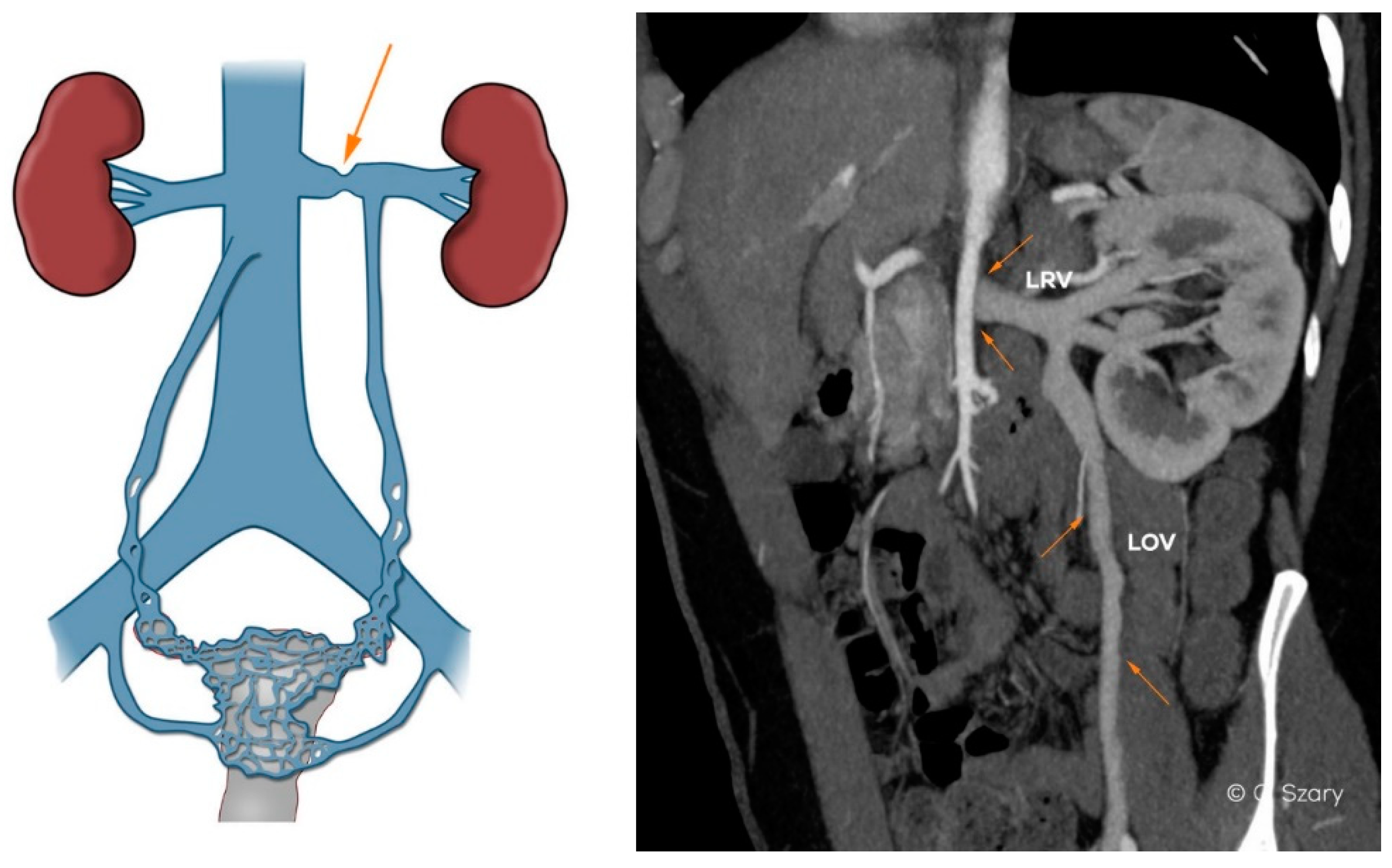
- narrow distal segment of the LRV (developmental variant);
- −
- extrinsic compression of the LRV by the superior mesenteric artery (SMA)–typical of the nutcracker phenomenon;
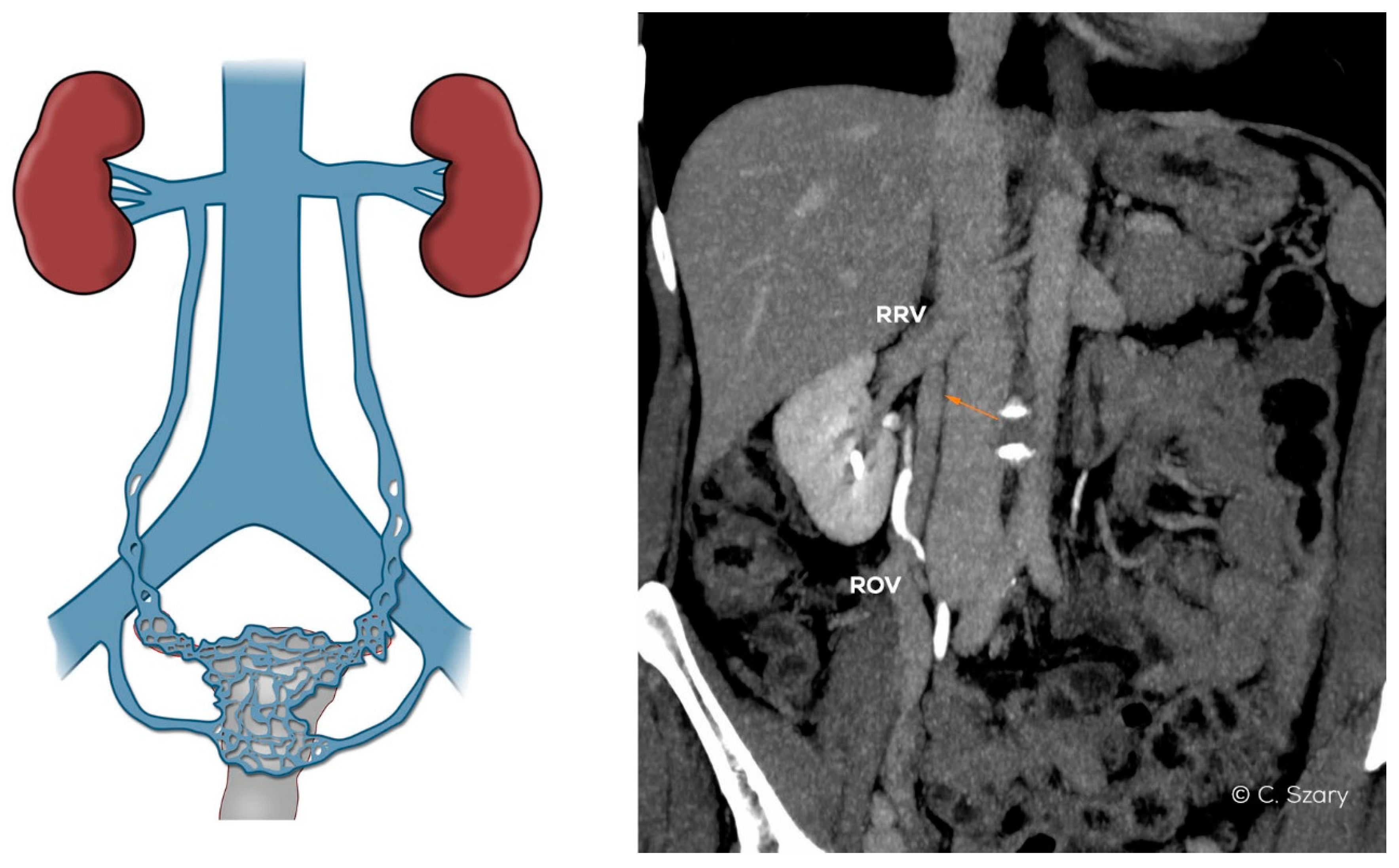
- −
- atypical drainage of the right ovarian vein into the trunk of the right renal vein (Figure 7).
- −
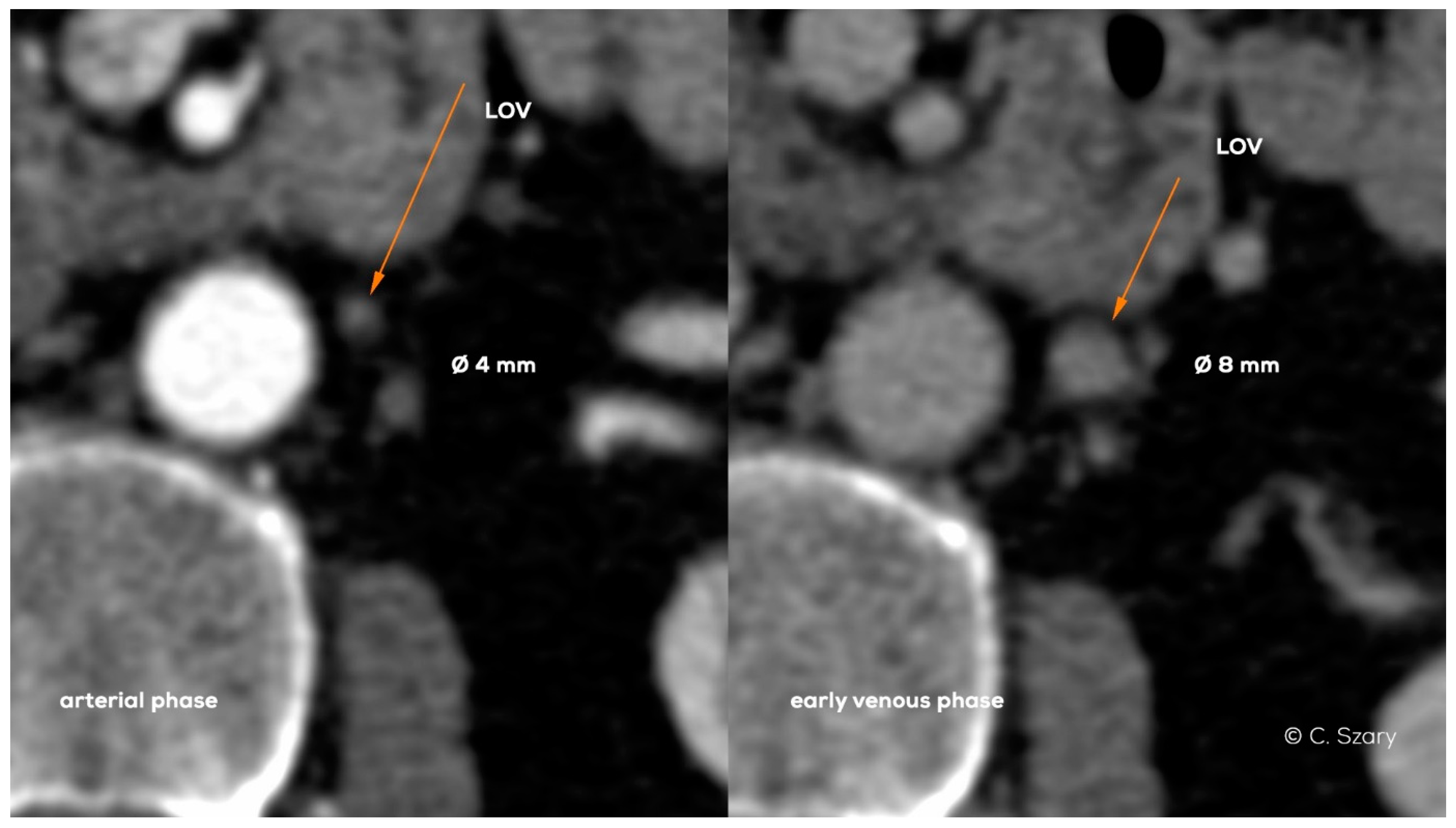
- the mean diameter of ovarian veins (the upper and lower segments are always assessed in the late phase of contrast enhancement);
- −
- the rate and order of the ovarian veins contrasting;
- −
- the dynamics of contrast enhancement in ovarian and iliac veins, assessed in dynamic radiological sequences;
- −
- the mean diameter of the internal iliac veins and their branches;
- −
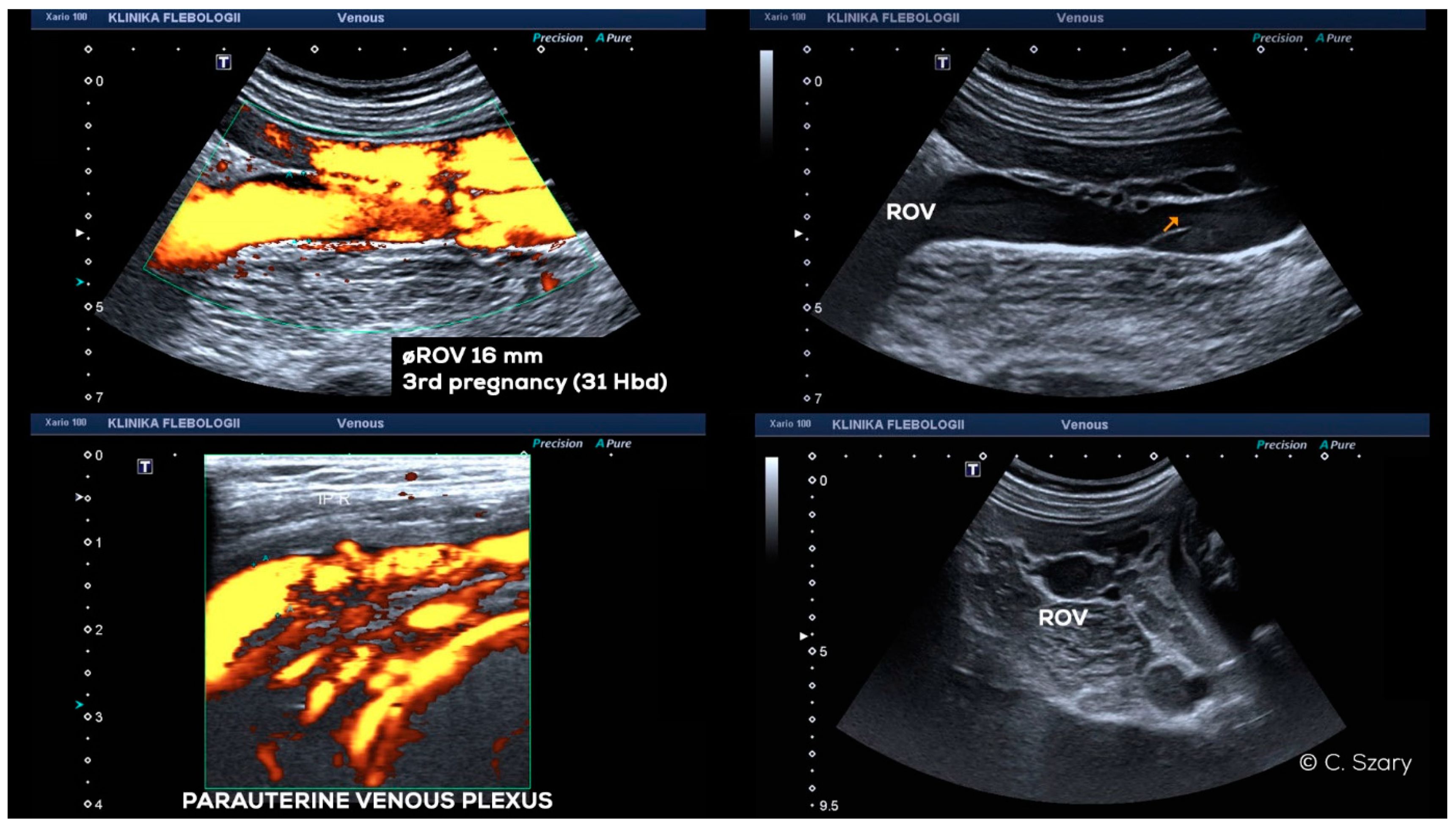
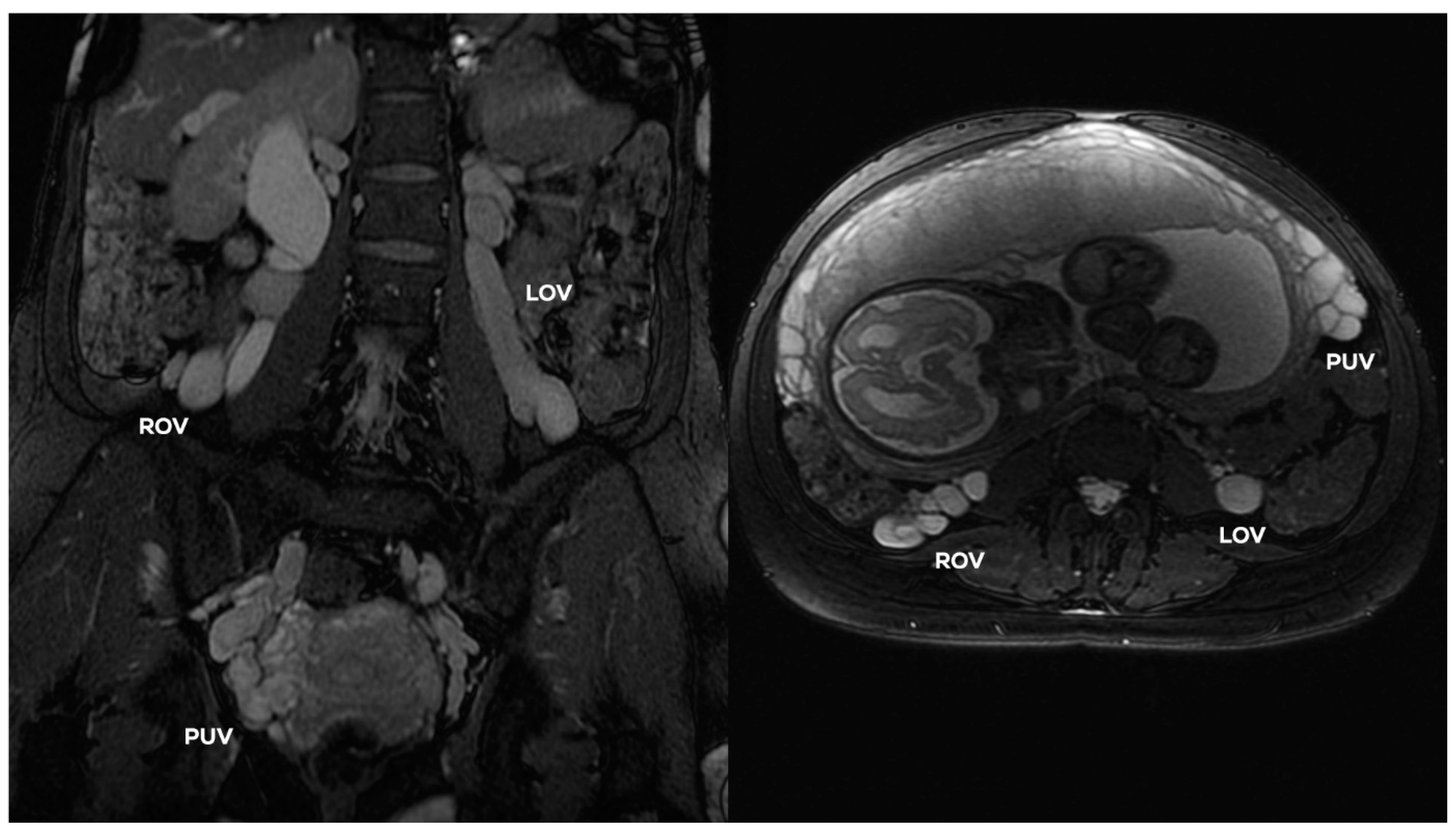
- maximum distension of the para-uterine venous plexuses on both sides;
- −
- the presence of collateral venous circulation generated as a result of venous outflow disorders (most often in the LRV axis drainage);
- −
- occurrence of venous anastomoses in the pelvis (the direction of flow can be assessed in the CDU, and often also in the dynamic contrast enhanced MRV examination).
4.2. Grading of Ovarian Veins Insufficiency
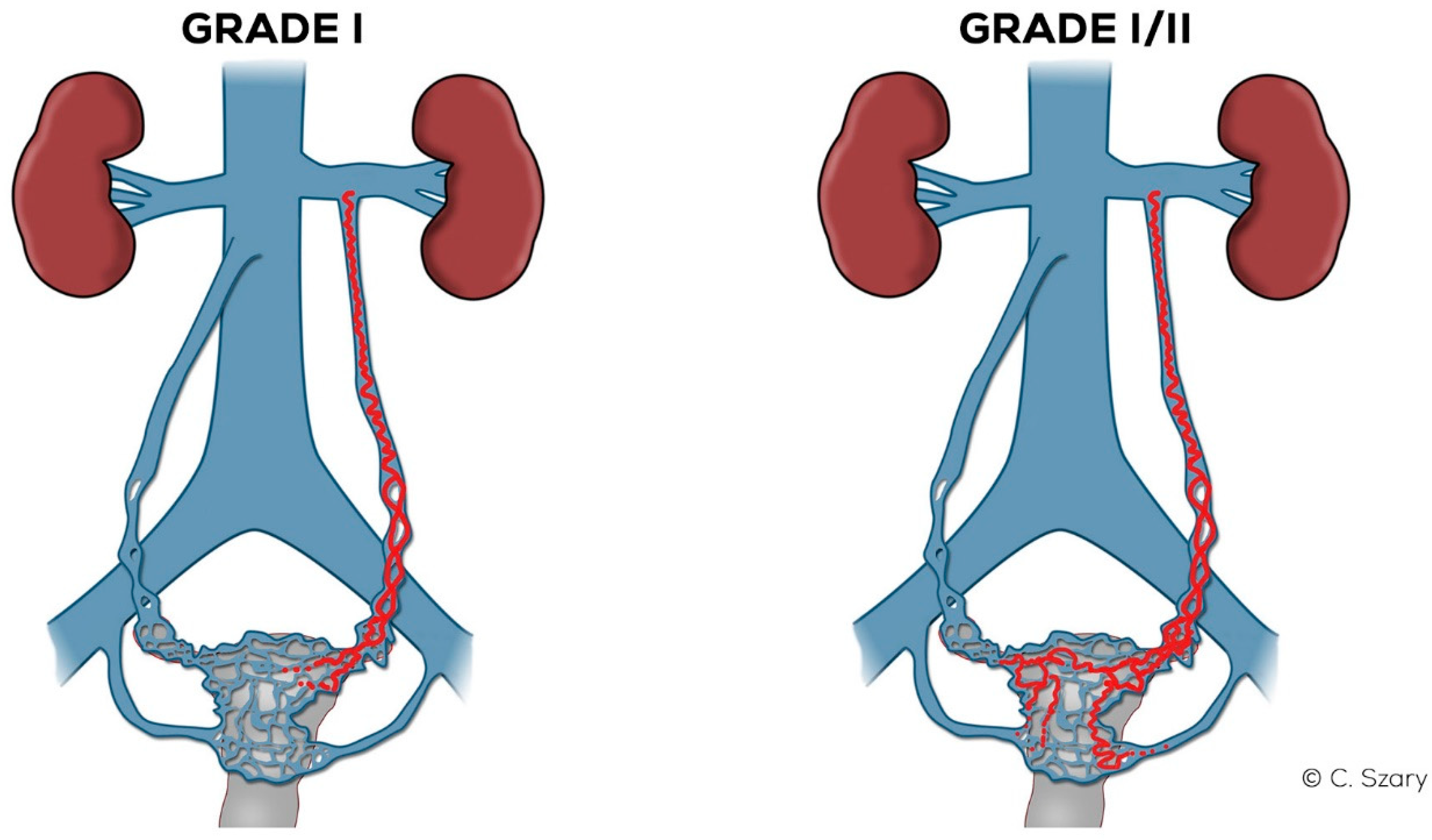
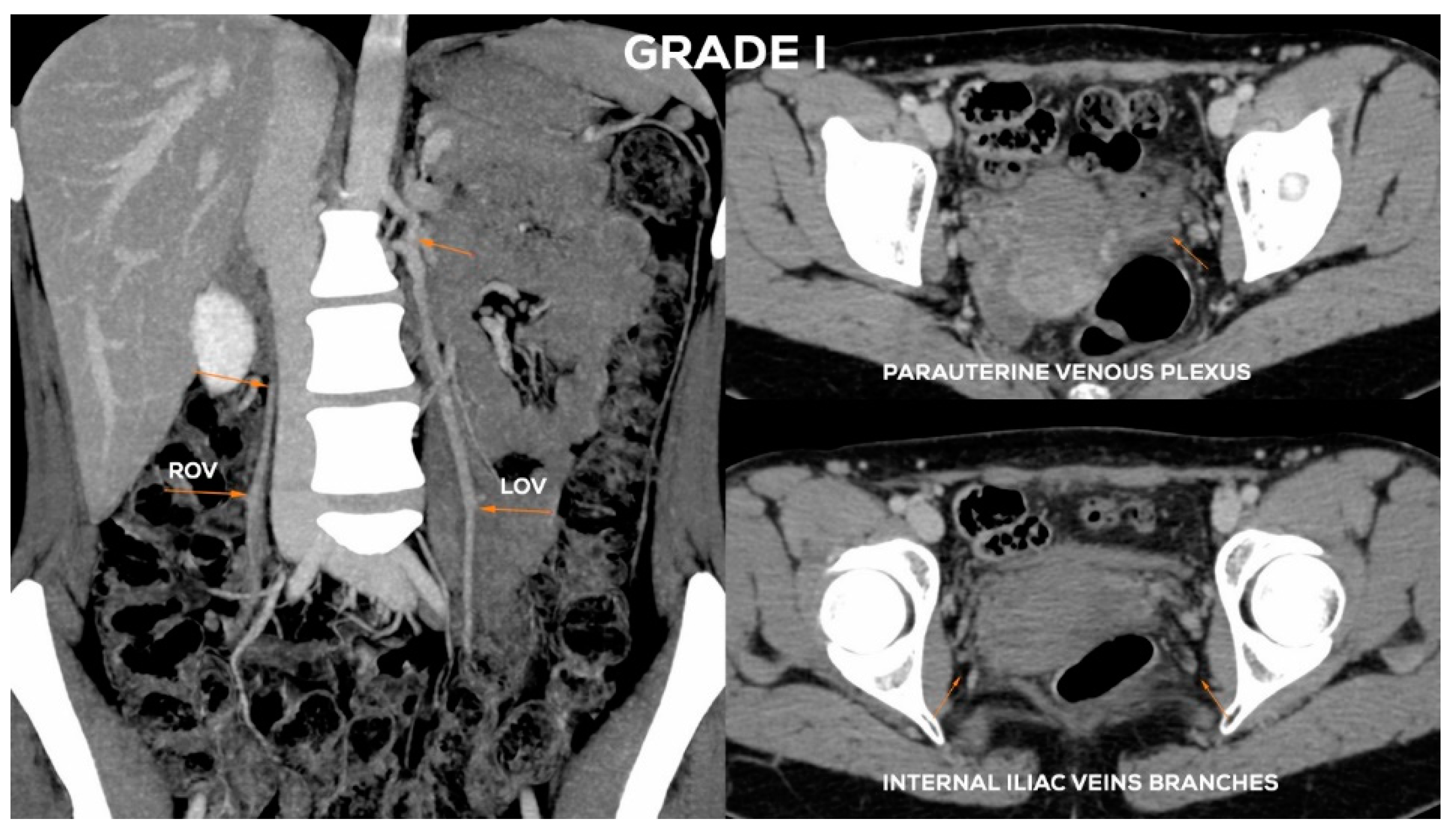
4.2.1. Grade I (GI)
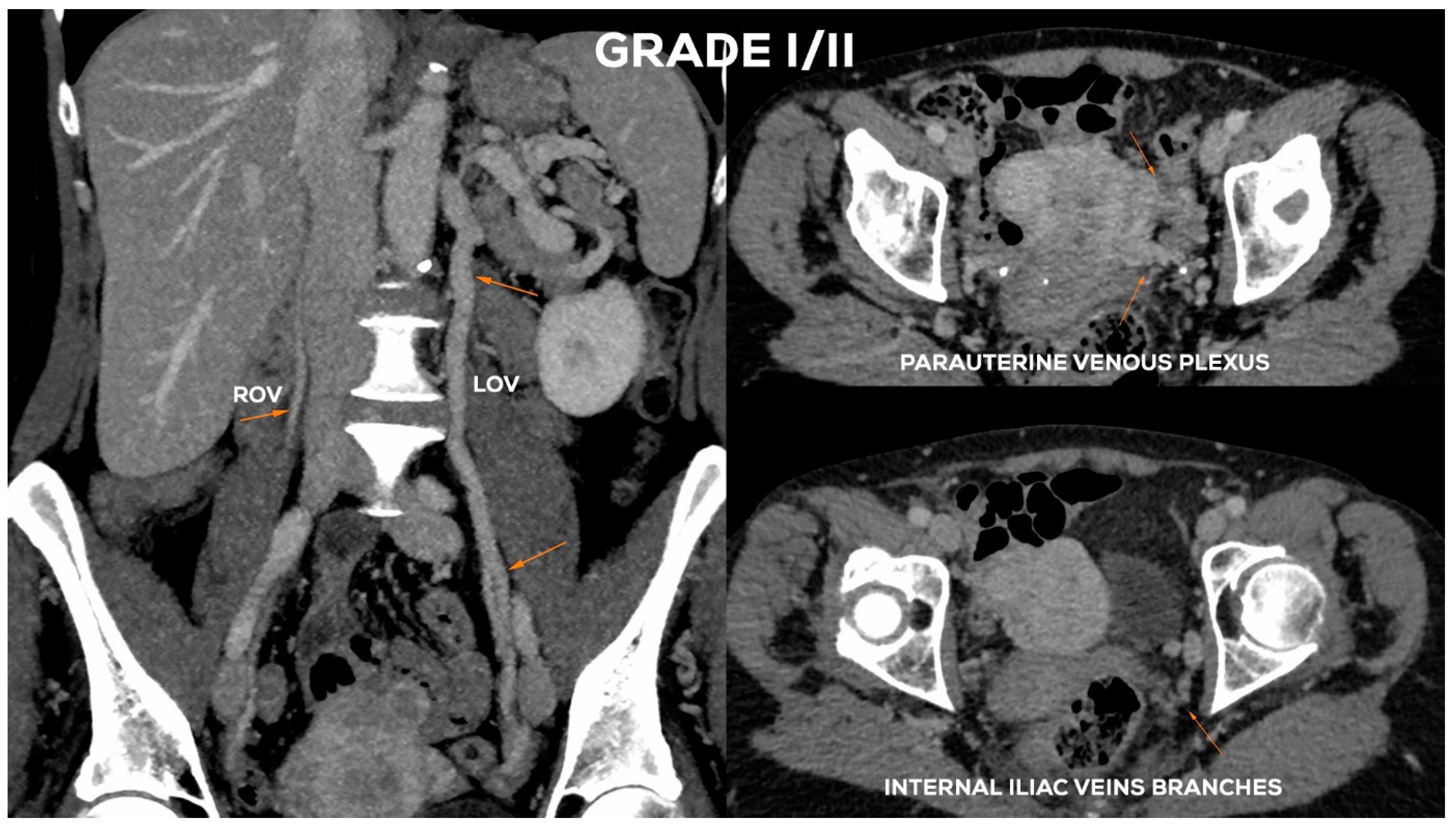
4.2.2. Grade I/II (GI/II)
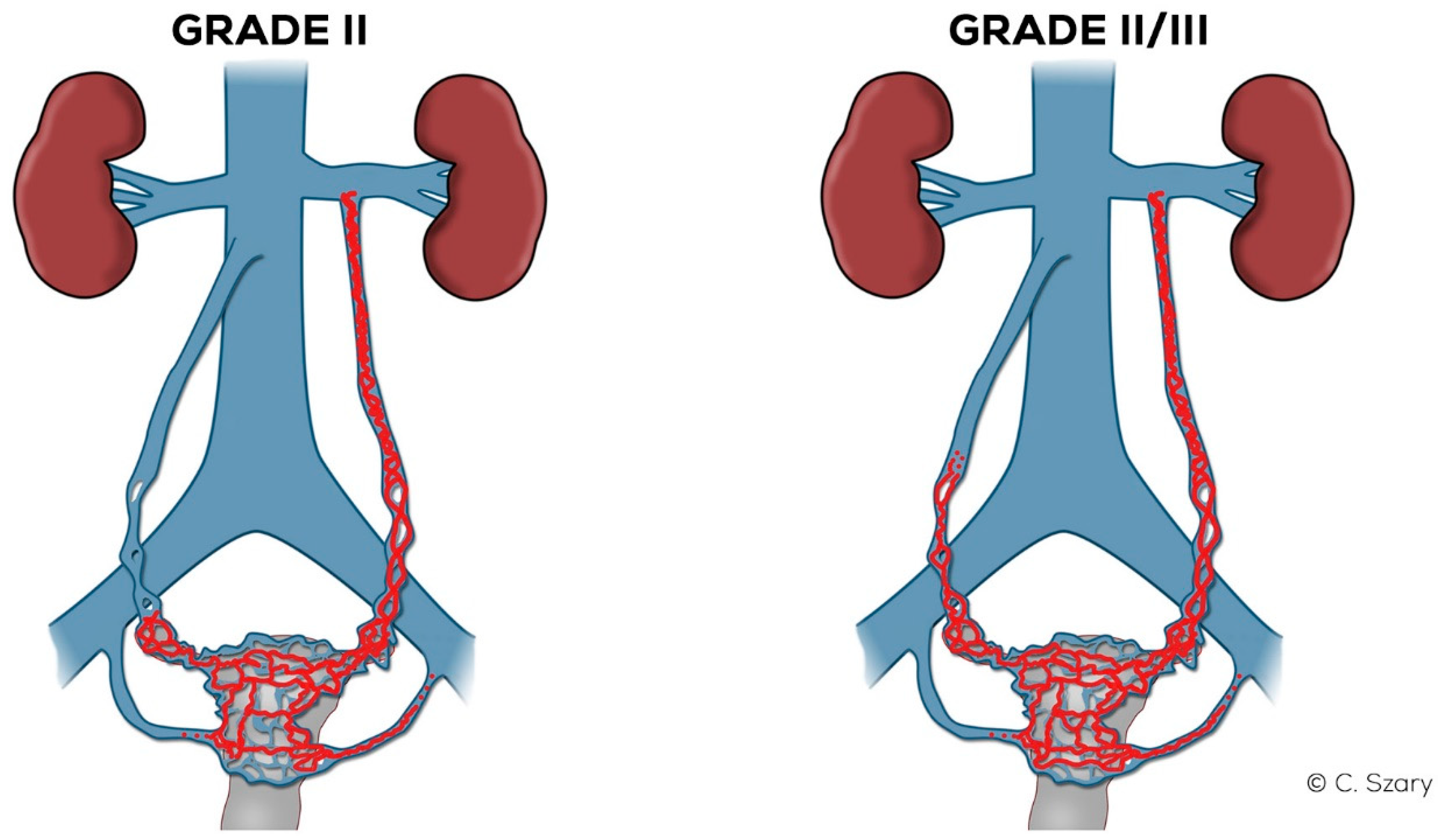
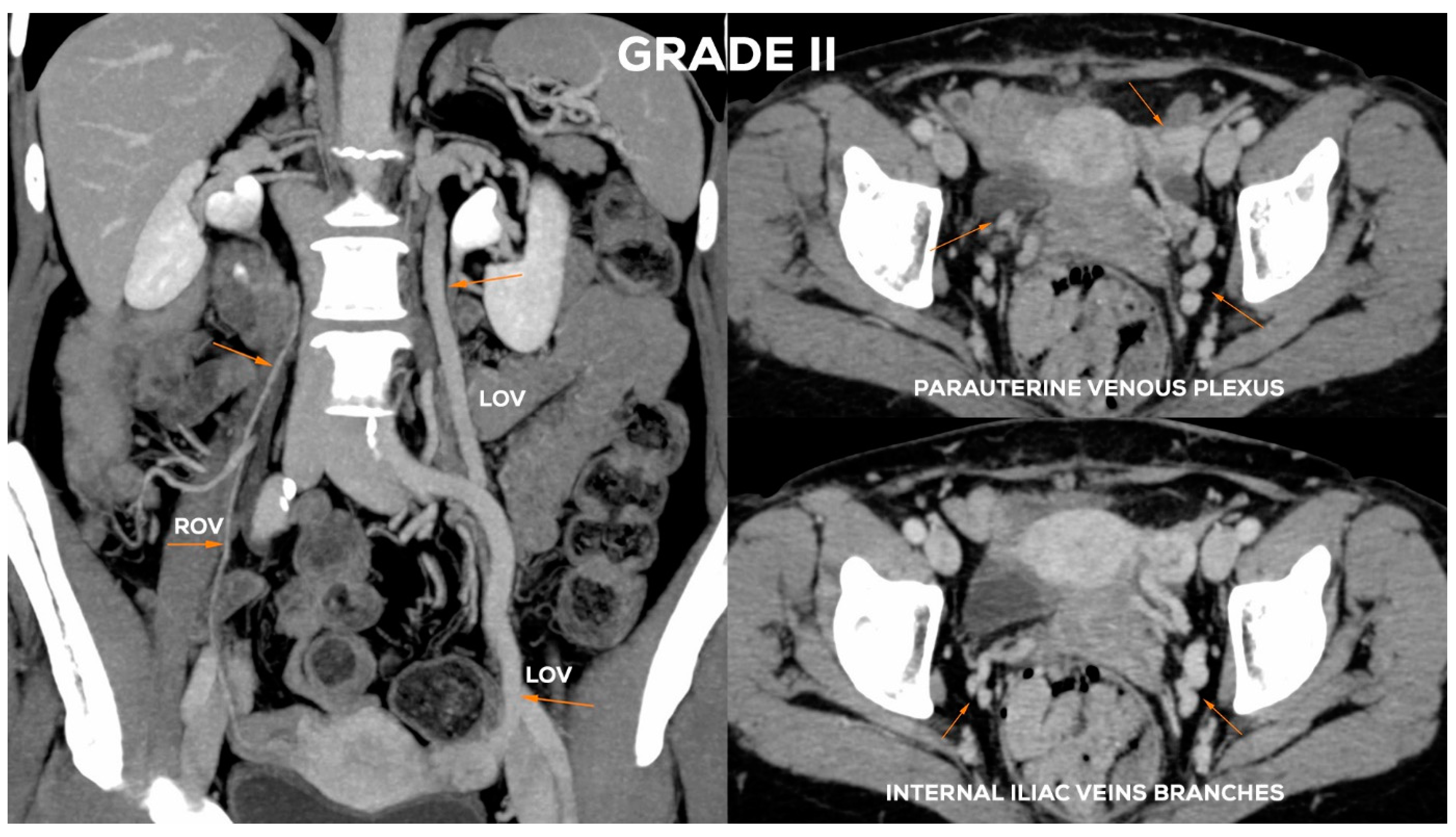
4.2.3. Grade II (GII)
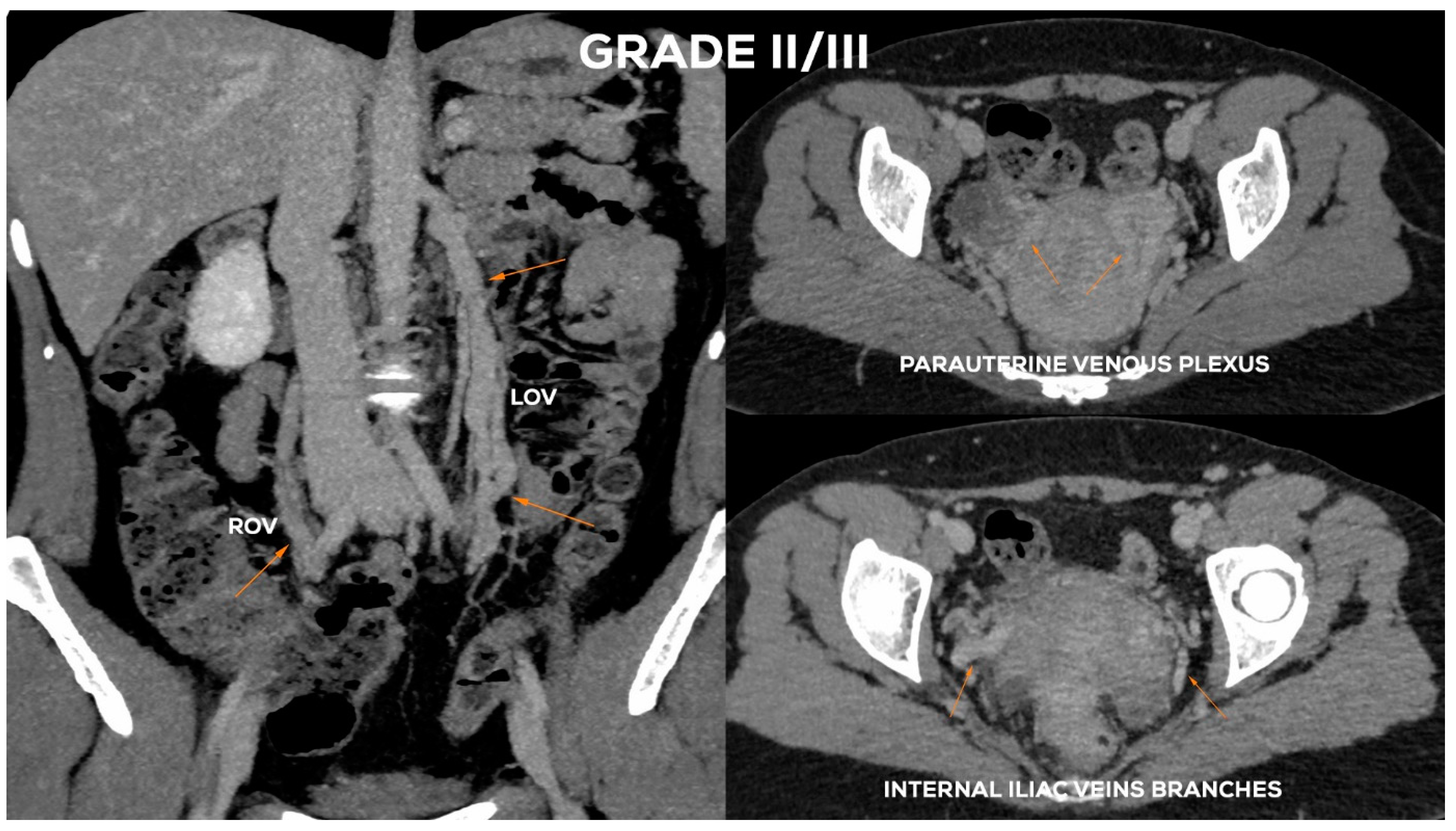
4.2.4. Grade II/III (GII/III)
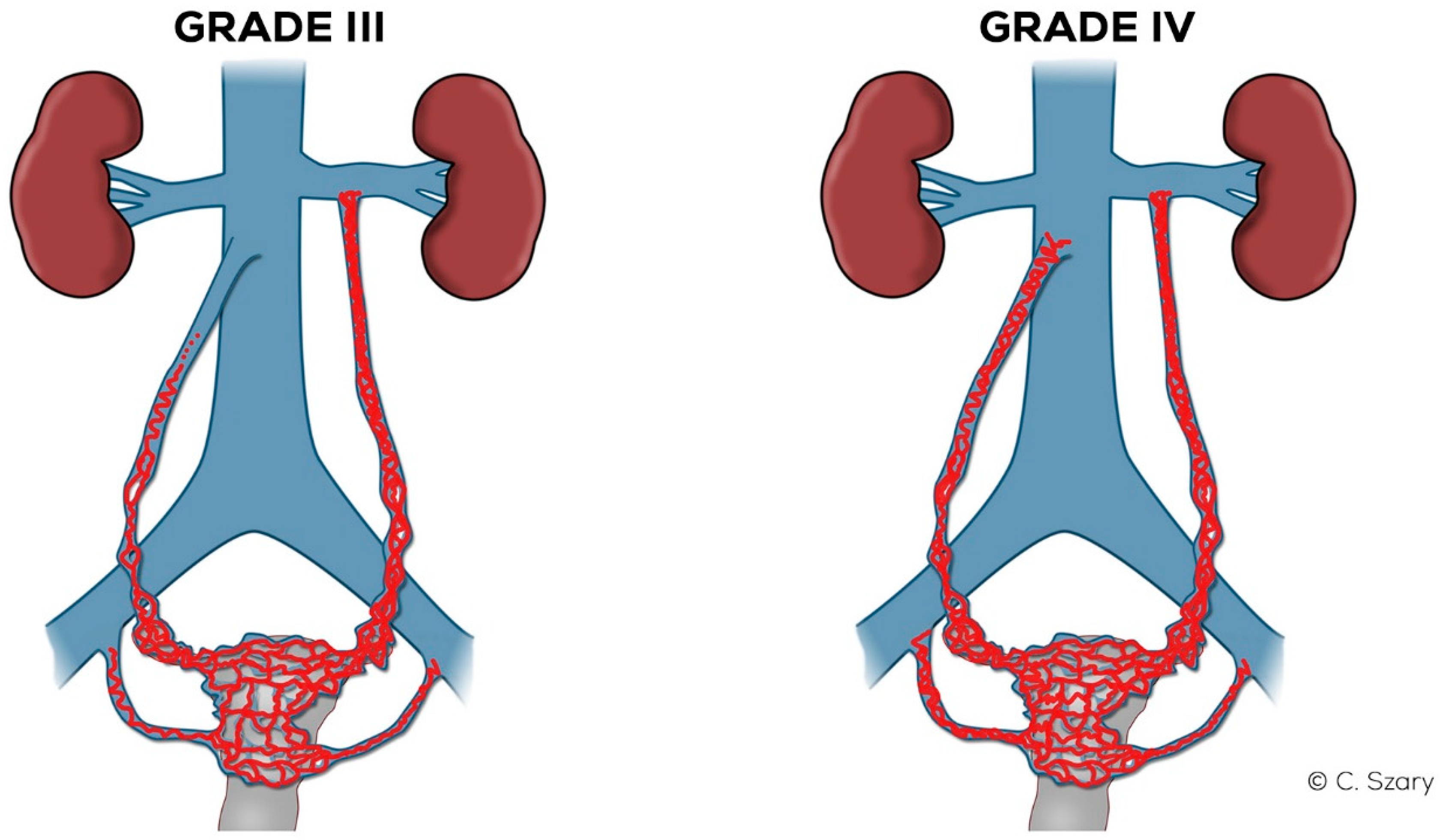
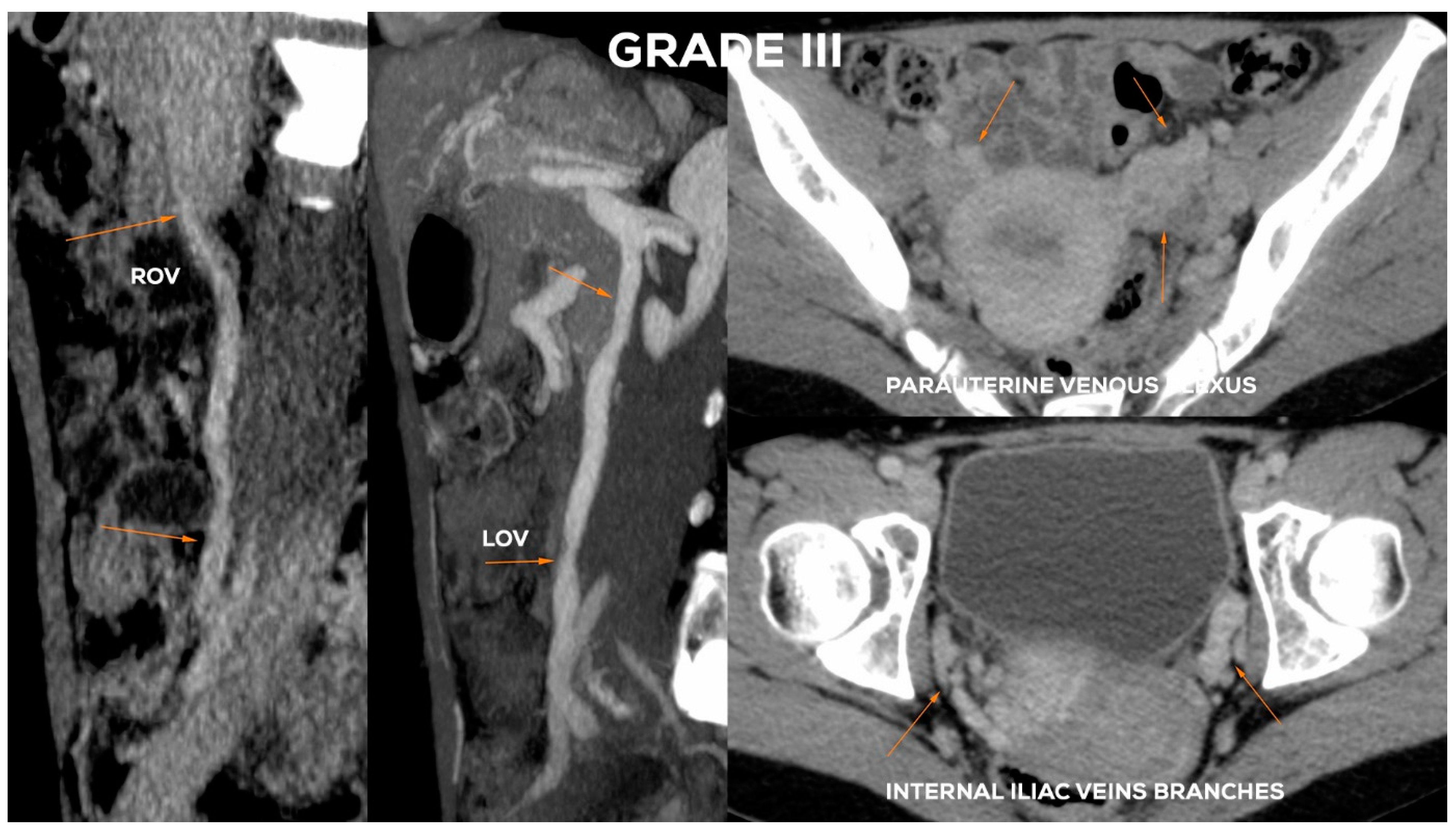
4.2.5. Grade III (GIII)
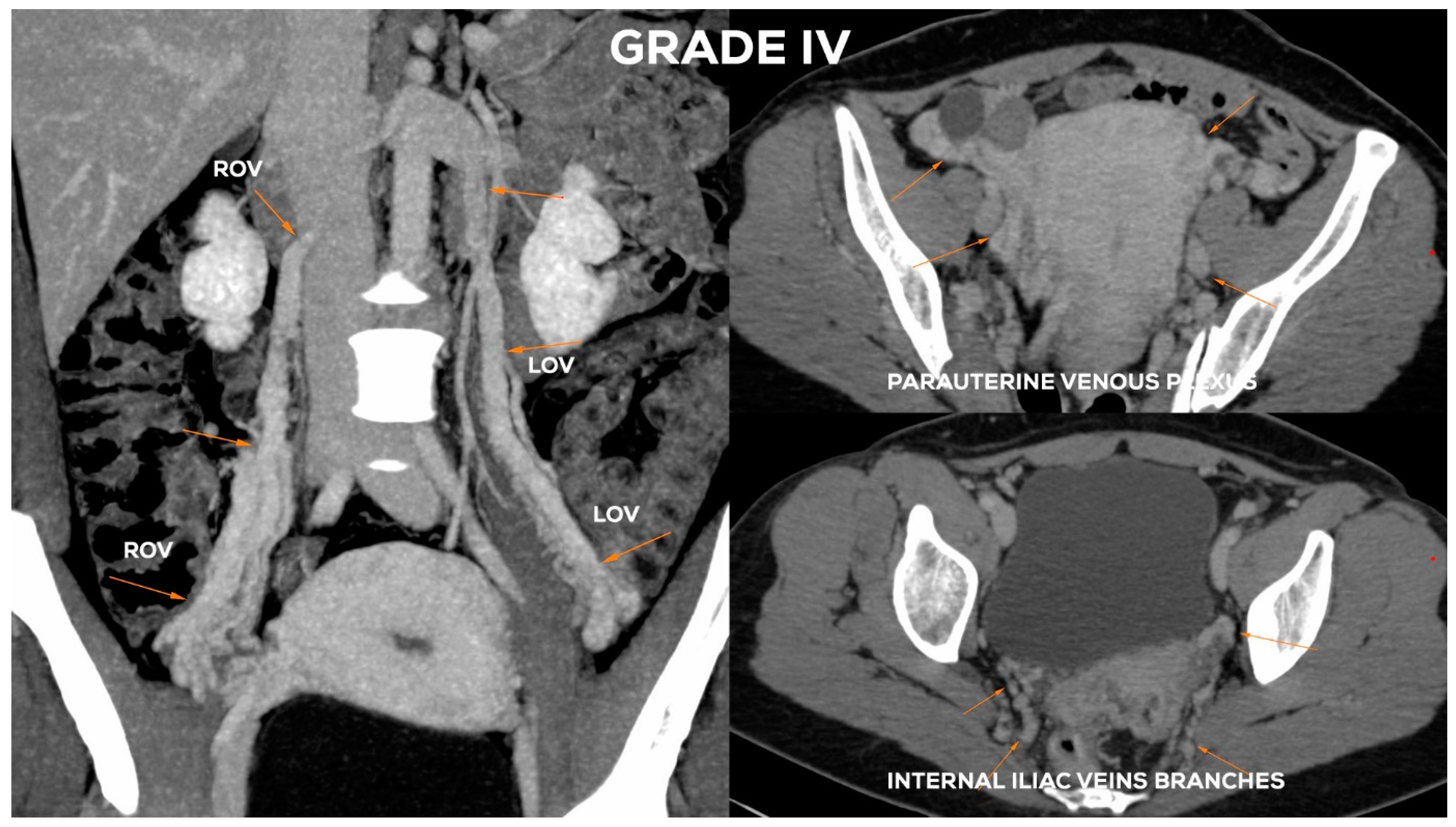
4.2.6. Grade IV (GIV)
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rizer, M.; Alexander, R.; Sharpe, E.E., 3rd; Rochon, P.J.; Brown, C.L. Pelvic Congestion Syndrome: Systematic Review of Treatment Success. Semin. Interv. Radiol. 2018, 35, 35–40. [Google Scholar] [CrossRef] [PubMed]
- Ahangari, A. Prevalence of chronic pelvic pain among women: An updated review. Pain Physician 2014, 17, E141–E147. [Google Scholar]
- Hansrani, V.; Morris, J.; Caress, A.-L.; Payne, K.; Seif, M.; Mccollum, C.N. Is pelvic vein incompetence associated with symptoms of chronic pelvic pain in women? A pilot study. Eur. J. Obstet. Gynecol. Reprod. Biol. 2016, 196, 21–25. [Google Scholar] [CrossRef]
- Hiromura, T.; Nishioka, T.; Nishioka, S.; Ikeda, H.; Tomita, K. Reflux in the left ovarian vein:analysis of MDCT findings in asymptomatic women. Am. J. Roentgenol. 2004, 183, 1411–1415. [Google Scholar] [CrossRef]
- Lechter, A.; Alvarez, A. Pelvic varices and gonadal veins. Phlebologie 1986, 85, 225–228. [Google Scholar] [CrossRef]
- Hobbs, J.T. The pelvic congestion syndrome. Br. J. Hosp. Med. 1990, 43, 200–206. [Google Scholar]
- Asciutto, G.; Asciutto, K.; Mumme, A.; Geier, B. Pelvic venous incompetence: Reflux patterns and treatment results. Eur. J. Vasc. Endovasc. Surg. 2009, 38, 381–386. [Google Scholar] [CrossRef] [Green Version]
- Szary, C.; Wilczko, J.; Plucinska, D.; Pachuta, A.; Napierala, M.; Bodziony, A.; Zawadzki, M.; Leszczynski, J.; Galazka, Z.; Grzela, T. The Analysis of Selected Morphological and Hemodynamic Parameters of the Venous System and Their Presumable Impact on the Risk of Recurrence after Varicose Vein Treatment. J. Clin. Med. 2021, 10, 455. [Google Scholar] [CrossRef]
- Koo, S.; Fan, C.-M. Pelvic congestion syndrome and pelvic varicosities. Tech. Vasc. Interv. Radiol. 2014, 17, 90–95. [Google Scholar] [CrossRef] [PubMed]
- Lopez, A.J. Female Pelvic Vein Embolization: Indications, Techniques, and Outcomes. Cardiovasc. Interv. Radiol. 2015, 38, 806–820. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Whiteley, A.; Taylor, D.; Whiteley, M.S. Pelvic Venous Reflux is a Major Contributory Cause of Recurrent Varicose Veins in more than a Quarter of Women. J. Vasc. Surgery Venous Lymphat. Disord. 2013, 1, 100–101. [Google Scholar] [CrossRef]
- Perrin, M.; Labropoulos, N.; Leon, L.R. Presentation of the patient with recurrent varices after surgery (REVAS). J. Vasc. Surg. 2006, 43, 327–334. [Google Scholar] [CrossRef] [PubMed]
- Marsh, P.; Holdstock, J.; Harrison, C.; Smith, C.; Price, B.A.; Whiteley, M.S. Pelvic vein reflux in female patients with varicose veins: Comparison of incidence between a specialist private vein clinic and the vascular department of a National Health Service District General Hospital. J. Venous Dis. 2009, 24, 108–113. [Google Scholar] [CrossRef]
- Gloviczki, P.; Comerota, A.J.; Dalsing, M.C.; Eklof, B.G.; Gillespie, D.L.; Gloviczki, M.L.; Lohr, J.M.; McLafferty, R.B.; Meissner, M.H.; Murad, M.H.; et al. The care of patients with varicose veins and associated chronic venous diseases: Clinical practice guidelines of the Society for Vascular Surgery and the American Venous Forum. J. Vasc. Surg. 2011, 53 (Suppl. 5), 2S–48S. [Google Scholar] [CrossRef] [Green Version]
- Beard, R.W.; Highman, J.H.; Pearce, S.; Reginald, P.W. Diagnosis of pelvic varicosities in women with chronic pelvic pain. Lancet 1984, 324, 946–949. [Google Scholar] [CrossRef]
- Ganeshan, A.; Upponi, S.; Hon, L.-Q.; Uthappa, M.C.; Warakaulle, D.R.; Uberoi, R. Chronic Pelvic Pain due to Pelvic Congestion Syndrome: The Role of Diagnostic and Interventional Radiology. Cardiovasc. Interv. Radiol. 2007, 30, 1105–1111. [Google Scholar] [CrossRef]
- Park, S.J.; Lim, J.W.; Ko, Y.T.; Lee, D.H.; Yoon, Y.; Oh, J.H.; Lee, H.K.; Huh, C.Y. Diagnosis of Pelvic Congestion Syndrome Using Transabdominal and Transvaginal Sonography. Am. J. Roentgenol. 2004, 182, 683–688. [Google Scholar] [CrossRef] [PubMed]
- Campbell, D.; Halligan, S.; Bartram, C.I.; Rogers, V.; Hollings, N.; Kingston, K.; Sahdev, A.; Beard, R.W. Transvaginal Power Doppler Ultrasound in Pelvic Congestion. A prospective comparison with transuterine venography. Acta Radiol. 2003, 44, 269–274. [Google Scholar] [CrossRef]
- Malgor, R.D.; Adrahtas, D.; Spentzouris, G.; Gasparis, A.P.; Tassiopoulos, A.K.; Labropoulos, N. The role of duplex ultrasound in the workup of pelvic congestion syndrome. J. Vasc. Surgery Venous Lymphat. Disord. 2014, 2, 34–38. [Google Scholar] [CrossRef]
- Labropoulos, N.; Jasinski, P.T.; Adrahtas, D.; Gasparis, A.P.; Meissner, M.H. A standardized ultrasound approach to pelvic congestion syndrome. Phlebol. J. Venous Dis. 2017, 32, 608–619. [Google Scholar] [CrossRef] [PubMed]
- Coakley, F.V.; Varghese, S.L.; Hricak, H. CT and MRI of pelvic varices in women. J. Comput. Assist. Tomogr. 1999, 23, 429–434. [Google Scholar] [CrossRef]
- Bookwalter, C.A.; VanBuren, W.M.; Neisen, M.J.; Bjarnason, H. Imaging Appearance and Nonsurgical Management of Pelvic Venous Congestion Syndrome. Radiographics 2019, 39, 596–608. [Google Scholar] [CrossRef]
- Yang, D.M.; Kim, H.C.; Nam, D.H.; Jahng, G.H.; Huh, C.Y.; Lim, J.W. Time-resolved MR angiography for detecting and grading ovarian venous reflux: Comparison with conventional venography. Br. J. Radiol. 2012, 85, e117–e122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Antignani, P.L.; Lazarashvili, Z.; Monedero, J.L.; Ezpeleta, S.Z.; Whiteley, M.S.; Khilnani, N.M.; Meissner, M.H.; Wittens, C.H.; Kurstjens, R.L.; Belova, L.; et al. Diagnosis and treatment of pelvic congestion syndrome: UIP consensus document. Int. Angiol. 2019, 38, 265–283. [Google Scholar] [CrossRef]
- Khilnani, N.M.; Meissner, M.H.; Learman, L.A.; Gibson, K.D.; Daniels, J.P.; Winokur, R.S.; Marvel, R.P.; Machan, L.; Venbrux, A.C.; Tu, F.F.; et al. Research Priorities in Pelvic Venous Disorders in Women: Recommendations from a Multidisciplinary Research Consensus Panel. J. Vasc. Interv. Radiol. 2019, 30, 781–789. [Google Scholar] [CrossRef] [PubMed]
- Giacchetto, C.; Catizone, F.; Cotroneo, G.B.; Cavallaro, V.; Cammisuli, F.; Minutolo, V.; Rodolico, G. Radiologic anatomy of the genital venous system in female patients with varicocele. Surgery Gynecol. Obstet. 1989, 169, 403–407. [Google Scholar]
- Gültaşli, N.Z.; Kurt, A.; Ipek, A.; Gümüş, M.; Yazicioğlu, K.R.; Dilmen, G.; Taş, I. The relation between pelvic varicose veins, chronic pelvic pain and lower extremity venous insufficiency in women. Diagn. Interv. Radiol. 2006, 12, 34–38. [Google Scholar]
- Koc, Z.; Ulusan, S.; Oguzkurt, L. Association of left renal vein variations and pelvic varices in abdominal MDCT. Eur. Radiol. 2007, 17, 1267–1274. [Google Scholar] [CrossRef]
- Humphries, A.; Mirjalili, S.A.; Tarr, G.P.; Thompson, J.M.D.; Stone, P.R. The effect of supine positioning on maternal hemodynamics during late pregnancy. J. Matern. Neonatal Med. 2019, 32, 3923–3930. [Google Scholar] [CrossRef]
- Ignacio, E.A.; Dua, R.; Sarin, S.; Harper, A.S.; Yim, D.; Mathur, V.; Venbrux, A.C. Pelvic congestion syndrome: Diagnosis and treatment. Semin. Interv. Radiol. 2008, 25, 361–368. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Asciutto, G.; Mumme, A.; Asciutto, K.C.; Geier, B. Oestradiol levels in varicose vein blood of patients with and without pelvic vein incompetence (PVI): Diagnostic implications. Eur. J. Vasc. Endovasc. Surg. 2010, 40, 117–121. [Google Scholar] [CrossRef] [PubMed]
- Hartung, O. Embolization is essential in the treatment of leg varicosities due to pelvic venous insufficiency. Phlebol. J. Venous Dis. 2015, 30 (Suppl. 1), 81–85. [Google Scholar] [CrossRef]
- Ratnam, L.A.; Marsh, P.; Holdstock, J.M.; Harrison, C.S.; Hussain, F.F.; Whiteley, M.S.; Lopez, A. Pelvic vein embolisation in the management of varicose veins. Cardiovasc. Interv. Radiol. 2008, 31, 1159–1164. [Google Scholar] [CrossRef] [PubMed]
- Creton, D.; Hennequin, L.; Kohler, F.; Allaert, F. Embolisation of symptomatic pelvic veins in women presenting with non-saphenous varicose veins of pelvic origin—Three-year follow-up. Eur. J. Vasc. Endovasc. Surg. 2007, 34, 112–117. [Google Scholar] [CrossRef] [PubMed] [Green Version]




















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter or Variable | Value (n = 535) |
|---|---|
| Age | 42.3 ± 10.5 |
| Mean number of pregnancies (P) P0 P1 P2 P3 P4+ | 1.7 ± 1.4 132 (24.7%) 104 (19.4%) 176 (32.9%) 78 (14.6%) 45 (8.4%) |
| Mean number of deliveries | 1.5 ±1.2 |
| Predominant signs and symptoms: dilated reticular and/or “spider” veins lower limbs pain/discomfort abdomino-pelvic pain/discomfort | 197 (33.5%) 252 (47.1%) 104 (19.4%) |
| Clinical CVD classification (CEAP): C1 C2 C3 C4 | 56 (10.5%) 314 (58.7%) 128 (23.9%) 37 (6.9%) |
| - absence, hypoplasia or postthrombotic septations of suprarenal or hepatic segment of IVC |
| - absence or (partial) hypoplasia of LRV (Figure 4) |
| - LRV extrinsic entrapment syndrome (“nutcracker phenomenon”) (Figure 5) |
| - postthrombotic septs or intraluminal webs, channels and spurs in LRV |
| - extrinsic compression of retroaortic LRV |
| - ascending course of the LRV (hilar segment below its distal part) |
| - distended ostium of the LOV draining into the LRV |
| - lack of an ostial or subostial valve in the LOV trunk |
| - atypical LOV drainage (the most frequent form draining into the main branch of LRV) |
| - combined anatomy of the LOV system (e.g., duplication of the main trunk) |
| - absence, hypoplasia or postthrombotic septations of suprarenal or hepatic segment of IVC |
| - absence or hypoplasia of RRV |
| - atypical ROV drainage (draining into the main branch of the RRV or accessory RRV) |
| - high localized ostium of ROV to IVC (on its ventral side) |
| - distended ostium of the ROV typically draining into the IVC |
| - lack of an ostial or subostial valve in the ROV trunk |
| - combined anatomy of the ROV system (e.g., duplication of the ROV trunk) |
| øLOV | incLOV | lPUV | bLIILV | øROV | incROV | rPUV | bRIILV | |
|---|---|---|---|---|---|---|---|---|
| GI | <6 | (−/+) | <5 | <5 | <5 | (−) | <5 | <5 |
| GI/II | 6–6.5 | (+) | <5.5 | <5.5 | <5 | (−) | <5 | <5 |
| GII | <7 | (+) | <6.5 | <6 | <5.5 | (−) | <5.5 | <5.5 |
| GII/III | 7.5–8 | (++) | <7 | <7 | <6 | (−/+) | <6.5 | <6 |
| GIII | >8 | (++) | 7–8 | <7.5 | <7.5 | (+/++) | <7 | <6.5 |
| GIV | >10 | (+++) | >8 | >8 | >8 | (+++) | >7.5 | >7 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Szary, C.; Wilczko, J.; Zawadzki, M.; Grzela, T. Hemodynamic and Radiological Classification of Ovarian Veins System Insufficiency. J. Clin. Med. 2021, 10, 646. https://doi.org/10.3390/jcm10040646
Szary C, Wilczko J, Zawadzki M, Grzela T. Hemodynamic and Radiological Classification of Ovarian Veins System Insufficiency. Journal of Clinical Medicine. 2021; 10(4):646. https://doi.org/10.3390/jcm10040646
Chicago/Turabian StyleSzary, Cezary, Justyna Wilczko, Michal Zawadzki, and Tomasz Grzela. 2021. "Hemodynamic and Radiological Classification of Ovarian Veins System Insufficiency" Journal of Clinical Medicine 10, no. 4: 646. https://doi.org/10.3390/jcm10040646