
Endorectal Ultrasound and Magnetic Resonance Imaging for Rectal Cancer Staging: A Modern Multimodality Approach

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
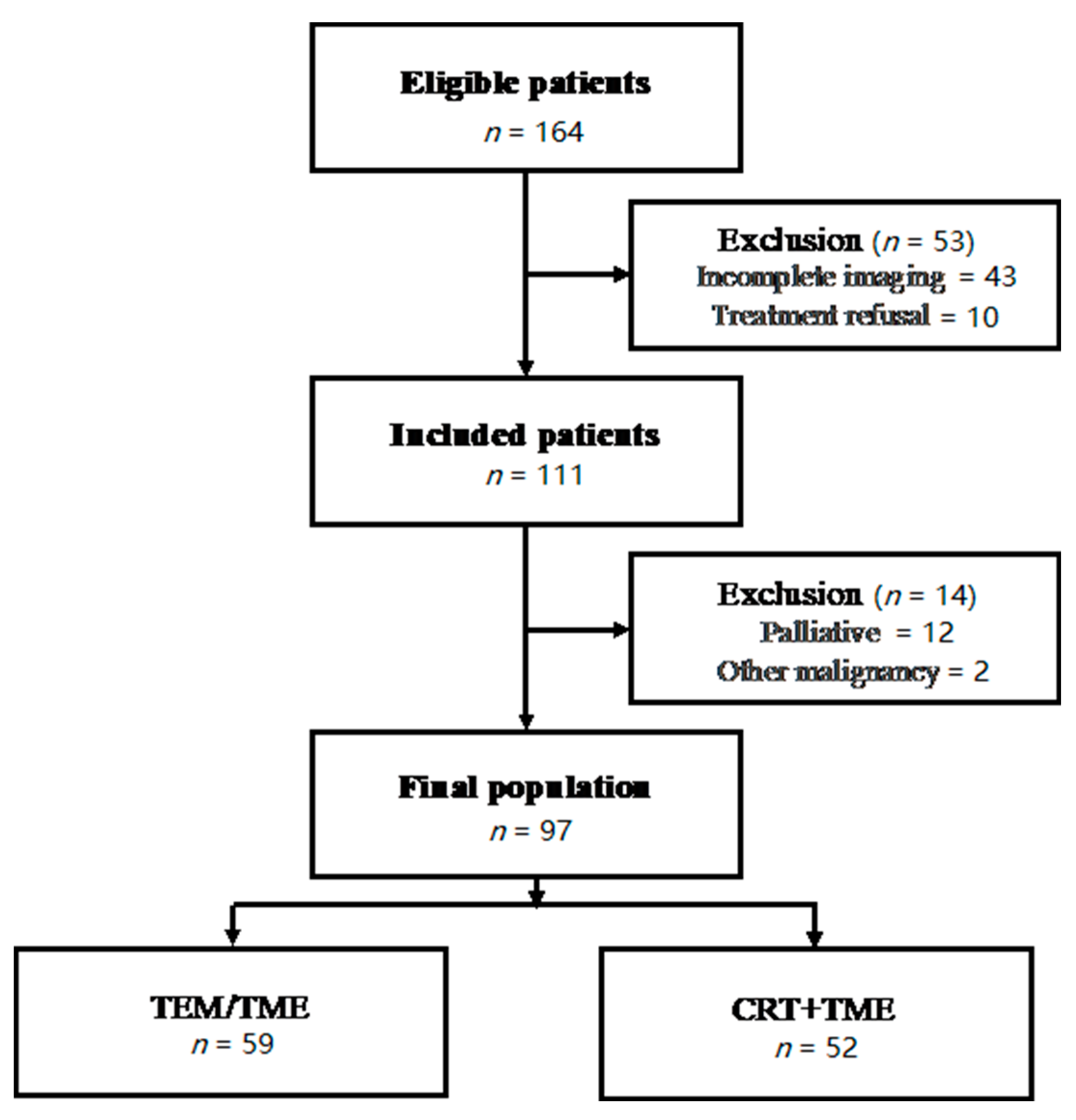
2.1. Patient Population
2.2. Imaging Interpretation
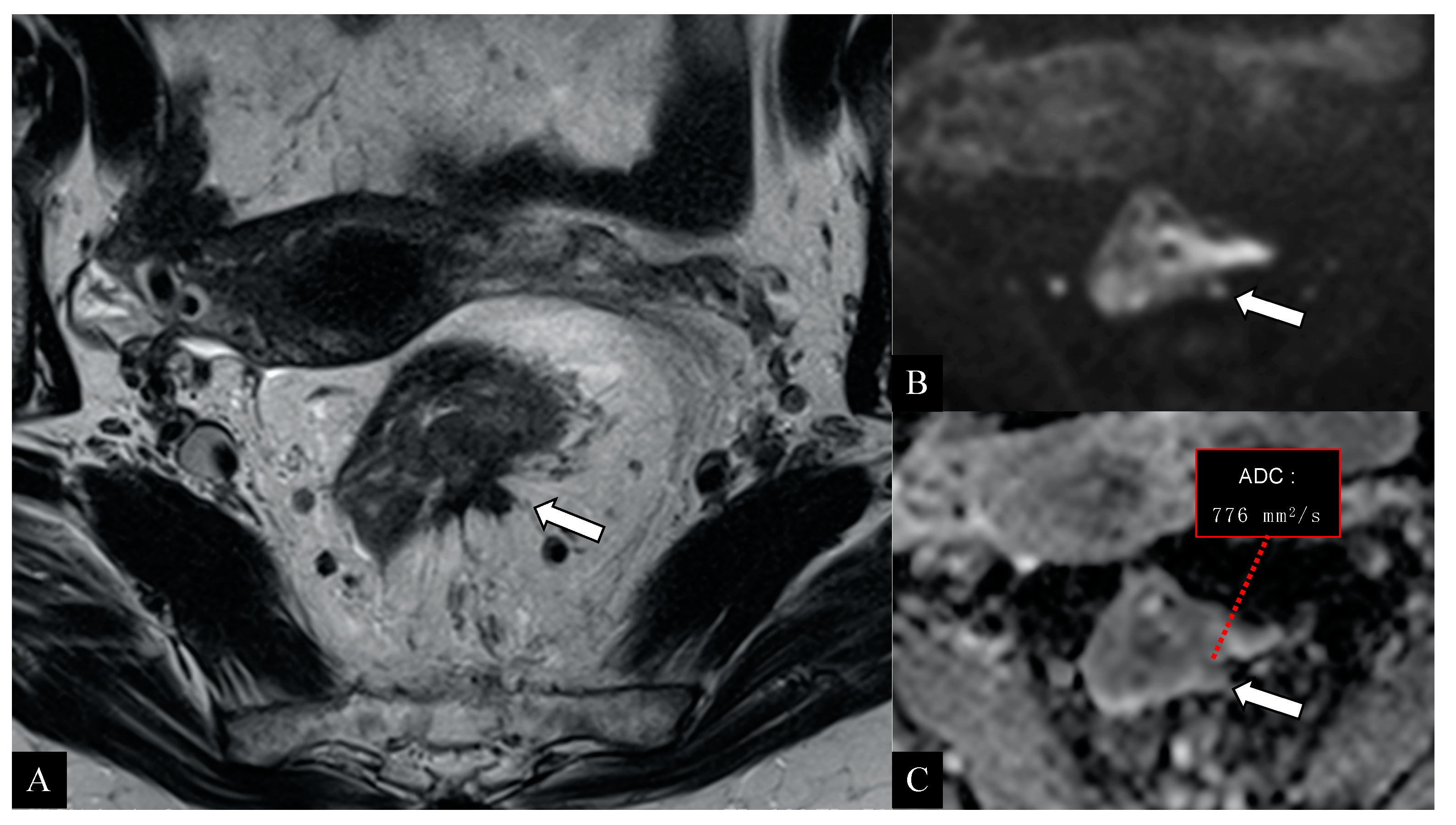
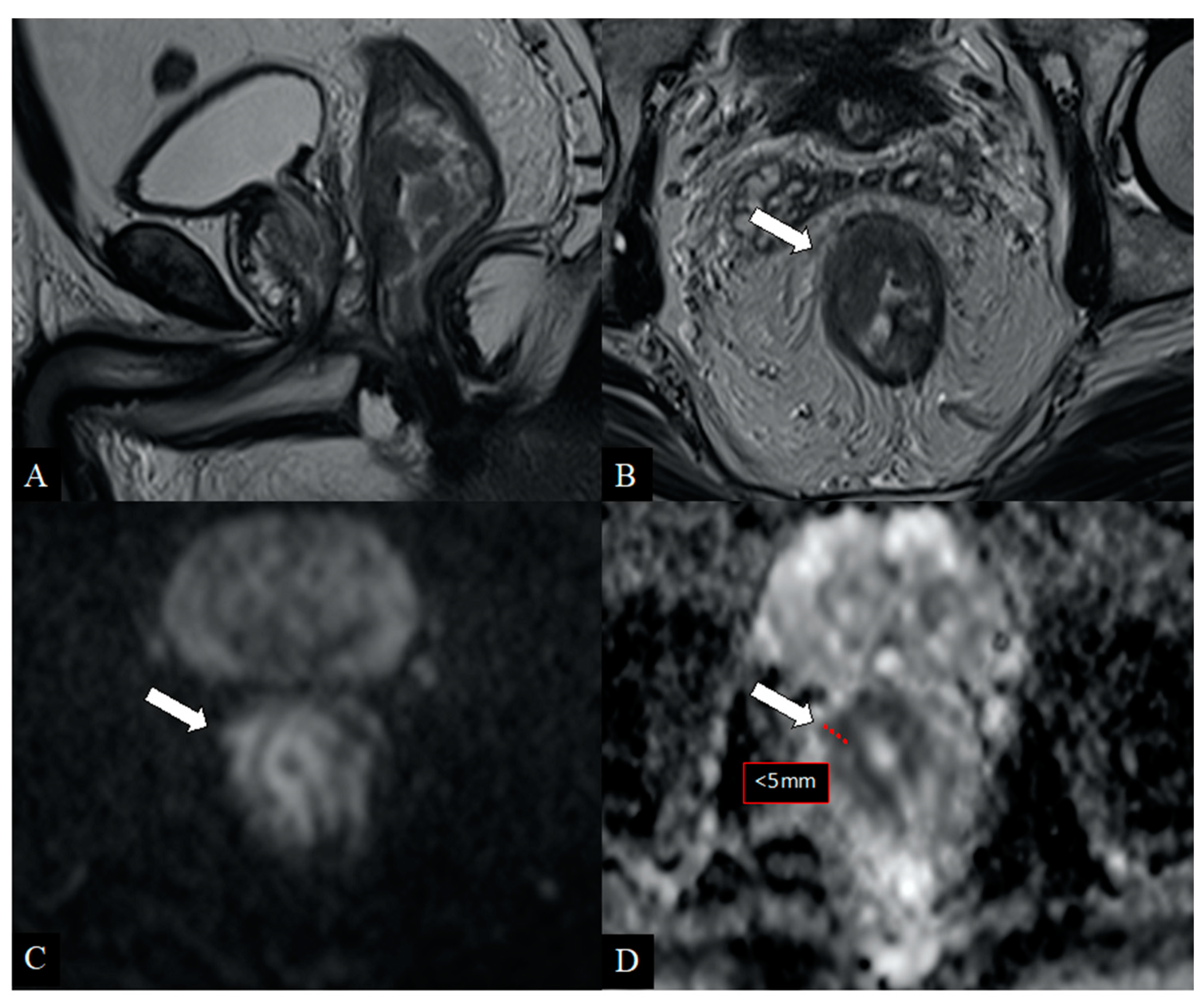
2.3. Magnetic Resonance Imaging
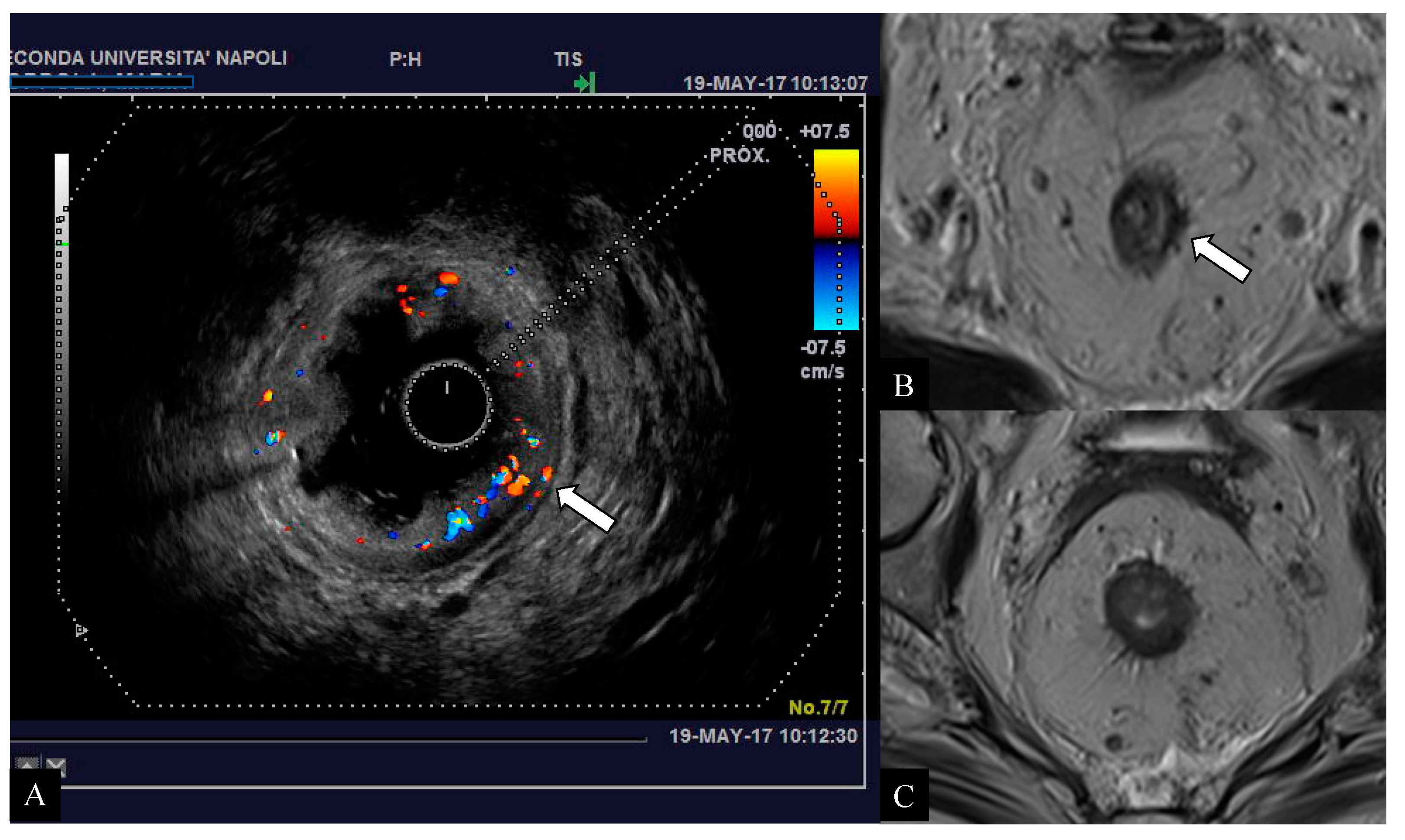
2.4. ERUS
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Jhaveri, K.S.; Hosseini-Nik, H. MRI of Rectal Cancer: An Overview and Update on Recent Advances. Am. J. Roentgenol. 2015, 205, W42–W55. [Google Scholar] [CrossRef]
- World Cancer Research Fund; American Institute for Cancer Research. Continuous Update Project Report Summary. Food, Nutrition, Physical Activity, and the Prevention of Colorectal Cancer 2011. Available online: https://www.wcrf.org/sites/default/files/Colorectal-Cancer-2011-Report.pdf (accessed on 30 September 2020).
- Plummer, J.M.; Leake, P.A.; Albert, M.R. Recent advances in the management of rectal cancer: No surgery, minimal surgery or minimally invasive surgery. World J. Gastrointest. Surg. 2017, 9, 139–148. [Google Scholar] [CrossRef] [PubMed]
- Kav, T.; Bayraktar, Y. How useful is rectal endosonography in the staging of rectal cancer? World J. Gastroenterol. 2010, 16, 691–697. [Google Scholar] [CrossRef]
- Glynne-Jones, R.; Wyrwicz, L.; Tiret, E.; Brown, G.; Rödel, C.; Cervantes, A.; Arnold, D. Rectal cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2017, 28 (Suppl. 4), 22–40. [Google Scholar] [CrossRef]
- National Comprehensive Cancer Network. Clinical Practice Guidelines in Oncology (NCCN Guidelines): Colon Cancer Version 1.2018. 2018. Available online: https://www.nccn.org/professionals/physician_gls/pdf/colon.pdf (accessed on 30 September 2020).
- Balyasnikova, S.; Brown, G. Imaging Advances in Colorectal Cancer. Curr. Colorectal Cancer Rep. 2016, 12, 162–169. [Google Scholar] [CrossRef] [Green Version]
- Merkel, S.; Mansmann, U.; Siassi, M.; Papadopoulos, T.; Hohenberger, W.; Hermanek, P. The prognostic inhomogeneity in pT3 rectal carcinomas. Int. J. Colorectal Dis. 2001, 16, 298–304. [Google Scholar] [CrossRef] [PubMed]
- Brierley, J.D.; Gospodarowicz, M.K.; Wittekind, C. (Eds.) TNM Classification of Malignant Tumours, 8th ed.; John Wiley & Sons, Inc.: Oxford, UK, 2017. [Google Scholar]
- Amin, M.D.; Edge, S.B.; Greene, F.; Byrd, D.R.; Brookland, R.K.; Washington, M.K.; Gershenwald, J.E.; Compton, C.C.; Hess, K.R.; Sullivan, D.C.; et al. (Eds.) AJCC Cancer Staging Manual, 8th ed.; Springer: New York, NY, USA, 2017; pp. 3–30. [Google Scholar]
- Horvat, N.; Carlos Tavares Rocha, C.; Clemente Oliveira, B.; Petkovska, I.; Gollub, M.J. MRI of Rectal Cancer: Tumor Staging, Imaging Techniques, and Management. Radiographics 2019, 39, 367–387. [Google Scholar] [CrossRef] [PubMed]
- Nougaret, S.; Reinhold, C.; Mikhael, H.W.; Rouanet, P.; Bibeau, F.; Brown, G. The use of MR imaging in treatment planning for patients with rectal carcinoma: Have you checked the “DISTANCE”? Radiology 2013, 268, 330–344. [Google Scholar] [CrossRef] [PubMed]
- Klessen, C.; Rogalla, P.; Taupitz, M. Local staging of rectal cancer: The current role of MRI. Eur. Radiol. 2007, 17, 379–389. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Franzè, E.; Dinallo, V.; Rizzo, A.; Di Giovangiulio, M.; Bevivino, G.; Stolfi, C.; Caprioli, F.; Colantoni, A.; Ortenzi, A.; Grazia, A.D.; et al. Interleukin-34 sustains pro-tumorigenic signals in colon cancer tissue. Oncotarget 2017, 9, 3432–3445. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Granata, V.; Fusco, R.; Reginelli, A.; DelRio, P.; Selvaggi, F.; Grassi, R.; Izzo, F.; Petrillo, A. Diffusion kurtosis imaging in patients with locally advanced rectal cancer: Current status and future perspectives. J. Int. Med. Res. 2019, 47, 2351–2360. [Google Scholar] [CrossRef] [Green Version]
- Schurink, N.W.; Lambregts, D.M.J.; Beets-Tan, R.G.H. Diffusion-weighted imaging in rectal cancer: Current applications and future perspectives. Br. J. Radiol. 2019, 92, 20180655. [Google Scholar] [CrossRef] [PubMed]
- Renzulli, M.; Clemente, A.; Ierardi, A.M.; Pettinari, I.; Tovoli, F.; Brocchi, S.; Peta, G.; Cappabianca, S.; Carrafiello, G.; Carrafiello, G. Imaging of Colorectal Liver Metastases: New Developments and Pending Issues. Cancers (Basel) 2020, 12, 151. [Google Scholar] [CrossRef] [Green Version]
- Berton, F.; Gola, G.; Wilson, S.R. Perspective on the role of transrectal and transvaginal sonography of tumors of the rectum and anal canal. Am. J. Roentgenol. 2008, 190, 1495–1504. [Google Scholar] [CrossRef] [PubMed]
- Rouse, H.C.; Godoy, M.C.; Lee, W.K.; Phang, P.T.; Brown, C.J.; Brown, J.A. Imaging findings of unusual anorectal and perirectal pathology: A multi-modality approach. Clin. Radiol. 2008, 63, 1350–1360. [Google Scholar] [CrossRef] [PubMed]
- Puli, S.R.; Bechtold, M.L.; Reddy, J.B.; Choudhary, A.; Antillon, M.R.; Brugge, W.R. How good is endoscopic ultrasound in differentiating various T stages of rectal cancer? Meta-analysis and systematic review. Ann. Surg. Oncol. 2009, 16, 254–265. [Google Scholar] [CrossRef] [PubMed]
- Napoleon, B.; Pujol, B.; Berger, F.; Valette, P.J.; Geralrd, J.P.; Souquet, J.C. Accuracy of endosonography in the staging of rectal cancer treated by radiotherapy. Br. J. Surg. 1991, 78, 785–788. [Google Scholar] [CrossRef] [PubMed]
- Beets, G.L.; Beets-Tan, R.G. Pretherapy imaging of rectal cancers: ERUS or MRI? Surg. Oncol. Clin. N. Am. 2010, 19, 733–741. [Google Scholar] [CrossRef] [PubMed]
- Srisajjakul, S.; Prapaisilp, P.; Bangchokdee, S. Pitfalls in MRI of rectal cancer: What radiologists need to know and avoid. Clin. Imaging 2018, 50, 130–140. [Google Scholar] [CrossRef] [PubMed]
- Oien, K.; Forsmo, H.M.; Rösler, C.; Nylund, K.; Waage, J.E.; Pfeffer, F. Endorectal ultrasound and magnetic resonance imaging for staging of early rectal cancers: How well does it work in practice? Acta Oncol. 2019, 58 (Suppl. 1), S49–S54. [Google Scholar] [CrossRef] [Green Version]
- Scheele, J.; Schmidt, S.A.; Tenzer, S.; Henne-Bruns, D.; Kornmann, M. Overstaging: A Challenge in Rectal Cancer Treatment. Visc. Med. 2018, 34, 301–306. [Google Scholar] [CrossRef] [PubMed]
- Reginelli, A.; Clemente, A.; Cardone, C.; Urraro, F.; Izzo, A.; Martinelli, E.; Troiani, T.; Ciardiello, F.; Brunese, L.; Cappabianca, S. Computed tomography densitometric study of anti-angiogenic effect of regorafenib in colorectal cancer liver metastasis. Future Oncol. 2018, 14, 2905–2913. [Google Scholar] [CrossRef] [PubMed]
- Zorcolo, L.; Fantola, G.; Cabras, F.; Marongiu, L.; D’Alia, G.; Casula, G. Preoperative staging of patients with rectal tumors suitable for transanal endoscopic microsurgery (TEM): Comparison of endorectal ultrasound and histopathologic findings. Surg. Endosc. 2009, 23, 1384–1389. [Google Scholar] [CrossRef] [PubMed]
- Beets-Tan, R.G.H.; Lambregts, D.M.J.; Maas, M.; Bipat, S.; Barbaro, B.; Curvo-Semedo, L.; Fenlon, H.M.; Gollub, M.C.; Gourtsoyianni, S.; Halligan, S.; et al. Magnetic resonance imaging for clinical management of rectal cancer: Updated recommendations from the 2016 European society of gastrointestinal and abdominal radiology (ESGAR) consensus meeting. Eur. Radiol. 2018, 28, 1465–1475. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taylor, F.G.; Swift, R.I.; Blomqvist, L.; Brown, G. A systematic approach to the interpretation of preoperative staging MRI for rectal cancer. Am. J. Roentgenol. 2008, 191, 1827–1835. [Google Scholar] [CrossRef] [PubMed]
- Luzietti, E.; Pellino, G.; Nikolaou, S.; Qiu, S.; Mills, S.; Warren, O.; Tekkis, P.; Kontovounisios, C. Comparison of guidelines for the management of rectal cancer. BJS Open 2018, 2, 433–451. [Google Scholar] [CrossRef] [Green Version]
- Battersby, N.J.; How, P.; Moran, B.; Stelzner, S.; West, N.P.; Branagan, G.; Strassburg, J.; Quirke, P.; Tekkis, P.; Pedersen, B.G.; et al. Prospective Validation of a Low Rectal Cancer Magnetic Resonance Imaging Staging System and Development of a Local Recurrence Risk Stratification Model: The MERCURY II Study. Ann. Surg. 2016, 263, 751–760. [Google Scholar] [CrossRef] [Green Version]
- Taylor, F.G.; Quirke, P.; Heald, R.J.; Moran, B.J.; Blomqvist, L.; Swift, I.R.; Sebag-Montefiore, D.; Tekkis, P.; Brown, G. Preoperative Magnetic Resonance Imaging Assessment of Circumferential Resection Margin Predicts Disease-Free Survival and Local Recurrence: 5-Year Follow-Up Results of the MERCURY Study. J. Clin. Oncol. 2014, 32, 34–43. [Google Scholar] [CrossRef] [PubMed]
- Hildebrandt, U.; Feifel, G.; Schwarz, H.P.; Scherr, O. Endorectal ultrasound: Instrumentation and clinical aspects. Int. J. Colorectal. Dis. 1986, 1, 203–207. [Google Scholar] [CrossRef] [PubMed]
- Gunderson, L.L.; Callister, M.; Marschke, R.; Young-Fadok, T.; Heppell, J.; Efron, J. Stratification of rectal cancer stage for selection of postoperative chemoradiotherapy: Current status. Gastrointest. Cancer Res. 2008, 2, 25–33. [Google Scholar]
- Sauer, R.; Liersch, T.; Merkel, S.; Fietkau, R.; Hohenberger, W.; Hess, C.; Becker, H.; Raab, H.-R.; Villanueva, M.-T.; Witzigmann, H.; et al. Preoperative versus postoperative chemoradiotherapy for locally advanced rectal cancer: Results of the German CAO/ARO/AIO-94 randomized phase III trial after a median follow-up of 11 years. J. Clin. Oncol. 2012, 30, 1926–1933. [Google Scholar] [CrossRef] [PubMed]
- Heo, S.H.; Kim, J.W.; Shin, S.S.; Jeong, Y.Y.; Kang, H.K. Multimodal imaging evaluation in staging of rectal cancer. World J. Gastroenterol. 2014, 20, 4244–4255. [Google Scholar] [CrossRef]
- Zhang, G.; Cai, Y.Z.; Xu, G.H. Diagnostic Accuracy of MRI for Assessment of T Category and Circumferential Resection Margin Involvement in Patients With Rectal Cancer: A Meta-Analysis. Dis. Colon Rectum 2016, 59, 789–799. [Google Scholar] [CrossRef]
- Yu, L.; Wang, L.; Tan, Y.; Hu, H.; Shen, L.; Zheng, S.; Ding, K.; Zhang, S.; Yuan, Y. Accuracy of Magnetic Resonance Imaging in Staging Rectal Cancer with Multidisciplinary Team: A Single-Center Experience. J. Cancer 2019, 10, 6594–6598. [Google Scholar] [CrossRef] [PubMed]
- Beets-Tan, R.G.; Beets, G.L.; Vliegen, R.F.; Kessels, A.; Van Boven, H.; De Bruine, A.; Von Meyenfeldt, M.F.; Baeten, C.; Van Engelshoven, J. Accuracy of magnetic resonance imaging in prediction of tumour free resection margin in rectal cancer surgery. Lancet 2001, 357, 497–504. [Google Scholar] [CrossRef]
- Gualdi, G.F.; Casciani, E.; Guadalaxara, A.; d’Orta, C.; Polettini, E.; Pappalardo, G. Local staging of rectal cancer with transrectal ultrasound and endorectal magnetic resonance imaging: Comparison with histologic findings. Dis. Colon Rectum 2000, 43, 338–345. [Google Scholar] [CrossRef]
- Nardone, V.; Reginelli, A.; Scala, F.; Carbone, S.F.; Mazzei, M.A.; Sebaste, L.; Cafragno, T.; Battaglia, G.; Pastina, P.; Correale, P.; et al. Magnetic-Resonance-Imaging Texture Analysis Predicts Early Progression in Rectal Cancer Patients Undergoing Neoadjuvant Chemoradiation. Gastroenterol. Res. Pract. 2019, 2019. [Google Scholar] [CrossRef] [PubMed]
- Attenberger, U.I.; Pilz, L.R.; Morelli, J.N.; Hausmann, D.; Doyon, F.; Hofheinz, R.; Koienle, P.; Post, S.; Michaely, H.J.; Schoenberg, S.O.; et al. Multi-parametric MRI of rectal cancer—Do quantitative functional MR measurements correlate with radiologic and pathologic tumor stages? Eur. J. Radiol. 2014, 83, 1036–1043. [Google Scholar] [CrossRef] [PubMed]
- Shinya, S.; Sasaki, T.; Nakagawa, Y.; Guiquing, Z.; Yamamoto, F.; Yamashita, Y. The efficacy of diffusion-weighted imaging for the detection of colorectal cancer. Hepatogastroenterology 2009, 56, 128–132. [Google Scholar] [PubMed]
- Chen, L.; Shen, F.; Li, Z.; Lu, H.; Chen, Y.; Wang, Z.; Lu, J. Diffusion-weighted imaging of rectal cancer on repeatability and cancer characterization: An effect of b-value distribution study. Cancer Imaging 2018, 18, 43. [Google Scholar] [CrossRef] [PubMed]
- Park, J.S.; Jang, Y.J.; Choi, G.S.; Park, S.Y.; Kim, H.J.; Kang, H.; Cho, S.H. Accuracy of preoperative MRI in predicting pathology stage in rectal cancers: Node-for-node matched histopathology validation of MRI features. Dis. Colon Rectum 2014, 57, 32–38. [Google Scholar] [CrossRef] [PubMed]
- Cai, Z.; Xie, X.; Chen, Y.; Chen, Z.; Cao, W.; Saad, K.S.S.; Zou, Y.; Lan, P.; Wu, X. Risk factor analysis for inaccurate pre-operative MRI staging in rectal cancer. BMC Cancer 2020, 20, 253. [Google Scholar] [CrossRef] [PubMed]
- Pellino, G.; Alós, R.; Biondo, S.; Codina-Cazador, A.; Enríquez-Navascues, J.M.; Espín-Basany, E.; Roig-Vila, J.V.; Cervantes, A.; Garcia-Granero, E. Spanish Rectal Cancer Project collaborators. Trends and outcome of neoadjuvant treatment for rectal cancer: A retrospective analysis and critical assessment of a 10-year prospective national registry on behalf of the Spanish Rectal Cancer Project. Eur. J. Surg. Oncol. 2021, 47, 276–284. [Google Scholar] [CrossRef] [PubMed]
- Baird, D.L.H.; Denost, Q.; Simillis, C.; Pellino, G.; Rasheed, S.; Kontovounisios, C.; Tekkis, P.; Ruller, E. The effect of adjuvant chemotherapy on survival and recurrence after curative rectal cancer surgery in patients who are histologically node negative after neoadjuvant chemoradiotherapy. Colorectal Dis. 2017, 19, 980–986. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garcia-Granero, A.; Pellino, G.; Giner, F.; Frasson, M.; Fletcher-Sanfeliu, D.; Romaguera, V.P.; Flor-Lorente, B.; Gamundi, M.; Brogi, L.; Garcia-Calderón, D.; et al. A mathematical 3D-method applied to MRI to evaluate prostatic infiltration in advanced rectal cancer. Tech. Coloproctol. 2020, 24, 605–607. [Google Scholar] [CrossRef] [PubMed]
- Johnson, N.; Pellino, G.; Simillis, C.; Qiu, S.; Nikolaou, S.; Baird, D.L.; Rasheed, S.; Tekkis, P.; Kontovounisios, C. Discrepancies between NCCN and ESMO guidelines in the management of anal cancer: A qualitative review. Updates Surg. 2017, 69, 345–349. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| a | |||||
| Pathology Stage | |||||
| MRI-Stage | T1 | T2 | T3 | T4 | Total |
| T1 | 2 | 0 | 0 | 0 | 2 |
| T2 | 1 | 16 | 0 | 0 | 17 |
| T3 | 0 | 6 | 58 | 1 | 65 |
| T4 | 0 | 0 | 3 | 10 | 13 |
| Total | 3 | 22 | 61 | 11 | 97 |
| b | |||||
| Pathology Stage | |||||
| MRI+DWI-Stage | T1 | T2 | T3 | T4 | Total |
| T1 | 3 | 0 | 0 | 0 | 3 |
| T2 | 0 | 19 | 0 | 0 | 19 |
| T3 | 0 | 3 | 59 | 0 | 62 |
| T4 | 0 | 0 | 2 | 10 | 13 |
| Total | 3 | 22 | 61 | 11 | 97 |
| c | |||||
| Pathology Stage | |||||
| ERUS-Stage | T1 | T2 | T3 | T4 | Total |
| T1 | 3 | 0 | 0 | 0 | 3 |
| T2 | 0 | 20 | 3 | 0 | 23 |
| T3 | 0 | 2 | 58 | 1 | 61 |
| T4 | 0 | 0 | 0 | 10 | 10 |
| Total | 3 | 22 | 61 | 11 | 97 |
| STAGE | MRI | MRI + DWI | ERUS | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| N | SE | SP | VPP | VPN | N | SE | SP | VPP | VPN | N | SE | SP | VPP | VPN | |
| T1 | 2 | 66.7 | 98.1 | 66.7 | 98.9 | 3 | 100.0 | 100.0 | 100.0 | 100.0 | 3 | 100.0 | 100.0 | 100.0 | 100.0 |
| T2 | 17 | 76.2 | 94.2 | 76.2 | 94.1 | 19 | 86.4 | 96.3 | 86.4 | 96.3 | 23 | 81.8 | 95.1 | 81.8 | 95.1 |
| T3 | 65 | 82.1 | 87.5 | 90.2 | 77.8 | 62 | 91.9 | 90.9 | 93.4 | 88.8 | 61 | 95.1 | 100.0 | 100.0 | 92.3 |
| T4 | 13 | 90.9 | 98.9 | 90.9 | 98.9 | 13 | 100.0 | 100.0 | 100.0 | 100.0 | 10 | 90.1 | 98.9 | 90.9 | 98.9 |
| Agreement | MRI | ERUS | |
|---|---|---|---|
| Conventional | DWI | ||
| Agreement (%) | 88.5 | 92.7 | 88.5 |
| Coefficient kappa Cohen (κ) | 0.759 | 0.845 | 0.762 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Reginelli, A.; Clemente, A.; Sangiovanni, A.; Nardone, V.; Selvaggi, F.; Sciaudone, G.; Ciardiello, F.; Martinelli, E.; Grassi, R.; Cappabianca, S. Endorectal Ultrasound and Magnetic Resonance Imaging for Rectal Cancer Staging: A Modern Multimodality Approach. J. Clin. Med. 2021, 10, 641. https://doi.org/10.3390/jcm10040641
Reginelli A, Clemente A, Sangiovanni A, Nardone V, Selvaggi F, Sciaudone G, Ciardiello F, Martinelli E, Grassi R, Cappabianca S. Endorectal Ultrasound and Magnetic Resonance Imaging for Rectal Cancer Staging: A Modern Multimodality Approach. Journal of Clinical Medicine. 2021; 10(4):641. https://doi.org/10.3390/jcm10040641
Chicago/Turabian StyleReginelli, Alfonso, Alfredo Clemente, Angelo Sangiovanni, Valerio Nardone, Francesco Selvaggi, Guido Sciaudone, Fortunato Ciardiello, Erika Martinelli, Roberto Grassi, and Salvatore Cappabianca. 2021. "Endorectal Ultrasound and Magnetic Resonance Imaging for Rectal Cancer Staging: A Modern Multimodality Approach" Journal of Clinical Medicine 10, no. 4: 641. https://doi.org/10.3390/jcm10040641