1. Introduction
Patients undergoing valve surgery due to infective endocarditis (IE) are heterogenous, yet they present with a persistently high perioperative mortality, ranging from 7.6 to 25% [
1,
2,
3]. Even if the patients receive optimal antibiotic treatment nowadays, postoperative sepsis is still the main reason for adverse outcomes [
4]. The biocompatibility of cardiopulmonary bypass (CPB) has undergone constant improvements in recent years [
5], since efficient regimens to treat septic shock, especially in endocarditis patients, are of paramount importance. Patients suffering from IE are at higher risk for complications such as stroke, heart failure, or in-hospital mortality compared to patients undergoing cardiac surgery without IE [
6], since they are in a higher inflammatory state [
7,
8]. It was shown that patients undergoing cardiac surgery with CPB that present with higher levels of preoperative inflammatory markers are also more prone to postoperative complications such as low cardiac output syndrome and cardiac death [
9].
Possibly, patients producing higher inflammatory mediator levels have suffered more severe valvular damages by IE than patients revealing lower inflammatory mediator levels. In addition, high serum levels of inflammatory mediators might reflect an insufficient control of the infection, which could lead to complications (e.g., multi-organ failure, myocardial failure, etc.) [
7,
9]. Interleukin-6 peak levels were shown to correlate with aortic cross clamp time as well as postoperative myocardial dysfunction [
10]. As a consequence, the potential of blood purification during CPB to reduce inflammatory mediators was investigated, yet with controversial results [
11,
12,
13].
The CytoSorb
® (HA, Cytosorbents Corporation, NJ, USA) hemoadsorption device is an extracorporeal cytokine adsorber that was designed to remove inflammatory mediators in critically ill patients. It consists of polymer beads that bind compounds in the range of 10 to 55 kDa and is installed into the venous system of the CPB between the oxygenator and the reservoir. Besides decreasing the inflammatory response, HA might even reduce bleeding complications in patients who undergo emergency cardiac surgery with ticagrelor or rivaroxaban [
10]. Promising case series in critically ill patients reported that HA is safe and not associated with adverse events [
7,
8,
14]. One unmatched retrospective study in patients with mitral valve IE reported a reduced demand of vasopressors and a lower incidence of postoperative sepsis [
15]. However, no study has shown significant clinical benefits in patients undergoing cardiac surgery to date. To the best of our knowledge, this is the first work based on a retrospective inverse probability of treatment-weighted analysis comparing the effects of HA in IE patients undergoing valve surgery with CPB. Aim of this study was the evaluation of clinical benefits of HA therapy with in-hospital mortality as primary outcome measure. The effect of HA on cytokine levels was not analyzed and, due to the nature of this retrospective study, not part of the study design.
2. Materials and Methods
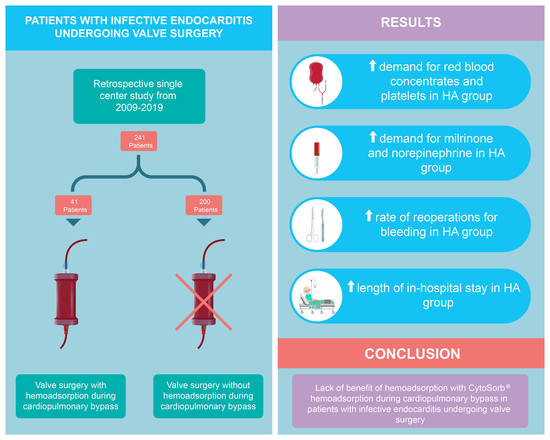
We performed a retrospective single-center database analysis at the Department of Cardiac Surgery, University Hospital of Basel, Switzerland. A total of 241 patients (>18 years) had undergone cardiac surgery for IE between January 2009 and December 2019. Hemoadsorption during CPB was introduced in Basel in 2016 and has ever since been used in most endocarditis patients during valve surgery. The HA device was installed into the venous CPB, so that the blood was pumped via a side arm back into the reservoir, as described previously (
Figure 1) [
15]. The average flow rate via the HA device was 500 mL/min. Hemoadsorption was discontinued at the ICU, for example during continuous veno-venous hemofiltration treatment. Endocarditis was diagnosed according to the Duke criteria [
16] in all patients. Two groups were formed: patients who were treated with HA during CPB were retrospectively assigned to the HA-group, all other patients served as control group. Patient characteristics, inclusion criteria, risk factors, surgical details, and outcome data are routinely collected in the department’s prospectively maintained quality management software (Dendrite Clinical Systems, V1.7), and regularly checked for completeness and consistency. Data from the intensive care unit (ICU) were analyzed for the first 24 postoperative hours. Inotropy and blood product demand during reoperations within the first 24 h were included into the analyses. Major adverse cardiac and cerebrovascular events (MACCE) were defined as in-hospital mortality, myocardial ischemia or stroke and serological parameters. Neurological complications included ischemic events, encephalopathy, meningitis, hemorrhages, and brain abscesses. According to standard protocol, no heparin was administered during the first six hours after arrival at the ICU. The study was conducted in accordance with the Declaration of Helsinki, and the protocol was approved by the local Ethics Committee of Northwestern and Central Switzerland (BASEC Req-2019-01740). The trial was registered at
ClinicalTrials.gov (
www.clinicaltrials.gov (accessed on 20 December 2020), identifier: NCT04309591).
Statistical Analysis
To investigate the impact of HA on the outcome, we used inverse probability of treatment weighting (IPTW) in order to achieve balanced distributions of baseline characteristics in both treatment groups, and to minimize confounding by indication. We included the perioperative intake of platelet aggregation inhibitors, European System for Cardiac Operative Risk Evaluation (EuroSCORE II) score after log-transformation, patient age, New York Heart Association Functional Classification (NYHA) class III or IV, prior myocardial infarction, peripheral artery disease, and nicotine use as covariates into the propensity model. We truncated IPT weights that exceeded the 1st or 99th percentile [
17]. As balance diagnostics, we calculated standardized differences of pre-treatment variables. Absolute values of standardized differences of 0.1 or less were considered to indicate no relevant difference between treatment groups. (Scatterplot in
Figure S1) We used mixed linear models after IPTW to study whether HA impacts the development of hemoglobin, fibrinogen, C-reactive protein (CRP), platelets, and white blood cell (WBC) counts within five days after surgery, including an interaction term HA × time. In order not to depend on linearity of marker development, we repeated the analysis only including measurements of day one and two, and day one, two, and three, respectively. During the period of patient enrollment, intensive care strategies underwent some relevant changes in our hospital. Fluid resuscitation at the ICU was changed in 2016 to less fluid and increased inotropic support and fresh frozen plasma was used to replace for hydroxyethyl starch since 2014. To account for these changes, we adjusted for impact of time using fractional polynomials as a sensitivity analysis, and report adjusted
p-values for variables which might be substantially affected by these changes: epinephrine, dobutamine, milrinone, norepinephrine, and fresh frozen plasma (FFP). Continuous variables were presented as mean ± standard deviation if normally distributed, or as geometric mean with standard deviations back-transformed from the log scale if distribution was skewed. Corresponding
p-values were calculated using linear regression on the variable or on the log-transformed variable. We dichotomized medical intensive care treatment details due to skewed distribution, zero inflation, and the small sample size. Categories were presented as numbers and percentage,
p-values were calculated using logistic regression for binary variables, or multinomial regression otherwise. Significance was accepted at
p < 0.05. Statistical analyses were performed with Stata 15 (StataCorp, College Station, TX, USA).
4. Discussion
This retrospective single-center study describes the outcome after HA application during CPB in IE patients undergoing valve surgery. While perioperative mortality and length of ICU stay were statistically comparable in both groups, the in-hospital stay was significantly longer in HA group. The most important finding of this study is that HA patients were associated with higher reoperation rates for bleeding than the patients in the control group. In addition, demand for norepinephrine, red blood cell concentrates, and platelets was markedly increased in the HA group.
In-hospital mortality in patients with IE undergoing valve surgery ranges from 7.6 to 25% [
1,
2,
3]. Träger et al. [
14] reported in-hospital mortality rates of 25% in 39 IE patients treated with HA perioperatively, which was higher than in our study. An explanation might be that, compared to our studied patients, the patient population in this study was more heterogenous (mean EuroSCORE II: 11 (2.2–96.7)%; mean CPB time: 132 (64–445) min). Two small single-center randomized controlled trials [
18,
19] comparing the cytokine profiles and clinical outcomes of patients undergoing elective cardiac surgery showed no influence of HA on short-term mortality [
18]. This is in line with our data, which show comparable in-hospital mortality rates for both the HA and the control group.
Hemoadsorption with Cytosorb
® targets molecules with a molecular weight from 10–60 kDa [
20], a range which also includes coagulation factors, such as protein C, antithrombin III (58 kDa), Factors VII (50 kDa) and X (58.8 kDa). While previous studies have reported a relevant platelet drop in patients treated with HA [
21,
22], a recent retrospective study by Hassan et al. [
23] on emergency open-heart surgery suggested that HA might reduce postoperative bleeding, drainage, and rethoracotomy rates in patients undergoing surgery with either Ticagrelor or Rivaroxaban. These results might be partly explained by a preclinical study that showed a >99% elimination of Ticagrelor in human blood experiments [
24]. However, besides its small sample size, the trial by Hassan et al. also lacks a matched control [
23]. In our control group, the reoperation rate for bleeding was consistent with the one reported in the existing literature [
25,
26]. However, an almost four-fold increased rate of reoperations for bleeding was observed in the HA group. Furthermore, the postoperative demand for blood products (red blood cell concentrates and platelets) was significantly higher in patients that had been treated with HA. Consecutively, the increased bleeding caused by adsorption of coagulation factors probably also led to hypovolemia in the HA group, which is another thinkable explanation for our observation of higher milrinone and norepinephrine support. Interestingly, although the fluid resuscitation protocol has been changed in 2016 from high volume and low inotropic support to low volume and high inotropic support at our institution, the HA group still showed an increased demand for norepinephrine and milrinone, even after adjustment for time. HA during CPB has been introduced at our department in 2016. Since postoperative hemodilution has been higher before 2014, we would have expected an increased rate of red blood cell concentrates (RBC), platelets, and reoperation for bleeding in the control group, if both groups were similar. To the best of our knowledge, no other study has shown an increased reoperation rate due to bleeding in the context of HA to date.
Next to the potential adsorption of coagulation factors, the higher demand for inotropic support might be explained by induction of vasoplegia due to HA, which affects the levels of various endogenous vasoconstrictors: HA reduces (1) cortisol in brain-dead subjects [
27,
28], (2) thromboxane levels in an ex-vivo model in porcine kidneys [
29], (3) Big-Endothelin-1, a precursor of vasoconstricting endothelin-1, that peaks at the onset of sepsis and is up-regulated by interleukin-1, interleukin-2 and interleukin-6 [
30], and (4) albumin, which maintains the plasma colloid oncotic pressure [
31] and might improve hemodynamics after cardiac surgery [
21,
32] (
Table 6). Further studies are needed to evaluate the eventual vasoplegic impact of HA via adsorption of these regulators.
Recent unmatched reports suggested a reduction of the duration of the ICU stay in HA-treated patients [
9,
10], as well as potential financial savings by the use of HA [
37], which could not be confirmed in our patient cohort. In our study, the HA group presented a prolonged length of in-hospital stay and a higher demand for blood products.
Data on the use of HA in cardiac surgery are scarce, and the existing literature is controversial. A randomized controlled trial (RCT) of 37 patients undergoing cardiac surgery with or without the concomitant use of HA failed to demonstrate a significant reduction of peri- and postoperative levels of pro-inflammatory cytokines and showed no differences in clinical outcomes between the two groups [
19]. Another study in patients with endocarditis showed postoperative IL-6 and IL-8 reduction and comparable hemodynamic stability in 39 patients treated with HA [
38]. In patients undergoing heart transplantation as well as in patients with severe postoperative SIRS, HA might improve the clinical outcome although all the conducted investigations described only small sample sizes [
38,
39]. Recently, Haidari et al. [
15] described similar postoperative WBC counts, but a reduction of postoperative sepsis in patients with mitral valve IE and HA therapy during CPB (HA vs. Control: 17 vs. 39%,
p = 0.005). Our results are not consistent with those of Haidari’s study, since although we even observed a significant reduction of WBCs in the HA group, postoperative sepsis has occurred more frequently in the HA group (HA vs. Control 14.4 vs. 6.2 %;
p = 0.108). According to Bernardi et al. [
19], IL-6 expression peaks around 24 h after the patient is taken off the CPB. Therefore, termination of HA administration together with CPB might be too soon to observe any clinical effect.
Study Limitations
The authors acknowledge three restricted limitations of the study. First, it was a single-center, retrospective study with a limited number of patients. Second, even though IPTW was performed to obtain comparable groups, standardized difference with respect to the intake of platelet inhibitors did not drop below 0.2, indicating residual confounding. However, to the best of our knowledge, this is the first study reporting HA outcomes in valve surgery in patients suffering from IE. Third, inflammatory blood values (e.g., IL-6) are not available for our patients since they are not part of routine laboratory analyses at our department.


 ,
, 



{kind=link}
{kind=link}
{kind=link}