The Analysis of Selected Morphological and Hemodynamic Parameters of the Venous System and Their Presumable Impact on the Risk of Recurrence after Varicose Vein Treatment

Abstract
:1. Introduction
2. Experimental Section
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Raffetto, J.D.; Mannello, F. Pathophysiology of chronic venous disease. Int. Angiol. 2014, 33, 212–221. [Google Scholar] [PubMed]
- Davies, A.H. The seriousness of chronic venous disease: A review of real-world evidence. Adv. Ther. 2019, 36, 5–12. [Google Scholar] [CrossRef] [PubMed]
- Rabe, E.; Guex, J.J.; Puskas, A.; Scuderi, A.; Quesada, F.F.; VCP Coordinators. Epidemiology of chronic venous disorders in geographically diverse populations: Results from the Vein Consult Program. Int. Angiol. 2012, 31, 105–115. [Google Scholar] [PubMed]
- Evans, C.J.; Fowkes, F.G.; Ruckley, C.V.; Lee, A.J. Prevalence of varicose veins and chronic venous insufficiency in men and women in the general population: Edinburgh Vein Study. J. Epidemiol. Community Health 1999, 53, 149–153. [Google Scholar] [CrossRef] [Green Version]
- Maurins, U.; Hoffmann, B.H.; Lösch, C.; Jöckel, K.H.; Rabe, E.; Pannier, F. Distribution and prevalence of reflux in the superficial and deep venous system in the general population—Results from the Bonn Vein Study, Germany. J. Vasc. Surg. 2008, 48, 680–687. [Google Scholar] [CrossRef] [Green Version]
- Jawien, A.; Grzela, T.; Ochwat, A. Prevalence of chronic venous insufficiency in men and women in Poland: Multicentre cross-sectional study in 40,095 patients. Phlebology 2003, 18, 110–122. [Google Scholar] [CrossRef]
- Feodor, T.; Baila, S.; Mitea, I.; Branisteanu, D.; Vittos, O. Epidemiology and clinical characteristics of chronic venous disease in Romania. Exp. Ther. Med. 2019, 17, 1097–1105. [Google Scholar] [CrossRef]
- Lawaetz, M.; Serup, J.; Lawaetz, B.; Bjoern, L.; Blemings, A.; Eklof, B.; Rasmussen, L. Comparison of endovenous ablation techniques, foam sclerotherapy and surgical stripping for great saphenous varicose veins. Extended 5-year follow-up of a RCT. Int. Angiol. 2017, 36, 281–288. [Google Scholar] [CrossRef]
- Van der Velden, S.K.; Biemans, A.A.; De Maeseneer, M.G.; Kockaert, M.A.; Cuypers, P.W.; Hollestein, L.M.; Neumann, H.A.; Nijsten, T.; van den Bos, R.R. Five-year results of a randomized clinical trial of conventional surgery, endovenous laser ablation and ultrasound-guided foam sclerotherapy in patients with great saphenous varicose veins. Br. J. Surg. 2015, 102, 1184–1194. [Google Scholar] [CrossRef]
- Bozkurt, A.K.; Yılmaz, M.F. A prospective comparison of a new cyanoacrylate glue and laser ablation for the treatment of venous insufficiency. Phlebology 2016, 31, 106–113. [Google Scholar] [CrossRef]
- Morrison, N.; Gibson, K.; Vasquez, M.; Weiss, R.; Cher, D.; Madsen, M.; Jones, A. VeClose trial 12-month outcomes of cyanoacrylate closure versus radiofrequency ablation for incompetent great saphenous veins. J. Vasc. Surg. Venous Lymphat. Disord. 2017, 5, 321–330. [Google Scholar] [CrossRef] [PubMed]
- PR Newswire: Global Varicose Vein Treatment Market to Clock CAGR of ~5% from 2019 to 2027, Expanding Array of New Minimally-Invasive Techniques Key to Growth: Transparency Market Research. Available online: https://www.prnewswire.com/news-releases/global-varicose-vein-treatment-market-to-clock-cagr-of-5--from-2019-to-2027-expanding-array-of-new-minimally-invasive-techniques-key-to-growth-transparency-market-research-301010531.html (accessed on 29 December 2020).
- Gibson, K.; Ferris, B. Cyanoacrylate closure of incompetent great, small and accessory saphenous veins without the use of post-procedure compression: Initial outcomes of a post-market evaluation of the VenaSeal System (the WAVES Study). Vascular 2017, 25, 149–156. [Google Scholar] [CrossRef]
- Rasmussen, L.; Lawaetz, M.; Bjoern, L.; Blemings, A.; Eklof, B. Randomized clinical trial comparing endovenous laser ablation and stripping of the great saphenous vein with clinical and duplex outcome after 5 years. J. Vasc. Surg. 2013, 58, 421–426. [Google Scholar] [CrossRef] [Green Version]
- Van der Velden, S.K.; Lawaetz, M.; De Maeseneer, M.G.; Hollestein, L.; Nijsten, T.; van den Bos, R.R.; Members of the Predictors of Endovenous Thermal Ablation Group. Predictors of recanalization of the great saphenous vein in randomized controlled trials 1 year after endovenous thermal ablation. Eur. J. Vasc. Endovasc. Surg. 2016, 52, 234–241. [Google Scholar] [CrossRef] [Green Version]
- Gauw, S.A.; Lawson, J.A.; van Vlijmen-van Keulen, C.J.; Pronk, P.; Gaastra, M.T.; Mooij, M.C. Five-year follow-up of a randomized, controlled trial comparing saphenofemoral ligation and stripping of the great saphenous vein with endovenous laser ablation (980 nm) using local tumescent anesthesia. J. Vasc. Surg. 2016, 63, 420–428. [Google Scholar] [CrossRef] [Green Version]
- O’Donnell, T.F.; Balk, E.M.; Dermody, M.; Tangney, E.; Iafrati, M.D. Recurrence of varicose veins after endovenous ablation of the great saphenous vein in randomized trials. J. Vasc. Surg. Venous Lymphat. Disord. 2016, 4, 97–105. [Google Scholar] [CrossRef] [PubMed]
- Rass, K.; Frings, N.; Glowacki, P.; Gräber, S.; Tilgen, W.; Vogt, T. Same site recurrence is more frequent after endovenous laser ablation compared with high ligation and stripping of the great saphenous vein: 5 year results of a randomized clinical trial (RELACS Study). Eur. J. Vasc. Endovasc. Surg. 2015, 50, 648–656. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ratnam, L.A.; Marsh, P.; Holdstock, J.M.; Harrison, C.S.; Hussain, F.F.; Whiteley, M.S.; Lopez, A. Pelvic vein embolisation in the management of varicose veins. Cardiovasc. Intervent. Radiol. 2008, 31, 1159–1164. [Google Scholar] [CrossRef] [PubMed]
- Hartung, O. Embolization is essential in the treatment of leg varicosities due to pelvic venous insufficiency. Phlebology 2015, 30, 81–85. [Google Scholar] [CrossRef] [PubMed]
- Coleridge-Smith, P.; Labropoulos, N.; Partsch, H.; Myers, K.; Nicolaides, A.; Cavezzi, A. Duplex ultrasound investigation of the veins in chronic venous disease of the lower limbs—UIP consensus document. Part I. Basic principles. Eur. J. Vasc. Endovasc. Surg. 2006, 31, 83–92. [Google Scholar] [CrossRef] [Green Version]
- Cavezzi, A.; Labropoulos, N.; Partsch, H.; Ricci, S.; Caggiati, A.; Myers, K.; Nicolaides, A.; Smith, P.C. Duplex ultrasound investigation of the veins in chronic venous disease of the lower limbs—UIP consensus document. Part II. Anatomy. Eur. J. Vasc. Endovasc. Surg. 2006, 31, 288–299. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Asciutto, G.; Asciutto, K.C.; Mumme, A.; Geier, B. Pelvic venous incompetence: Reflux patterns and treatment results. Eur. J. Vasc. Endovasc. Surg. 2009, 38, 381–386. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beard, R.W.; Highman, J.H.; Pearce, S.; Reginald, P.W. Diagnosis of pelvic varicosities in women with chronic pelvic pain. Lancet 1984, 2, 946–949. [Google Scholar] [CrossRef]
- Coakley, F.V.; Varghese, S.L.; Hricak, H. CT and MRI of pelvic varices in women. J. Comput. Assist. Tomogr. 1999, 23, 429–434. [Google Scholar] [CrossRef] [PubMed]
- Park, S.J.; Lim, J.W.; Ko, Y.T.; Lee, D.H.; Yoon, Y.; Oh, J.H.; Lee, H.K.; Huh, C.Y. Diagnosis of pelvic congestion syndrome using transabdominal and transvaginal sonography. AJR Am. J. Roentgenol. 2004, 182, 683–688. [Google Scholar] [CrossRef]
- Ganeshan, A.; Upponi, S.; Hon, L.Q.; Uthappa, M.C.; Warakaulle, D.R.; Uberoi, R. Chronic pelvic pain due to pelvic congestion syndrome: The role of diagnostic and interventional radiology. Cardiovasc. Intervent. Radiol. 2007, 30, 1105–1111. [Google Scholar] [CrossRef]
- Bookwalter, C.A.; VanBuren, W.M.; Neisen, M.J.; Bjarnason, H. Imaging appearance and nonsurgical management of pelvic venous congestion syndrome. Radiographics 2019, 39, 596–608. [Google Scholar] [CrossRef]
- Lurie, F.; Passman, M.; Meisner, M.; Dalsing, M.; Masuda, E.; Welch, H.; Bush, R.L.; Blebea, J.; Carpentier, P.H.; De Maeseneer, M.; et al. The 2020 update of the CEAP classification system and reporting standards. J. Vasc. Surg. Venous Lymphat. Disord. 2020, 8, 342–352. [Google Scholar] [CrossRef]
- Dermody, M.; O’Donnell, T.F.; Balk, E.M. Complications of endovenous ablation in randomized controlled trials. J. Vasc. Surg. Venous Lymphat. Disord. 2013, 1, 427–436. [Google Scholar] [CrossRef]
- Nesbitt, C.; Bedenis, R.; Bhattacharya, V.; Stansby, G. Endovenous ablation (radiofrequency and laser) and foam sclerotherapy versus open surgery for great saphenous vein varices. Cochrane Database Syst. Rev. 2014, 7, CD005624. [Google Scholar] [CrossRef]
- Dermody, M.; Schul, M.W.; O’Donnell, T.F. Thromboembolic complications of endovenous thermal ablation and foam sclerotherapy in the treatment of great saphenous vein insufficiency. Phlebology 2015, 30, 357–364. [Google Scholar] [CrossRef] [PubMed]
- Healy, D.A.; Kimura, S.; Power, D.; Elhaj, A.; Abdeldaim, Y.; Cross, K.S.; McGreal, G.T.; Burke, P.E.; Moloney, T.; Manning, B.J.; et al. A systematic review and meta-analysis of thrombotic events following endovenous thermal ablation of the great saphenous vein. Eur. J. Vasc. Endovasc. Surg. 2018, 56, 410–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cavezzi, A. Medicine and phlebolymphology: Time to change? J. Clin. Med. 2020, 9, 4091. [Google Scholar] [CrossRef] [PubMed]
- Morrison, N.; Kolluri, R.; Vasquez, M.; Madsen, M.; Jones, A.; Gibson, K. Comparison of cyanoacrylate closure and radiofrequency ablation for the treatment of incompetent great saphenous veins: 36-month outcomes of the VeClose randomized controlled trial. Phlebology 2019, 34, 380–390. [Google Scholar] [CrossRef] [Green Version]
- Zollmann, P.; Zollmann, C.; Zollmann, P.; Veltman, J.; Kerzig, D.; Doerler, M.; Stücker, M. Determining the origin of superficial venous reflux in the groin with duplex ultrasound and implications for varicose vein surgery. J. Vasc. Surg. Venous Lymphat. Disord. 2017, 5, 82–86. [Google Scholar] [CrossRef] [PubMed]
- Zolotukhin, I.A.; Seliverstov, E.I.; Zakharova, E.A.; Kirienko, A.I. Short-term results of isolated phlebectomy with preservation of incompetent great saphenous vein (ASVAL procedure) in primary varicose veins disease. Phlebology 2017, 32, 601–607. [Google Scholar] [CrossRef]
- Onida, S.; Davies, A.H. CHIVA, ASVAL and related techniques—Concepts and evidence. Phlebology 2015, 30, 42–45. [Google Scholar] [CrossRef] [PubMed]
- Gianesini, S.; Occhionorelli, S.; Menegatti, E.; Zuolo, M.; Tessari, M.; Spath, P.; Ascanelli, S.; Zamboni, P. CHIVA strategy in chronic venous disease treatment: Instructions for users. Phlebology 2015, 30, 157–171. [Google Scholar] [CrossRef]
- Bellmunt-Montoya, S.; Escribano, J.M.; Dilme, J.; Martinez-Zapata, M.J. CHIVA method for the treatment of chronic venous insufficiency. Cochrane Database Syst. Rev. 2015, 6, CD009648. [Google Scholar] [CrossRef]
- Zygmunt, J.A. Duplex ultrasound for chronic venous insufficiency. J. Invasive Cardiol. 2014, 26, E149–E155. [Google Scholar]
- Garcia, R.; Labropoulos, N. Duplex ultrasound for the diagnosis of acute and chronic venous diseases. Surg. Clin. North Am. 2018, 98, 201–218. [Google Scholar] [CrossRef] [PubMed]
- Szary, C.; Wilczko, J.; Plucinska, D.; Pachuta, A.; Napierala, M.; Bodziony, A.; Zawadzki, M.; Grzela, T. The numbers of pregnancies and deliveries and their association with the selected morphological and hemodynamic parameters of pelvic and abdominal venous system. J. Clin Med. 2021. under review. [Google Scholar]
- Brown, C.L.; Rizer, M.; Alexander, R.; Sharpe, E.E., 3rd; Rochon, P.J. Pelvic congestion syndrome: Systematic review of treatment success. Semin. Interv. Radiol. 2018, 35, 35–40. [Google Scholar] [CrossRef]
- Hiromura, T.; Nishioka, T.; Nishioka, S.; Ikeda, H.; Tomita, K. Reflux in the left ovarian vein: Analysis of MDCT findings in asymptomatic women. AJR Am. J. Roentgenol. 2004, 183, 1411–1415. [Google Scholar] [CrossRef]
- Hansrani, V.; Morris, J.; Caress, A.L.; Payne, K.; Seif, M.; McCollum, C.N. Is pelvic vein incompetence associated with symptoms of chronic pelvic pain in women? A pilot study. Eur. J. Obstet. Gynecol. Reprod. Biol. 2016, 196, 21–25. [Google Scholar] [CrossRef]
- Szary, C.; Wilczko, J.; Zawadzki, M.; Grzela, T. Hemodynamic and radiological classification of ovarian veins system insufficiency. J. Clin. Med. 2021. under review. [Google Scholar]
- Del Frate, R.; Bricchi, M.; Franceschi, C. Minimally-invasive procedure for pelvic leak points in women. Veins Lymphat. 2019, 8, 7789. [Google Scholar] [CrossRef]
- Zamboni, P.; Franceschi, C.; Del Frate, R. The overtreatment of illusory May Thurner syndrome. Veins Lymphat. 2019, 8, 8020. [Google Scholar] [CrossRef]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter or Variable | Recurrence (n = 183) | No Treatment (n = 352) |
|---|---|---|
| Age | 45.5 (44.9) ± 9.9 | 40.7 (38.9) ± 10.4 * |
| Number of pregnancies (P) | 1.8 (2.0) ±1.3 | 1.7 (2.0) ±1.5 |
| 34 (18.6%) | 98 (27.8%) * |
| 41 (22.4%) | 63 (17.9%) |
| 65 (35.5%) | 111 (31.5%) |
| 32 (17.5%) | 46 (13.1%) |
| 11 (6.0%) | 34 (9.6%) |
| Number of deliveries | 1.7 (2.0) ± 1.2 | 1.4 (1.0) ± 1.3 * |
| Predominant signs and symptoms: | ||
| 75 (40.9%) | 122 (34.6%) |
| 104 (56.8%) | 148 (42.0%) * |
| 33 (18.0%) | 71 (20.2%) |
| Clinical classification (CEAP): | ||
| 17 (9.3%) | 39 (11.1%) |
| 101 (55.2%) | 213 (60.5%) |
| 52 (28.4%) | 76 (21.6%) |
| 13 (7.1%) | 24 (6.8%) |
| Parameter or Variable | Result |
|---|---|
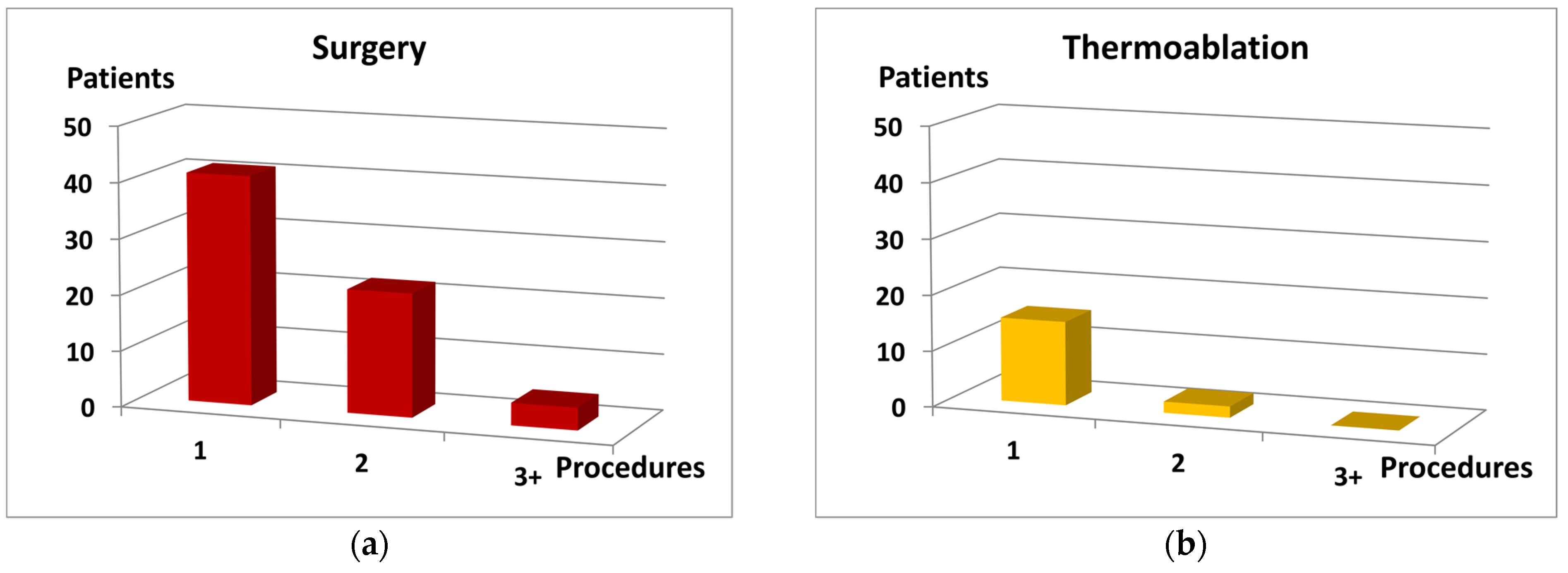
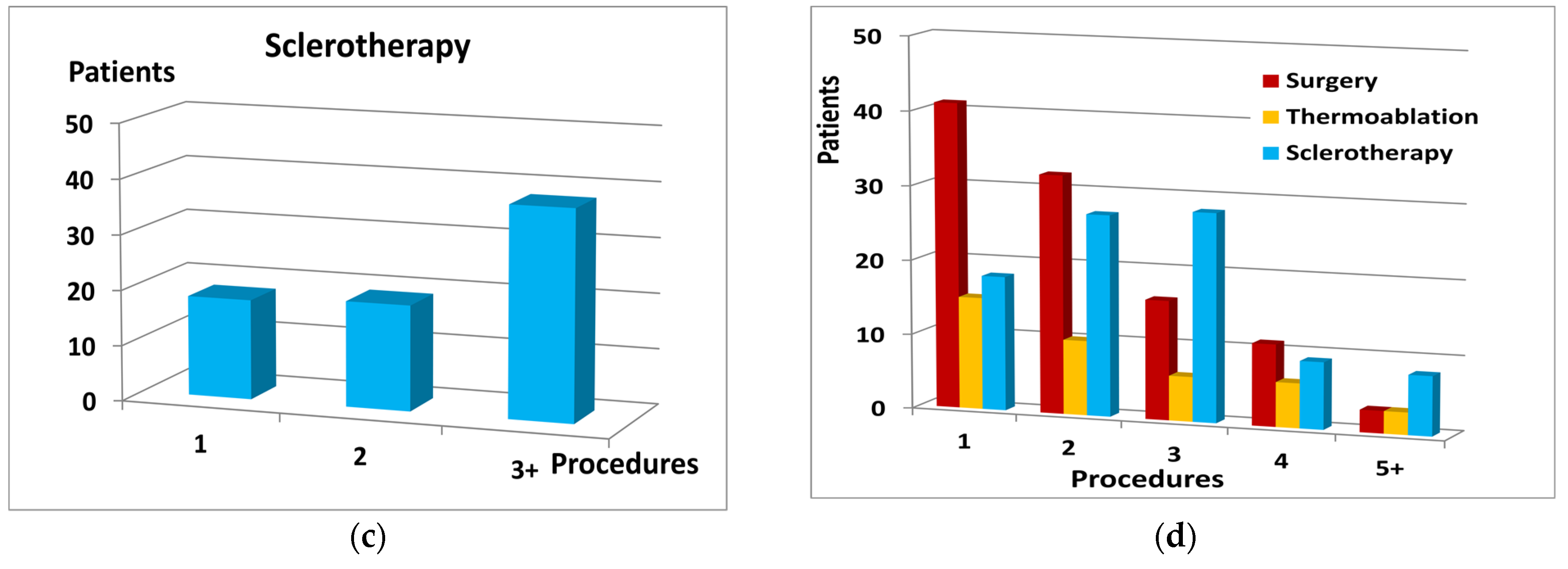
| Mean (median) number of procedures per patient | 2.1 (2.0) ± 1.2 |
| Type of procedure with the frequency of the same location recurrence: | |
| 103 (56.3%) |
| 92 (89.3%) |
| 40 (21.8%) |
| 32 (80.0%) |
| 88 (48.1%) |
| 82 (93.2%) |
| Parameter or Variable | Recurrence (n = 183) | No Treatment (n = 352) |
|---|---|---|
| Number of main venous trunks with reflux | 2.02 ± 0.9 | 1.75 ± 0.8 * |
| Incompetence in sapheno-femoral junction (SFJ) | 54 (29.5%) | 72 (20.4%) * |
| Bilateral incompetence in SFJ | 25 (13.6%) | 27 (7.7%) * |
| Detected entry points for reflux in the superficial system: | ||
| 8 (4.4%) | 3 (0.8%) * |
| 157 (85.8%) | 312 (88.6%) |
| 4 (2.2%) | 9 (2.6%) |
| 3 (1.6%) | 4 (1.1%) |
| Reflux in deep venous system | 10 (5.5%) | 22 (6.2%) |
| Parameter or Variable | Recurrence (n = 183) | No Treatment (n = 352) |
|---|---|---|
| Diameter of LCILV (mm) (1) | 14.1 (14.5) ± 2.2 | 13.4 (13.5) ± 2.7 |
| Diameter of LRV (mm) (2) | 8.1 (9.0) ± 3.8 | 7.8 (9.0) ± 3.6 |
| Diameter of LOV (mm) (3) | 6.7 (6.5) ± 1.9 | 6.6 (6.5) ± 2.1 |
| Diameter of ROV (mm) (3) | 5.8 (5.5) ± 1.7 | 5.9 (5.5) ± 1.9 |
| Diameter of PUV (mm) (4) | 6.7 (7.0) ± 1.3 | 6.6 (6.1) ± 1.4 |
| Reflux in LOV | 125 (68.3%) | 231 (65.6%) |
| Reflux in ROV | 49 (26.8%) | 112 (31.8%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Szary, C.; Wilczko, J.; Plucinska, D.; Pachuta, A.; Napierala, M.; Bodziony, A.; Zawadzki, M.; Leszczynski, J.; Galazka, Z.; Grzela, T. The Analysis of Selected Morphological and Hemodynamic Parameters of the Venous System and Their Presumable Impact on the Risk of Recurrence after Varicose Vein Treatment. J. Clin. Med. 2021, 10, 455. https://doi.org/10.3390/jcm10030455
Szary C, Wilczko J, Plucinska D, Pachuta A, Napierala M, Bodziony A, Zawadzki M, Leszczynski J, Galazka Z, Grzela T. The Analysis of Selected Morphological and Hemodynamic Parameters of the Venous System and Their Presumable Impact on the Risk of Recurrence after Varicose Vein Treatment. Journal of Clinical Medicine. 2021; 10(3):455. https://doi.org/10.3390/jcm10030455
Chicago/Turabian StyleSzary, Cezary, Justyna Wilczko, Dominika Plucinska, Anna Pachuta, Marcin Napierala, Anna Bodziony, Michal Zawadzki, Jerzy Leszczynski, Zbigniew Galazka, and Tomasz Grzela. 2021. "The Analysis of Selected Morphological and Hemodynamic Parameters of the Venous System and Their Presumable Impact on the Risk of Recurrence after Varicose Vein Treatment" Journal of Clinical Medicine 10, no. 3: 455. https://doi.org/10.3390/jcm10030455