
Vascular Dysfunction Predicts Future Deterioration of Left Ventricular Ejection Fraction in Patients with Heart Failure with Mildly Reduced Ejection Fraction

 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Protocol 1
2.2. Study Protocol 2
2.3. Measurements of FMD and NID
2.4. Measurement of Brachial IMT
2.5. Measurement of baPWV
2.6. Echocardiography
2.7. Statistical Analysis
3. Results
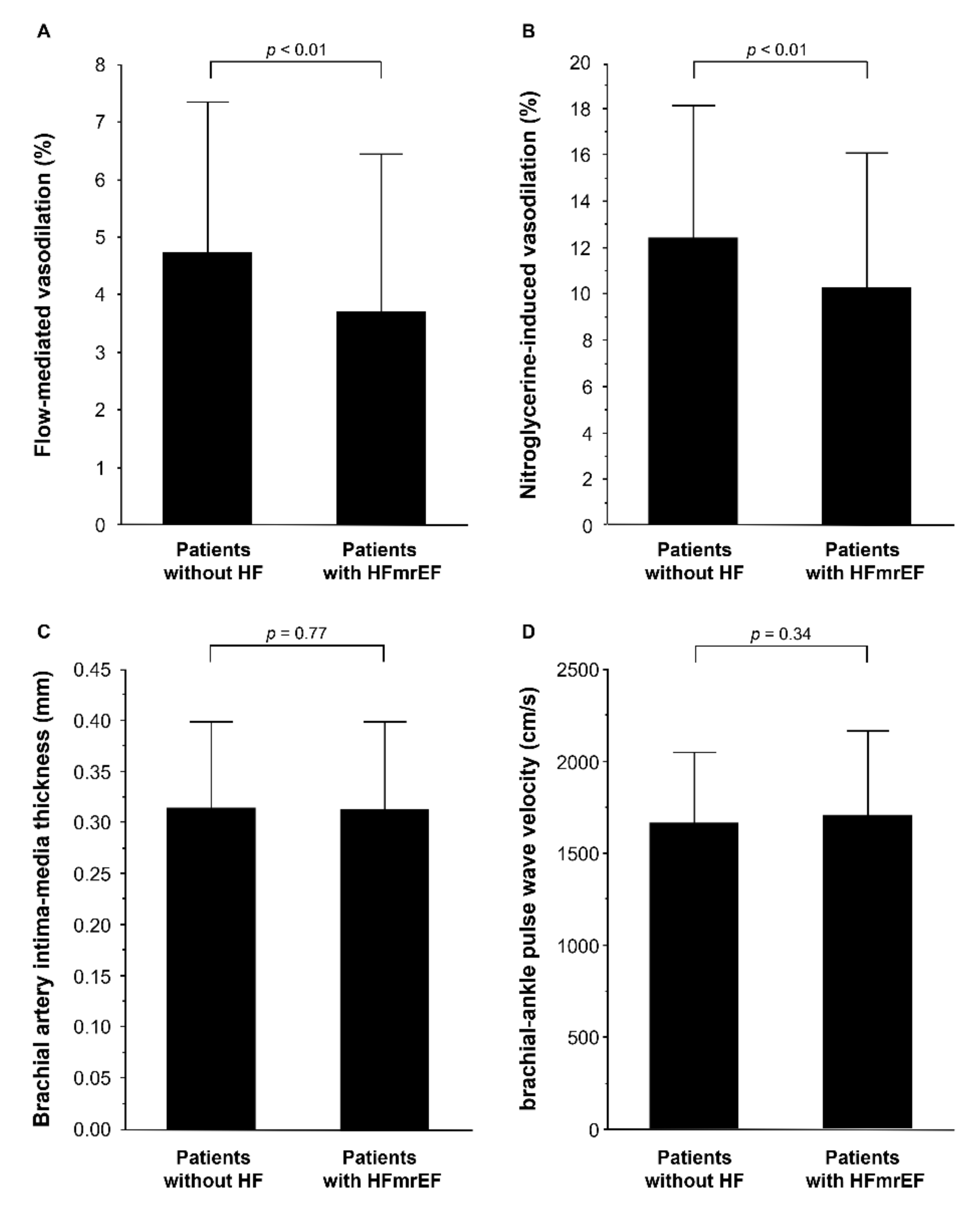
3.1. Study Protocol 1: Vascular Function and Vascular Structure in Patients with HFmrEF
3.2. Study Protocol 2: Association of NID with Future Deterioration of LVEF in Patients with HFmrEF
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cheng, R.K.; Cox, M.; Neely, M.L.; Heidenreich, P.A.; Bhatt, D.L.; Eapen, Z.J.; Hernandez, A.F.; Butler, J.; Yancy, C.W.; Fonarow, G.C. Outcomes in patients with heart failure with preserved, borderline, and reduced ejection fraction in the Medicare population. Am. Heart J. 2014, 168, 721–730. [Google Scholar] [CrossRef] [PubMed]
- Shah, K.S.; Xu, H.; Matsouaka, R.A.; Bhatt, D.L.; Heidenreich, P.A.; Hernandez, A.F.; Devore, A.D.; Yancy, C.W.; Fonarow, G.C. Heart Failure with Preserved, Borderline, and Reduced Ejection Fraction: 5-Year Outcomes. J. Am. Coll. Cardiol. 2017, 70, 2476–2486. [Google Scholar] [CrossRef]
- Katz, S.D.; Hryniewicz, K.; Hriljac, I.; Balidemaj, K.; Dimayuga, C.; Hudaihed, A.; Yasskiy, A. Vascular endothelial dysfunction and mortality risk in patients with chronic heart failure. Circulation 2005, 111, 310–314. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kubo, S.H.; Rector, T.S.; Bank, A.J.; Williams, R.E.; Heifetz, S.M. Endothelium-dependent vasodilation is attenuated in patients with heart failure. Circulation 1991, 84, 1589–1596. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nishioka, K.; Nakagawa, K.; Umemura, T.; Jitsuiki, D.; Ueda, K.; Goto, C.; Chayama, K.; Yoshizumi, M.; Higashi, Y. Carvedilol improves endothelium-dependent vasodilation in patients with dilated cardiomyopathy. Heart 2007, 93, 247–248. [Google Scholar] [CrossRef]
- Kishimoto, S.; Kajikawa, M.; Maruhashi, T.; Iwamoto, Y.; Matsumoto, T.; Iwamoto, A.; Oda, N.; Matsui, S.; Hidaka, T.; Kihara, Y.; et al. Endothelial dysfunction and abnormal vascular structure are simultaneously present in patients with heart failure with preserved ejection fraction. Int. J. Cardiol. 2017, 231, 181–187. [Google Scholar] [CrossRef] [Green Version]
- Premer, C.; Kanelidis, A.J.; Hare, J.M.; Schulman, I.H. Rethinking Endothelial Dysfunction as a Crucial Target in Fighting Heart Failure. Mayo Clin. Proceedings. Innov. Qual. Outcomes 2019, 3, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Lupón, J.; Gavidia-Bovadilla, G.; Ferrer, E.; de Antonio, M.; Perera-Lluna, A.; López-Ayerbe, J.; Domingo, M.; Núñez, J.; Zamora, E.; Moliner, P.; et al. Dynamic Trajectories of Left Ventricular Ejection Fraction in Heart Failure. J. Am. Coll Cardiol. 2018, 72, 591–601. [Google Scholar] [CrossRef]
- Savarese, G.; Vedin, O.; D’Amario, D.; Uijl, A.; Dahlström, U.; Rosano, G.; Lam, C.S.P.; Lund, L.H. Prevalence and Prognostic Implications of Longitudinal Ejection Fraction Change in Heart Failure. JACC Heart Fail. 2019, 7, 306–317. [Google Scholar] [CrossRef]
- Tsuji, K.; Sakata, Y.; Nochioka, K.; Miura, M.; Yamauchi, T.; Onose, T.; Abe, R.; Oikawa, T.; Kasahara, S.; Sato, M.; et al. Characterization of heart failure patients with mid-range left ventricular ejection fraction-a report from the CHART-2 Study. Eur. J. Heart Fail. 2017, 19, 1258–1269. [Google Scholar] [CrossRef] [Green Version]
- Chang, W.T.; Lin, C.H.; Hong, C.S.; Liao, C.T.; Liu, Y.W.; Chen, Z.C.; Shih, J.Y. The predictive value of global longitudinal strain in patients with heart failure mid-range ejection fraction. J. Cardiol. 2020, 77, 509–516. [Google Scholar] [CrossRef]
- Song, Y.; Li, F.; Xu, Y.; Liu, Y.; Wang, Y.; Han, X.; Fan, Y.; Cao, J.; Luo, J.; Sun, A.; et al. Prognostic value of sST2 in patients with heart failure with reduced, mid-range and preserved ejection fraction. Int. J. Cardiol. 2020, 304, 95–100. [Google Scholar] [CrossRef] [PubMed]
- Higashi, Y.; Noma, K.; Yoshizumi, M.; Kihara, Y. Endothelial function and oxidative stress in cardiovascular diseases. Circ. J. 2009, 73, 411–418. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ross, R. Atherosclerosis—An inflammatory disease. N. Engl. J. Med. 1999, 340, 115–126. [Google Scholar] [CrossRef] [PubMed]
- Celermajer, D.S.; Sorensen, K.E.; Gooch, V.M.; Spiegelhalter, D.J.; Miller, O.I.; Sullivan, I.D.; Lloyd, J.K.; Deanfield, J.E. Non-invasive detection of endothelial dysfunction in children and adults at risk of atherosclerosis. Lancet 1992, 340, 1111–1115. [Google Scholar] [CrossRef]
- Soga, J.; Noma, K.; Hata, T.; Hidaka, T.; Fujii, Y.; Idei, N.; Fujimura, N.; Mikami, S.; Maruhashi, T.; Kihara, Y.; et al. Rho-associated kinase activity, endothelial function, and cardiovascular risk factors. Arterioscler. Thromb. Vasc. Biol. 2011, 31, 2353–2359. [Google Scholar] [CrossRef] [Green Version]
- Gokce, N.; Keaney, J.F., Jr.; Hunter, L.M.; Watkins, M.T.; Menzoian, J.O.; Vita, J.A. Risk stratification for postoperative cardiovascular events via noninvasive assessment of endothelial function: A prospective study. Circulation 2002, 105, 1567–1572. [Google Scholar] [CrossRef] [Green Version]
- Maruhashi, T.; Soga, J.; Fujimura, N.; Idei, N.; Mikami, S.; Iwamoto, Y.; Kajikawa, M.; Matsumoto, T.; Hidaka, T.; Kihara, Y.; et al. Nitroglycerine-induced vasodilation for assessment of vascular function: A comparison with flow-mediated vasodilation. Arterioscler. Thromb. Vasc. Biol. 2013, 33, 1401–1408. [Google Scholar] [CrossRef] [Green Version]
- Lerman, A.; Zeiher, A.M. Endothelial function: Cardiac events. Circulation 2005, 111, 363–368. [Google Scholar] [CrossRef]
- Pandey, A.; Khan, H.; Newman, A.B.; Lakatta, E.G.; Forman, D.E.; Butler, J.; Berry, J.D. Arterial Stiffness and Risk of Overall Heart Failure, Heart Failure With Preserved Ejection Fraction, and Heart Failure With Reduced Ejection Fraction: The Health ABC Study (Health, Aging, and Body Composition). Hypertension 2017, 69, 267–274. [Google Scholar] [CrossRef]
- Ponikowski, P.; Voors, A.A.; Anker, S.D.; Bueno, H.; Cleland, J.G.; Coats, A.J.; Falk, V.; Gonzalez-Juanatey, J.R.; Harjola, V.P.; Jankowska, E.A.; et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. J. Heart Fail. 2016, 18, 891–975. [Google Scholar] [CrossRef]
- 2. Classification and Diagnosis of Diabetes. Diabetes Care 2017, 40, S11–S24. [CrossRef] [PubMed] [Green Version]
- Executive Summary of The Third Report of The National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, And Treatment of High Blood Cholesterol In Adults (Adult Treatment Panel III). Jama 2001, 285, 2486–2497. [CrossRef]
- Iwamoto, Y.; Maruhashi, T.; Fujii, Y.; Idei, N.; Fujimura, N.; Mikami, S.; Kajikawa, M.; Matsumoto, T.; Kihara, Y.; Chayama, K.; et al. Intima-media thickness of brachial artery, vascular function, and cardiovascular risk factors. Arterioscler. Thromb. Vasc. Biol. 2012, 32, 2295–2303. [Google Scholar] [CrossRef] [Green Version]
- Kimoto, E.; Shoji, T.; Shinohara, K.; Inaba, M.; Okuno, Y.; Miki, T.; Koyama, H.; Emoto, M.; Nishizawa, Y. Preferential stiffening of central over peripheral arteries in type 2 diabetes. Diabetes 2003, 52, 448–452. [Google Scholar] [CrossRef] [Green Version]
- Marti, C.N.; Gheorghiade, M.; Kalogeropoulos, A.P.; Georgiopoulou, V.V.; Quyyumi, A.A.; Butler, J. Endothelial dysfunction, arterial stiffness, and heart failure. J. Am. Coll. Cardiol. 2012, 60, 1455–1469. [Google Scholar] [CrossRef] [Green Version]
- Ontkean, M.; Gay, R.; Greenberg, B. Diminished endothelium-derived relaxing factor activity in an experimental model of chronic heart failure. Circ. Res. 1991, 69, 1088–1096. [Google Scholar] [CrossRef] [Green Version]
- Akiyama, E.; Sugiyama, S.; Matsuzawa, Y.; Konishi, M.; Suzuki, H.; Nozaki, T.; Ohba, K.; Matsubara, J.; Maeda, H.; Horibata, Y.; et al. Incremental prognostic significance of peripheral endothelial dysfunction in patients with heart failure with normal left ventricular ejection fraction. J. Am. Coll. Cardiol. 2012, 60, 1778–1786. [Google Scholar] [CrossRef] [Green Version]
- Münzel, T.; Feil, R.; Mülsch, A.; Lohmann, S.M.; Hofmann, F.; Walter, U. Physiology and pathophysiology of vascular signaling controlled by guanosine 3’,5’-cyclic monophosphate-dependent protein kinase. Circulation 2003, 108, 2172–2183. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Engström, G.; Melander, O.; Hedblad, B. Carotid intima-media thickness, systemic inflammation, and incidence of heart failure hospitalizations. Arterioscler. Thromb. Vasc. Biol. 2009, 29, 1691–1695. [Google Scholar] [CrossRef] [Green Version]
- Thakore, A.H.; Guo, C.Y.; Larson, M.G.; Corey, D.; Wang, T.J.; Vasan, R.S.; D’Agostino, R.B., Sr.; Lipinska, I.; Keaney, J.F., Jr.; Benjamin, E.J.; et al. Association of multiple inflammatory markers with carotid intimal medial thickness and stenosis (from the Framingham Heart Study). Am. J. Cardiol. 2007, 99, 1598–1602. [Google Scholar] [CrossRef] [PubMed]
- Neglia, D.; Michelassi, C.; Trivieri, M.G.; Sambuceti, G.; Giorgetti, A.; Pratali, L.; Gallopin, M.; Salvadori, P.; Sorace, O.; Carpeggiani, C.; et al. Prognostic role of myocardial blood flow impairment in idiopathic left ventricular dysfunction. Circulation 2002, 105, 186–193. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prasad, A.; Higano, S.T.; Al Suwaidi, J.; Holmes, D.R., Jr.; Mathew, V.; Pumper, G.; Lennon, R.J.; Lerman, A. Abnormal coronary microvascular endothelial function in humans with asymptomatic left ventricular dysfunction. Am. Heart J. 2003, 146, 549–554. [Google Scholar] [CrossRef]
- Kajikawa, M.; Maruhashi, T.; Hida, E.; Iwamoto, Y.; Matsumoto, T.; Iwamoto, A.; Oda, N.; Kishimoto, S.; Matsui, S.; Hidaka, T.; et al. Combination of Flow-Mediated Vasodilation and Nitroglycerine-Induced Vasodilation Is More Effective for Prediction of Cardiovascular Events. Hypertension 2016, 67, 1045–1052. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Variables | Total (n = 495) | Patients without HF (n = 426) | Patients with HFmrEF (n = 69) | p Value |
|---|---|---|---|---|
| Age, year | 61 ± 15 | 60 ± 15 | 66 ± 13 | <0.01 |
| Sex, men/women | 310/185 | 257/169 | 53/16 | <0.01 |
| Body mass index, kg/m2 | 24.0 ± 4.4 | 24.2 ± 4.4 | 22.8 ± 4.2 | 0.01 |
| Systolic blood pressure, mmHg | 133 ± 20 | 134 ± 20 | 127 ± 21 | <0.01 |
| Diastolic blood pressure, mmHg | 78 ± 12 | 79 ± 12 | 75 ± 14 | 0.01 |
| Heart rate, bpm | 71 ± 13 | 71 ± 13 | 73 ± 15 | 0.27 |
| Total cholesterol, mmol/L | 4.8 ± 1.0 | 4.9 ± 1.0 | 4.6 ± 0.9 | 0.03 |
| Triglycerides, mmol/L | 1.5 ± 1.0 | 1.5 ± 1.0 | 1.5 ± 1.1 | 0.59 |
| HDL cholesterol, mmol/L | 1.5 ± 0.5 | 1.6 ± 0.5 | 1.4 ± 0.4 | <0.01 |
| LDL cholesterol, mmol/L | 2.8 ± 0.9 | 2.8 ± 0.9 | 2.7 ± 0.8 | 0.26 |
| Glucose, mmol/L | 6.2 ± 1.9 | 6.1 ± 1.6 | 6.7 ± 2.5 | 0.01 |
| Hemoglobin A1c, % | 5.7 ± 0.8 | 5.6 ± 0.8 | 6.1 ± 1.1 | <0.01 |
| Blood urea nitrogen, mmol/L | 5.7 ± 1.9 | 5.4 ± 2.0 | 7.1 ± 2.5 | <0.01 |
| Creatinine, μmol/L | 71.6 ± 20.3 | 69.8 ± 17.7 | 88.4 ± 28.3 | <0.01 |
| NT-proBNP, pg/mL | 402 ± 873 | 199 ± 293 | 1373 ± 1704 | <0.01 |
| Etiology, n (%) | ||||
| Ischemic heart disease | 30 (43.5) | |||
| Dilated cardiomyopathy | 2 (2.9) | |||
| Hypertensive cardiomyopathy | 8 (11.6) | |||
| Valve disease | 11 (15.9) | |||
| Other | 18 (26.1) | |||
| Medical history, n (%) | ||||
| Hypertension | 376 (76.1) | 323 (75.8) | 53 (76.8) | 0.88 |
| Dyslipidemia | 315 (63.6) | 263 (61.7) | 52 (75.4) | 0.03 |
| Diabetes mellitus | 135 (27.2) | 112 (26.3) | 23 (33.3) | 0.23 |
| Previous coronary heart disease | 114 (23.1) | 83 (19.5) | 31 (44.9) | <0.01 |
| Previous stroke | 49 (10.0) | 37 (8.8) | 12 (17.4) | 0.04 |
| Current smoker, n (%) | 76 (15.5) | 64 (15.0) | 12 (17.4) | 0.64 |
| Medication, n (%) | ||||
| Antiplatelets | 143 (29.1) | 111 (26.1) | 32 (46.4) | <0.01 |
| Calcium channel blockers | 222 (45.2) | 203 (47.7) | 19 (27.5) | <0.01 |
| ACEI or ARB | 203 (41.3) | 156 (36.7) | 47 (68.1) | <0.01 |
| β-blockers | 121 (24.6) | 81 (19.0) | 40 (58.0) | <0.01 |
| Diuretics | 59 (12.0) | 31 (7.3) | 28 (40.6) | <0.01 |
| Statins | 199 (40.5) | 160 (37.6) | 39 (56.5) | <0.01 |
| Nitrates | 0 (0.0) | 0 (0.0) | 0 (0.0) | |
| Medically treated diabetes mellitus | ||||
| Any | 87 (17.7) | 77 (18.1) | 10 (14.5) | 0.44 |
| Insulin dependent | 22 (4.5) | 15 (3.5) | 7 (10.1) | 0.03 |
| Echocardiography | ||||
| LV ejection fraction, % | 61 ± 7 | 63 ± 5 | 45 ± 3 | <0.01 |
| LV end-diastolic dimension index, mm/m2 | 30 ± 1 | 29 ± 4 | 32 ± 6 | <0.01 |
| LV end-systolic dimension index, mm/m2 | 20 ± 8 | 19 ± 3 | 25 ± 4 | <0.01 |
| LV mass index, g/m2 | 95 ± 30 | 90 ± 23 | 126 ± 47 | <0.01 |
| LA volume index, mL/m2 | 36 ± 13 | 35 ± 11 | 46 ± 19 | <0.01 |
| Variables | Patients without HF (n = 55) | Patients with HFmrEF (n = 55) | p Value |
|---|---|---|---|
| Age, year | 67 ± 9 | 65 ± 14 | 0.51 |
| Sex, men/women | 43/12 | 42/13 | 0.82 |
| Body mass index, kg/m2 | 23.3 ± 3.8 | 22.7 ± 4.3 | 0.44 |
| Systolic blood pressure, mmHg | 128 ± 18 | 129 ± 22 | 0.78 |
| Diastolic blood pressure, mmHg | 75 ± 11 | 76 ± 15 | 0.80 |
| Heart rate, bpm | 69 ± 11 | 73 ± 15 | 0.05 |
| Total cholesterol, mmol/L | 4.6 ± 0.8 | 4.6 ± 0.8 | 0.96 |
| Triglycerides, mmol/L | 1.5 ± 1.1 | 1.6 ± 1.2 | 0.68 |
| HDL cholesterol, mmol/L | 1.5 ± 0.4 | 1.4 ± 0.4 | 0.16 |
| LDL cholesterol, mmol/L | 2.6 ± 0.7 | 2.7 ± 0.8 | 0.23 |
| Glucose, mmol/L | 6.2 ± 1.4 | 6.9 ± 2.7 | 0.55 |
| Hemoglobin A1c, % | 5.8 ± 1.0 | 6.1 ± 1.3 | 0.23 |
| Blood urea nitrogen, mmol/L | 6.4 ± 2.4 | 7.1 ± 2.8 | 0.15 |
| Creatinine, μmol/L | 81.3 ± 27.4 | 86.6 ± 30.1 | 0.36 |
| NT-proBNP, pg/mL | 245 ± 399 | 1390 ± 1779 | <0.01 |
| Etiology, n (%) | |||
| Ischemic heart disease | 23 (41.8) | ||
| Dilated cardiomyopathy | 1 (1.8) | ||
| Hypertensive cardiomyopathy | 8 (14.6) | ||
| Valve disease | 10 (18.2) | ||
| Other | 13 (23.6) | ||
| Medical history, n (%) | |||
| Hypertension | 46 (83.6) | 44 (80.0) | 0.62 |
| Dyslipidemia | 40 (72.7) | 39 (70.9) | 0.83 |
| Diabetes mellitus | 19 (34.6) | 20 (36.3) | 0.84 |
| Previous coronary heart disease | 20 (36.4) | 23 (41.8) | 0.56 |
| Previous stroke | 10 (18.2) | 12 (21.8) | 0.63 |
| Current smoker, n (%) | 9 (16.4) | 11 (20.0) | 0.62 |
| Medication, n (%) | |||
| Antiplatelets | 19 (34.6) | 23 (41.8) | 0.43 |
| Calcium channel blockers | 24 (43.6) | 15 (27.3) | 0.07 |
| ACEI or ARB | 34 (61.8) | 37 (67.3) | 0.55 |
| β-blockers | 21 (38.2) | 29 (52.7) | 0.12 |
| Diuretics | 11 (20.0) | 22 (40.0) | 0.02 |
| Statins | 28 (50.9) | 27 (49.1) | 0.85 |
| Nitrates | 0 (0.0) | 0 (0.0) | |
| Medically treated diabetes mellitus | |||
| Any | 15 (27.3) | 9 (16.4) | 0.16 |
| Insulin dependent | 3 (5.5) | 7 (12.7) | 0.18 |
| Echocardiography | |||
| LV ejection fraction, % | 61 ± 6 | 45 ± 3 | <0.01 |
| LV end-diastolic dimension index, mm/m2 | 29 ± 4 | 32 ± 5 | <0.01 |
| LV end-systolic dimension index, mm/m2 | 19 ± 3 | 25 ± 5 | <0.01 |
| LV mass index, g/m2 | 97 ± 35 | 127 ± 48 | <0.01 |
| LA volume index, mL/m2 | 38 ± 16 | 48 ± 19 | 0.59 |
| Variables | High and Intermediate NID (≥7.0%) (n = 26) | Low NID (<7.0%) (n = 13) | p Value |
|---|---|---|---|
| Age, year | 62 ± 14 | 66 ± 16 | 0.45 |
| Sex, men/women | 23/3 | 8/5 | 0.06 |
| Body mass index, kg/m2 | 23.0 ± 4.3 | 23.9 ± 4.1 | 0.55 |
| Systolic blood pressure, mmHg | 128 ± 20 | 133 ± 23 | 0.52 |
| Diastolic blood pressure, mmHg | 76 ± 12 | 74 ± 13 | 0.64 |
| Heart rate, bpm | 71 ± 11 | 78 ± 20 | 0.20 |
| Total cholesterol, mmol/L | 4.8 ± 0.8 | 4.3 ± 0.8 | 0.10 |
| Triglycerides, mmol/L | 1.8 ± 1.5 | 1.6 ± 0.9 | 0.79 |
| HDL cholesterol, mmol/L | 1.3 ± 0.3 | 1.5 ± 0.3 | 0.23 |
| LDL cholesterol, mmol/L | 2.9 ± 0.8 | 2.2 ± 0.5 | 0.03 |
| Glucose, mmol/L | 6.8 ± 2.1 | 8.0 ± 5.0 | 0.34 |
| Hemoglobin A1c, % | 6.3 ± 1.5 | 6.1 ± 0.3 | 0.67 |
| Blood urea nitrogen, mmol/L | 6.5 ± 2.4 | 7.6 ± 2.5 | 0.23 |
| Creatinine, μmol/L | 84.9 ± 28.3 | 100.8 ± 23.0 | 0.11 |
| NT-proBNP, pg/mL | 1114 ± 1741 | 1052 ± 634 | 0.91 |
| Etiology, n (%) | |||
| Ischemic heart disease | 11 (42.3) | 6 (46.2) | 0.65 |
| Dilated cardiomyopathy | 2 (7.7) | 0 (0.0) | 0.20 |
| Hypertensive cardiomyopathy | 2 (7.7) | 3 (23.1) | 0.19 |
| Valve disease | 5 (19.2) | 2 (15.4) | 0.77 |
| Other | 6 (23.1) | 2 (15.4) | 0.57 |
| Medical history, n (%) | |||
| Hypertension | 17 (65.4) | 12 (92.3) | 0.05 |
| Dyslipidemia | 21 (80.8) | 10 (76.9) | 0.78 |
| Diabetes mellitus | 10 (38.4) | 4 (30.8) | 0.63 |
| Previous coronary heart disease | 11 (42.3) | 6 (46.2) | 0.65 |
| Previous stroke | 2 (7.7) | 3 (23.1) | 0.19 |
| Current smoker, n (%) | 7 (26.9) | 2 (15.4) | 0.41 |
| Medication, n (%) | |||
| Antiplatelets | 11 (42.3) | 5 (38.5) | 0.82 |
| Calcium channel blockers | 10 (38.5) | 4 (30.8) | 0.63 |
| ACEI or ARB | 17 (65.4) | 9 (69.2) | 0.81 |
| β-blockers | 14 (53.9) | 8 (61.5) | 0.65 |
| Diuretics | 9 (34.6) | 4 (30.8) | 0.81 |
| Statins | 14 (53.9) | 7 (53.9) | 1.00 |
| Nitrates | 0 (0.0) | 0 (0.0) | |
| Medically treated diabetes mellitus | |||
| Any | 4 (15.4) | 0 (0.0) | 0.06 |
| Insulin dependent | 3 (11.5) | 1 (7.7) | 0.70 |
| Echocardiography | |||
| LV ejection fraction, % | 44 ± 3 | 46 ± 3 | 0.16 |
| LV end-diastolic dimension index, mm/m2 | 33 ± 5 | 31 ± 5 | 0.13 |
| LV end-systolic dimension index, mm/m2 | 26 ± 4 | 24 ± 4 | 0.17 |
| LV mass index, g/m2 | 128 ± 44 | 114 ± 48 | 0.38 |
| LA volume index, mL/m2 | 42 ± 13 | 54 ± 25 | 0.07 |
| FMD, % | 3.7 ± 2.6 | 3.2 ± 2.6 | 0.58 |
| NID, % | 12.4 ± 5.6 | 4.0 ± 1.7 | <0.01 |
| Brachial IMT, mm | 0.32 ± 0.10 | 0.32 ± 0.08 | 0.97 |
| baPWV, cm/s | 1655 ± 523 | 1916 ± 535 | 0.27 |
| Variable | Unadjusted HR (95% CI) p Value | Model 1 HR (95% CI) p Value | Model 2 HR (95% CI) p Value | Model 3 HR (95% CI) p Value | Model 4 HR (95% CI) p Value | Model 5 HR (95% CI) p Value |
|---|---|---|---|---|---|---|
| NID ≥ 7.0% | 1 (reference) | 1 (reference) | 1 (reference) | 1 (reference) | 1 (reference) | 1 (reference) |
| NID < 7.0% | 10.9 (1.3–93.7) 0.03 | 10.5 (1.2–92.1) 0.03 | 12.5 (1.0–152.5) 0.04 | 11.9 (1.3–106.3) 0.03 | 11.3 (1.2–102.6) 0.03 | 10.7 (1.2–93.8) 0.03 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kishimoto, S.; Maruhashi, T.; Kajikawa, M.; Harada, T.; Yamaji, T.; Han, Y.; Mizobuchi, A.; Hashimoto, Y.; Yoshimura, K.; Nakano, Y.; et al. Vascular Dysfunction Predicts Future Deterioration of Left Ventricular Ejection Fraction in Patients with Heart Failure with Mildly Reduced Ejection Fraction. J. Clin. Med. 2021, 10, 5980. https://doi.org/10.3390/jcm10245980
Kishimoto S, Maruhashi T, Kajikawa M, Harada T, Yamaji T, Han Y, Mizobuchi A, Hashimoto Y, Yoshimura K, Nakano Y, et al. Vascular Dysfunction Predicts Future Deterioration of Left Ventricular Ejection Fraction in Patients with Heart Failure with Mildly Reduced Ejection Fraction. Journal of Clinical Medicine. 2021; 10(24):5980. https://doi.org/10.3390/jcm10245980
Chicago/Turabian StyleKishimoto, Shinji, Tatsuya Maruhashi, Masato Kajikawa, Takahiro Harada, Takayuki Yamaji, Yiming Han, Aya Mizobuchi, Yu Hashimoto, Kenichi Yoshimura, Yukiko Nakano, and et al. 2021. "Vascular Dysfunction Predicts Future Deterioration of Left Ventricular Ejection Fraction in Patients with Heart Failure with Mildly Reduced Ejection Fraction" Journal of Clinical Medicine 10, no. 24: 5980. https://doi.org/10.3390/jcm10245980