
Pursuing More Aggressive Timelines in the Surgical Treatment of Traumatic Spinal Cord Injury (TSCI): A Retrospective Cohort Study with Subgroup Analysis

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Preconditions
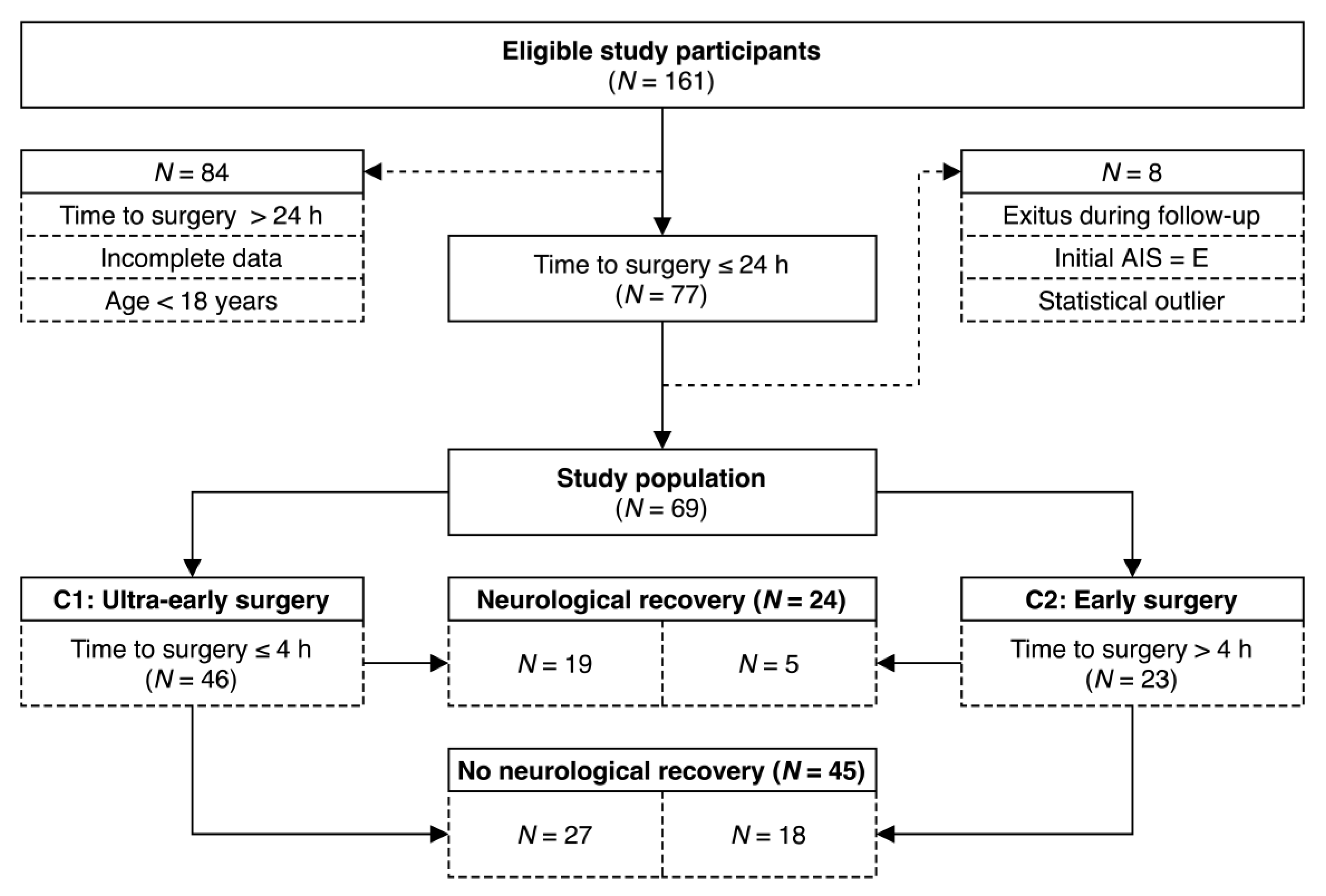
2.2. Study Population: Inclusion and Exclusion Criteria
2.3. Grouping
2.4. Standardized Treatment
2.5. Outcome
2.6. Variables of Interest
2.7. Statistical Methods
2.8. Power
2.9. Missing Data
3. Results
3.1. Demographics
3.2. Timing Characteristics
3.3. Neurological Recovery
3.4. Post hoc Analysis
3.4.1. Cutpoint of Time from Injury to Surgery vs. Optimal Cutpoint
3.4.2. Subgroup Analysis
4. Discussion
4.1. Post hoc Analysis
4.1.1. Optimal Cutpoint
4.1.2. Subgroups
4.2. Defining “Early” Surgery
4.3. Efficacy and Feasibility of Early Surgical Treatment of the Spinal Cord
4.4. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Furlan, J.C.; Sakakibara, B.M.; Miller, W.C.; Krassioukov, A.V. Global incidence and prevalence of traumatic spinal cord injury. Can. J. Neurol. Sci. J. Can. Sci. Neurol. 2013, 40, 456–464. [Google Scholar] [CrossRef]
- National Spinal Cord Injury Statistical Center (NSCISC). Spinal Cord Injury (SCI), Facts and Figures at a Glance. 2017. Available online: https://www.nscisc.uab.edu/Public/Facts%20and%20Figures%20-%202017.pdf (accessed on 22 May 2017).
- Khazaeipour, Z.; Norouzi-Javidan, A.; Kaveh, M.; Khanzadeh Mehrabani, F.; Kazazi, E.; Emami-Razavi, S.H. Psychosocial outcomes following spinal cord injury in Iran. J. Spinal Cord Med. 2014, 37, 338–345. [Google Scholar] [CrossRef] [Green Version]
- Krueger, H.; Noonan, V.K.; Trenaman, L.M.; Joshi, P.; Rivers, C.S. The economic burden of traumatic spinal cord injury in Canada. Chronic Dis. Inj. Can. 2013, 33, 113–122. [Google Scholar] [CrossRef]
- Tator, C.H. Update on the pathophysiology and pathology of acute spinal cord injury. Brain Pathol. 1995, 5, 407–413. [Google Scholar] [CrossRef]
- Cadotte, D.W.; Fehlings, M.G. Spinal cord injury: A systematic review of current treatment options. Clin. Orthop. Relat. Res. 2011, 469, 732–741. [Google Scholar] [CrossRef] [Green Version]
- Fehlings, M.G.; Kwon, B.K.; Tetreault, L.A. Guidelines for the Management of Degenerative Cervical Myelopathy and Spinal Cord Injury: An Introduction to a Focus Issue. Glob. Spine J. 2017, 7, 6s–7s. [Google Scholar] [CrossRef]
- Fehlings, M.G.; Vaccaro, A.; Wilson, J.R.; Singh, A.; Cadotte, D.; Harrop, J.S.; Aarabi, B.; Shaffrey, C.; Dvorak, M.; Fisher, C.; et al. Early versus delayed decompression for traumatic cervical spinal cord injury: Results of the Surgical Timing in Acute Spinal Cord Injury Study (STASCIS). PLoS ONE 2012, 7, e32037. [Google Scholar] [CrossRef] [PubMed]
- Biglari, B.; Child, C.; Yildirim, T.M.; Swing, T.; Reitzel, T.; Moghaddam, A. Does surgical treatment within 4 hours after trauma have an influence on neurological remission in patients with acute spinal cord injury? Clin. Risk Manag. 2016, 12, 1339–1346. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- La Rosa, G.; Conti, A.; Cardali, S.; Cacciola, F.; Tomasello, F. Does early decompression improve neurological outcome of spinal cord injured patients? Appraisal of the literature using a meta-analytical approach. Spinal Cord 2004, 42, 503–512. [Google Scholar] [CrossRef] [Green Version]
- Liu, J.M.; Long, X.H.; Zhou, Y.; Peng, H.W.; Liu, Z.L.; Huang, S.H. Is Urgent Decompression Superior to Delayed Surgery for Traumatic Spinal Cord Injury? A Meta-Analysis. World Neurosurg. 2016, 87, 124–131. [Google Scholar] [CrossRef]
- Mattiassich, G.; Gollwitzer, M.; Gaderer, F.; Blocher, M.; Osti, M.; Lill, M.; Ortmaier, R.; Haider, T.; Hitzl, W.; Resch, H.; et al. Functional Outcomes in Individuals Undergoing Very Early (<5 h) and Early (5–24 h) Surgical Decompression in Traumatic Cervical Spinal Cord Injury: Analysis of Neurological Improvement from the Austrian Spinal Cord Injury Study. J. Neurotrauma 2017, 34, 3362–3371. [Google Scholar] [CrossRef]
- Dvorak, M.F.; Noonan, V.K.; Fallah, N.; Fisher, C.G.; Finkelstein, J.; Kwon, B.K.; Rivers, C.S.; Ahn, H.; Paquet, J.; Tsai, E.C.; et al. The influence of time from injury to surgery on motor recovery and length of hospital stay in acute traumatic spinal cord injury: An observational Canadian cohort study. J. Neurotrauma 2015, 32, 645–654. [Google Scholar] [CrossRef]
- van Middendorp, J.J.; Hosman, A.J.; Doi, S.A. The effects of the timing of spinal surgery after traumatic spinal cord injury: A systematic review and meta-analysis. J. Neurotrauma 2013, 30, 1781–1794. [Google Scholar] [CrossRef] [PubMed]
- Piazza, M.; Schuster, J. Timing of Surgery After Spinal Cord Injury. Neurosurg. Clin. N. Am. 2017, 28, 31–39. [Google Scholar] [CrossRef] [PubMed]
- Levi, L.; Wolf, A.; Rigamonti, D.; Ragheb, J.; Mirvis, S.; Robinson, W.L. Anterior decompression in cervical spine trauma: Does the timing of surgery affect the outcome? Neurosurgery 1991, 29, 216–222. [Google Scholar] [CrossRef]
- Mirza, S.K.; Krengel, W.F., 3rd; Chapman, J.R.; Anderson, P.A.; Bailey, J.C.; Grady, M.S.; Yuan, H.A. Early versus delayed surgery for acute cervical spinal cord injury. Clin. Orthop. Relat. Res. 1999, 359, 104–114. [Google Scholar] [CrossRef]
- Croce, M.A.; Bee, T.K.; Pritchard, E.; Miller, P.R.; Fabian, T.C. Does optimal timing for spine fracture fixation exist? Ann. Surg. 2001, 233, 851–858. [Google Scholar] [CrossRef] [PubMed]
- Duh, M.S.; Shepard, M.J.; Wilberger, J.E.; Bracken, M.B. The effectiveness of surgery on the treatment of acute spinal cord injury and its relation to pharmacological treatment. Neurosurgery 1994, 35, 240–248. [Google Scholar] [CrossRef]
- Chen, L.; Yang, H.; Yang, T.; Xu, Y.; Bao, Z.; Tang, T. Effectiveness of surgical treatment for traumatic central cord syndrome. J. Neurosurg. Spine 2009, 10, 3–8. [Google Scholar] [CrossRef] [Green Version]
- Liu, Y.; Shi, C.G.; Wang, X.W.; Chen, H.J.; Wang, C.; Cao, P.; Gao, R.; Ren, X.J.; Luo, Z.J.; Wang, B.; et al. Timing of surgical decompression for traumatic cervical spinal cord injury. Int. Orthop. 2015, 39, 2457–2463. [Google Scholar] [CrossRef]
- Wilson, J.R.; Witiw, C.D.; Badhiwala, J.; Kwon, B.K.; Fehlings, M.G.; Harrop, J.S. Early Surgery for Traumatic Spinal Cord Injury: Where Are We Now? Glob. Spine J. 2020, 10, 84S–91S. [Google Scholar] [CrossRef] [Green Version]
- Grassner, L.; Wutte, C.; Klein, B.; Mach, O.; Riesner, S.; Panzer, S.; Vogel, M.; Buhren, V.; Strowitzki, M.; Vastmans, J.; et al. Early Decompression (<8 h) after Traumatic Cervical Spinal Cord Injury Improves Functional Outcome as Assessed by Spinal Cord Independence Measure after One Year. J. Neurotrauma 2016, 33, 1658–1666. [Google Scholar] [CrossRef]
- Wilson, J.R.; Singh, A.; Craven, C.; Verrier, M.C.; Drew, B.; Ahn, H.; Ford, M.; Fehlings, M.G. Early versus late surgery for traumatic spinal cord injury: The results of a prospective Canadian cohort study. Spinal Cord 2012, 50, 840–843. [Google Scholar] [CrossRef]
- Löfvenmark, I.; Norrbrink, C.; Nilsson-Wikmar, L.; Hultling, C.; Chakandinakira, S.; Hasselberg, M. Traumatic spinal cord injury in Botswana: Characteristics, aetiology and mortality. Spinal Cord 2015, 53, 150–154. [Google Scholar] [CrossRef] [Green Version]
- Anderson, K.K.; Tetreault, L.; Shamji, M.F.; Singh, A.; Vukas, R.R.; Harrop, J.S.; Fehlings, M.G.; Vaccaro, A.R.; Hilibrand, A.S.; Arnold, P.M. Optimal Timing of Surgical Decompression for Acute Traumatic Central Cord Syndrome: A Systematic Review of the Literature. Neurosurgery 2015, 77 (Suppl. S4), S15–S32. [Google Scholar] [CrossRef]
- Noonan, V.K.; Kwon, B.K.; Soril, L.; Fehlings, M.G.; Hurlbert, R.J.; Townson, A.; Johnson, M.; Dvorak, M.F. The Rick Hansen Spinal Cord Injury Registry (RHSCIR): A national patient-registry. Spinal Cord 2012, 50, 22–27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DeVivo, M.; Biering-Sorensen, F.; Charlifue, S.; Noonan, V.; Post, M.; Stripling, T.; Wing, P. International Spinal Cord Injury Core Data Set. Spinal Cord 2006, 44, 535–540. [Google Scholar] [CrossRef] [PubMed]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. Ann. Intern. Med. 2007, 147, 573–577. [Google Scholar] [CrossRef] [Green Version]
- World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA 2013, 310, 2191–2194. [CrossRef] [PubMed] [Green Version]
- Tukey, J.W. Exploratory Data Analysis, [Repr.] ed.; Addison-Wesley: Reading, MA, USA, 1977; Volume 2. [Google Scholar]
- Kirshblum, S.; Snider, B.; Rupp, R.; Read, M.S. Updates of the International Standards for Neurologic Classification of Spinal Cord Injury: 2015 and 2019. Phys. Med. Rehabil. Clin. N. Am. 2020, 31, 319–330. [Google Scholar] [CrossRef]
- Kirshblum, S.C.; Waring, W.; Biering-Sorensen, F.; Burns, S.P.; Johansen, M.; Schmidt-Read, M.; Donovan, W.; Graves, D.; Jha, A.; Jones, L.; et al. Reference for the 2011 revision of the International Standards for Neurological Classification of Spinal Cord Injury. J. Spinal Cord. Med. 2011, 34, 547–554. [Google Scholar] [CrossRef] [Green Version]
- Fawcett, J.W.; Curt, A.; Steeves, J.D.; Coleman, W.P.; Tuszynski, M.H.; Lammertse, D.; Bartlett, P.F.; Blight, A.R.; Dietz, V.; Ditunno, J.; et al. Guidelines for the conduct of clinical trials for spinal cord injury as developed by the ICCP panel: Spontaneous recovery after spinal cord injury and statistical power needed for therapeutic clinical trials. Spinal Cord 2007, 45, 190–205. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Youden, W.J. Index for rating diagnostic tests. Cancer 1950, 3, 32–35. [Google Scholar] [CrossRef]
- Boschloo, R. Raised conditional level of significance for the 2 × 2-table when testing the equality of two probabilities. Stat. Neerl. 1970, 24, 1–9. [Google Scholar] [CrossRef]
- Hanley, J.A.; McNeil, B.J. The meaning and use of the area under a receiver operating characteristic (ROC) curve. Radiology 1982, 143, 29–36. [Google Scholar] [CrossRef] [Green Version]
- Wilke, C.O. gridtext: Improved Text Rendering Support for ‘Grid’ Graphics. 2020. Available online: https://wilkelab.org/gridtext/ (accessed on 17 June 2021).
- Wilke, C.O. ggtext: Improved Text Rendering Support for ‘ggplot2’. 2020. Available online: https://wilkelab.org/ggtext/ (accessed on 17 June 2021).
- Wickham, H.; François, R.; Henry, L.; Müller, K. dplyr: A Grammar of Data Manipulation. 2020. Available online: https://dplyr.tidyverse.org/reference/dplyr-package.html (accessed on 17 June 2021).
- Wickham, H.; Bryan, J. readxl: Read Excel Files. 2019. Available online: https://www.scirp.org/(S(lz5mqp453ed%20snp55rrgjct55))/reference/referencespapers.aspx?referenceid=2761680 (accessed on 17 June 2021).
- Wickham, H.; Averick, M.; Bryan, J.; Chang, W.; McGowan, L.D.A.; François, R.; Grolemund, G.; Hayes, A.; Henry, L.; Hester, J.; et al. Welcome to the tidyverse. J. Open Source Softw. 2019, 4, 1686. [Google Scholar] [CrossRef]
- Wickham, H. ggplot2: Elegant Graphics for Data Analysis; Springer: New York, NY, USA, 2016. [Google Scholar]
- Thiele, C. cutpointr: Determine and Evaluate Optimal Cutpoints in Binary Classification Tasks. 2020. Available online: https://rdrr.io/cran/cutpointr/ (accessed on 17 June 2021).
- R Core Team. R: A Language and Environment for Statistical Computing; R Core Team: Vienna, Austria, 2020. [Google Scholar]
- Ooms, J. writexl: Export Data Frames to Excel ‘xlsx’ Format. 2020. Available online: https://www.R-project.org/ (accessed on 17 June 2021).
- Hester, J.; Wickham, H. fs: Cross-Platform File System Operations Based on ‘libuv’. 2020. Available online: https://cran.r-project.org/web/packages/fs/index.html (accessed on 17 June 2021).
- Hester, J. glue: Interpreted String Literals. 2020. Available online: https://glue.tidyverse.org/ (accessed on 17 June 2021).
- Heinzen, E.; Sinnwell, J.; Atkinson, E.; Gunderson, T.; Dougherty, G. arsenal: An Arsenal of ‘R’ Functions for Large-Scale Statistical Summaries. 2020. Available online: https://mayoverse.github.io/arsenal/reference/arsenal.html (accessed on 17 June 2021).
- Vaccaro, A.R.; Oner, C.; Kepler, C.K.; Dvorak, M.; Schnake, K.; Bellabarba, C.; Reinhold, M.; Aarabi, B.; Kandziora, F.; Chapman, J.; et al. AOSpine thoracolumbar spine injury classification system: Fracture description, neurological status, and key modifiers. Spine 2013, 38, 2028–2037. [Google Scholar] [CrossRef] [PubMed]
- van Middendorp, J.J.; Barbagallo, G.; Schuetz, M.; Hosman, A.J. Design and rationale of a Prospective, Observational European Multicenter study on the efficacy of acute surgical decompression after traumatic Spinal Cord Injury: The SCI-POEM study. Spinal Cord 2012, 50, 686–694. [Google Scholar] [CrossRef]
- Jug, M.; Kejzar, N.; Vesel, M.; Al Mawed, S.; Dobravec, M.; Herman, S.; Bajrovic, F.F. Neurological Recovery after Traumatic Cervical Spinal Cord Injury Is Superior if Surgical Decompression and Instrumented Fusion Are Performed within 8 Hours versus 8 to 24 Hours after Injury: A Single Center Experience. J. Neurotrauma 2015, 32, 1385–1392. [Google Scholar] [CrossRef] [PubMed]
- Coleman, W.P.; Geisler, F.H. Injury severity as primary predictor of outcome in acute spinal cord injury: Retrospective results from a large multicenter clinical trial. Spine J. Off. J. N. Am. Spine Soc. 2004, 4, 373–378. [Google Scholar] [CrossRef]
- Khorasanizadeh, M.; Yousefifard, M.; Eskian, M.; Lu, Y.; Chalangari, M.; Harrop, J.S.; Jazayeri, S.B.; Seyedpour, S.; Khodaei, B.; Hosseini, M.; et al. Neurological recovery following traumatic spinal cord injury: A systematic review and meta-analysis. J. Neurosurg. Spine 2019, 30, 683–699. [Google Scholar] [CrossRef]
- Wilson, J.R.; Jaja, B.; Kwon, B.K.; Guest, J.; Harrop, J.S.; Aarabi, B.; Shaffrey, C.; Badhiwala, J.; Toups, E.; Grossman, R.; et al. Natural History, Predictors of Outcome and Effects of Treatment in Thoracic Spinal Cord Injury: A Multicenter Cohort Study from the North American Clinical Trials Network. J. Neurotrauma 2018, 35, 2554–2560. [Google Scholar] [CrossRef]
- Furlan, J.C.; Noonan, V.; Cadotte, D.W.; Fehlings, M.G. Timing of decompressive surgery of spinal cord after traumatic spinal cord injury: An evidence-based examination of pre-clinical and clinical studies. J. Neurotrauma 2011, 28, 1371–1399. [Google Scholar] [CrossRef] [PubMed]
- Ahuja, C.S.; Badhiwala, J.H.; Fehlings, M.G. “Time is spine”: The importance of early intervention for traumatic spinal cord injury. Spinal Cord 2020, 58, 1037–1039. [Google Scholar] [CrossRef] [PubMed]
- Samuel, A.M.; Bohl, D.D.; Basques, B.A.; Diaz-Collado, P.J.; Lukasiewicz, A.M.; Webb, M.L.; Grauer, J.N. Analysis of Delays to Surgery for Cervical Spinal Cord Injuries. Spine 2015, 40, 992–1000. [Google Scholar] [CrossRef] [PubMed]
- Aarabi, B.; Akhtar-Danesh, N.; Chryssikos, T.; Shanmuganathan, K.; Schwartzbauer, G.T.; Simard, J.M.; Olexa, J.; Sansur, C.A.; Crandall, K.M.; Mushlin, H.; et al. Efficacy of Ultra-Early (<12 h), Early (12–24 h), and Late (>24–138.5 h) Surgery with Magnetic Resonance Imaging-Confirmed Decompression in American Spinal Injury Association Impairment Scale Grades A, B, and C Cervical Spinal Cord Injury. J. Neurotrauma 2020, 37, 448–457. [Google Scholar] [CrossRef] [PubMed]
- Saadoun, S.; Werndle, M.C.; Lopez de Heredia, L.; Papadopoulos, M.C. The dura causes spinal cord compression after spinal cord injury. Br. J. Neurosurg. 2016, 30, 582–584. [Google Scholar] [CrossRef]
- Furlan, J.C.; Bracken, M.B.; Fehlings, M.G. Is age a key determinant of mortality and neurological outcome after acute traumatic spinal cord injury? Neurobiol. Aging 2010, 31, 434–446. [Google Scholar] [CrossRef]
- Ahn, H.; Bailey, C.S.; Rivers, C.S.; Noonan, V.K.; Tsai, E.C.; Fourney, D.R.; Attabib, N.; Kwon, B.K.; Christie, S.D.; Fehlings, M.G.; et al. Effect of older age on treatment decisions and outcomes among patients with traumatic spinal cord injury. CMAJ 2015, 187, 873–880. [Google Scholar] [CrossRef] [Green Version]
- Wilson, J.R.; Voth, J.; Singh, A.; Middleton, J.; Jaglal, S.B.; Singh, J.M.; Mainprize, T.G.; Yee, A.; Fehlings, M.G. Defining the Pathway to Definitive Care and Surgical Decompression after Traumatic Spinal Cord Injury: Results of a Canadian Population-Based Cohort Study. J. Neurotrauma 2016, 33, 963–971. [Google Scholar] [CrossRef]
- Steeves, J.D.; Lammertse, D.; Curt, A.; Fawcett, J.W.; Tuszynski, M.H.; Ditunno, J.F.; Ellaway, P.H.; Fehlings, M.G.; Guest, J.D.; Kleitman, N.; et al. Guidelines for the conduct of clinical trials for spinal cord injury (SCI) as developed by the ICCP panel: Clinical trial outcome measures. Spinal Cord 2007, 45, 206–221. [Google Scholar] [CrossRef] [PubMed]
- Burns, A.S.; Marino, R.J.; Kalsi-Ryan, S.; Middleton, J.W.; Tetreault, L.A.; Dettori, J.R.; Mihalovich, K.E.; Fehlings, M.G. Type and Timing of Rehabilitation Following Acute and Subacute Spinal Cord Injury: A Systematic Review. Glob. Spine J 2017, 7, 175S–194S. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| C1 | C2 | Total | p-Value | |
|---|---|---|---|---|
| Ultra-Early (<4 h) | Early (4–24 h) | |||
| (N = 46) | (N = 23) | (N = 69) | ||
| Neurological recovery | 0.112 a | |||
| yes | 19 (41.3%) | 5 (21.7%) | 24 (34.8%) | |
| no | 27 (58.7%) | 18 (78.3%) | 45 (65.2%) | |
| Sex | 1.000 a | |||
| female | 8 (17.4%) | 4 (17.4%) | 12 (17.4%) | |
| male | 38 (82.6%) | 19 (82.6%) | 57 (82.6%) | |
| Age | 0.010 b | |||
| M ± SD | 41.1 (15.7) | 53.9 (20.2) | 45.4 (18.2) | |
| Median (IQR) | 41.0 (20.0, 86.0) | 59.0 (20.0, 80.0) | 43.0 (20.0, 86.0) | |
| Etiology of injury | 0.142 c | |||
| Falls | 28 (60.9%) | 11 (47.8%) | 39 (56.5%) | |
| Transport activities | 16 (34.8%) | 10 (43.5%) | 26 (37.7%) | |
| Sports and leisure activities | 0 (0.0%) | 2 (8.7%) | 2 (2.9%) | |
| Other traumatic causes | 2 (4.3%) | 0 (0.0%) | 2 (2.9%) | |
| Severity of TSCI | 0.657 a | |||
| Incomplete | 21 (45.7%) | 12 (52.2%) | 33 (47.8%) | |
| Complete | 25 (54.3%) | 11 (47.8%) | 36 (52.2%) | |
| Neurological level of injury | 0.528 c | |||
| Cervical | 18 (39.1%) | 12 (52.2%) | 30 (43.5%) | |
| Thoracic | 20 (43.5%) | 7 (30.4%) | 27 (39.1%) | |
| Lumbar | 8 (17.4%) | 4 (17.4%) | 12 (17.4%) | |
| AO Classification | 0.942 c | |||
| A | 24 (52.2%) | 11 (47.8%) | 35 (50.7%) | |
| B | 8 (17.4%) | 5 (21.7%) | 13 (18.8%) | |
| C | 14 (30.4%) | 7 (30.4%) | 21 (30.4%) | |
| AIS initial | 0.383 c | |||
| A | 31 (67.4%) | 13 (56.5%) | 44 (63.8%) | |
| B | 6 (13.0%) | 3 (13.0%) | 9 (13.0%) | |
| C | 7 (15.2%) | 3 (13.0%) | 10 (14.5%) | |
| D | 2 (4.3%) | 4 (17.4%) | 6 (8.7%) | |
| AIS final | 1.000 c | |||
| A | 23 (50.0%) | 12 (52.2%) | 35 (50.7%) | |
| B | 4 (8.7%) | 1 (4.3%) | 5 (7.2%) | |
| C | 7 (15.2%) | 4 (17.4%) | 11 (15.9%) | |
| D | 12 (26.1%) | 6 (26.1%) | 18 (26.1%) | |
| Time from injury to surgery (min) | <0.001 b | |||
| M ± SD | 191.7 (35.6) | 304.9 (69.3) | 229.4 (72.7) | |
| Median (IQR) | 195.0 (118.0, 240.0) | 273.0 (244.0, 463.0) | 225.0 (118.0, 463.0) | |
| Time from injury to admission (min) | <0.001 b | |||
| M ± SD | 58.7 (26.1) | 92.3 (51.8) | 69.9 (39.7) | |
| Median (IQR) | 53.5 (22.0, 132.0) | 75.0 (46.0, 244.0) | 63.0 (22.0, 244.0) | |
| Time from admission to surgery (min) | <0.001 b | |||
| M ± SD | 133.0 (36.6) | 212.5 (42.5) | 159.5 (53.8) | |
| Median (IQR) | 126.5 (69.0, 210.0) | 206.0 (158.0, 309.0) | 158.0 (69.0, 309.0) | |
| Duration of surgery (min) | 0.688 b | |||
| M ± SD | 163.8 (58.1) | 169.5 (85.3) | 165.7 (67.8) | |
| Median (IQR) | 156.0 (33.0, 314.0) | 141.0 (64.0, 371.0) | 150.0 (33.0, 371.0) |
| Cervical | Thoracic | Lumbar | Total | p-Value | |
|---|---|---|---|---|---|
| (N = 30) | (N = 27) | (N = 12) | (N = 69) | ||
| Improvement | 0.101 a | ||||
| yes | 11 (36.7%) | 6 (22.2%) | 7 (58.3%) | 24 (34.8%) | |
| no | 19 (63.3%) | 21 (77.8%) | 5 (41.7%) | 45 (65.2%) | |
| Time from injury to surgery (min) | 0.258 b | ||||
| M ± SD | 252.1 (88.0) | 212.9 (57.6) | 209.9 (43.6) | 229.4 (72.7) | |
| Median (IQR) | 233.5 (125.0, 463.0) | 209.0 (118.0, 385.0) | 210.5 (127.0, 275.0) | 225.0 (118.0, 463.0) | |
| Min | 125 | 118 | 127 | 118 | |
| Max | 463 | 385 | 275 | 463 | |
| Time from injury to admission (min) | 0.330 b | ||||
| M ± SD | 76.9 (51.9) | 60.6 (26.4) | 73.5 (25.0) | 69.9 (39.7) | |
| Median (IQR) | 65.0 (24.0, 244.0) | 54.0 (22.0, 132.0) | 67.5 (47.0, 118.0) | 63.0 (22.0, 244.0) | |
| Min | 24 | 22 | 47 | 22 | |
| Max | 244 | 132 | 118 | 244 | |
| Time from admission to surgery (min) | 0.088 b | ||||
| M ± SD | 175.2 (59.2) | 152.3 (48.9) | 136.4 (40.4) | 159.5 (53.8) | |
| Median (IQR) | 185.5 (84.0, 286.0) | 141.0 (80.0, 309.0) | 150.0 (69.0, 182.0) | 158.0 (69.0, 309.0) | |
| Min | 84 | 80 | 69 | 69 | |
| Max | 286 | 309 | 182 | 309 | |
| Duration of surgery (min) | 0.124 b | ||||
| M ± SD | 151.9 (70.7) | 182.1 (64.9) | 163.2 (64.0) | 165.7 (67.8) | |
| Median (IQR) | 133.0 (33.0, 314.0) | 162.0 (110.0, 371.0) | 152.5 (77.0, 297.0) | 150.0 (33.0, 371.0) | |
| Min | 33 | 110 | 77 | 33 | |
| Max | 314 | 371 | 297 | 371 | |
| Severity of TSCI | 0.053 a | ||||
| Incomplete | 18 (60.0%) | 8 (29.6%) | 7 (58.3%) | 33 (47.8%) | |
| Complete | 12 (40.0%) | 19 (70.4%) | 5 (41.7%) | 36 (52.2%) | |
| Type of plegia | <0.001 a | ||||
| Paraplegia | 9 (30.0%) | 26 (96.3%) | 12 (100.0%) | 47 (68.1%) | |
| Tetraplegia | 21 (70.0%) | 1 (3.7%) | 0 (0.0%) | 22 (31.9%) | |
| Incomplete (N = 33) | Complete (N = 36) | Total (N = 69) | p-Value | |
|---|---|---|---|---|
| Neurological improvement | 0.006 a | |||
| yes | 17 (51.5%) | 7 (19.4%) | 24 (34.8%) | |
| no | 16 (48.5%) | 29 (80.6%) | 45 (65.2%) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bock, T.; Heller, R.A.; Haubruck, P.; Raven, T.F.; Pilz, M.; Moghaddam, A.; Biglari, B. Pursuing More Aggressive Timelines in the Surgical Treatment of Traumatic Spinal Cord Injury (TSCI): A Retrospective Cohort Study with Subgroup Analysis. J. Clin. Med. 2021, 10, 5977. https://doi.org/10.3390/jcm10245977
Bock T, Heller RA, Haubruck P, Raven TF, Pilz M, Moghaddam A, Biglari B. Pursuing More Aggressive Timelines in the Surgical Treatment of Traumatic Spinal Cord Injury (TSCI): A Retrospective Cohort Study with Subgroup Analysis. Journal of Clinical Medicine. 2021; 10(24):5977. https://doi.org/10.3390/jcm10245977
Chicago/Turabian StyleBock, Tobias, Raban Arved Heller, Patrick Haubruck, Tim Friedrich Raven, Maximilian Pilz, Arash Moghaddam, and Bahram Biglari. 2021. "Pursuing More Aggressive Timelines in the Surgical Treatment of Traumatic Spinal Cord Injury (TSCI): A Retrospective Cohort Study with Subgroup Analysis" Journal of Clinical Medicine 10, no. 24: 5977. https://doi.org/10.3390/jcm10245977